
Abstract
Background:
Undernutrition accounts for at least 50% of the annual global under-five mortality burden. Although disparities in the childhood stunting between urban and rural areas in Sierra Leone have been documented, information on factors associated with these differences is lacking. We aimed to determine rural-urban correlates of stunting among children under the age of 5 in Sierra Leone.
Methods:
We analyzed data from 2019 Sierra Leone demographic and health survey (SLDHS) focusing on under-five children. We conducted multivariable logistic regression to examine rural-urban factors associated with childhood stunting.
Results:
Prevalence of stunting was 31.6% (95% CI 29.8-33.2) in rural areas and 24.0% (95% CI 21.6-26.1) in urban areas. Within the rural areas, children of stunted mothers (aOR = 2.37; 95% CI 1.07-5.24, P < .05), younger mothers aged 15 to 19 years (aOR = 2.08; 95% CI 1.17-3.69, P < .05), uneducated mothers (aOR = 1.87; 95% CI 1.28-2.71, P < .01), as well as older children (24-59 months) (aOR = 1.83; 95% CI 1.48-2.27, P < .001), and boys (aOR = 1.37; 95% CI 1.12-1.66, P < .01) were more likely to be stunted compared to those of non-stunted, older, post-primary education mothers and those who were less than 24 months and girls respectively. While urban children whose fathers had lower education (aOR = 1.94; 95% CI 1.10-3.42, P < .05), whose mothers were more parous (para 2-4) (aOR = 1.74; 95% CI 1.03-2.95, P < .05), and boys (aOR = 1.48; 95% CI 1.06-2.08, P < .05) were more likely to be stunted compared to their counterparts with fathers that had tertiary education, mothers of low parity and girls, respectively.
Conclusions:
Stunting is more prevalent in the rural areas compared to the urban areas. Sex of the child was the only significant factor in both rural and urban areas. Our study findings suggest that programs designed to reduce stunting should aim for integrated yet context specific interventions in rural and urban areas.
Introduction
Undernutrition is a crucial health indicator for monitoring growth status and survival of children under 5 years in low and middle-income countries.1-3 Globally, undernutrition accounts for at least half of all the under-five mortality burden annually. 4 Stunting is one of the manifestation of undernutrition and a preferred anthropometric measure for the assessment of chronic nutritional status.5,6 A child is considered stunted when he/she has z-score value for height-for-age below minus 2 standard deviations (−2SD) from the median of the World Health Organization (WHO) standard growth charts. 7 Stunting is considered as “best overall indicator” of children’s well-being and an “accurate reflection” of disparities among populations. 8
Globally, childhood stunting remains a major public health concern with an estimated 155 million children under age of 5 years being stunted.6,9,10 Despite steady declines in the global prevalence childhood stunting, progress has been too slow to achieve the 2025 global nutrition target of reducing stunting by 40%. 9 Recent data shows that the prevalence of under-five stunting in Africa is 29.1%, which is higher than the global average of 21.3%. 9 Within the continent, Eastern Africa has the highest burden of stunting (34.5%) while Western Africa has one of the lowest at 27.7%. 9
Stunting results from a complex interaction of household, environmental, socioeconomic, and cultural factors and is associated with many negative consequences such as; increased susceptibility to infections, impaired cognitive, motor, and language development as well as increased risk of non-communicable diseases later in life.11-13 Very often, stunted children tend to have poor school performance and low productivity as adults.14,15 Poor academic performance, the repetition of grades/classes, and high school-dropout rates lead to significant economic losses for the education system, families, and the labor market.11,16 In addition, stunted children who experience rapid weight gain after 2 years of age have a higher likelihood of becoming overweight or obese in adulthood, so they are at a higher risk of developing non-communicable diseases (NCD’s).17,18
In Sierra Leone, more than 3 million people are estimated to lack access to sufficient food. 19 Consequently, chronic undernutrition is widespread and nearly a third of under 5 children are stunted.19,20 In order to ensure the WHO nutrition targets of reducing stunting by 40% before 2025 and by 50% before 2030, annual reduction of 4% in the average stunting rate is needed.21,22 However, Sierra Leone is far from achieving this having had a meager average annual reduction of only 0.25% between 2005 and 2013. 5 Studies based on national and regional data from the country have shown stark inequalities in stunting prevalence across regions, residence, and socio-economic status. 5 While wealth and educational inequalities have been shown to have slightly improved over time, residence (rural and urban) and subnational regional inequalities have remained unchanged. 5 Although disparities in childhood stunting between urban and rural areas have been documented, 5 information on factors responsible for these differences have not been explained adequately. Information on the factors associated with the rural-urban differentials in childhood stunting is of especial importance as policies, programs, and interventions that are necessary to reduce stunting may differ between rural and urban areas. Understanding the various factors associated with stunting in different settings is key to designing effective context-specific interventions. Therefore, we aimed to determine rural and urban correlates of stunting among children under 5 years of age (under-fives) in Sierra Leone in a nationally representative sample.
