
Abstract
Background:
Globally, acute malnutrition threatens the lives of several million children under 5 years of age. Malnutrition affects the social, economic, and medical aspects of all countries. In Ethiopia, acute malnutrition is not decreasing at the intended rate for unclear reasons.
Objective:
This study aimed to assess the burden of acute malnutrition and its associated factors among children under 5 years of age in a rural setting of southern Ethiopia.
Methods:
A community-based cross-sectional study was conducted from January to March 2022. A multistage sampling technique was used to select 421 children. Mothers/caretakers were interviewed using interviewer-administered questionnaire, while their children’s height/length and weight were measured. Logistic regression analyses were used and presented as the crude odds ratio (COR) and adjusted odds ratio (AOR) with their 95% confidence intervals (CI).
Results:
The burden of acute malnutrition among children under 5 years of age in the study area was 22.6% (95% CI = 18.5-26.8). Fathers with primary education (AOR = 4.48; 95% CI = 1.93-10.39), households with improper solid waste disposal (AOR = 2.54; 95% CI = 1.11-5.82), not usually sleeping under insecticide-treated bed net (ITN) (AOR = 1.79; 95% CI = 1.01-3.19), unacceptable children dietary diversity score (DDS) (AOR = 2.56; 95% CI = 1.28-5.14), and unacceptable household DDS (AOR = 2.26; 95% CI = 1.02-5.00) were factors associated with acute malnutrition.
Conclusions:
The prevalence of acute malnutrition among children was critically high. Upgrading paternal educational status, encouraging safe solid waste disposal, ensuring consistent use of ITN, and improving both child and household DDS should be stressed.
Plain language title
Very High Level of Acute Malnutrition and Related Factors Among Children Under 5 Years in the Rural Parts of Southern Ethiopia
Plain language summary
Why was the study done?
Acute malnutrition is a cause of death for several million children under 5 years of age in the world. It affects the social, economic, and medical features of all countries. In Ethiopia, acute malnutrition is not decreasing at the intended rate for unclear reasons. Numerous studies in the country reported varying level on acute malnutrition in spite of similarities in the study area and time. Therefore, this study aimed to find out the level of acute malnutrition and related factors among children under 5 years of age in rural parts of southern Ethiopia.
What did the researchers do?
The research team selected 421 representative children and collected information by asking their mothers/caretakers some relevant questions, and by weighing and measuring their height. Then, the collected information was computed by a computer software.
What did the researchers find?
One out of 5 children in the rural parts of southern Ethiopia had acute malnutrition. Educational status of fathers, households with inappropriate solid waste, not usually sleeping under mosquito bed net, low level of children and household food variety were factors related to acute malnutrition.
What do the findings mean?
The level of acute malnutrition among children in the study area was very high. Educating fathers, encouraging safe solid waste disposal, ensuring consistent use of mosquito bed net, and improving both the level of children and household food variety should be underlined.
Introduction
The term malnutrition refers to all forms of poor nutrition, including undernutrition, micronutrient deficiencies, overweight, and obesity, as well as the resulting diet-related noncommunicable diseases. 1,2 World Health Organization (WHO) defines acute malnutrition, also known as wasting, as a recent and severe weight loss due to lack of enough food to eat and/or because of an infectious disease, such as diarrhea. 2 Acute malnutrition usually occurs in children due to insufficient food intake or infectious diseases. 3
Every country is facing a serious public health challenge from the developmental, economic, social, and medical impacts of malnutrition. 4 Globally, approximately 45% of deaths among children under 5 years of age are linked to undernutrition, which mostly occurs in low- and middle-income countries. 2 Children who are undernourished have lowered resistance to infection and are more likely to have functional impairment and die from different infectious diseases. 2,5 The economic consequences represent losses of 11% of gross domestic product every year in Africa and Asia. 4
In 2020, 45.4 million (6.7%) children under 5 years of age worldwide were affected by acute malnutrition, two-thirds and one-quarter of whom were affected by Asia and Africa, respectively. 6 According to the Ethiopia Mini Demographic and Health Survey in 2019, 7.2% of children in Ethiopia were wasted. 7
The world’s countries have agreed to end all forms of malnutrition by 2030, but despite some progress in recent years, they are off track to reach those targets. 4 Despite the government of Ethiopia joining the global campaign to end malnutrition by 2030 and decreasing the acute malnutrition rate, the prevalence of acute malnutrition is still higher than the national rate in some parts of Ethiopia and remains a public health problem in the country. 7 -9
The most recent conceptual framework on malnutrition from the United Nations Children’s Fund has broadly outlined the factors influencing malnutrition, categorizing them into immediate determinants (diets and care), underlying determinants (food, practices, and services), and enabling determinants (governance, resources, and norms). 10 A substantial number of studies have identified different factors associated with acute malnutrition among children. For instance, a study performed in Afghanistan identified the education level of household heads, income, age of children, and history of children with diarrhea in the last 2 weeks as determinants of acute malnutrition. 11 Nonaccess to health services was associated with acute malnutrition in Iran. 12 Different studies in Ethiopia determined that the age of the child, fever 2 weeks before the survey, socioeconomic status, family size, and paternal control over resources were among the factors associated with acute malnutrition. 13 -15 Another study conducted in Ethiopia by Tekile et al reported that wasting is associated with maternal education and safety of water facility. 16
The 2019 Ethiopia Mini Demographic and Health Survey was hardly able to identify factors associated with acute malnutrition. 7 Moreover, various studies in the country reported inconsistent findings on acute malnutrition in spite of temporal and spatial similarities. 8,13,15 Therefore, this study aimed to determine the burden of acute malnutrition and its associated factors among children under 5 years of age in the study area.
