
Abstract
INTRODUCTION
Smoking remains a major health risk factor and China is the world’s largest consumer of tobacco. Smoke-free policies in public places are a powerful weapon in tobacco control. Therefore, the aim of this study was to assess the association between smoke-free policies in public places and smoking cessation among smokers in China from 2012 to 2020.
METHODS
In this study, we assessed the impact of smoke-free public places policies on smoking cessation situation among smokers aged 16 years and older. We do this by conducting a difference-in-differences analysis using data from the China Family Panel Study (CFPS) 2012-2020.
FINDINGS
By 2020, about 60.2% of the cities were covered by partial smoke-free policies and about 38.5% by comprehensive smoke-free policies. Based on the results of the study, we found that the medium-term effect model (Model 2, 2012:2016; Model 3, 2012:2018) of the impact of partial smoke-free policies on smoking cessation was not statistically significant using 2012 as the study baseline; the short-term effect model (Model 1; 2012:2014; P< .01) and the long-term effect model (Model 4; 2012:2020; P< .05) were statistically significant; the effect of a comprehensive smoke-free policy on smoking cessation (Model 5; 2012:2020; P<.05) was statistically significant.
CONCLUSION
China’s existing comprehensive smoke-free policies have had a modest impact on smoking cessation among the smoking population, and a strong, comprehensive national smoke-free law is urgently needed to achieve greater public health outcomes.
IMPLICATIONS
Smoke-free policies are an important intervention to influence smoking behavior. This study demonstrates that comprehensive smoke-free policies in public places in China can effectively influence smoking behavior and show long-term trends in smoke-free behavior, while also reflecting the need to promote comprehensive smoke-free policies. This study provides a basis for the implementation of comprehensive smokefree policies into law and also provides a basis for policy makers.
Introduction
China has a huge burden of noncommunicable diseases and tobacco use is the leading risk factor for major non-communicable diseases. China is the world’s largest cultivator of tobacco, producing about 3 million tons of tobacco leaf in 2009 (43% of the global total), and 3.4 million tons in 2012. 1 In 2018, 26.6% of Chinese adults used tobacco (about 300 million current smokers). 2 According to 2019 data, the average daily smoking prevalence among adults is 13% in Britain and Northern Ireland, 14% in the United States of America, and 23% in China. 3 The adverse effects of smoking are reflected in the damage to human health. A large number of epidemiological studies have shown that smoking is a leading cause of lung cancer, colorectal cancer, fatal coronary heart disease, and chronic obstructive pulmonary disease.4–7 The economic burden of tobacco is substantial. In 2012, hospital treatment costs for acute myocardial infarction and stroke alone were estimated at ¥50 billion (US$8 billion). 8 The tobacco control situation in China is very serious.
In addition to active smokers, there are also people who are passively exposed to second-hand smoke. In China, the number of smokers exceeds 350 million, and 750 million people are passive smokers. 2 The implementation of smoke-free policies in public places such as workplaces and transportation are necessary to protect passive smokers from second-hand smoke exposure and to motivate smokers to quit. A comprehensive smoke-free policy requires that all indoor public places, workplaces, and transportation are smoke-free, and that there are penalties for violators. To better build a fully smoke-free environment, China became a party to the WHO Framework Convention on Tobacco Control (FCTC) in 2005. 9 Among its many provisions, the evidence-based treaty requires its member states to protect people from tobacco smoke by enacting national smoke-free indoor air laws, but smoking rates in public places remain high and there is still no national smoke-free legislation. 9 Only a few cities, such as Beijing and Shanghai, have fully smoke-free policies. By 2021, most provinces and cities will still have incomplete smoke-free policies, only partially implemented smoke-free policies, and will lack strong enforcement agencies. 10
Some studies 11 have selected public places in 7 Chinese cities to evaluate smoke-free policies, but few studies have observed the overall effect of smoke-free environments in the context of smoke-free policies in each Chinese province. To this aim, this study developed 5 DID statistical models using data from the China Family Panel Studies (CFPS) database for the period 2012-2020 to assess the impact of partial smoke-free policies and full smoke-free policies on smoking cessation in 19 Chinese provinces, and to observe overall smoke-free trends and explore the future direction of local smoke-free policies in China.
