
Abstract
Objectives:
We explored the maternal characteristics that mediate the effect of household poverty on childhood undernutrition.
Methods:
We used the population-based Bangladesh Demographic Health Survey data from 2014 for demographic characteristics, child and maternal factors.
Results:
Of the 7173 under-5 children, 3456 (48.2%) had undernutrition. The prevalence of undernutrition was less common in wealthy households (poorest vs richest: adjusted prevalence ratio [aPR] = 1.37), mothers having history of antenatal care (ANC) visits (no visit vs ≥ 4 visits: aPR = 1.22), maternal higher education (no education vs higher education: aPR = 1.54), and mothers with good nutritional status (underweight vs healthy: aPR = 1.13). The risk of undernutrition (37.1%) was attributed to household wealth, mediated 55% by maternal factors; of which 20% by maternal education, 21% by ANC visits, and 14% by maternal nutritional status.
Conclusions:
Our study findings outlined higher maternal education, ≥ 4 ANC visits and good maternal nutritional status in mediating the impact of household wealth on childhood nutrition.
Introduction
Any anthropometric failure which is an indicator of undernutrition among children under-5 years of age is an important public health problem that influences child’s growth, brain development, disease resistance, 1 -5 mortality, 6 educational attainment, and economic productivity in their later life. 7 Globally, undernutrition categorized as stunting affects 155 million, wasting affects 55 million and underweight affects 41 million under-5 children. 8 Among the undernourished children around the world 70% to 80% live in lower- and middle-income countries. 9 In the 65th World Health Assembly in 2012, a global target was set for the reduction of global number of under-5 stunted children up to 40% and wasted children up to 5% by the year 2025. 10 Improvement of undernutrition among children under-5 years is also included in the Sustainable Development Goal 2 by 2030. 11 Bangladesh has set a target to decrease the prevalence of childhood stunting to 25%, wasting to < 8% and underweight to 20% by 2020. 12,13 Thereby, it is crucial to develop effective strategies to prevail over childhood undernutrition. However, to develop effective strategies for the decision-making by the health policy makers it is imperative to mount up sufficient evidence to understand the explicit determinants of undernutrition among children.
The existing evidence on undernutrition among children has been focused on commonly used single indicators which may overlap with biological processes. Therefore, these single indicators cannot provide a comprehensive estimate of overall undernutrition among children in the population. 14
Socioeconomic factors are an important contributor to nutritional status of children and are consistent in different countries worldwide for a long duration in relation to age, gender, or other demographic factors. 9,15,16 Hence, household poverty is a consistent determinant of poor nutrition in children aged 0 to 59 months 17,18 and affects their health outcomes. 19 Though studies have identified different demographic, maternal, sociocultural, and political factors to be important determinants of childhood undernutrition, the mediating factors of household poverty are unrecognized. In our study, maternal factors have been hypothesized to mediate the association between household poverty and undernutrition among children. 20 -25 Thereby, studies in new settings on the effects of household poverty on maternal factors and undernutrition among children under 5 years of age may be useful in developing effective strategy.
This study examines the prevalence and investigates the risk factors of undernutrition among children under 5 years of age in Bangladesh. We hypothesized that there is household wealth inequality among undernourished children and this inequality is the maternal education, antenatal care (ANC) visits during pregnancy, maternal nutritional status, dietary quality, environmental sanitation, and housing factors such as crowding and other potential confounders. We considered the household wealth, maternal factors, and confounders in the analysis due to data availability in the study as shown in Figure 1 (conceptual framework). We aim to estimate the burden of undernutrition among children and to identify the determinants of undernutrition among children under 5 years of age and to investigate the factors mediating the observed relationship between household wealth and undernutrition among children.
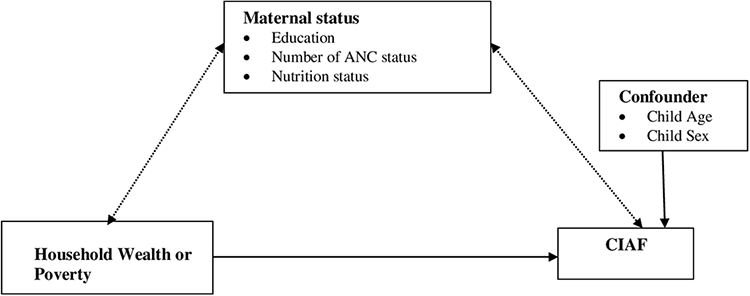
Conceptual framework for Composite Index of Anthropometric Failure (CIAF).