Methods
Study Area
The study was conducted in Bakadawula Ari district, which is located 745 km south of Addis Ababa, the capital city of Ethiopia. Found in Southern Ethiopia, the district is a rural setting inhabited mainly by agrarian farmers. In 2021, the district had a total population of 47 749, comprising 7454 children aged 6 to 59 months. The district has 9 kebeles (the smallest administrative units in Ethiopia). There are 2 health centers and 5 private clinics in the district.
Study Design and Period
A community-based cross-sectional study was conducted from January 2022 to March 2022.
Study and Source Population
The source population for this study was all children aged 6 to 59 months living in Bakadawula Ari district, whereas the study population was all selected children aged 6 to 59 months living in Bakadawula Ari district.
Eligibility and Exclusion Criteria
All children aged 6 to 59 months who were permanent residents in Bakadawula Air district were eligible. Children aged 6 to 59 months who had deformity (a structural abnormality or deviation from the normal form or shape of a body part, organ, or system) and critical sickness (severe and potentially life-threatening medical conditions that require immediate and intensive medical intervention for stabilization and recovery) were excluded from the study.
Sample Size Calculation
The sample size for this study was determined using a single population proportion formula:
Hence, assuming a 95% confidence level (z = 1.96), a 5% margin of error (w), and a 21.2% acute malnutrition prevalence (p) from another study in Ethiopia, 9 the formula yielded a sample size (n) of 255. Since the study employed a multistage sampling method, a design effect of 1.5 was assumed, and the sample size became 383. After adding 10% for the nonresponse rate, the final sample size was 421.
Sampling Procedure
A multistage sampling method, with 2 sampling stages, was used. The first 3 kebeles were selected by a simple random sampling technique from all kebeles in the district. Then, the sample size was allocated proportionally to each kebele based on the total number of 6- to 59-month-old children. Eventually, using a sampling frame prepared by health extension workers, a lottery technique was applied to select study participants from each kebele. For households with more than one eligible child, one of the children was selected randomly.
Data Collection Instruments and Procedures
A structured interviewer-administered questionnaire, adapted from available literature, was used. 17,18 The questionnaire was composed of questions about sociodemographic factors, health, dietary intake, and environmental factors, and it was first prepared in the English language and translated into the Amharic language and then back to English by 2 fluent speakers to check the consistency. The data were collected by interviewing the mother/caretakers, while anthropometric measurements were taken by weighing and measuring the height/length of the children. Children were weighed without clothes and shoes using a Seca 874 (Seca, Germany) digital weighing scale. Weight was taken to the nearest 0.1 kg. Height/length was measured after taking off shoes and caps via a portable wooden height/length measuring board by ensuring that the head, shoulders, buttocks, knees, and heels of the child touched the measuring board. Length while lying down was measured for children younger than 24 months, whereas older children’s height was measured while standing. Height/length was measured to the nearest 0.1 cm.
Study Variables
Dependent variable
Prevalence of acute malnutrition among children under 5 (either wasted or not wasted).
Independent variables
Child’s sex, average family size, educational status of parents, sex of household, head, wealth index, household waste disposal practice, hand washing practice, fever in the last 2 weeks, diarrhea in the last 2 weeks, taking the child to health facility during sickness, sleeping under insecticide-treated bed net (ITN), child’s age at complementary food introduction, child’s meal frequency per day, child’s dietary diversity score (DDS), and household’s DDS.