Methods
Study design and participants
Sierra Leone Demographic and Health Survey (SLDHS) 2019 was a nationally representative cross-sectional survey implemented by Statistics Sierra Leone (Stats SL) with technical assistance from ICF through the DHS Program and funded by the United States Agency for International Development (USAID). Data collection took place from May to August 2019. 23 The primary sampling unit (PSU), referred to as a cluster was based on enumeration areas (EAs) from the 2015 EA population census frame. 23 Stratification was achieved by separating districts into urban and rural areas with a total of 31 sampling strata created. In the first stage, 578 EAs were selected with probability proportional to EA size which was the number of households within the EA. 23 The survey used a stratified 2-stage cluster sampling design that resulted in the random selection of 13 872 households. 23 DHS uses different questionnaires for the various thematic parts covered in the survey. The household questionnaire collects data on household environment, assets, and basic demographic information of household members while women’s questionnaire collects data regarding women’s reproductive health, domestic violence, and nutrition indicators. The men’s questionnaire collects data on men’s health and the biomarker questionnaire collects data on anthropometry and blood tests.24,25 This secondary analysis included children aged less than 60 months whose anthropometric characteristics have been recorded with consent from their parents or caretakers. To ensure quality of anthropometric measurements, trained health technicians were deployed to measure the height and weight of participants. 23 The height of children less than 24 months of age was measured with the child lying down while that of older children was measured in the upright position using ShorrBoard® measuring boards. 23 SECA scales with a digital display (model number SECA 878U) were used for measuring weight. 23 Out of the weighted sample of 9771 children in the data set, 5345 were not sampled for anthropometry in the original survey design, 57 were flagged cases while 324 had missing measurements. A final weighted sample of 4045 children aged less than 60 months was included in our secondary analysis as summarized in Supplemental File 1. A full protocol with detailed explanation about the data collection process and sampling is available online. 23
Variables
Outcome variables
The outcome variable was stunting, coded as one (1) for stunted children and zero (0) for non-stunted children. The DHS used the WHO standard growth charts for children and collected data on every child’s height, age, and sex to calculate the height-for-age Z-scores to assess stunting.16,26 Finally, stunting was defined as a z-score lower than—2 standard deviations from the median of the World Health Organization (WHO) 26 child growth standards.
Independent variables
Independent variables included in the study were based on previous studies,6,16,27,28 the WHO stunting framework11,29 and availability in the SLDHS data base. We included a total of 15 variables categorized as below.
Parental characteristics
Mother’s parity (para 1, para 2-5, and above), mother’s place of delivery (home or health facility), mother’s working status (working and not working), mother’s marital status (married and not married), mother’s and father’s levels of education (no education, primary, secondary, and tertiary), mother’s age (15-19, 20-34, 35-49), and mother’s stunting status (stunted defined as less than 145 cm and not stunted). 24 In rural areas, the number of children with mothers and fathers with tertiary education was extremely low (9 and 65, respectively) thus we re-categorized level of education into no education, primary and post primary levels during bivariable and multivariable analysis.
