
Abstract
Background:
Community-based management of acute malnutrition is implementing in Ethiopia but there is scarce information in our study set up regarding the time to recovery and its predictors of severe acute malnutrition among 6 to 59 months children, so this study aimed to assess the time to recovery and its predictors for uncomplicated severe acute malnutrition among 6 to 59 children managed at the outpatient therapeutic program in north Shewa zone, Ethiopia.
Methods:
A health post-based prospective follow-up study was conducted on 6 to 59 months children from November 20/2020 to February 20/2021. A total of 423 children had included in the study. A structured interviewer-administered questionnaire had used. The median time to recovery had calculated using the Kaplan-Meier curve. Bi-variable and multi-variable Cox regression models with a 95% confidence interval (CI) were done. Finally, the variable that had a P-value < .05 in the multi-variable analysis was declared as the predictors of time to recovery. Proportional hazard assumption was checked graphically and using Schoenfeld residual test.
Result:
From the total 423 Children, 327 (77.3%) recovered. The median time to recovery was 42 (IQR 14) days. Children from food secure households; AHR = 9.6 with 95% CI (8.1-18.5), mild food insecure; AHR = 6.5 with 95% CI (3.1, 13.8), moderate food insecure; AHR = 2.5 with 95% CI (1.2-5.3). Mothers who traveled less than 2 hours walking distance to the health post; AHR = 2.6 with 95% CI (1.8-18.7). Children who received the correct dose of the RUTF AHR = 1.6 with 95% CI (1.1-2.3), children who measured their weight weekly AHR = 1.5 with 95% CI (1.1-2.0), and children treated by health extension worker who took the Nutrition-related training AHR = 2.1 with 95% CI (1.0-4.5) were predictors of time to recovery.
Conclusion:
The median time to recovery was within the acceptable range of the Ethiopian protocol for the management of uncomplicated SAM in the Outpatient setup. Household food security status, the distance between home and health posts, the correct dose of RUTF, weekly weight measurement per protocol, and HEWs nutrition-related training status were the significant predictors of time to recovery.
Background
Community-Based Management of Acute Malnutrition (CMAM) is a decentralized community-based approach to treating acute malnutrition. 1 Uncomplicated Severe acute malnutrition (SAM) can be defined as; a weight-for-height measurement of ⩽70%, weight for height Z score < −3 Standard deviations (SD), And/Or a mid-upper-arm circumference of <115 mm (MUAC) in children age 6 to 59 months without any medical complications. 1 Both macro and micronutrient malnutrition is a public health problem in under-5 children in the world. Globally around 17 million children suffered from SAM in 2018. 2 The Ethiopian demographic and health survey, 3 revealed that 38%, 24%, 10%, and 3% of children under the age of 5 years had stunting, underweight, wasting, and severe wasting respectively. In Ethiopia, malnutrition attributes about 53% of all under-5 deaths. 3
Treatment is offered based on the nutritional and clinical needs of the child, with the majority of children receiving treatment at home using ready-to-use foods. Complicated SAM treatments are undergoing in the stabilization centers (SC). CMAM consists of 4 components: stabilization care for acute malnutrition with complications, outpatient therapeutic care for SAM without complications, supplementary feeding for moderate acute malnutrition, and community mobilization.
It is an evidence-based model currently implemented in more than 70 countries worldwide and is the globally endorsed standard for the management of acute malnutrition. It is an appropriate model to address acute malnutrition, both in the development and humanitarian context. 4
Timely diagnosis of cases, delivering effective treatment, and building local capacity (health system and community) in the identification and management of acute malnutrition 5 are the main objectives of CMAM. 5 Over the past 50 years, the case fatality rates for SAM treated in health facilities in most developmental settings have largely remained unchanged at 20% to 30% for marasmus and up to 50% to 60% for kwashiorkor. By contrast, for the past 30 years, management protocols implemented in specialist units have achieved case fatality rates on the order of 1% to 5%.