Operational Definitions
Acute malnutrition
The percentage of children suffering from moderate or severe acute malnutrition (below −2 standard deviations from the median weight-for-height [WFH] of the reference population). 19
Children’s DDS
This is calculated from the number of food items consumed 24 hours prior to the survey date (24 hours recall was used) by the children from the following 8 recommended food groups: grain, roots, or tubers; vitamin A rich fruits and vegetables; other fruits and vegetables; meat, poultry, fish, sea foods; eggs; legumes and nuts; breast milk; and dairy products. Hence, a child with 5 or more DDS has acceptable DDS. 20
Household DDS
This is computed by summing up the number of food items consumed 24 hours prior to the survey date by the household from the following 12 recommended food groups: cereals; roots and tubers; vegetables; fruits; meat, poultry, offal; eggs; fish and seafood; pulses, legumes, nuts; milk and milk products; oils/fats; sugar/honey; and miscellaneous. Consequently, a household with 5 or more DDS has acceptable DDS. 20
Quality Assurance
All data collectors and supervisors were given 2 days of training on the study objectives, ethical considerations, ways to approach the study participant, and methods of taking anthropometric measurements. Having a pretested questionnaire among children (5% of the sample size) in the surrounding kebele, an appropriate change was made to the questionnaire. The weight scale was monitored for its accuracy using an object with known weight. The investigators and supervisors checked the completeness of each questionnaire daily. Two data clerks entered the data, and consistency was cross-checked by comparing the 2 separately entered data.
Data Processing and Analysis
The data were entered into and analyzed by SPSS v26 after coding and cleaning. The anthropometric index (WFH) was calculated using ENA for SMART (Emergency Nutrition Assessment for Standardized Monitoring and Assessment of Relief and Transitions) 2020 software. The wealth status of each household was assessed using the WHO recommended wealth index construction method by principal component analysis, and the wealth status was divided into 5 quintiles: first (lowest), third (second lowest), third (middle), fourth (second highest), and fifth (highest). 21 Frequencies, summary measures, and tables were used to present the characteristics of the participants.
The outcome variable was recoded to dichotomous outcomes: either they are wasted or not. Children who were wasted (WFH <−2 standard deviation) were coded as 1, whereas those who were not wasted (WFH >−2 standard deviation) were coded as 0. The independent variables were coded based on previous related studies. All covariates with a P value < 0.25 in bivariate logistic regression analysis were considered for further multivariate analysis. Covariates with P values < .05 during multivariate logistic regression analysis were considered significantly associated with acute malnutrition. The logistic regression analysis results were expressed by crude odds ratio (COR) and adjusted odds ratio (AOR) with their respective 95% confidence intervals (CIs). The data were explored by SPSS v26, and the normality of the data distribution was checked. Multivariable logistic regression analysis was run to control for confounding factors. Finally, the fitness of the model was tested by Hosmer-Lemeshow’s goodness of fit test.
Ethical Considerations
Ethical approval letters were received from the Jinka University Research Ethics Review Committee (reference number: JKU/RCE/ERC/001/14). Confidentiality was assured, and mother/caretakers signed an informed consent form.