Household characteristics
These included region (Northwest, Eastern, Western, Southern, and Northern), wealth index of household (categorized into quintiles: richest, richer, middle, poorer, and poorest), and sex of household head (female and male). In the urban data set, the poorest quintile had only 5 children (0.4% of the sample) so we re-categorized wealth index into poor (combining poorest and poorer quintiles), middle, richer, and richest during logistic regression analysis. Similarly, among rural children, wealth index was re-categorized into rich (combining richest and richer quintiles), middle, poor, and poorest quintiles since the richest quintile had only 18 children (0.7% of the sample).
Child characteristics
Age of the child was categorized into months (less than 24 months and 24-59 months) while sex of the child into male and female.
Statistical analysis
Frequency tables and proportions/percentages were used to describe summaries of categorical variables while mean ± standard deviation (sd) was used for continuous variables. To account for the unequal probability sampling in different strata and to ensure representativeness of the survey results at all levels, we used sample weights. Furthermore, we used SPSS version 25.0 statistical software complex samples package incorporating the following variables in the analysis plan to account for the multistage sample design inherent in the DHS dataset: individual sample weight, sample strata for sampling errors/design, and cluster number.30-32 Use of complex samples package ensures that the sample design is incorporated into the analysis leading to accurate and reliable results. Cross tabulation was conducted and associations between background characteristics and children’s nutritional status (stunting) including their P-values were presented in Table 1. To assess the association of each independent variable with stunting, bivariable logistic regressions were conducted and crude odds ratio (COR), 95% confidence interval (CI) and P-values presented separately for rural and urban samples. Independent variables found significant at bivariable level (P-value ⩽.25) were included in the final multivariable logistic regression models. Variables that had P-values above .25 33 at bivariable level were not included in Tables 2 and 3. To enable a comparison between both areas at the bivariable level, we used the same independent variables for both rural and urban children. Adjusted odds ratios (AOR), 95% Confidence Intervals (CI) and P-values were calculated with statistical significance level set at P-value <.05. All variables in the model were assessed for collinearity, and no variables had a variance inflation factor (VIF) greater than 2.34,35 Sensitivity analysis was done by excluding mother’s stunting status in the rural children’s multivariable logistic regression model since a small sample of 40 mothers (1.5%) were stunted.
Background characteristics of children and their stunting status based on place of residence using SLDHS 2019.
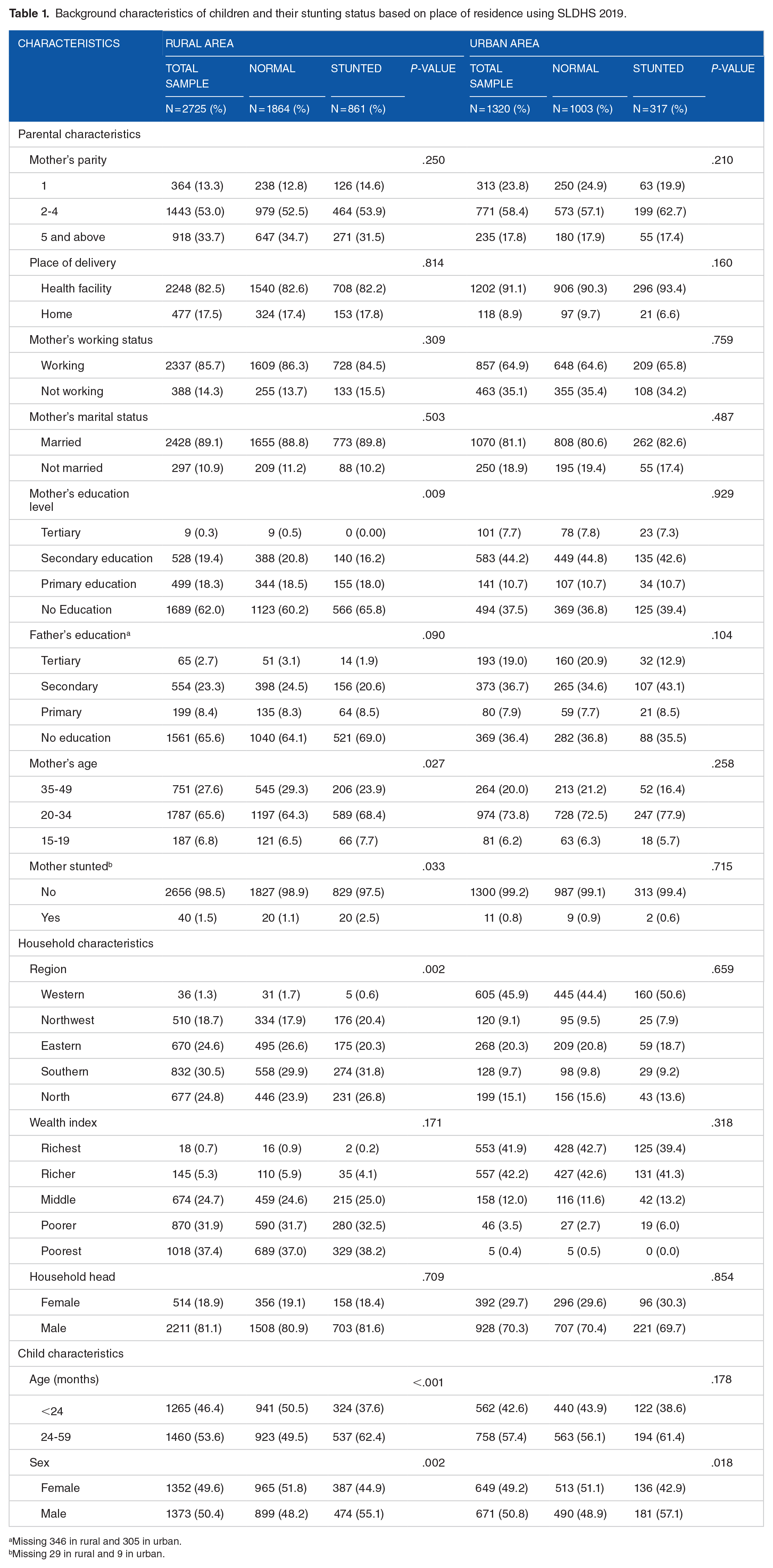
Missing 346 in rural and 305 in urban.
Missing 29 in rural and 9 in urban.
Correlates of stunting among rural under-5 children in Sierra Leone using 2019 SLDHS (N = 2725).

Multivariable logistic regression used. Values in bold were statistically significant.