Methods
Data sources and sample
In this study, we used the nationally representative China Family Panel Studies (CFPS; link: http://www.isss.pku.edu.cn/cfps/ (accessed on 21 February 2021)) data collected by the Institute of Social Science Survey (ISSS) of Peking University. The CFPS provides data for academic research and policy decision-making by tracking and collecting data at 3 levels—individual, family, and community—to reflect changes in China’s society, economy, population, education, and health. The baseline survey was officially launched in 2010. The CFPS sample covers 25 provinces, municipalities, and autonomous regions with a target sample size of 16,000 households and includes all household members in the sample. 12 We exclude Hainan Province due to the small amount of data. In addition, 5 cities in Jiangxi, Zhejiang, Jilin, Shanxi and Hebei had 2 successive policy interventions during the observation period, and it is not feasible to analyze the effect of one policy alone, so we also exclude them. Therefore, our analysis was based on 19 provinces. For the smoke-free policies, we obtained the provincial smoke-free policies from the official websites of the provincial people's governments and the official websites of the National Health Commission (policy source websites in the Supplement).
The follow-up of the CFPS data started in 2010. As there were insufficient smoking-related data in 2010 and the proportion of non-null values in the total sample was too small, we chose 2012 as the baseline year for a biennial survey ending in 2020. The remaining 4 surveys were compared with 2012 one by one to create 4 models. We considered the 2 years as a unit and called the period 2010-2012 period1, the period 2012-2014 period2, the period 2014-2016 period3, the period 2016-2018 period4 and the period 2018-2020 period5. Research subjects were screened as follows: (1) aged over 16 years; (2) had a history of smoking or were current smokers.
Variables
Outcome: Smoking status
Subjects who had answered the question “Age of quitting smoking” and the time of quitting smoking for one year or more were defined as ever smokers when enrolled at baseline. Subjects who had answered yes to the question “Whether smoked cigarettes last month” or the time of quitting for less one year were defined as current smokers.
Treatment: Smoke-free policy
We collected smoke-free regulations published on official provincial government websites, mainly from the Regulations on the Management of Public Health and the Regulations on the Control of Smoking in Public Places. Figure1 shows the distribution of partial smoke-free policies and comprehensive smoke-free policies in each province in China and the starting dates of the 2 policies. For example, the partial smoke-free policy in Tianjin was implemented in 2012, and the comprehensive smoke-free policy in Shanghai was implemented in 2017. The distribution of partial and comprehensive smoke-free policies in the 24 provinces of China.
Covariates
Potential covariates included demographic characteristics: age, gender, education level (primary school or below, middle or technical secondary school, undergraduate or junior college), current marital status (unmarried, married), income (denotes total income from all work) history of alcohol that was measured in the question “Have you had 3 drinks in the past month?” (yes/no), occupation (ISCO-88 Code).
Statistical analysis
We used a quasi-experimental difference-in-difference (DID) analysis to assess the effect of a smoke-free policy on smokers' cessation behavior.13–15 Typically, an intervention and control group are observed in 2 time periods, with only the intervention group affected by the policy in the second time period. The DID model estimates policy effects by comparing the mean change in outcome in the intervention group before and after the policy intervention. The appeal of DID estimation lies in its simplicity and its potential to avoid many of the endogeneity problems that typically arise when making comparisons between heterogeneous individuals. Each DID model contains 2 dimensions, time and treatment, and an interaction term between these 2 variables. The parallel trend assumption was verified using linear models that included an indicator for the intervention state, year dummies, and interaction terms between these 2 variables. A common trend test and a placebo test were done at the same time (eFigure 1 and eTable 1 in the Supplement). A detailed chart of the exclusion criteria can be found in the Supplement (eFigure 2).
Unbiased DID estimates must satisfy the parallel trend assumption, which requires that, in the absence of the policy, outcomes in the intervention and control groups follow parallel trends over time, a property that cannot be observed because the policy has been implemented. 13 Therefore, in this study we included data before (2010-2012) and after (2012-2014, 2014-2016, 2016-2018, 2018-2020).
As the smoke-free policy interventions differed across Chinese provinces, we observed the effects of the 2 smoke-free policies on 5 statistical models that were run identically: (a) Model 1 includes a control for the status of provinces with partial smoke-free policy interventions and provinces without smoke-free policy interventions, comparing the years 2010-2012 and 2012-2014, to observe the short-term effects of the partial smoke-free policy on smokers’ cessation behavior. (b) Model 2 is the same as model 1, comparing the years 2010-2012 and 2014-2016, to examine the medium-term effects of partial smoke-free policies on smokers’ cessation behavior. (c) Model 3 is the same intervention as Model 1, comparing the years 2010-2012 with 2016-2018, looking at the medium-term effects of partial smoke-free policies on smokers' cessation behavior. (d) Model 4 is the same intervention as model 1, comparing the years 2010-2012 with 2018-2020 to observe the long-term effects of a partial smoke-free policy on smokers' cessation behavior. (e) Model 5 includes controls for provinces with a comprehensive smoke-free policy intervention and provinces without a smoke-free policy intervention, comparing the years 2010-2012 with 2018-2020, to observe the effect of a comprehensive smoke-free policy on smokers' cessation behavior. The same adjustments were made in all 5 models.