Results
Sociodemographic Characteristics
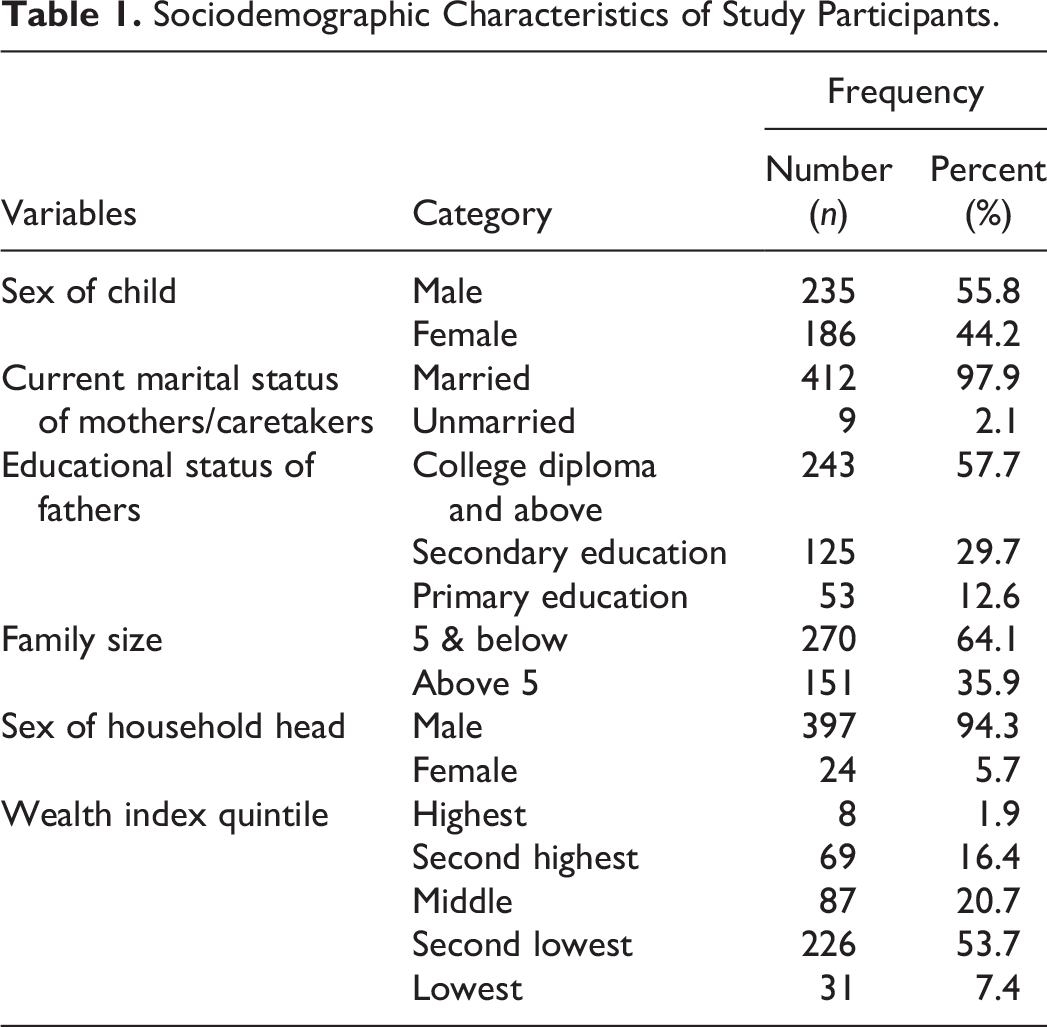
Four hundred twenty-one children aged 6 to 59 months participated. The average age of the children was 22.94 months, with a standard deviation of 14.28 months. The average age of the mother/caretakers of the children was 27.69 years, with a standard deviation of 4.83 years. Regarding educational status, 246 (58.4%) of mothers/caretakers of the children had no formal education (Table 1).
Sociodemographic Characteristics of Study Participants.
Hygiene and Health-Related Results
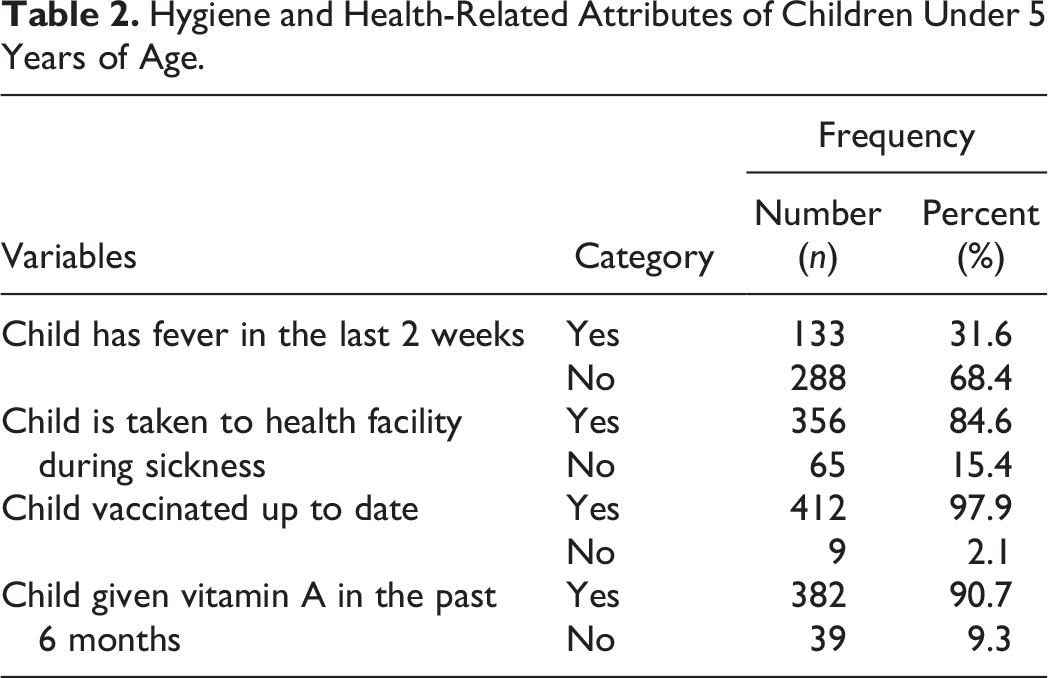
Four-fifths (83.6%) of the mothers/caretakers of the children in the study were washing hands before feeding the child; however, three-fourths (73.6%) of them were disposing solid waste improperly. Of all children, almost one-third (33.7%) had diarrhea 2 weeks prior to the study. More than half (57.2%) of the children were sleeping under ITN (Table 2).