Correlates of stunting among urban under-5 children in Sierra Leone in 2019 SLDHS (N = 1320).
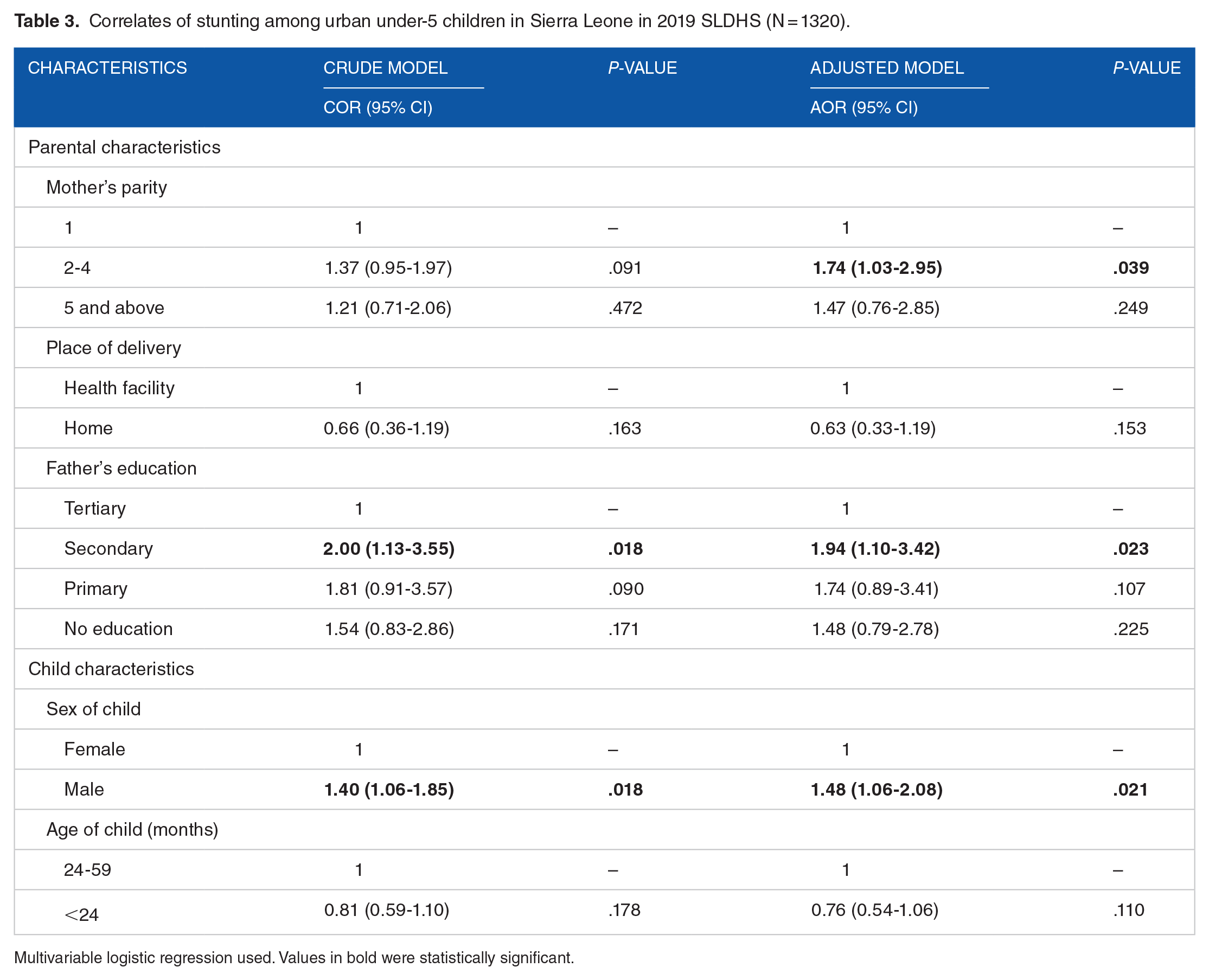
Multivariable logistic regression used. Values in bold were statistically significant.
Results
The study included 4045 children aged less than 60 months (2725 rural children and 1320 urban children). In rural areas, over half of mothers (62%) and fathers (57.3%) had no education, 37.4% of households belonged to the poorest quintile and only 0.7% were in the richest quintile. Southern region had the highest proportion of rural children (30.5%) and Western had the lowest (1.3%). The mean age of rural children was 26.75 ± 17.33 months (data not shown in the table). In urban areas, 37.5% (mothers) and 28.0% (fathers) had no education, 41.9% of households belonged to the richest quintile and only 0.4% belonged to the poorest quintile. Western region had the highest proportion of urban children (45.9%) and Northwest had the lowest (9.1%). The mean age of urban children was 27.93 ± 7.37 months. The overall mean height-for-age Z-scores were −1.27 ± 1.50 in total sample. The mean height-for-age Z-scores for rural children were −1.37 ± 1.43 compared to −1.07 ± 1.62 for urban children (data not shown in the table). The overall prevalence of stunting was 29.1% (1177/4045) (95% CI 27.7-30.4) (data not shown in the table). The prevalence of stunting among children in the rural areas was 31.6% (861/2725) (95% CI 29.8-33.2) while the prevalence among urban children was 24.0% (317/1320) (95% CI 21.6-26.1). More detailed characteristics of study participants are shown in Table 1.