Community therapeutic care is based upon the fundamental principle that all people whose lives are at risk from malnutrition should receive appropriate care and assistance. 6 The provision of care should be impartial, targeted only based on need. It should be delivered without discriminating between or within affected populations and should not favor any particular side in conflicts or disputes. In practice, this principle translates into a commitment and obligation to provide the largest possible proportion of the acutely malnourished population with access to appropriate care in a timely fashion for as long as necessary. The core operating principles are thus the following: Although inpatient SAM management was successful in terms of the recovery of treated children, it failed to tackle SAM at the community level hence the service is provided at the facility level not at the community. 7
The response to nutritional emergencies requires a high workload and infrastructure. This was especially the case in open situations amongst dispersed communities living in chronic poverty where specialized inpatient feeding centers were not accessible. In their absence, children need to be referred to overcrowded pediatric or general wards ill-equipped to give adequate care to malnourished children. The community-based approach is based upon proactive engagement with communities combined with a simple outpatient treatment model. Early presentation to the service will result from no admission into hospitals or clinics. The decision-making relied upon key individuals of the family and the community. This makes them understand and appreciate the care provided, early presentation and case finding increased dramatically. This model is easily implemented and resourced even in impoverished environments. 7 The timely detection and improved access to standardized treatment reduced the case fatality rate to less than 5%. 8 According to the World Health Organization (WHO) and the Ethiopia national guideline, children who have passed an appetite test and are clinically well will be treated through the outpatient therapeutic program (OTP). 9
The acceptable level of recovery from SAM is about 75% and above. The minimum weight gain is about 8 g/kg/day and above. The Antibiotic intake, vitamin A intake, admission WHZ (weight-for-height Z-score) and deworming status were some of the predictors of time to recovery. 10 Despite some studies conducted at different parts of the country,11-16 there is no adequate information regarding time to recovery and its predictors from uncomplicated SAM. This study incorporated many additional variables that were not studied in other studies. Additionally, no study had conducted in the study area. This study will be a source of information for the readers, researchers and CMAM service provider.
Material and Methods
Study design, setting, and period
A health post-based prospective cohort study had performed from November 20/2020 to February 20/2021 in the 4 districts of the north Shewa zone including; Dera, Abichu, Jida, and Kuyu districts. This zone has 13 woredas and 1 urban administration. Fiche town is the capital city of the Zone. It is located 112 km far from Addis Ababa in the Northwest direction. This zone has a total of 5 hospitals, 64 health centers, and 268 health posts. It has 1 690 403 population from these 274 690 (16.25%) are under 5 years, and 247 689 children are 6 to 59 months/North Shewa Zonal Health Department 2020.
Study participants and sampling procedures
All 6 to 59 months children in the north Shewa zone who have uncomplicated SAM were the source population. While 6 to 59 months children who fulfilled the inclusion criteria were the study participants. Through multi-stage sampling, from 13 woredas, 4 were selected using simple random sampling techniques as shown in Figure 1. Through a simple random sampling technique, a total of 30 health posts from 89 had selected. The sample size was determined using both single and double population proportion formulas. A total sample size of 423 children was determined using a log-rank test by medcalc© setup 32 programs as shown in Table 1. The sampling uses the assumption of 95% confidence level, 80% power, 1.5 adjusted hazard ratios to be detected as significant (equivalence of medium effect size) for the time-to-recovery outcome variable, 13 1.5 as the design effect, and 5% compensation for possible non-response.

Schematic presentation of sampling procedure of time to recover and determinants of recovery among 6 to 59 months children enrolled at the outpatient therapeutic feeding Program in north Shewa zone, Oromia region, Ethiopia 2020/2021.
Sample size determination using log-rank test for the study participants, north Shewa, 2021.

Abbreviation: AHR, adjusted hazard ratio.