Hygiene and Health-Related Attributes of Children Under 5 Years of Age.
Feeding Practice and Dietary Diversity
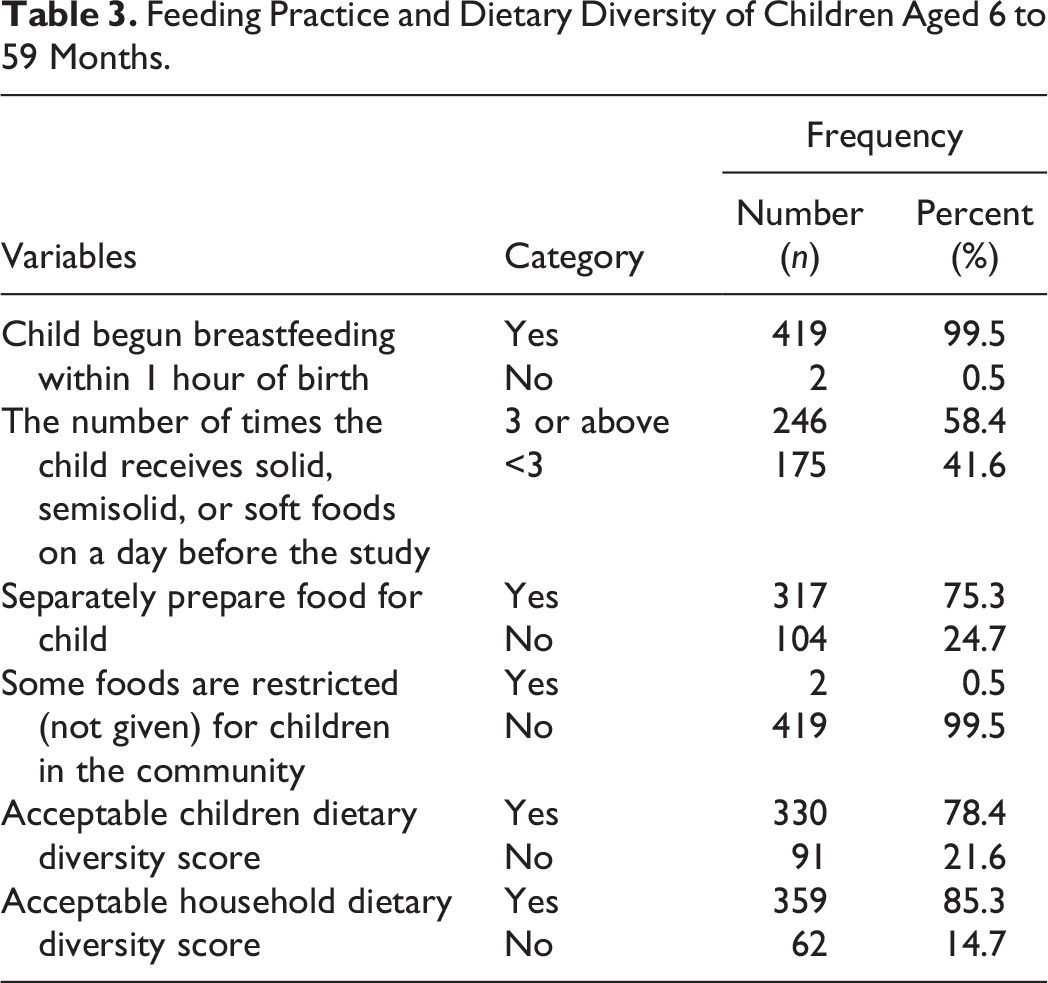
Most (95.2%) of the children were exclusively breastfed up to 6 months of age, while 373 (88.6%) of them began complementary feeding at 6 months. Three hundred and thirty (78.4%) children had acceptable child DDS. Meanwhile, 359 (85.3%) households had acceptable household DDS (Table 3).