Factors associated with stunting among rural and urban under-five children
In the multivariable analysis, mother’s level of education, age, stunting status (as parental characteristics), region (as a household characteristic), and age and sex of the child (as child characteristics) were significantly associated with childhood stunting among rural children (Table 2). While among urban children, mother’s parity, and father’s level of education (as parental characteristics) and sex of the child (as child characteristics) were the factors associated with stunting (Table 3). Among rural children, those with mothers with no education (aOR = 1.87; 95% CI 1.28-2.71, P < .01), younger mothers aged 15 to 19 years (aOR = 2.08; 95% CI 1.17-3.69, P < .05), stunted mothers (aOR = 2.37; 95% CI 1.07-5.24, P < .05), older children (24-59 months) (aOR = 1.83; 95% CI 1.48-2.27, P < .001), and boys (aOR = 1.37; 95% CI 1.12-1.66, P < .01) were more likely to be stunted compared to those with mothers with post-primary education, older mothers, non-stunted mothers, younger children, and girls, respectively. Children from the Western region (aOR = 0.40; 95% CI 0.16-0.99, P < .05) were less likely to be stunted compared to those from the Northern region. Among urban children, children whose mothers were para 2 to 4 (aOR = 1.74; 95% CI 1.03-2.95, P < .05), those whose fathers had secondary education (aOR = 1.94; 95% CI 1.10-3.42, P < .05) and boys (aOR = 1.48; 95% CI 1.06-2.08, P < .05) were more likely to be stunted compared to children whose mothers were less parous (para 1), those with fathers having tertiary level of education and girls, respectively.
Sensitivity analysis
When mother’s stunting status was excluded in rural children’s multivariable model, mother’s level of education, age, region, and age and sex of the child remained significant, and no significant changes were observed in the strengths of associations.
Discussion
In this study, we found that the overall prevalence of stunting in Sierra Leone was 29.1% (Rural prevalence was 31.6% while in urban areas it was 24.0%), which is slightly higher than the global (21.3%) and Western Africa (27.7%) prevalence, 9 and lower than the average prevalence in sub-Saharan Africa (34.0%).16,36 It is however, similar to the overall African region prevalence (29.1%). 9 Six factors (mother’s level of education, age, stunting status, region, and child’s age and sex) were significantly associated with childhood stunting in rural areas while 3 factors (mother’s parity, father’s level of education, and sex of the child) were significantly associated with childhood stunting in urban areas.
Sex of the child was a common factor in both rural and urban settings. The strength of association between sex of the child and childhood stunting did not vary substantially across both areas. Boys had more odds of being stunted compared to girls. These sex differences could partly be explained by behavioral patterns employed by the communities such as, favoring girls by feeding them more than boys.37,38 Boys require comparatively more calories for growth and development than girls because they are more physically active and hence expend more amounts of energy which should have been channeled into increasing growth.6,38 On the contrary, girls are culturally expected to be less active as they are given lighter duties to perform. 38 Furthermore, epidemiological evidence shows boys are more biologically vulnerable to illnesses than girls39,40 which might predispose them to stunting. Boys have been documented in several studies done in similar contexts to have more odds of stunting compared to girls.6,37,41,42
We observed stark differences between rural and urban areas in factors associated with childhood stunting. This has also been observed in several other studies.43-45 In all these studies, these differences were attributed to nutrition adequacy and availability of healthcare services. In our study, these differences can partly be attributed to socio-economic differences in rural and urban areas in Sierra Leone.46,47
In rural areas, mainly maternal factors of stunting status, age, and education were significantly associated with childhood stunting compared to parity and paternal education in urban areas. The strong impact of these maternal factors on rural children’s stunting is mostly multifaceted. Poor nutrition mainly experienced in rural areas 5 leads to maternal undernutrition.48,49 A mother’s social and nutritional environment during early life is an important determinant of her children’s subsequent health and nutrition outcomes, sometimes even more than maternal nutritional status during pregnancy. 50 Children born into this environment of already existing nutritional deficiency and other risk factors are at an increased risk of stunting and other forms of undernutrition which perpetuates an intergenerational cycle of undernutrition and related adverse outcomes.49,51 Mother’s stunting status has been shown to be associated with higher odds of stunting among children in several other studies.6,42,50 The extremely low numbers of stunted mothers in urban areas could partly explain why mother’s stunting status was not found to be associated with stunting among urban children.
