
Abstract
Introduction:
Due to its widespread distribution and effects, type 2 diabetes is a frequently researched topic. However, the amount of information about type 2 diabetes in nursing homes residents is inadequate. The aim of this study is to elucidate on the frequency, treatments, comorbidities, and deaths of nursing home residents diagnosed with type 2 diabetes.
Materials and methods:
Type 2 diabetes was evaluated in 612 people accepted to nursing homes as residents between January 2005 and January 2013. Medical records, prescriptions, laboratory results, and comorbidities were evaluated statistically.
Results:
Approximately 26% (159) patients of the cohort had either preexisting type 2 diabetes during registration to nursing home or was diagnosed with it during the 8-year follow-up. The prevalence of DM was 25% in males and 26% in females. Average age was 75.7 ± 10.6 in diabetics and 76.7 ± 11.6 in non-diabetics. Hemoglobin, creatinine, triglycerides, HDL-cholesterol, and CRP values were not found to be different between the groups. Hypertension was diagnosed in 75% of diabetics versus 59% of non-diabetics, hyperlipidemia in 21% versus 7% (P < .01); however, atrial fibrillation was more common in non-diabetics (P = .022). There was no difference for survival rate between diabetic and non-diabetic groups (P = .743).
Conclusion:
Approximately 1 out of 4 nursing home residents were found to have diabetes, with females being more affected then males. The survival rates both at the diabetic and non-diabetic patients were detected similar. Glucose, total cholesterol, LDL-cholesterol, and blood pressure values which can all impact survival should be closely watched from early on in the disease progress and their values should be optimized.
Introduction
The ever aging population in Europe, as well as in Turkey, brings on new challenges such as increased expenditure on healthcare for the ageing population and necessitates better information on the direct or indirect factors effecting the health of old people. This information would lead to the optimization of health care policies towards the elderly and better guidance for the healthcare personnel on dealing with the chronic diseases.
Type 2 diabetes is a frequently researched topic since it is a common widespread issue causing worldwide effects. The diabetes prevalence in the US nursing homes was 16% in 1995 but it had jumped to 23% in just 9 years in 2004. 1 It is known that approximately 50% of Americans older than 65 have been diagnosed with diabetes.2,3 This high prevalence is particularly worrying in long term care facilities such as nursing homes.1,4,5 But the prevalence is approximately 21.7% in a 2020 study in Spain. 6 .In a study done in 2018 in US, the diabetes prevalence changes according to the state and ranges 12.3% to 22.5%. 7 The prevalence is nearly the same in the past years. It can be thought that diabetes can be cured because diabetes is a chronic disease.
The complications of diabetes are also more common in the elderly. Increased CV risk factors, mortality and morbidity related to diabetes, chronic renal disease, congestive heart failure, cognitive dysfunction and diabetes are all more common in ageing population with diabetes.8-10 Quality of life and depressive symptoms as well as nutritional status of elderly diabetic patients are also discussed at some researches.11-13 Little is known about the type 2 diabetes in the nursing home residents in Turkey. The aim of this study was to elucidate the frequency, treatments, survival rates and comorbidities of nursing home residents diagnosed with type 2 diabetes.
Materials and Methods
This study was conducted between January 2005 and January 2013 in a private 150-bed nursing home in Istanbul. Individuals older than 65 that have been residing in the nursing home for more than a month were included in the study. An eight-year longitudinal follow-up was performed. Each patient was followed for 8 years since admission but their follow-up durations were different. 12 Every new patient was taken to follow-up in this period. The medical history, biochemical laboratory values and consultations of patients were recorded at their first and the other visits. These records were used for the study retrospectively. The same internist, neurologist and psychiatrist monitored subjects. However, they were hospitalized in different regional hospitals in case of emergencies or surgeries. The medical records in these hospitals and blood tests which were taken by contracted laboratory coming to nursing home were collected and evaluated. Exclusion criteria were being younger than 65, the follow-up length being shorter than 1 month or patient not consenting. 720 ageing people were accepted into the nursing home during this period and 612 were incorporated into our study.
Patients demonstrating their diabetic status with medical records, or patients being diagnosed with diabetes during the follow-up were included in the diabetics group. Diagnosis criteria for diabetes were fasting blood glucose 126 mg/dl and/or random blood glucose >200 mg/dl and/or HbA1c > 6.5%. 14
Extensive past medical history including but not limited to age, gender, weight, current medications, current ailments (e.g. hypertension, diabetes, arthritis, heart failure, dementia, renal failure), nutritional status was obtained and a physical examination was performed within the first 3 days following the acceptance to the nursing home.