Feeding Practice and Dietary Diversity of Children Aged 6 to 59 Months.
Burden of Acute Malnutrition Among Children
The burden of acute malnutrition among the children was 22.6% (95% CI: 18.5-26.8). The overall magnitude of severe acute malnutrition was 14.8%, whereas the prevalence of moderate acute malnutrition was 7.8%. Girls (11.9%) suffered slightly more from acute malnutrition than boys (10.8%). The prevalence of acute malnutrition among children aged 6 to 23 months (26.4%) was greater than the rate among children aged 24 to 59 months (18.7%). Unlike age of children, sex of children was significantly associated with prevalence of acute malnutrition during bivariate analysis.
Factors Associated With Acute Malnutrition
The bivariate logistic regression showed that the following 15 variables were associated, at a P value < .25, with acute malnutrition among the children: sex of a child, educational status of father, family size, sex of household head, wealth index, solid waste disposal practice, hand washing, child’s diarrheal history, child’s fever history, taking child to health facility during sickness, use of ITN, beginning of complementary feeding at 6 months, the number of times a child received complementary foods a day before the study, acceptable children DDS, and acceptable household DDS. All aforementioned variables did not show any multicollinearity and were candidates for multivariate analysis. Upon multivariate logistic regression, the following 5 covariates were found to be factors associated with acute malnutrition: primary educational status of fathers, improper solid waste disposal, not usually using ITN, unacceptable child DDS, and unacceptable household DDS (Table 4).
Factors Associated With Acute Malnutrition Among Children Aged 6 to 59 Months.
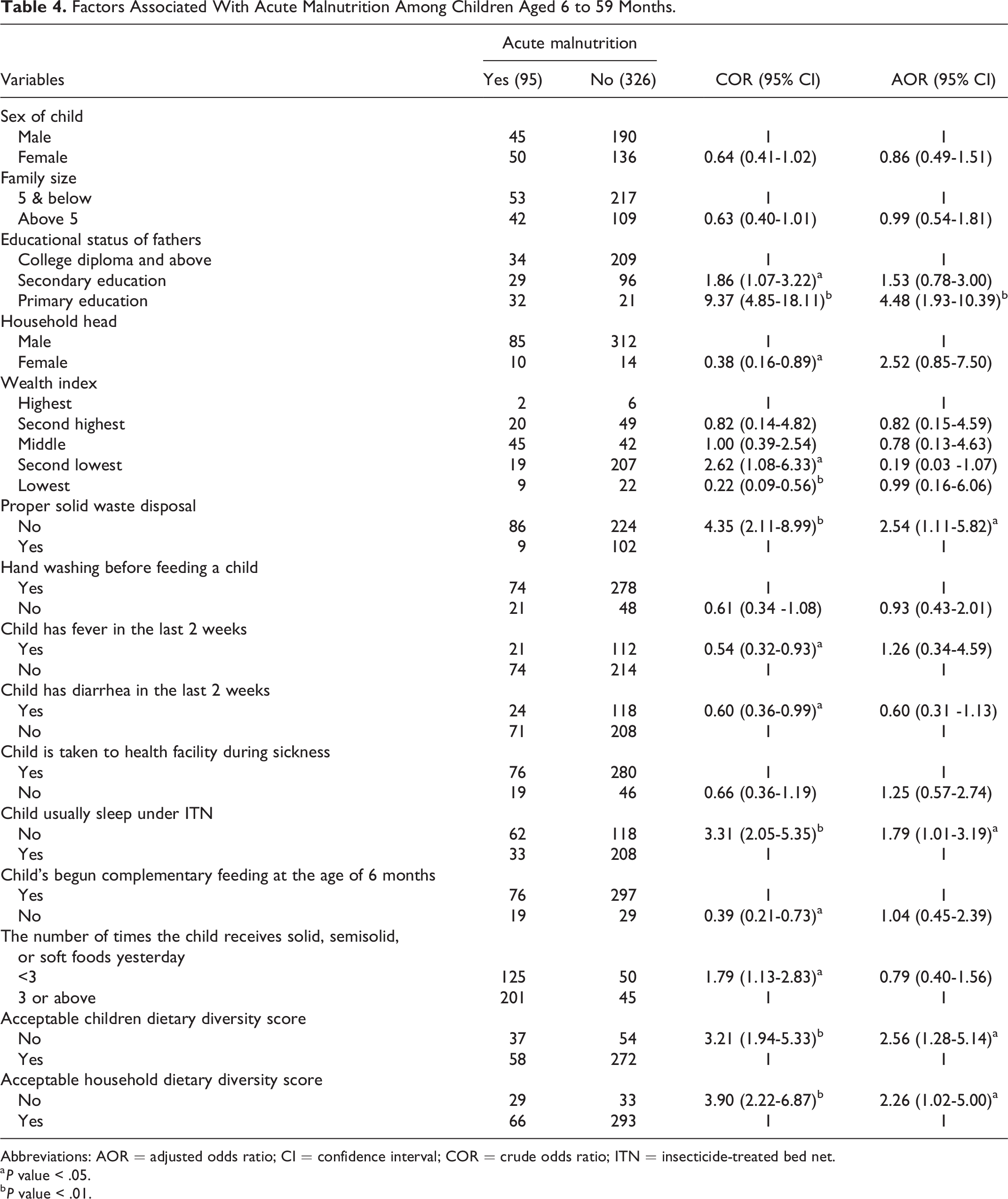
Abbreviations: AOR = adjusted odds ratio; CI = confidence interval; COR = crude odds ratio; ITN = insecticide-treated bed net.
a P value < .05.
b P value < .01.
Children born to fathers who had educational status at most primary were 4.48 times (AOR = 4.48; 95% CI = 1.93-10.39) more likely to have acute malnutrition than children whose fathers had educational status of college diploma and above. In contrast to children under 5 years of age whose household dispose solid waste properly, a counterpart had 2.54 times (AOR = 2.54; 95% CI = 1.11-5.82) increased odds of acute malnutrition. A child who had not been sleeping under ITN was 1.79 times (AOR = 1.79; 95% CI = 1.01-3.19) more likely to be wasted than a child who had been sleeping under a mosquito bed net. The odds of being wasted among children with unacceptable DDS were 2.56 times (AOR = 2.56; 95% CI = 1.28-5.14) higher than those among children with acceptable DDS. Children with unacceptable household DDS were 2.26 times (AOR = 2.26; 95% CI = 1.02-5.00) more likely to have acute malnutrition than children with acceptable household DDS.