Materials and Methods
Study Design
The National Institute of Population Research and Training (NIPORT), ICF International (USA), and Mitra and Associates conducted a population-based cross-sectional study from June to November 2014 in Bangladesh. 26 For our study purpose, we extracted the data set on under-5 children from the Bangladesh Demographic and Health Survey (BDHS), 2014.
Sampling Technique
Bangladesh Bureau of Statistics constructed a list of Enumeration Areas (EAs) for the 2011 Population and Housing Census of the People’s Republic of Bangladesh, and this was the sampling frame in the survey. A primary sampling unit in each EA consisted of an average of 120 households. The sampling method was a 2-stage stratified sample of households stratified by rural and urban areas. In the first stage, the probability proportional to the size of EAs was used to select the 207 EAs in urban areas and 393 in rural areas. In the second stage of sampling, systematic sampling was used to select an average of 30 households in each selected EA. 26 The BDHS 2014 reported information on 7886 children under 5 years for anthropometric measurements. We excluded 713 children who were flagged as having invalid data in the z-score for stunting, wasting, or underweight. Thereby, finally, we used 7173 children who had available observed measures of anthropometric data for this study.
Measurements
Composite Index of Anthropometric Failure (CIAF) Outcomes
The conventional measurement of undernutrition among children under 5 years includes −2 SD from the median height for age Z score (HAZ), weight for age Z score (WAZ), and weight for height Z score (WHZ). 27 There are three single anthropometric indices to categorize children based upon their nutritional status; stunted (HAZ < −2 SD) children indicate a long-term nutritional deficiency; wasted (WHZ < −2 SD) children are known as a short-term or current nutritional deficiency and underweight (WAZ < −2 SD) children indicate both long-term or short-term nutritional deficiency.
The traditional method excludes children who have other indices in the measurement of undernutrition, so the conventional approach underestimates the overall prevalence of undernutrition among children. Economist Peter Svedberg disagrees with the traditional nutrition indices for measuring the burden of undernutrition among children and suggested the Svedberg model 14 which has classified the children into 6 groups of anthropometric failures (Table 1). He has proposed the composite index of anthropometric failure (CIAF) as a more precise approach for measuring undernutrition. The CIAF includes those children who are stunted, wasted, and underweight or any combination 14,28 of 3 for a further level of analysis and interpretation of their health status.