Linear DID regression models report marginal effects of strategies and all other covariates of different intensity classes as well as a 95% confidence interval (CI). The data used for this analysis is open source and has been audited to qualify for downloading the data. All analyses were performed using Stata V.14 with P-values of P < .05 to determine statistical significance.
Results
Participant Characteristics and Smoke-free Policy Distribution.

Effect of smoke-free policies on ever smokers and current smokers.
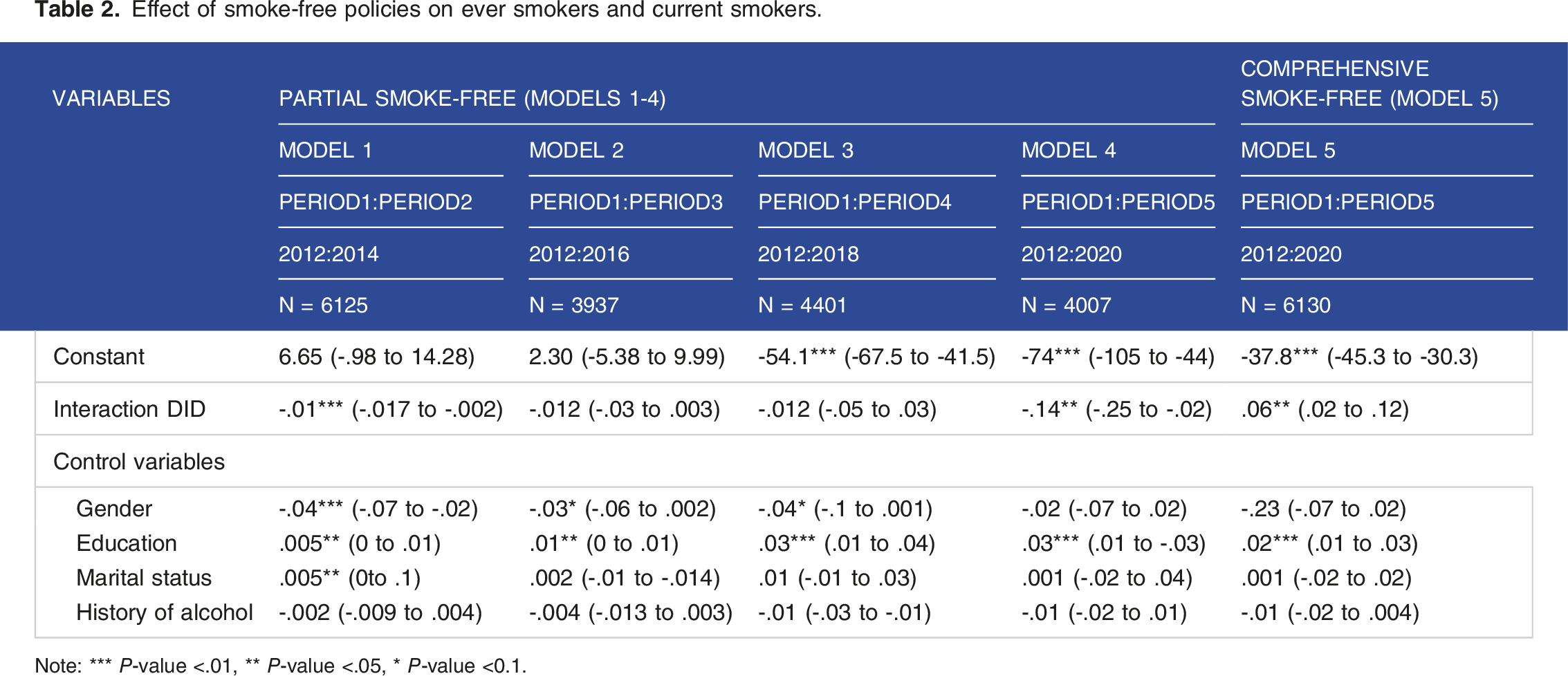
Note: *** P-value <.01, ** P-value <.05, * P-value <0.1.
Discussion
We examined the relationship between the effects of implementing 2 levels of smoke-free policies and smokers’ cessation status in 19 Chinese provinces. This study found that partial smoke-free policies did not motivate smokers to quit and that comprehensive smoke-free policies had a catalytic effect on smokers’ cessation behavior, supporting the urgent need for strong comprehensive smoke-free laws in China.