Data collection methods and instruments
A structured pre-validated interviewer-administered questionnaire was developed in English. It was also translated to the local Affan Oromo language and re-translated back to the English version to check the consistency. The data were collected by 4 diploma nurses. The anthropometric measurements and physical examination had used to collect data from study children. Initially, MUAC measurement for every child from the left mid-upper arm was taken using a MUAC tape meter and recorded to the nearest 0.1 mm. Weight was measured using a calibrated 25 kg hanging spring BMI balance to the nearest 0.1 kg for children below the age of 2 years weekly. For children older than 2 years, a calibrated SECA balance was used and recorded to the nearest 0.1 kg. The height and length were measured using the wooden measuring board and UNICEF provided stadiometer. For the children younger than 2 years, the length measuring board was placed on the ground and read to the nearest 0.1 cm in the recumbent position. On the other hand, a child older than 2 years height was measured using a measuring stadiometer with the head’s Frankfurt position and reads to the nearest 0.1 cm. Any medical complications and development of bilateral pitting edema were screened at admission and recorded during a follow-up on a standard individual treatment card. The appetite test had done in a separate quiet room. Cases that passed the appetite test were recruited for the study and continued weekly. Children who failed the appetite test in any visit had transferred to inpatient care. At admission, the data collectors assessed the condition of every child using the OTP cards. Every participant recruited in the OTP had visited their health posts weekly to receive the diet given by HEW and a medical assessment performed by data collectors. During the weekly visit, every child was examined and given a weekly RUTF based on the Ethiopian CMAM guideline. 17
Variables of the study
The dependent variable was time to recovery. The independent variables were; socio-demographic characteristics (mothers age, educational status, age of the child, sex of the child, and household food security status); Child healthcare-related factors (type of malnutrition at admission, comorbidity, admission weight, antibiotic intake status, vitamin A intake status, vaccination status, The quantity of RUTF dispatched, deworming status, and folic acid intake status), other factors (distance between residence and health post, children food preparation way, and water treatment status), and the health extension worker-related factors (age of HEW, service year, educational status, nutrition-related training status, monthly supportive supervision, support from none governmental organization (NGO), and integrated community cases management (ICCM) guideline utilization status).
Measurements and study variables
Data quality control
Three days of training had given for both the data collectors and supervisor. The questionnaires were prepared initially in the English version and translated to the Amharic version and then back to the English version for consistency. The pre-test had done on 5% of the sample in the other district before the actual data collection. The completeness of data, and inappropriate data filling was checked daily by supervisor and principal investigator. Epi data manager version 4.6.0.4 had used for data entry.
Data processing and analysis
STATA version 16 was used for the analysis. The descriptive statistics, percentage, and median are used to describe the categorical and continuous variables orderly. Proportional Hazard Assumption (PHA) was checked both graphically and using Schoenfeld residual tests. Cox regression model had computed for both bi-variable and multivariate analysis, and finally, results had taken as significant at a 5% level of significance. Adjusted hazard ratio (AHR) with its respective 95% confidence interval (CI) had been reported to show the strength of association.
Result
Socio-demographic characteristics
A total of 423 study subjects had registered for this study with a response rate of 100%. Among 423 study participants, 345 (81.6%), 183 (43.2%) of children were below 24 and 12 months, respectively. The female-to-male ratio was 1 to 1.2. The median age of the mother/caretaker and the children were 35 (IQR 11) years and 14 (IQR 8) months respectively. More than half of the mothers/caretakers (59.1%) did not read and write in their educational status. Most households (239, 56.5%) were food secured in their food security status (FSS) as shown in Table 2.
Socio-demographic characteristics of the study participants in North Shewa Zone, Oromia, Ethiopia 2021.

Health extension worker related factors
The mean age of the HEW in the study area was 29.8 (±3.7 SD) with a minimum age of 20 years and a maximum age of 38 years. More than half, (269, 63.6%) of them were level 4 (10+4) diplomas, and the rest (154, 36.4%) were level 3 (10+3) in their educational status. Regarding nutrition training, about (321, 75.9%) of HEW took the training. Around 76% of the HEW got supportive supervision with feedback from the woredas health office, and 38% of health posts had supported by NGOs as shown in Table 3.
The HEW related factors of the study participants in North Shewa Zone, Oromia Ethiopia June 2021.

Abbreviations: HEW, health extension worker; ICCM, integrated community cases management.