Classification of Children With Anthropometric Failures.a
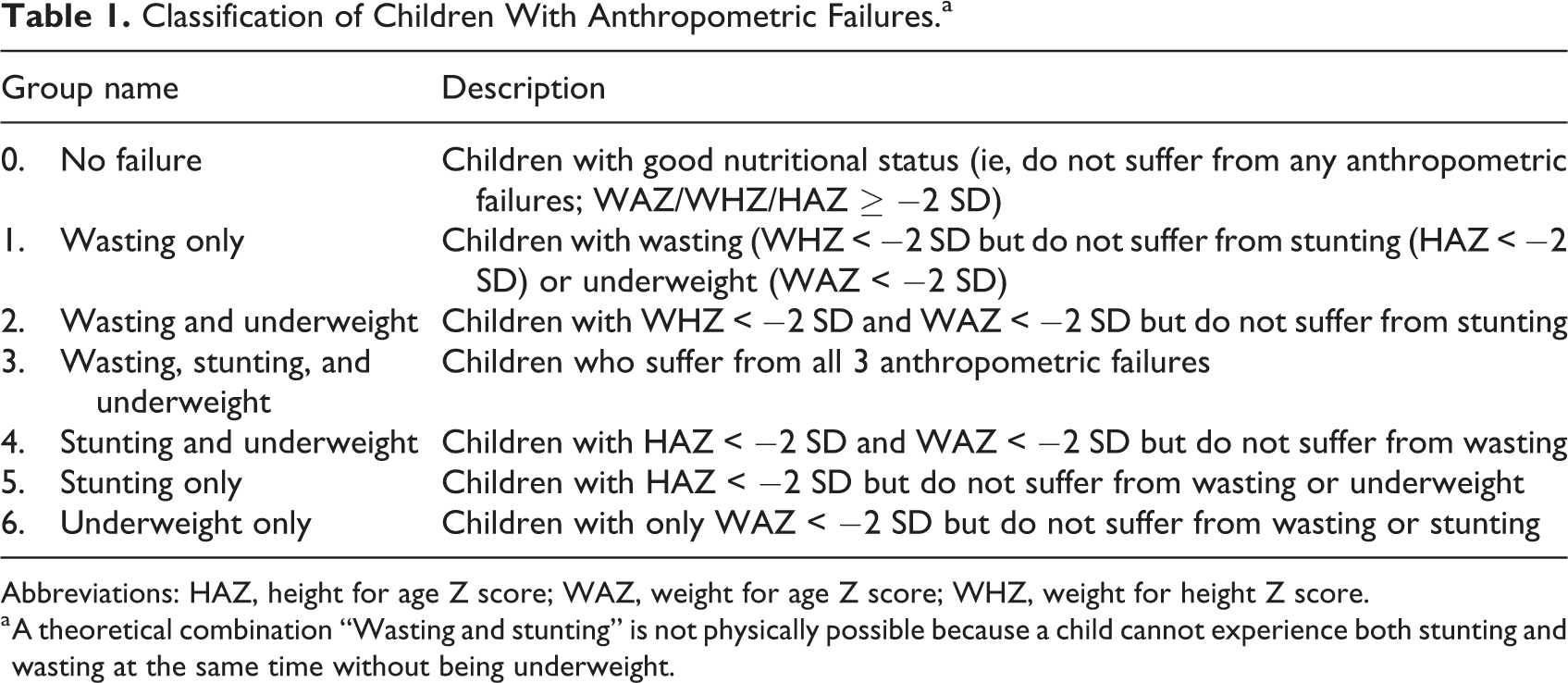
Abbreviations: HAZ, height for age Z score; WAZ, weight for age Z score; WHZ, weight for height Z score.
a A theoretical combination “Wasting and stunting” is not physically possible because a child cannot experience both stunting and wasting at the same time without being underweight.
Household Wealth Index
The principal component analysis (PCA) was applied to construct the household wealth index from household ownership assets. The PCA is a weighted combination of the indicators that maximized most of the information in the first principal component (first PC). Therefore, first PC was used to generate a wealth of household and then categorized into 5 quintiles: poorest, poor, middle, rich, and richest. 29
Mediating Factors
There are maternal factors hypothesized to mediate the association between poverty and undernutrition among children: maternal education, number of ANC visits during pregnancy, and maternal nutrition status. These factors were positively associated with childhood undernutrition, and were also influenced by wealth. 22,30 -32 Moreover, maternal determinants interrelated in the components of the causal pathway linking poverty to undernutrition among children.
We categorized mothers into 5 groups based on schooling attainment: No formal education, primary incomplete, primary completed, secondary incomplete and secondary completed, and higher education, 26 and three groups based on history of ANC visits during pregnancy: no ANC visits, 1 to 4 ANC visits, and more than 4 ANC visits. 22 We categorized maternal body mass index (BMI) into 3 groups: underweight (BMI < 18.5), well-healthy (range of BMI: 18.5-24.9), overweight and obese (BMI: ≥ 25). 27
Statistical Analysis
We calculated the prevalence of binary outcome CIAF (1 = any malnutrition and 0 = none) and explored the distributions of demographic characteristics, maternal factors, and anthropometric failures; using proportions for categorical or binary variables; using mean and SD for continuous variables. We performed the Poisson regression with account for the sampling clusters and strata in models for CIAF to adjust for the intra-cluster correlation of children. 33 -35 We estimated prevalence ratios (PRs) and robust CI for variables using modified Poisson regressions 36,37 in models based on the constructed conceptual framework (Figure 1).