Study was designed and conducted in compliance with the Declaration of Helsinki. Approval was also obtained from the local committee on ethics.
Statistical Analysis
Data was analyzed on a computer running Windows XP on the 21st version of SPSS (Statistical Packages of Social Sciences). The distribution of the data was gauged with Kolmogorov-Smirnov test. Explanatory statistics for continuous variables were given as average ±SD and frequency and percent for categorical variables. Unpaired two-sample t-test was performed to compare the data with normal distribution from 2 independent groups. Chi-square test was performed to analyze categorical variables. Log-rank distribution was carried out to compare the survival distributions. Hazard ratios with 95% confidence intervals were calculated to analyze the risk factors effecting survival. P < .05 was accepted as the threshold of statistical significance.
Results
About 612 subjects were included in our study. Approximately 26% of these (159) was either diagnosed with diabetes either previously or during the 8 year follow-up. Average age was 75.7 ± 10.6 years in diabetic patients and 76.7 ± 11.6 years in non-diabetic patients (P = .327). About 61% of the diabetics were female (P = .402). About 14% of the diabetic patients had BMI’s higher than 30 kg/m2 compared with 8% of non-diabetic patients; but the difference wasn’t statistically significant. On the other hand, average follow-up length was statistically longer in non-diabetic patients at 19.3 ± 24.9 months compared to 16.7 ± 19.4 months (P < .001). Total number of comorbidity was higher in diabetic patients during the beginning of the study, however this difference died out during the follow-up period (P = 1.117). Percentage of subjects having comorbidity more than 4 was 65%, in diabetic patients and 56% in non-diabetic patients and more than 6 comorbidity was 22% in diabetic patients, 13% in non-diabetic patients (P < .001). Being on more than 4 concurrent medications was also more common in diabetic patients at 90% compared to 77% (P < .001). There was no statistical difference in dependency rates interestingly (P = . 295). Demographic characteristics of both diabetic patients and non-diabetic group are outlined in Table 1.
Demographic characteristics of old diabetics and non-diabetics.

BMI: Body mass index, meds: medications, prev: previous, mo: months.
Fasting blood glucose levels were higher in diabetic patients, as expected, during the initial screening (143.9 ± 62.4 vs 99.8 ± 20.5; P < .001) and at the end of the follow-up period (123.0 ± 36.8 vs 97.5 ± 18.0; P < .01). The average of HbA1c in the diabetic groups showed that the metabolic control of these patients was well done. Severe hypoglycemia was not seen during the study.
