
Abstract
Aim:
The aim of this study was to analyze prescription patterns and disease control in patients with type 2 diabetes mellitus (T2DM) in nursing home and home care settings in Germany.
Methods:
The present study is based on data from the Disease Analyzer database (QuintilesIMS). Patients with an initial diagnosis of T2DM and documented HbA1c values between January 2011 and December 2015 were included in the analysis. The index date corresponded to the last documented HbA1c value. Patients in nursing homes were matched (1:1) with patients living at home based on age, gender, and dementia diagnosis. The first outcome of the study was the share of use of several antidiabetic drugs in the two different settings. The second outcome was the mean HbA1c value and the proportion of patients with HbA1c values lower than 7% in the two different groups.
Results:
In this study, 4925 individuals lived in nursing homes and 4925 individuals lived at home. The mean age was 80.7 years (SD = 7.7). Prescription patterns differed significantly between nursing home and home care settings: insulin (57.9% vs 41.1%), metformin (46.6% vs 60.5%), sulfonylurea (24.9% vs 34.2%), DPP4 inhibitors (13.4% vs 19.8%), and other antihyperglycemic drugs (7.8% vs 12.1%). In contrast, mean HbA1c values (nursing home: 7.2%; home: 7.2%) and the share of patients with Hb1Ac values lower than 7% (nursing home: 49.1%; home: 50.9%) did not differ significantly between the two groups.
Conclusion:
Overall, the differences in prescription patterns between nursing homes and home care were not associated with significant differences in the management of T2DM.
Keywords
Throughout the world, 9% of adults suffer from diabetes, 90% of whom are affected by type 2 diabetes mellitus (T2DM).1,2 Each year, diabetes is involved in approximately 1.5 million deaths. It is estimated that around 7.2% of adults in Germany are diagnosed with type 2 diabetes (7.0% of male adults and 7.4% of female adults). 1 Therefore, the health and economic burdens associated with this chronic disorder are considerable in this region of the world.
Since the mid-2000s, several studies have found that the prevalence of diabetes is between 11% and 36% in nursing homes.3-10 Unfortunately, the management of this disease remains suboptimal in this setting. In 2010, Bouillet and colleagues discovered that 32% of elderly people hospitalized in French long-term-care homes had HbA1c levels lower or equal to 6.5% and thus were at a particular risk of severe hypoglycemia. 6 These findings were corroborated 2 years later in a study including 88 diabetes residents from three Italian nursing homes whose HbA1c values were well below the recommended targets. 9 More recently, Andreassen et al found that mean HbA1c levels were 7.3% and that 46% of people had HbA1c values lower than 7.0%. 10 Unfortunately, since no work has yet compared HbA1c values in T2DM patients between nursing home and home care settings, no reference is available, and interpreting the previous findings has been difficult.
Therefore, the goal of the present retrospective study was to analyze prescription patterns and disease control in patients with T2DM in nursing home and home care settings in Germany.
Methods
Database
The present study is based on the data from the Disease Analyzer database (QuintilesIMS), which compiles drug prescriptions, diagnoses, and basic medical and demographic data obtained directly and in anonymous format from computer systems used in the practices of general practitioners. 11 The quality of reported data has been monitored by IMS based on a number of criteria (eg, completeness of documentation, linkage between diagnoses and prescriptions).
In Germany, the sampling methods used for the selection of physicians’ practices were appropriate for obtaining a representative database of primary care practices. 11
Finally, this database has already been used in several studies focusing on T2DM.12-14
Study Population
Patients with an initial diagnosis of T2DM (ICD 10: E11) and documented HbA1c values between January 2011 and December 2015 were included in the analysis. The index date corresponded to the last documented HbA1c value. Patients in nursing homes were much older than patients living at home (80.7 vs 74.8 years). The proportions of female patients and of patients with dementia were much higher in nursing homes compared to patients in home care settings (Table 1). To enable the comparison of both cohorts (nursing home vs home care settings), patients were matched (1:1) based on age, gender, and dementia diagnosis.
Baseline Characteristics of T2DM Patients in Nursing Home and Home Care Settings.