Child healthcare-related factors
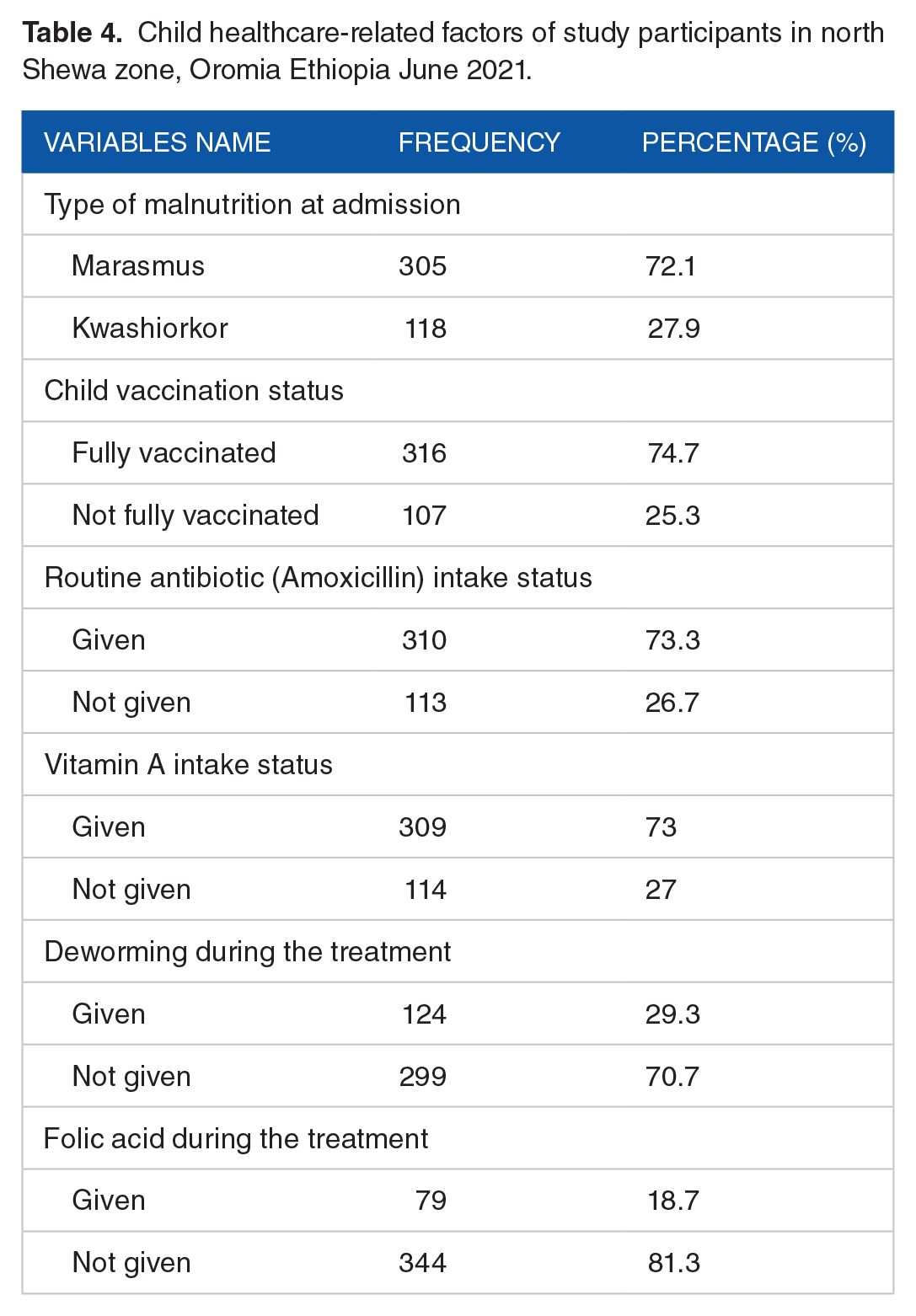
The majority of children (305, 72.1%) were marasmic type malnutrition at admission, and the rest were kwashiorkor. About (310, 73.3%) children had taken routine antibiotics (amoxicillin) during the treatment period, and (309, 73%) children had taken vitamin A. Most of the children (316, 74.7%) had fully vaccinated as shown in Table 4.
Child healthcare-related factors of study participants in north Shewa zone, Oromia Ethiopia June 2021.