Discussion
This study assessed the magnitude of acute malnutrition and associated factors among children aged 6 to 59 months in Bakadawula Ari district. Consequently, the study found a critically high, 22.6% (95% CI = 18.5-26.8), burden of acute malnutrition in the study area that is associated with paternal education, household solid waste disposal practices, children’s utilization of ITN, children’s DDS, and household DDS. Unlike other studies, acute malnutrition were not significantly associated with the sex of a child, 22 wealth index, 23 duration of child breast feeding, 24 and diarrhea 2 weeks prior to the study. 9
In spite of high magnitude of acceptable children and household DDS in the study area, the prevalence of acute malnutrition is critically high. This might be due to the fact that acute malnutrition can be affected by various factors apart from diet, such as access to health care, water and sanitation, economic conditions, cultural practices, and the overall health environment could affect the prevalence of acute malnutrition. 10 Interventions to combat malnutrition should be multifaceted and address the complex interplay of these factors.
Although the prevalence of acute malnutrition was critically high in this study, 3 it was in line with studies performed in Gursum, which was 21.2%, 9 and in the Tierkedi South Sudanese refugee camp, which was 23.2%. 25 However, the current finding was much higher than that of a study conducted in Addis Ababa (4.7%). 26 The possible reasons for the discrepancy could be the setting difference where caretakers of children live; caretakers in Addis Ababa were closer to nutrition-related information, child care during illness, and easy access to the market and were economically better off than the current study participants. The recent Ethiopian Mini Health and Demographic Survey revealed that 7% of children under 5 years were wasted, but the current finding was 3-fold higher. 7 This difference may be due to the national survey reporting the national average, where a higher proportion in some areas was masked by very smaller proportions in some other parts of the country. Elsewhere, studies performed in Kenya and Nigeria also revealed lower magnitudes of acute malnutrition than this study, which were 7.1% and 8.8%, respectively. 27,28 The gap may be due to a recent lack of rain and drought in the current study area, which could play a pivotal role indirectly in this critically high prevalence of acute malnutrition by decreasing the production of cereals and crops as well as affecting household livelihood security.