We used bivariate and multivariate models separately step-by-step to examine the factors independently associated (PR) with CIAF. Multivariate analysis was applied in the full model considering the maternal factors which were found statistically significant (P value < .05) in bivariate analysis (model 1) to identify the associated factors with CIAF. Followed by model 2 additionally including the maternal education variable, model 3 additionally included ANC visit variables and model 4 additionally included maternal nutritional status separately.
Besides, we calculated attributable risks for the total study population (ART) to quantify the risk of undernutrition among children. Walter has proposed the ART for binary or more categorical variables and defined as
Ethical Approval and Informed Consent
Since BDHS 2014 data sets were publicly available, there was no need for ethical approval for the secondary data analysis. Written informed consent was sought from the participants prior to interview in the survey and data were confidentially collected.
Results
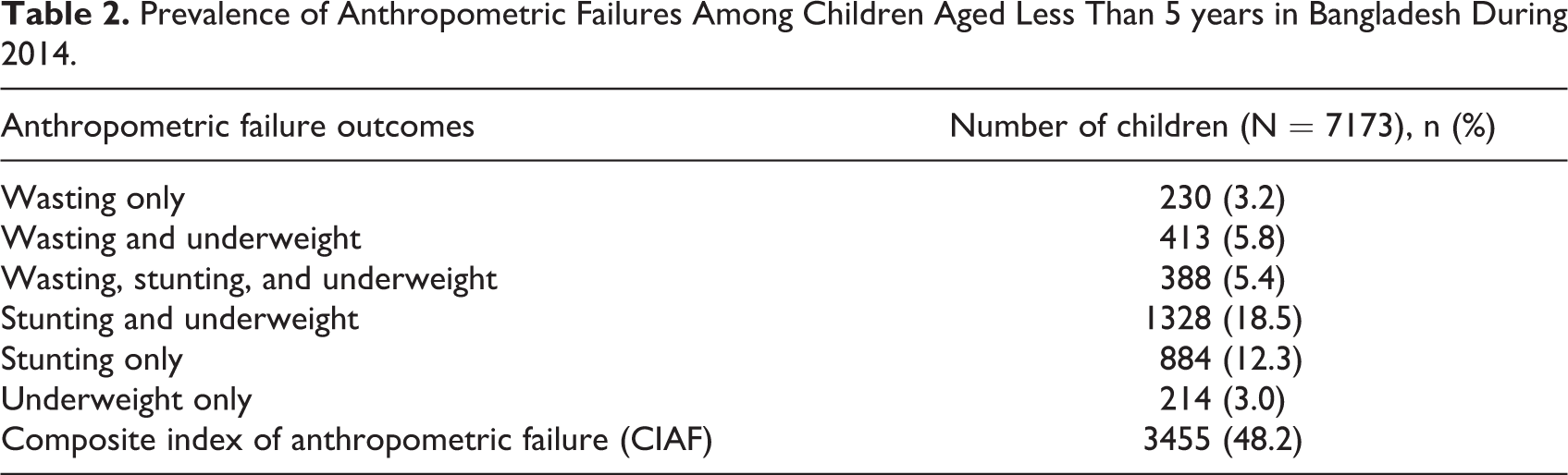
The survey consisted of 7173 children for whom the anthropometric measurements were available, the mean (SD) age of children were 29.3 (17.0) months, 3794 (52.9%) children were male, and one-third of the children had lived in rural areas. The CIAF was 48.2% for children under 5 years of age (Table 2).
Prevalence of Anthropometric Failures Among Children Aged Less Than 5 years in Bangladesh During 2014.