Other factors
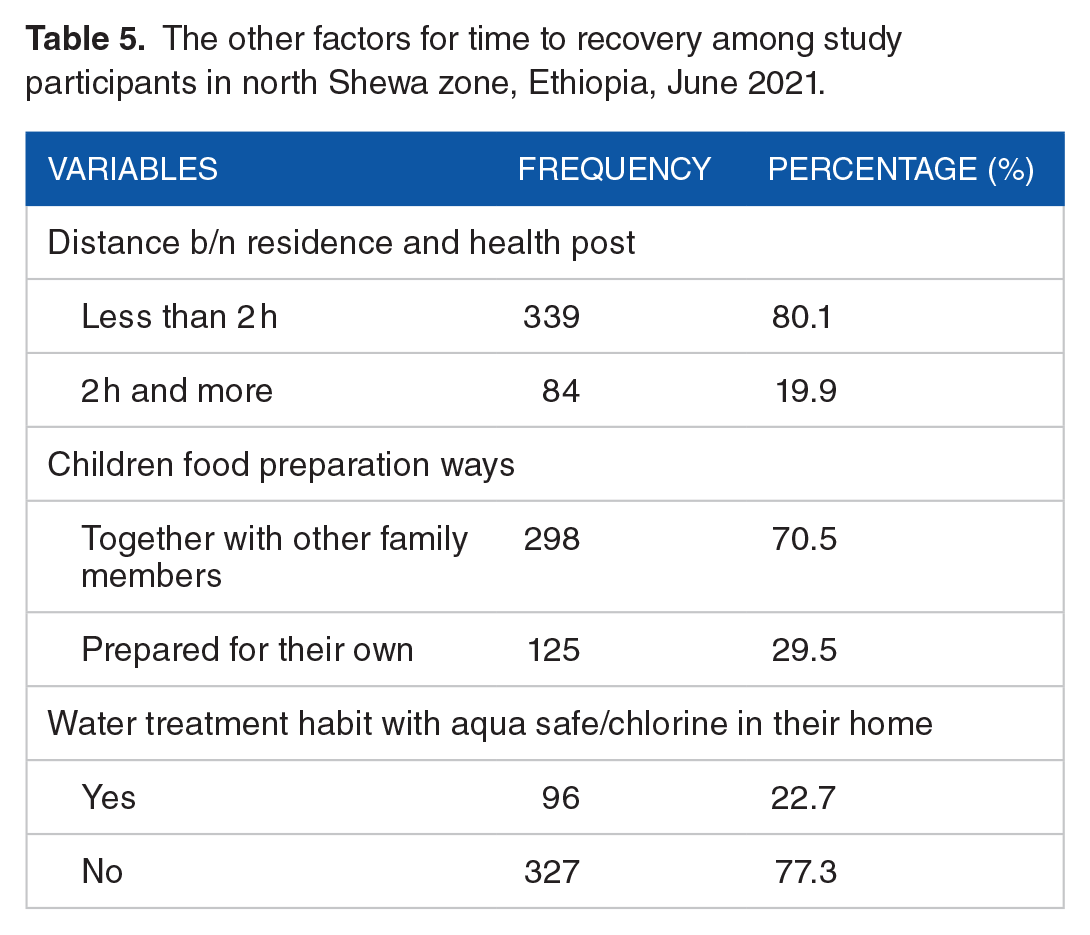
The mother/caretaker who traveled less than 2 hours to receive OTP were 339 (80.1%) as shown in Table 5.
The other factors for time to recovery among study participants in north Shewa zone, Ethiopia, June 2021.
The time-to-recovery and treatment outcomes of children with uncomplicated SAM
From the total recruited subjects, 327 (77.3%, 95% CI: 73.1-81.1) were successfully recovered, and hence they developed the event of interest. On the contrary, 22.7% of children have not developed the event. The reason for failure, 42 (9.9%), 33 (7.8%), 18 (4.3%), and 3 (0.7%), was none responder, defaulter, medical transfer, and transfer out respectively.
The mean weight gain of the recovered children was 5.7 g/kg/day. The median time to recovery was 42 (IQR 14) days (6 weeks) as determined by the Kaplan-Meier survival estimate as shown in Figure 2.