Belonging to younger mothers less than 35 years among rural children was associated with more odds of stunting compared to having mothers aged 35 to 49 years. The odds were higher among teenage mothers. This may be attributed to the fact that younger mothers lack the requisite experience or knowledge to provide the child with the proper care. 37 Hence in rural areas, special attention should be given to younger mothers during antenatal and postnatal care to ensure that they receive adequate nutrition counseling. Mother’s age has been shown to be a predictor of childhood stunting in several studies.27,37,52 The documented challenges in availability of public health facilities in rural areas limit proper healthcare access including nutrition counseling, immunizations in these settings.43,53,54 Such lack of access coupled with low education levels among rural women (only 19.7% had post-primary education in rural areas compared to 51.9% in urban areas) might have negative effects on the young and inexperienced rural mothers which could partly explain why mother’s younger age was significantly associated with stunting in rural areas and not in urban.
Parity was the only maternal factor associated with stunting among urban children. However, only the sub-category of para 2 to 4 showed statistically significant association and the observed non significance among mothers of para 5 and above could be partly attributed to the smaller number of children in this category. Higher parity was associated with higher odds of stunting, a finding similar to several other studies.55-58 The higher odds of stunting among children with high parity mothers may be attributed to the increased family size associated with higher parity. 55 Increase in family size especially in urban areas where families are less likely to grow their own food and have to purchase food may lead to scarcity of resources mainly food hence inadequate nutrient intake. 55 Furthermore, the decreased maternal contact time due to tight work schedules in urban areas unlike rural areas may lead to insufficient time to ensure that the health and nutrition needs of each child are given close attention.40,55 This inadequate care risks inadequate nutrient intake and infections which increases the likelihood of stunting.
Parental levels of education were significantly associated with stunting as shown in several other studies.27,37,38,59-61 Differences were observed with fathers’ level of education being significant in urban areas while mothers’ level of education being significant in rural areas. In predominantly patriarchal African societies, 62 fathers are the main sources of household income and have the highest decision making on food purchases. Given that rural communities are more likely to grow their own food unlike urban areas where most of the food is purchased,40,63 fathers’ level of education in this context is translates to a higher household income, better understanding of health and nutrition information, hence making informed decisions regarding food choices for improved nutrition of their children.61,64 Women in rural areas tend to be less empowered than their urban counterparts due to the conservative nature of societies in the area yet are the main care givers. Furthermore, rural areas unlike urban have limited access to clean and safe water, proper sanitation, and good health facilities. These factors are crucial, as they directly affect children’s health. 64 Given that mothers are mainly the care givers; increased levels of education lead to better health and nutrition literacy and higher levels of empowerment. This translates to higher decision making powers hence active involvement in the making of better health decisions regarding their children.5,59,61 There is a need to further study these observed rural and urban differences and associations between stunting and parental education.