Factors Associated With the CIAF
The number of children born to mothers having no formal education was 1169 (16.3%); whereas 1110 (15.5%) of the children were born to secondary and higher educated mothers. The number of children born to mothers having no ANC visit during pregnancy were 878 (21.0%); while 1313 (31.3%) children were born to mothers who received ANC more than 4 times. The proportion of children born to underweight, good health, and overweight or obese mothers were 4265 (59.5%), 1576 (22.0%), and 1332 (18.6%), respectively. According to multivariate analysis (full model), the prevalence of CIAF was 37% more common in children from poorer households than those from wealthier households (poorest vs richest: aPR = 1.37; 95% CI: 1.13-1.66) after adjusting for maternal factors, child age, and sex. Moreover, after adjusting for children age, sex, and other factors, the prevalence of CIAF was higher in the children born to mothers with no formal education (no education vs secondary and higher education: aPR = 1.54; 95%CI: 1.30-1.84) than those born to mothers with secondary and higher education. The prevalence of CIAF was higher in the children born to mothers having no ANC visit during pregnancy (no visit vs ≥ 4 visits: aPR = 1.22; 95% CI: 1.07-1.39) than those born to mothers having more than 4 ANC visits, and the prevalence of CIAF was more common in the children of maternal underweight (underweight vs good health: aPR = 1.13; 95% CI: 1.07-1.23) than the children of good healthy mothers after controlling for children age, sex, and other factors (Table 3).
Household Wealth and Maternal Factors Contributing to Composite Index of Anthropometric Failure (CIAF) Among Children Under 5 Years in Bangladesh During 2014.a
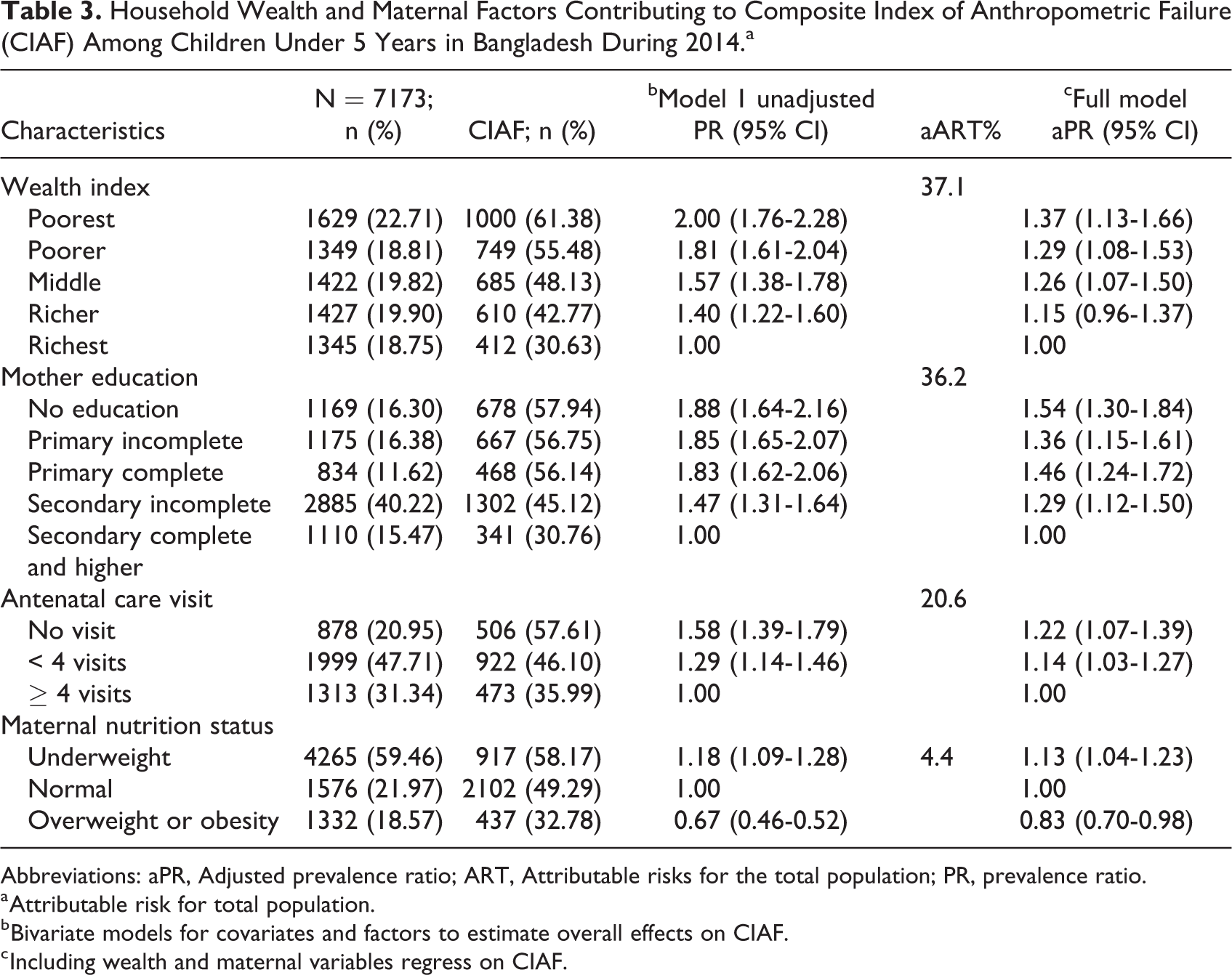
Abbreviations: aPR, Adjusted prevalence ratio; ART, Attributable risks for the total population; PR, prevalence ratio.