Kaplan-Meier survival estimate of the enrolled children in the OTP program in north Shewa zone, Oromia Ethiopia June 2021.
Determinants of time to recovery from uncomplicated SAM enrolled children in the OTP
Among the socio-demographic factors, household food security was identified as a predictor for time to recovery among children with SAM. As a result, cases from mild food insecure recovered 6.5 times faster than cases from severe food-insecure households (HHs) (AHR = 6.5; 95% CI: 3.1-13.8); whereas, cases from moderate food insecure HHs recover at a rate of 2.5 times faster than cases from severe food insecure HHs (AHR = 2.5; 95% CI: 1.2-5.3). The rate of time to recover among children from food secure HHs was 9.6 times faster than cases of severe food insecure HHs (AHR = 9.60; 95% CI: 8.1-18.5). Children whose residence was at less than 2 hours walking distance from the nearby health post recovered 2.6 times faster than those who lived at a distance taking 2 hours or more walking distance (AHR = 2.6; 95% CI: 1.8-18.7). Taking the correct dose of RUTF enabled the recovery time to be 1.6 times faster than those who did not take the appropriate one (AHR = 1.6; 95% CI: 1.1-2.3). The rate of time to recovery among children who had weekly weight measurements was 50% faster than those who were not measured (AHR = 1.5; 95% CI: 1.1-2.0). Having SAM management service by HEWs who had nutritional-related training enabled the recovery time of cases to be 2 times faster (AHR = 2.1; 95% CI: 1.0-4.5) as shown in Table 6.
Outputs of the Cox-proportional hazard model analyses on the predictors of time-to-recovery from severe acute malnutrition in north Shewa zone, Oromia Ethiopia June 2021.

Abbreviations: AHR, adjusted hazard ratio; CHR, crude hazard ratio; HEW, health extension worker; ICCM, integrated community cases management; MUAC, mid-upper arm circumference; NGO, none governmental organization; RUTF, ready to use therapeutic food.
Discussion
The median time to recover from this study was 42 (IQR 14) days (6 weeks) as determined by the Kaplan-Meier survival estimate. The significant predictors of the time to recovery were household food insecurity status, the distance between home and health posts, the correct dose of RUTF, weekly weight measurement of the children per protocol, and health extension workers’ nutrition-related training status. The recovery rate reported in this study (77.3%) was in line with the minimum 75% threshold set by the SPHERE standard, 10 the facility-based prospective cohort study done at Shebedino, southern Ethiopia that was 79.6% 11 and the study done at Zambia that was 80%. 20 However, this was lower than a prospective cohort study done in the Afar region that was 83.2%. 12 This deviation may be due to the nutrition training status difference of the HEW and treatment adherence status of the child. On the other hand; it was higher than the prospective cohort study done at north Gondar that was 65.3%, 13 a study done at India that was 33.6%, 21 a retrospective cohort study done at Gubalafto district that was 65%, 22 and a retrospective study done at Accra, Ghana that was 34.5%. 23 The variation may be due to the differences in study period, HEW educational status, and distance between home and nearby health post. It was also higher than the retrospective cohort study done in Tigray that was 61.8% 14 Kamba district, southwest Ethiopia that was 67.7%, 15 and the retrospective cross-sectional study conducted in Wolaita that was 64.9%. 16 The variations could be attributed to differences in educational status of the HEW and cultural practices in different geographical locations within the same country.