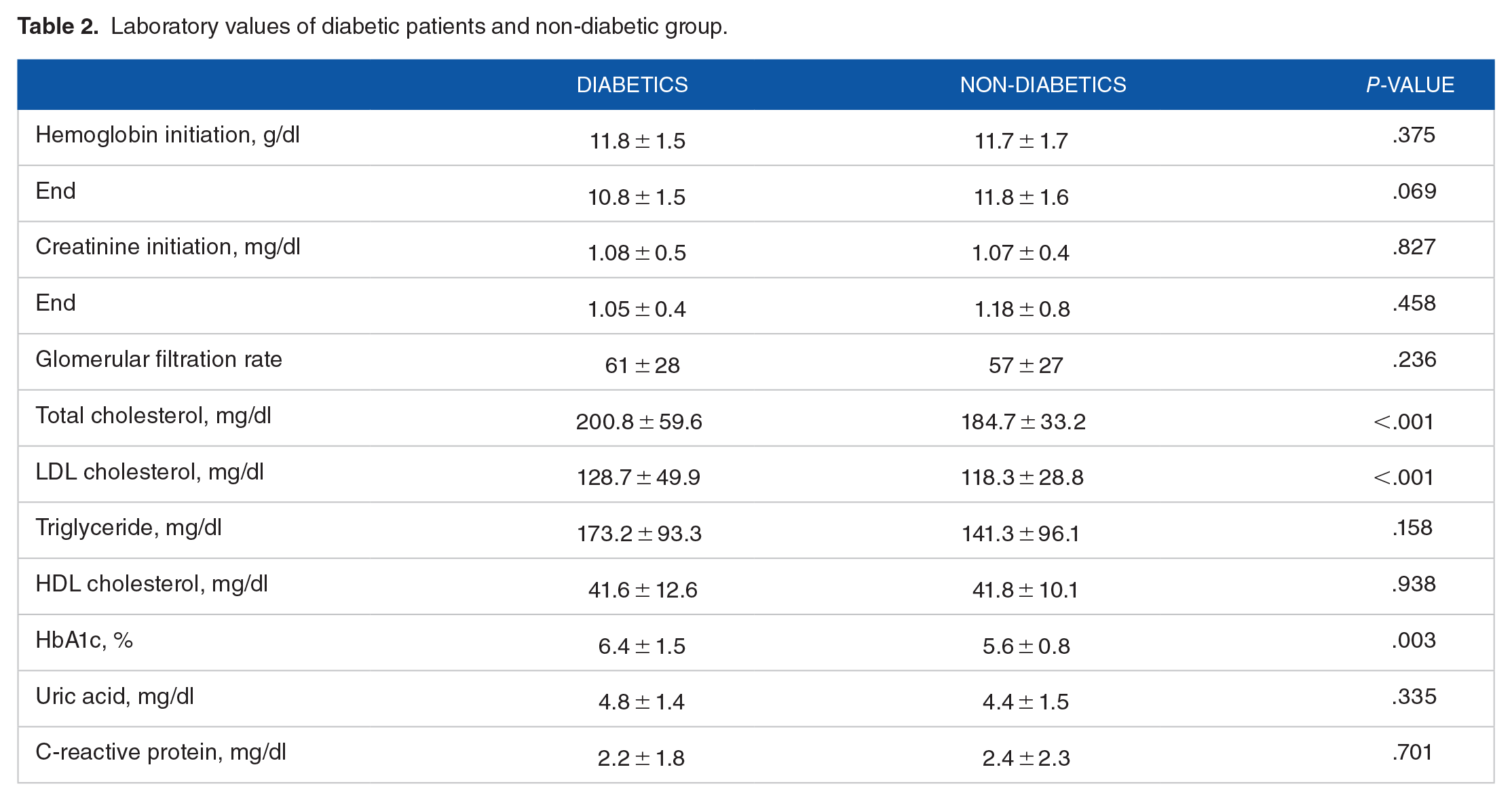
Total cholesterol levels and LDL-C were higher in diabetic patients with the reached statistical significance (P < .001). On the other hand hemoglobin, creatinine, triglyceride, HDL-C, uric acid, and CRP levels were not statistically different (P > .05). Laboratory values are further outlined in Table 2.
Laboratory values of diabetic patients and non-diabetic group.
About 75% of diabetic patients were hypertensive and 21% of them were hyperlipidemic compared with 59% and 7% consecutively in non-diabetic group, both statistically significant (P < .05). Atrial fibrillation was statistically more common in non-diabetic group (P = .022). No other comorbidity had a statistical difference between the 2 groups (P > .05) these results are summarized in Table 3.
Comorbidities in diabetic patients versus non-diabetic group (%).

Anti-diabetic, antihypertensive, aspirin and statin usage were statistically more prevalent in diabetic patients. (P < .001) Most of the antidiabetics which were used were sulfonilureas, metformin and insulin (41%, 42%, and 42%, respectively). Prevalence of other medications had no difference in-between groups. Medication usage is encapsulated in Table 4.
Distribution of most commonly prescribed medications (%).

Abbreviations: ACE-Is, angiotensin converting enzyme inhibitors; DHP-CCBs, dihydropyridine calcium channel blockers; PPIs, proton pump inhibitors; meds, medications; ARBs, angiotensin receptor blockers.
When patients were grouped based on an arbitrary cutoff blood glucose level of 126 mg/dl, there was a non-significant trend towards lower survival in the subjects with higher levels than the cutoff (P = .059). Survival based on glucose levels is charted in Figure 1.

Survival rates of diabetic and non-diabetic groups.
Discussion
We aimed to elucidate the treatment, survival and comorbidities of type 2 diabetic patients aged older than 65 living in nursing homes. The prevalence of type 2 diabetes was reported 16.5% in general population in the recently published Turkish study (TURDEP-2) in Turkey. 15 Our prevalence is in concordance with the results found by Zhang et al in a study in 2004 conducted in nursing homes in the US 1 . But our results are also much higher than 8.8% found by a similar questionnaire type study conducted by Taylor and Hendra. 16 It is also higher than that found by a systematic review conducted by Garcia et al on 20 studies. 17 It can be argued that the causative factor in this difference is the fact that a questionnaire type study such as the one conducted by Taylor et al may be underpowered to detect prevalence whereas the studies chosen to be systematically reviewed by Garcia et al might have been conducted in regions with low diabetes prevalence.