a Attributable risk for total population.
b Bivariate models for covariates and factors to estimate overall effects on CIAF.
c Including wealth and maternal variables regress on CIAF.
The ART of household wealth for the risk of CIAF was 37.1% (Table 4). Such risk for CIAF can be mediated up to 55% by maternal factors; of which 20% by maternal education, 21% by ANC visits, and 14% by maternal nutritional status (Figure 2).
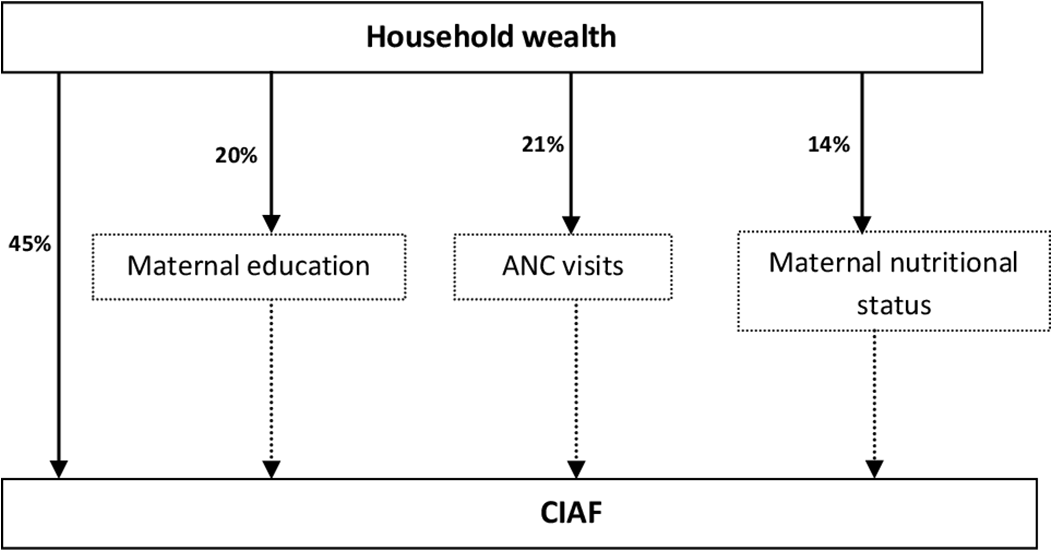
Proportion of attributable risk for the total population (ART) explained by mediating proportion.