The mean rate of weight gain for this study was 5.98 g/kg/day with 95% CI 5.61 to 6.36. That was almost in line with the expected mean weight gain as determined by the SPHERE standard that recommends mean weight gain should be from 6 to 8 g/kg/day. 10 This finding was higher than the study done at Shebedino, southern Ethiopia that was 5.4 g/kg/day, 11 a retrospective study done at Tigray that was 5.23 g/kg/day, 14 and a retrospective cross-sectional study done at Wolaita that was 4.29 g/kg/day. 16 The reason behind this may be the difference in treatment adherence across different geographical locations within the same country and HEW’s educational status. The median time to recovery of this study was 42 (IQR 14) days (6 weeks). That was within the acceptable range of the Ethiopian protocol for the management of uncomplicated SAM in the OTP that allows the children can stay up to 8 weeks on the treatment, 18 in line with the prospective study done at north Gondar that was 38.5 ± IQR of 14 days 13 and a study done in India that was 51 days with IQR of 5.6 days. 21 However, the recovery time in this study was a little longer day than the international standard that recommends below 6 weeks, 10 and the study at Shebedino, Ethiopia that was 36 days. 11 These may be due to none- adherence of the health extension workers to the management protocol. However, this was shorter days than the prospective cohort study at the Afar region that was 44.15 (±8.77) days, 12 the retrospective study done in Kamba district southwest Ethiopia that was 7.14 weeks IQR 5.28 to 8.1, 15 the retrospective cross-sectional study done at Wolaita that was 6.8 weeks 16 and a retrospective study was conducted at Zambia that was 24 weeks 20 respectively. The variations could be attributed to differences in the treatment adherence and treatment protocol utilization in different geographical locations within the same country. From socio-demographic factors household, food security status was the predictor of time to recovery. Cases from food secured HHs (AHR = 9.6), mild food insecure (AHR = 6.5), and moderate food insecure (AHR = 2.5) recovered faster than cases from severe food insecure HHs. This finding had supported by the result at Shebedino, southern Ethiopia. 11 The distance between the residence and the health post had significantly associated with the time to recovery. Those cases who traveled less than 2 hours were 2.6 times recover faster than their counterparts. This finding was in line with the study conducted in the Afar region. 12 Taking the correct dose of RUTF enabled the recovery time to be faster than those who didn’t. The children that had in the OTP program should get the correct caloric dose to respond faster. The rate of time to recovery among children who weekly measured their weight was 50% faster than those who didn’t. It may improve the monitoring of cases and intervene on the finding early. The other factor had significantly associated with the time to recovery was health extension workers’ nutrition-related training status. Those who had nutrition-related training were 2 times improved time to recover than those who did not take the training. Giving updated nutrition-related training for the health extension workers can improve the quality of treatment and adherence to the management guideline. The type of malnutrition at admission, the age of the children, Amoxicillin intake, vitamin A supplementation, and deworming were not the predictors in this study. Those were predictors in other studies for the time to recovery. 13 The discrepancy may be due to adherence to the treatment, shortage of supplies, and inadequate management quality of health extension workers as indicated by the protocol, study area, and study period difference.
Conclusion
The median time to response (recovery) of this study was 42 (IQR 14) days (6 weeks) as determined by the Kaplan-Meier survival estimate that was within the acceptable range of the Ethiopian protocol for the management of uncomplicated SAM in the OTP. The significant predictors of the time to recovery were household food insecurity status, the distance between home and health posts, the correct dose of RUTF, weekly weight measurement of the children per protocol, and health extension workers’ nutrition-related training status. It is advisable to improve the household food security status and the health extension worker’s nutrition-related training status.
Footnotes
Acknowledgements
First, we would like to say thanks more to North Shewa zonal health department staff for their provision of valuable information. Secondly, we want to extend our thanks to Salale University’s department of Public Health for giving us the chance to conduct research. Lastly, we would like to extend our deep gratitude to study Woredas health offices, health centers, and health posts staff members for their friendly support.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study had funded by Salale University for the data collection, supervision, and analysis.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization: AB. Formal analysis: AB, DS, and AWT. Development or design of methodology: AM, DS, and AWT. Entering data into software: AB and AW. Supervision: AB, DS, and AWT. Validation: AB, DS, AWT, BA, YH, and BT writing original draft: AB, DS, AWT, BA, YH, and BT. Writing review and editing: AB, DS, AWT, BA, YH, and BT. All authors read and approved the final manuscript.
Ethics Approval and Consent to Participate
The study approval had obtained from the institutional ethical review Committee of Salale University with the reference number [SU/210/20/13]. An official letter of cooperation had written from the selected districts, and each respective health office gave a permission letter. Oral consent had taken from every mother before the interview started after explaining the objective of the study. The study participants did not get any incentives as compensation. The confidentiality of the respondent had kept by avoiding the name and household numbers of the respondents. The questionnaire had also kept in a secured locked cabinet and the database with a secured strong password.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.