Models 1-4 were designed to investigate the effect of partial smoke-free policies on smokers’ quitting behavior. The results of Models 1 and 4 were statistically significant and showed a negative effect, with the implementation of a partial smoke-free policy not encouraging smokers to quit and having a small effect on current smokers. The results of this study are consistent with the results of 2 studies11,16 which both found that the implementation of a partial smoke-free policy had a negligible effect on smoking, expressing the urgent need for a comprehensive smoke-free policy. As of 2021, local smoke-free policies are not comprehensive enough and some smoke-free policies cover a larger proportion of the population and are not fully implemented. For example, workplaces, restaurants and bars are often not covered and have designated smoking areas,17,18 which further hampers the development of smoke-free programmes.19,20 The results of model 5 show a positive and significant effect, demonstrating the facilitating effect of a comprehensive smoke-free policy on smokers’ cessation behavior. This result is consistent with the findings from studies of provinces with comprehensive smoke-free policies – Beijing,21,22 Guangzhou 23 and Shanghai 24 where comprehensive smoke-free policies have better tobacco control effects, reducing exposure to second-hand smoke in public places and helping smokers to quit.
We suspect that the reasons for the modest impact of partial and complete smoke-free policies on smoking cessation are related to warnings on cigarette packaging, 25 tobacco prices 26 and policy implementation, 10 such as the impact of the 2015 tobacco tax increase on cigarette prices, which increased retail cigarette prices by an average of 11% and the cheapest cigarette brands by 20%. However, the cheapest cigarettes are still cheaper than in other countries and the persistence of such cigarettes remains a major public health challenge and will become more widespread over time as people's incomes continue to rise. 26
The main limitation of this study was that the effect of the policy intervention could not be directly observed. After preliminary data analysis, we found that the proportion of people who had quit smoking during the 2 years of the policy intervention before the observation point was too small for this to introduce error, so we included people who had quit smoking for many years to indirectly observe the effect of the policy intervention by observing changes in the total number of people who had quit smoking. In addition, those who have quit smoking for less than one year are counted as current smokers because they have a high rate of relapse 27 and their smoking status is unstable, indirectly observing the effect of the policy on curbing relapse.
The descriptive statistics of this study show an increase in the proportion of ever smokers, demonstrating a national trend towards smoking cessation, and there are national research studies that show a clear development of a smoke-free trend in China 28 and that this trend is likely to be due to the promotion of smoke-free policies over several years. 11 However, it is not enough to simply implement comprehensive smoke-free legislation. First, managers of smoky workplaces, restaurants and bars should strictly enforce smoke-free policies 16 to protect customers’ rights; second, this can be achieved by changing the textual warnings on cigarette packages to graphic warnings. 25 Some studies have shown that the use of graphic warnings can reduce the intention to smoke among young people. 29 Policymakers, practitioners and researchers should design more appropriate warnings to reduce smoking rates. 30 Third, a significant increase in tobacco taxes could help reduce overall demand. 17 Only by combining smoke-free policies with other smoking cessation measures can the country achieve its goal of reducing smoking rates to 20% by 2030.
Conclusion
The new 'Healthy China 2030’ strategy sets ambitious targets for policymakers, including a reduction in smoking prevalence to 20% by 2030, to be achieved through the implementation of comprehensive smoke-free policies across the country. China’s existing comprehensive smoke-free policies have had a moderate impact on the health status of the smoking population, and a strong, comprehensive national smoke-free law is urgently needed to achieve better public health outcomes.
Supplemental Material
Supplemental Material - China’s Smoke-free Policies in Public Place and the Smoking Cessation Status of Smokers
Supplemental Material for China’s Smoke-free Policies in Public Place and the Smoking Cessation Status of Smokers by Jing Wen, Wenlu Shang, Yong Ding, Hui Qiao, and Jiangping Li in Tobacco Use Insights.
Footnotes
Acknowledgements
We would particularly like to thank the China Family Tracking Study (CFPS) for providing a database for academic research and public policy analysis. Thanks to a large number of staff for their great efforts and selfless contributions to the investigation of CFPS, the results obtained by CFPS embody collective wisdom and efforts. Thank you to the frontline interviewers for their tremendous efforts in the investigation. Thanks to ISSS for providing reliable and easily accessible data. Thanks to the fund for providing support for the project.
Author contributions
Jiangping Li & Jing Wen designed the study. Wenlu Shang & Yong Ding & Hui Qiao conducted the data analysis. Wenlu Shang drafted the manuscript. Jing Wen & Yong Ding & Hui Qiao revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Literacy Monitoring Project in Yongning County, Yinchuan City.
Data availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.