The Risk Factors Associated With CIAF For Children Under 5 Years in Bangladesh During 2014.a
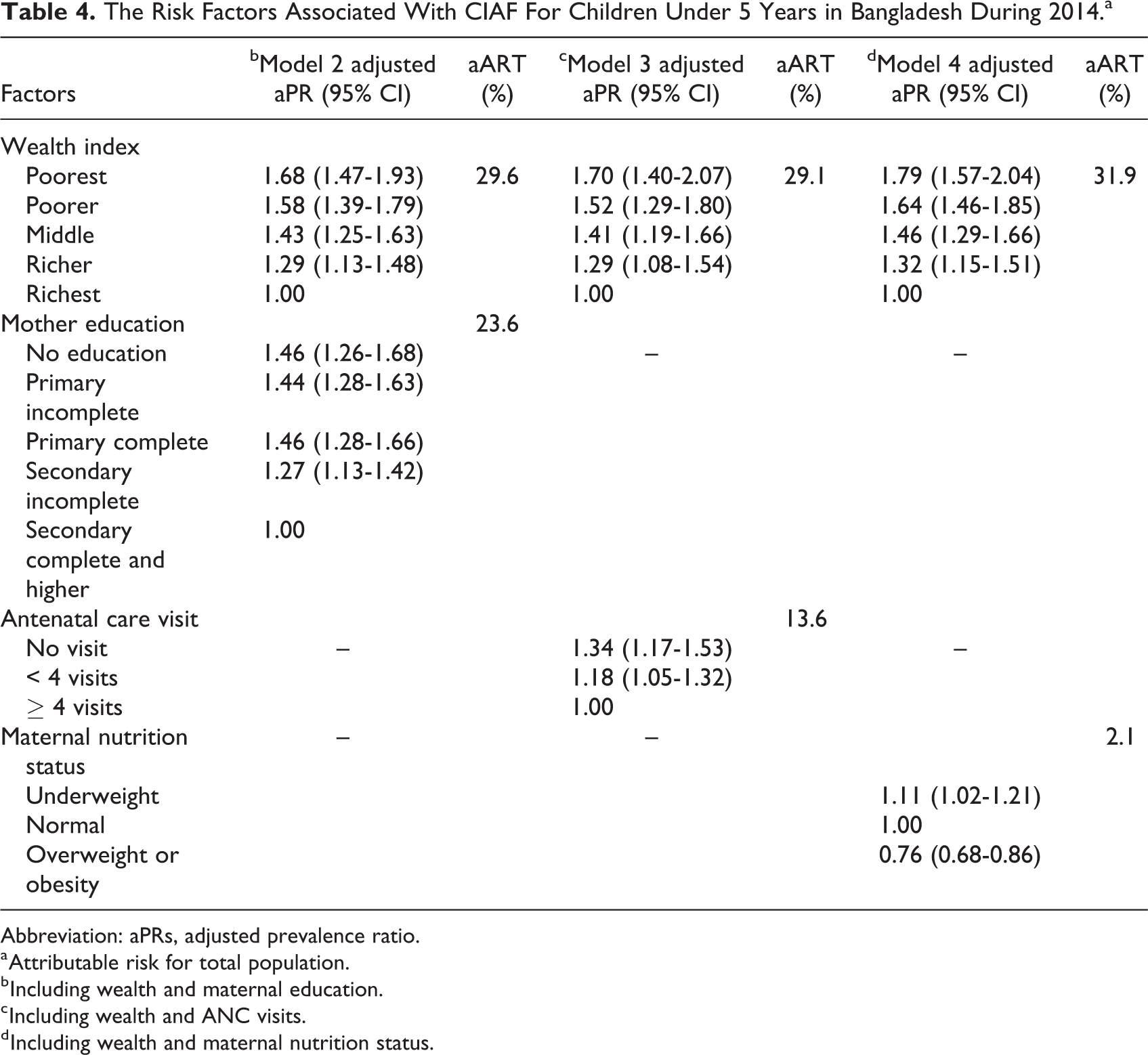
Abbreviation: aPRs, adjusted prevalence ratio.
a Attributable risk for total population.
b Including wealth and maternal education.
c Including wealth and ANC visits.
d Including wealth and maternal nutrition status.
Discussion
We used nationally representative BDHS survey data for the year of 2014 in Bangladesh, to estimate the burden of undernutrition among children under 5 years. We have identified the household wealth and maternal characteristics for the risk of CIAF, quantified the magnitude of ART, and have investigated the maternal factors mediate the effect of household wealth on CIAF. We found that the household wealth quintiles, maternal education, ANC visits during pregnancy, and maternal nutritional status were inversely associated with undernutrition. The household wealth attributed risk of CIAF can be mediated by maternal characteristics.