Our study found that rural children aged 24 to 59 months had higher odds of stunting compared to those aged below 24 months. Similar findings have been reported by several other studies.6,37,42,64 This may be partly attributed to the protective effect of breastfeeding during the first 6 months and timely introduction of appropriate complementary foods with continued breastfeeding up to 23 months and unhealthy food consumption during the complementary feeding window predisposing older children to inadequate nutrient intake. 37 Furthermore, older children require more energy and adequate nutrients for proper growth and development42,64 which are usually lacking in rural children’s meals.5,65
Region was the only significant household level variable and was significant only among rural children. Rural children in the Western and Eastern regions were less likely to be stunted compared to those from the Northern region. From past studies, Northern and Western regions have registered the highest and lowest prevalence of stunting respectively. 5 This persistent high levels of stunting in the Northern region require further exploration to identify its drivers and pave the way for context specific interventions that would help reduce the subnational disparities in stunting. 5 The observed regional differences could be attributed to the differences in values, beliefs, culture, and socio-economic conditions that exist within each region. Several studies in Sierra Leone have found residents of western region to have higher levels of education than those from other regions.62,66 The 2018 government of Sierra Leone and UNICEF 67 multidimensional child poverty report shows that Western and Eastern regions have the lowest child poverty headcount ratios compared to other regions . In addition, the Western region has the largest concentration of health workers, is the most developed and houses the capital and economic city of the country and hence has higher quality social amenities which could translate to better healthcare and access to food.68,69 Furthermore, children in Northern Sierra Leone have also been documented to be more likely to have childhood illnesses compared to children in the Western region. 70 Less poverty, easier access to healthcare and low incidence of childhood illnesses might be among the reasons explaining lower likelihood of stunting in the Western and Eastern regions. Region has been shown to be a predictor of childhood stunting in several other studies.27,38,52
Strengths and limitations
Data used in our study was population-based with a large sample size which achieved a 99% household response rate. The study used the 2019 SLDHS dataset which is the most recent nationally and internationally recognized data available in Sierra Leone. Hence findings from this study can be generalized to all children in Sierra Leone. However, due to the cross-sectional nature of the study design, establishing a causal relationship between the observed predictors and stunting is not possible. Most data on the predictors were based on self-reporting and could not be verified through records which risks socially acceptable answers hence information bias. Some variables such as stunted mothers across rural and urban areas and Western region in rural areas had smaller samples which could have affected the results
In addition, although a comprehensive set of variables were used in our analysis, residual confounding from unavailable factors such as history of chronic conditions could not be ruled out.
Conclusion
In Sierra Leone, stunting is more prevalent in the rural areas compared to the urban areas. Sex of the child is a strong and the only common predictor in both rural and urban areas hence interventions designed to reduce stunting should target boys in both rural and urban areas. Our study findings suggest that stunting could be reduced if tailored interventions are implemented in both rural and urban areas. For rural areas, there is need to target older, male children with younger, stunted, uneducated mothers from Northern Sierra Leone and male children belonging to multiparous mothers and fathers with lower levels of education in urban areas.
Supplemental Material
sj-docx-1-nmi-10.1177_11786388211047056 – Supplemental material for Rural and Urban Correlates of Stunting Among Under-Five Children in Sierra Leone: A 2019 Nationwide Cross-Sectional Survey
Supplemental material, sj-docx-1-nmi-10.1177_11786388211047056 for Rural and Urban Correlates of Stunting Among Under-Five Children in Sierra Leone: A 2019 Nationwide Cross-Sectional Survey by Quraish Sserwanja, Kassim Kamara, Linet M Mutisya, Milton W Musaba and Shirin Ziaei in Nutrition and Metabolic Insights
Footnotes
Acknowledgements
We thank the MEASURE DHS program for availing us with the data.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
QS conceived the idea, drafted the manuscript, performed analysis, and interpreted the results. SZ participated in reviewing the first version of the manuscript, interpretation of results and drafted the subsequent versions of the manuscript. LMM, KK, and MWM participated in the design of the study and helped in results interpretation and writing. All authors read and approved the final manuscript.
Ethics and Consent
High international ethical standards are ensured for MEASURE DHS surveys as ethical approval from the country is obtained from a national ethical review board and local authorities before implementing the survey and well-informed verbal consent is sought from the respondents prior to data collection. This data set was obtained from the MEASURE DHS website (URL: ![]() ) after getting their permission and no formal ethical clearance was obtained since we conducted secondary analysis of publicly available data.
) after getting their permission and no formal ethical clearance was obtained since we conducted secondary analysis of publicly available data.
Data Sharing Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.