As per the current study, children from mothers/care givers whose partners had no primary education had higher odds of being wasted compared to children from mothers/care givers whose partner had a college diploma and above educational status. This association was supported by studies performed in Ethiopia, 12 Sudan, 29 and Bangladesh, 30 which depicted that a lower level of educational status of the caregiver’s partner or children’s father was a risk factor for acute malnutrition among children. This could be explained by the higher financial constraints and limited access to health care and resources, including nutritious food and nutrition information, faced by partners who had lower education.
This study also showed that children whose households dispose solid waste improperly were more likely to suffer from acute malnutrition than children whose households properly dispose solid waste. Poor hygiene creates room for an increase in diarrheal disease occurrence among children under 5 years of age by favoring houseflies and other disease-causing vectors that could lead to infection and then acute malnutrition. 31,32
Children who were not usually sleeping under ITN were more prone to wasting than children who were usually sleeping under ITN. Different studies have revealed that prevention of malarial infection among children by using ITN is crucial for minimizing under 5 malnutrition and mortality. 33 -35 The possible reason could be the use of ITNs reduces the incidence of malaria that can lead to a decrease in appetite, increased metabolic demands, and impaired nutrient absorption, all of which that can contribute to wasting in children.
Compared with children with acceptable DDS, the odds of being wasted among children with unacceptable DDS were more than double. This association was in the same direction as a study conducted in Karat town, 24 Kalafo district, 36 and Ghana, 37 which reported that unacceptable child DDS was a risk factor for acute malnutrition. Moreover, another study performed in Tanzania revealed that the consumption of a diverse diet was significantly associated with a reduction in acute malnutrition in children. 38 This association could be attributed to the fact that limited dietary diversity is indicative of insufficient intake of essential nutrients critical for growth and immune function, underscoring the importance of a balanced diet in childhood development.
This study found that household dietary diversity is associated with acute malnutrition among children under 5 years of age. Hence, children with unacceptable household DDS were more likely to be wasted than those with acceptable household DDS. This is perhaps due to children with better household dietary diversity having a higher probability of obtaining sufficient balanced dietary intake. A diverse diet is likely to provide a broader spectrum of essential nutrients necessary for proper growth and immune function, reducing the risk of acute malnutrition.
Regarding the limitations of the study, the cross-sectional design of the study limits the establishment of causality. The reliance on maternal recall for information such as dietary intake and health history introduces the potential for recall bias. Memory lapses or inaccuracies in reporting could impact the reliability of certain data. The study could be affected by social desirability bias as respondents may provide answers they believe are socially acceptable or expected, potentially leading to an underreporting of certain practices or conditions.
On the positive note, the study included a substantial sample size (421 children), enhancing the statistical power and reliability of the findings. The use of a multistage sampling method increases the representativeness of the sample, allowing for a more accurate reflection of the population in the Bakadawula Ari district. The study employed multivariate logistic regression analysis, adjusting for potential confounding factors, which strengthens the validity of the identified associations.
In conclusion, the study revealed a critically high burden of acute malnutrition in Bakadawula Ari district. This rate surpasses national averages and is higher than findings from other regions, indicating a pressing public health concern in the area. Consequently, it is crucial that policymakers and other concerned bodies improve both children’s and households’ dietary diversity and endorse proper solid waste disposal. It should be striven to ensure that children sleep under ITNs by making the mosquito bed net accessible and affordable. Stakeholders should also emphasize enhancing and promoting parental education. Additionally, the authors emphasize the importance of promptly screening and treating children for acute malnutrition to prevent the progression to severe acute malnutrition or the development of morbidities that may result in fatality.
Footnotes
Authors’ Note
The data for this research article are available in the Mendeley repository, DOI:10.17632/ myzxkbwtr5.1
Acknowledgments
The authors would like to thank Jinka University for financial and material support for data collection. Jinka Hospital and Bakadawula Ari district office also deserve credit for their material support. They extend their sincere gratitude to the data collectors, supervisors, and study participants.
Author Contributions
GAT and EWW participated in the conception and design of the study, supervision of data collection and management, data analysis, interpretation of the findings, and writing the final report. GAT, EWW, and MGW were involved in data management and analysis, interpretation of the findings, and writing the final report. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.