Previous studies constructed aggregated anthropometric failures such as CIAF to estimate the overall prevalence of childhood undernutrition. This study used individual CIAF for undernutrition among children because conventional indicators exclude a large number of undernourished children; therefore, it underestimates the overall burden of undernutrition among children. The most vulnerable children with single and overlapping anthropometric failures were identified by disaggregating the CIAF. 28,41 We observed undernutrition among almost half of the under-5 children.
The household wealth quintiles were significantly disproportionate among undernourished children in Bangladesh. The children who lived in richer households were less likely to be undernourished than the children who lived in poorer households, where poor sanitation, lack of pure drinking water, and inadequate food for children led to undernourishment. 42 It seems to be consistent with the previous population-based studies conducted in 39 countries in the world including Bangladesh. 41 Similarly, prior studies observed the effect of household wealth inequalities in different single indicators such as stunting, wasting, and underweight. 23,43
After controlling the effect of child age, sex, and household wealth, maternal education was the strongest predictor of undernutrition among children. We found that being a child of the higher educated mother is one and half times less likely to be undernourished than a child of an illiterate mother. The previous studies have described the impact of maternal education on the undernutrition of children. 20,44 Maternal education reduces childhood undernutrition because educated mothers earn more and can make better decisions to improve the health of their children. 45,46 Household wealth affects a child’s schooling, particularly enrollment of girls in school and later their education affects their child’s nutritional status. 47
We observed that the mother who received ANC during pregnancy could reduce the risk of undernutrition among their children. Other studies also found an inverse association between a number of ANC visits and the development of childhood undernutrition. The number of repeated visits for ANC during pregnancy may likely be essential in reducing undernutrition among children under-5 years. 22,48 A mother having repeated ANC visits get more opportunities to discuss their nutritional status and get advice on childcare from health professionals. 10 A report from WHO showed that the number of antenatal care visits made during pregnancy could improve the possibility of using skilled attendants at birth contributes to her child’s nutrition and can promote child nutrition practices including exclusive breastfeeding within the first 6 months of infant’s age. These factors might contribute to the prevention of childhood illness which may lead to the reduction childhood undernutrition. 48,49
Prior national representative studies from 1999 to 2011 21,50 found that childhood stunting was a single indicator of undernutrition associated with maternal underweight (BMI < 18.5). We observed that the prevalence of undernutrition among children of underweight mothers was 13% higher compared to children of mothers with good health.
Household poverty being a potential determinant of childhood undernutrition (ART = 37.1%) was the most significant finding observed in our analysis. Maternal factors mediated (Mediating proportion = 55%) more than half of the effect of household poverty. This might be due to poor households being firmly related to poor maternal status, such as lack of formal education, inadequate antenatal care, and poor maternal nutritional status. This finding of mediation of household poverty is not unexpected and found in other studies too. 21,23,28,41 The impact of household poverty on child’s undernutrition can be altered indirectly by improving maternal characteristics.
Limitations
In the analysis, concern was raised with the causal association and also to conduct pathway analysis as the household wealth quintiles, mediating factors, and outcomes were measured simultaneously to assess the childhood anthropometric failure outcomes. Child’s food habit and mother’s hygiene practices are very important for a child’s nutritional status, but the data were not available in BDHS 2014 survey. Further studies should be considered with time-varying exposures and repeated measurement of undernutrition.
Conclusion
Our study findings underscored higher maternal education, ≥ 4 ANC visits during pregnancy, and good maternal nutritional status in mediating the impact of household poverty on childhood undernutrition. Thereby, more emphasis should be given on current poverty mitigation efforts in the country, promoting girls schooling in early life, providing support to receive ANC during pregnancy period and ensuring maternal dietary food intake in early reproductive ages to reduce the inequalities in undernutrition among children under 5 years of age.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to BDHS, NIPORT, MEASURE DHS, and ICF International teams for data collection and for allowing to use these data for this study. The authors would like to acknowledge the contribution of caregivers/mothers of the study participants for their consent to enroll children in the study. icddr, b is also grateful to the Governments of Bangladesh, Canada, Sweden, and the UK for providing core/unrestricted support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.