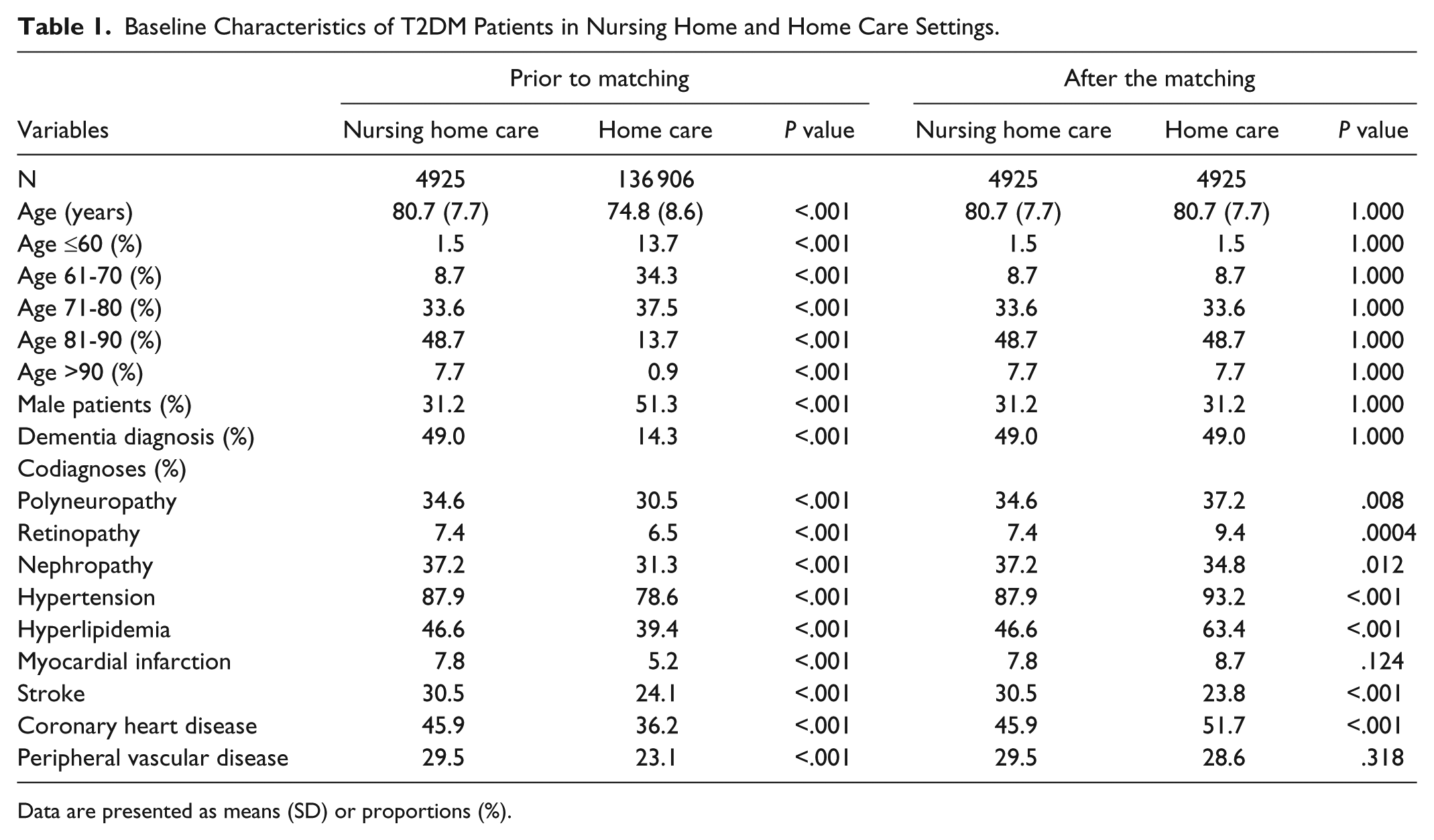
Data are presented as means (SD) or proportions (%).
Study Outcomes
The first outcome of the study were the shares of use of several antidiabetic drugs (insulin: EphMRA ATC A10C; metformin: A10J; sulfonylurea: A10H; dipeptidyl peptidase-4 [DPP4] inhibitors: A10N; and other molecules: A10K, A10L, A10M, A10P and A10S) in the year prior to the index date in nursing home and home care settings. The second outcome were the mean HbA1c value and the proportion of patients with HbA1c values lower than 7% in the two different groups.
Independent Variables
Demographic data included age and gender. Medical data included the type of practice (diabetologist and general practitioner practices) and 10 different comorbidities: dementia (F01, F03, G30), polyneuropathy (E11.4), retinopathy (E11.3), nephropathy (E11.2, N18, N19), hypertension (I10), hyperlipidemia (E78), myocardial infarction (I21, I22, I23), stroke (I63, I64, G45), coronary heart disease (I20, I24, I25), and peripheral vascular disease (E11.5, I73.9).