Another characteristic finding of our study was that 61% of diabetic patients were female. This is in concord with the 65% found by a study conducted by Gill et al on nursing home residents in New Zealand and 63.1% by a study by Sjoblom et al on discontinuation of oral anti-diabetics in nursing homes.18,19 The fact that developing more than 6 ailments was more common in diabetics can be explained that diabetes is a confounder and risk factor for infections. The more common usage of more than 4 medications in diabetics can on the other hand be explained by the prescription of oral anti-diabetics and other medications aimed at reducing the CV disease risk conferred by diabetes.
Another important aspect of our study was the continued evaluation of blood glucose levels. Blood glucose levels of diabetic patients were 143.9 ± 62.4 mg/dl at the beginning of our study compared to 123.0 ± 36.8 mg/dl at the end. These were 99.8 ± 20.5 mg/dl and 97.5 ± 18 mg/dl in non-diabetic group concurrently. A study by Lubart et al also confirms our results in diabetic patients with a published fasting blood glucose value at 144 mg/dl. 20
Diabetes is considered a CAD equivalent for the purposes of risk mitigation. This necessitates the fact that the target lipid levels in diabetic patients be much lower than those for the normal population. Lipid levels are especially important in geriatric practice such as people living in nursing homes. McNabney et al 21 found out that nursing home physicians didn’t check lipid levels in 2% of their patients or did so infrequently in 41%. Our study has also shown that diabetic patients had higher total cholesterol and LDL cholesterol levels, as a statistically significant result. The reasons behind this may be related to directly increased blood glucose levels, oxidative stress, insulin resistance, impaired lipid metabolism or an increased tendency towards obesity.
Comorbidities in old diabetics are another subject of importance. Our study has shown that nearly 75% of diabetic patients were also hypertensive, a rate statistically more than non-diabetic group. Travis et al 4 also reported in their study that 69% of diabetic applicants to nursing homes were hypertensive. 18 Same study also demonstrated that 30% had depression and another 26% had CHF. Our study revealed 42% of diabetic patients had concomitant depression and 15% CHF, but this was not statistically significant. Although it is known that diabetes is associated with an increased risk for atrial fibrillation, 22 atrial fibrillation was less prevalent in diabetic patients in our study. But diabetic neuropathy which could possibly mask the cardiac symptoms and diagnosis of atrial fibrillation should be kept in mind in old patients. 23
Nursing home residents older than 65, are on more medications about diabetes or comorbidities. As expected, our study shows that statistically more diabetic patients are on anti-diabetics compared with non-diabetic group. Also, when comparing different groups of anti-diabetic drugs such as metformin, insulin or sulfonylureas; the average prevalence of diabetic patients on them was interestingly about the same. The finding of our study that ACE-I, dihydropyridine CCB, ARB, NSAID, and statin usage is statistically more common in diabetic patients is more than probably due to the fact that recent guidelines necessitating the fact of cardio protection in diabetics are being incorporated into clinical practice by clinicians. The higher prevalence of antihypertensive and statin use in diabetic patients can be also due to higher prevalence of hypertension and hyperlipidemia in diabetic patients.
Nutritional status, quality of life and depressive symptoms and association of diabetic elderly patients are searched in a nursing home in Vietnam.11-13 The study shows nutritional status can prevent the diabetic complication of diabetic elderly patients. 11 The presence of diabetes and comorbidity are responsible for a significant decrease in health-related quality of life. 12 The another study related with depressive symptoms shows that diabetic elderly patients have them more than non-diabetic patients. 13
Yet another important result is the survival rates. In a meta-analysis including 35 eligible study, Nwaneri et al stated that diabetes has 2 fold increased mortality and macrovascular disease was the principal cause of death. 24 Even though our results bordered on but was not less than the accepted level of significance (P = .059), cumulative survival rates were higher in subjects with blood glucose levels less than 126 mg/dl. Considering that our P value fell just short of the traditional definition of statistical significance, we are of the opinion that had our sample size been bigger, we would have obtained a statistically significant result.
Our study is the largest and longest study to date conducted in Turkey. A major limitation of our study was that it was conducted in a private nursing home, where the general care could be described as above far of that considered for the general old population in Turkey. Thus, our results may or may not be valid if generalized for Turkey.
Conclusion
In conclusion we found that about 1 in every 4 nursing home resident was diabetic patient, with an increased prevalence in females. Diabetic patients were also more likely to be polymedicated, have increased levels of glucose, total cholesterol, LDL cholesterol, and blood pressure. The survival rates both at the diabetic and non-diabetic patients were detected similar. Therefore, we suggest that all these values be watched closely throughout their stay and optimized.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MÖ wrote the paper, do teh statistical analyze, AG check the language, sent the paper, YK collect the patients, check the paper.