Statistical Analyses
Descriptive statistics were provided, and differences in patient characteristics (nursing home versus home) were assessed using Wilcoxon tests and chi-square tests. P values < .05 were considered statistically significant. The analyses were carried out using SAS version 9.3.
Results
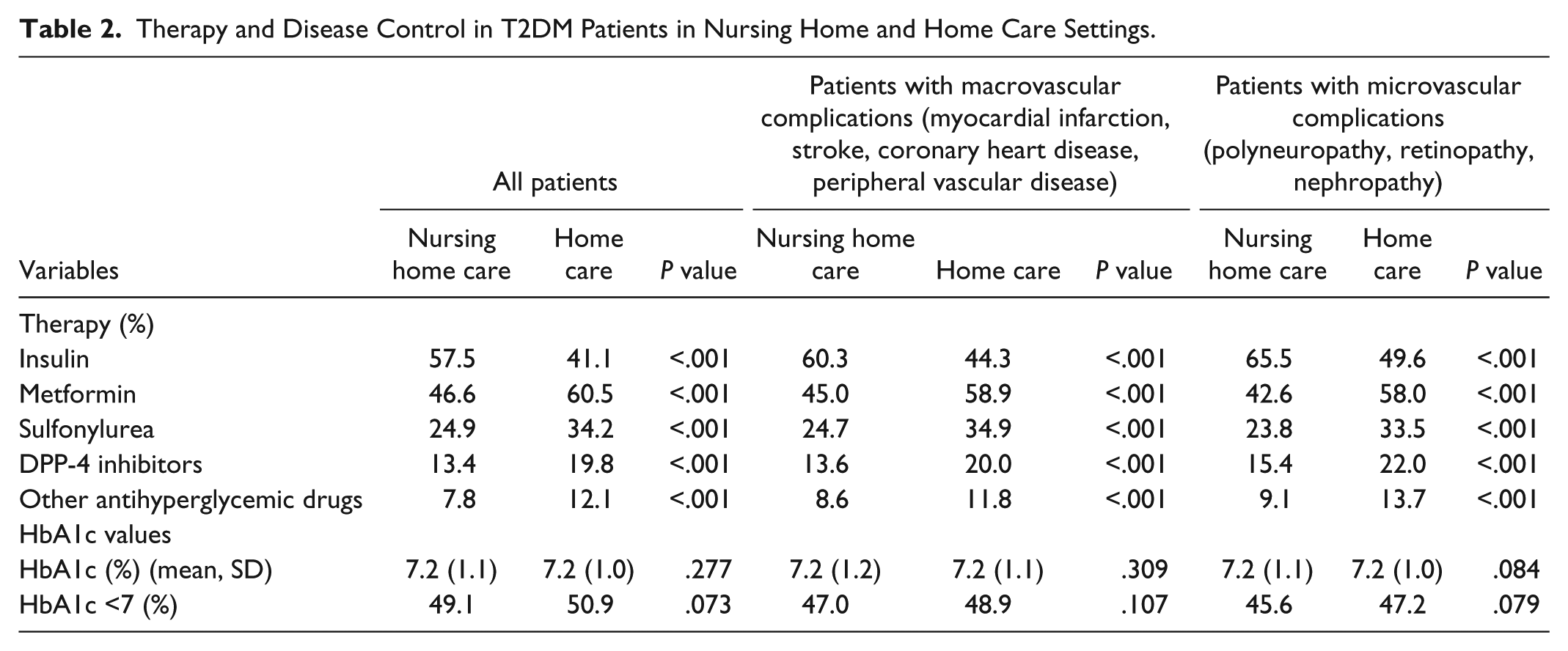
Patient characteristics are shown in Table 1. This study included 4925 individuals living in nursing homes and 4925 individuals living at home. The mean age was 80.7 years (SD = 7.7) in both groups. Of the subjects, 31.2% were men and 49.0% of patients had been diagnosed with dementia. The three most common comorbidities in nursing home and home care settings were hypertension (87.9% and 93.2%), hyperlipidemia (46.6% and 63.4%), and coronary heart disease (45.9% and 51.7%). Prescription patterns and disease control in the two care settings are displayed in Table 2. Prescription patterns differed significantly between nursing home and home care settings: insulin (57.9% vs 41.1%), metformin (46.6% vs 60.5%), sulfonylurea (24.9% vs 34.2%), DPP4 inhibitors (13.4% vs 19.8%), and other antihyperglycemic drugs (7.8% vs 12.1%). In contrast, mean HbA1c values (7.2% and 7.2%) and the share of patients with Hb1Ac values lower than 7% (nursing home: 49.1%; home: 50.9%) did not differ significantly between the two groups. In patients treated with sulfonylurea and insulin, no differences were found in mean HbA1c values and the shares of patients with Hb1Ac values lower than 7%. There were also no significant HbA1c differences in patients diagnosed with macro- and microvascular conditions (Table 2).
Therapy and Disease Control in T2DM Patients in Nursing Home and Home Care Settings.
Discussion
In the present retrospective analysis, which included almost 10 000 T2DM patients from Germany, insulin was found to be more commonly prescribed in nursing homes than in home care, whereas metformin, sulfonylurea, DPP-4 inhibitors, and other antihyperglycemic drugs were less frequently prescribed. Nonetheless, no significant differences were found in the control of T2DM between the two settings, as mean HbA1c values and the share of patients with HbA1c lower than 7% were similar between the two groups.
Although diabetes is frequently found in nursing home residents, it has been suggested that T2DM management remains suboptimal in such settings. In a 2010 study including 100 diabetes patients aged 65 years or over and living in seven French geriatric institutions, it was discovered that almost one-third of the population had HbA1c values lower or equal to 6.5% and were thus at a particular risk of developing severe hypoglycemia. 6 The authors further estimated that the prescription of a specific diet did not have a significant impact on HbA1c values. Later, Basso et al assessed diabetes control in 88 individuals living in three Italian nursing homes. 9 They showed that 41% of patients received insulin, 17% sulfonylureas, 17% metformin, 9% a combination of metformin and sulfonylureas, 11% glinides, and 5% alpha-glucosidase inhibitors. In this analysis, mean HbA1c was 6.5% and the share of patients with HbA1c values lower than 6% was around 30%. More recently, in 2014, Andreassen and colleagues discovered in a sample of 742 long-term care patients from 19 randomly selected nursing homes in Norway that 32% of them were only prescribed insulin, 15% insulin and oral antidiabetics, 27% only oral antidiabetics, and 26% no drugs. 10 Moreover, patients with cognitive alterations were more likely to receive no treatment for diabetes than other patients. Finally, the mean HbA1c value was 7.3% and 46% of patients had HbA1c values lower than 7%. Even if these findings suggest that T2DM management remains suboptimal in nursing homes, no work has yet compared such management between nursing home and home care settings. The present study including 4925 patients living in nursing homes and 4925 patients living at home in Germany showed that the share of patients with HbA1c values lower than 7% was around 50% and similar between both settings. Even if these results must be interpreted with great caution, it is likely that this high share of individuals at a particular risk of hypoglycemia is not explained by the type of residence but rather by other patient characteristics (eg, age, nutrition, or frailty). Another important result of this work is that the prevalence of insulin use was significantly higher in nursing home residents than in patients at home. Such a finding may be explained by the fact that people for whom oral antidiabetics were insufficient are more likely to live in nursing homes than at home. Another explanation is that insulin treatment is favored in nursing homes as the injections are usually given by nurses and may simplify the treatment and management of diabetes. 15
Retrospective primary care database analyses are generally limited by the validity and completeness of the data on which they are based. The present study included several limitations, which should be mentioned at this point. First, no valid information was provided on diabetes duration. Furthermore, the assessment of complications and comorbidities relied solely on ICD codes entered by primary care physicians. Data on socioeconomic status (eg, education and income) and lifestyle-related risk factors (eg, smoking, alcohol, and physical activity) were also lacking. Unfortunately, the documentation of hypoglycemia was also insufficient and could not be used, although hypoglycemia indirectly reflects the quality of diabetes management. Finally, no information on the patients’ dependency or disability was available in the database. The main strength of this study is the number of individuals available for analysis.
Conclusion
Overall, the differences in prescription patterns between nursing home and home care settings were not associated with significant differences in the management of T2DM. Further studies are needed to gain a better understanding of the potential factors that impact the quality of such management in both settings.
Footnotes
Acknowledgements
Professional English language editing services were provided by Claudia Jones, MA, Radford, VA, USA.
Abbreviations
ATC, Anatomical Therapeutic Chemical Classification System; DPP4i, dipeptidyl peptidase-4 inhibitors; GLP-1, glucagon-like peptide 1; HbA1c, hemoglobin A1c; ICD, International Classification of Diseases; SD, standard deviation; SGLT-2, sodium dependent glucose transporter; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.