
Abstract
Background:
Many health systems fail to fully link evidence to decisions and suffer from inadequate ability to respond to priority health needs. Routine data use capacity-building efforts are poorly implemented, lacking integration, quality training, and adequate support.
Objective:
This study was aimed to evaluate the effect of Augmented Capacity Development Interventions (ACDI) strategies on information utilization for decision-making in the Routine Health Information System (RHIS).
Methods:
A two-arm parallel-group cluster randomized controlled trial was conducted across clusters of public health institutions. Baseline data were collected in April 2023, an eight-month intervention was implemented from July 2023 to February 2024, and end-line data were collected in April 2024. Training, supportive supervision, mentorship, recognition, and monitoring and evaluation were the ACDI strategies implemented in this study. The study involved 72 health institutions and 304 health workers. A general linear mixed model analysis was used to assess the effect of the intervention on information utilization.
Results:
The proportion of participants with good information utilization increased significantly from 55.2% at baseline to 82.3% at the end-line among the intervention groups. The ACDI intervention has a significant effect on information utilization (β = 0.19, 95% CI: 0.05, 0.33, P = .006). Moreover, availability of internet service (β = 0.21, 95% CI: 0.04, 0.38; P = .017), culture of information utilization (β = 0.12; 95% CI: 0.02, 0.22; P = .018), ease or skill of data management (β = 0.31, 95% CI: 0.23, 0.39; P < .001) and timeliness of reports (β = 0.27; 95% CI: 0.13, 0.40; P < .001) were predictors that increased information utilization in intervention health institutions as compared to control institutions.
Conclusion:
This study demonstrated that the implementation of ACDI led to a significant improvement in information utilization. These results suggest that the intervention effectively improved information use in the RHIS and support adopting this approach in similar settings.
Trial registration ID:
PACTR202212472091194, registered on 14 December 2022.
Keywords
Introduction
Information utilization is the application of information for decision-making in Routine Information Health System (RHIS), policy formulation and development of health care services. 1 Informed decision-making at all levels of a health system require timely and reliable information for effective and efficient health management.2,3 Availability of quality data allows healthcare workers and managers to make relatively accurate decisions.4,5
Capacity development efforts targeting health workers and health systems are believed to enhance data use for evidence-based decision-making in RHIS. These efforts implement various strategies such as training and feedback-guided supportive supervision. 6 These interventions aim to strengthen capacity at the individual, organizational, and system levels. 7 Through trainings, health workers acquire technical skills to collect, analyze, interpret and visualize data accurately. 8 Supportive supervision provides continuous guidance and helps address challenges in data management. 9 Feedback system reinforces good practices and identifies areas for improvement. 10 On the other hand, strategies like mentorship offer personalized support that builds skills, confidence and promotes accountability. 11 Together, these strategies foster a culture of learning and responsibility, improve data quality, and create an environment where reliable data is consistently used for informed decision making, thereby improving health system performance. 12
In the current health system, different actions are practiced to enhance data quality and information utilization. 13 A variety of routine interventions were implemented to improve knowledge, skill, self-efficacy, changes in practice and health system-level capacity on RHIS management. 7 The common RHIS interventions often fully or partially implemented in current health system in developing countries include competency-based training, supportive supervisions, experience sharing, quality improvement initiatives, and technological adaptations. 14 However, the level and performance of existing health system interventions aimed at promoting effective data use for decision making have been found to be poor. 15
Although various efforts to improve the level of data use have been implemented in developing nations, data use remains poor for informed decision-making. 16 For instance, the RHIS utilization in Africa ranges between 10% and 79%.4,17,18 Similarly, the Health Management Information System (HMIS) data utilization rate in Addis Ababa, Ethiopia was only 42%; Tigray region 43%; 19 Amhara region 53%; and Hadiya Zone of Southern Ethiopia 55%. 20
In the Ethiopian health sector, the RHIS interventions are implemented in the traditional ways, unable to attain the intended targets of health information system. 21 In the country, training coverage on HMIS among health workers remains low, with only 20% to 36% reportedly trained across regions.22 -26 On the other hand, routinely provided trainings are often traditional, lacking practical exercises, planning, follow-up, and other complementary interventions. 27 Even the available training opportunities have overlooked many health workers and leaders involved in data management practice beyond the HMIS unit staff. 28
Health facilities that receive consistent support and feedback on data management tend to improve their knowledge and increase their commitment in using data for decision-making. 29 Supervision should be program-specific and conducted by skilled personnel. However, the RHIS supervision system in Ethiopia is intermixed with other programs, resulting in a lack of focus and emphasis, and is frequently led by untrained personnel. 30 Based on available evidence, the supervision system in Ethiopia is poor, as only 18% of health workers in the Oromia region reported receiving any form of supportive supervision. 31
Sustained staff motivation is a key driver for achieving excellence in patient care, optimizing the operational success of healthcare institutions, improving health outcomes, and enhancing health data management. 32 In Ethiopia, poor human resource management and weak motivation schemes have hindered recording and reporting process in health facilities. 33 Only 53% of professionals reported being motivated to use routine health information. 34 Despite its importance, motivation is often overlooked in interventions aimed at improving health information system performance across the public health sector. 35
Overall, routine health practices of applying capacity development efforts to enhance data use for decision-making have been limited by fragmented implementation, where key actions such as training, mentorship, supervision, and feedback were not effectively integrated. These efforts often lacked the necessary quality, depth, and comprehensiveness, leading to minimal impact on sustainable data use behaviors among health workers and managers.
To address the effectiveness gaps of interventions of data use in the routine health system, we implemented Augmented Capacity Development Interventions (ACDI), which combined complex strategies such as training, feedback-based supportive supervision, mentorship, motivation, and monitoring and evaluation.
Therefore, this study was designed to evaluate the effect of ACDI strategies on information utilization within the RHIS among health workers in public health institutions of Gofa Zone, Southern Ethiopia.
Methods
Study Setting
The study was carried out in public health institutions of Gofa Zone, Southern Ethiopia. 36 A total of 1,510 health professionals are currently working in 26 Health Centers (HCs), 179 Health Posts (HPs), 2 government hospitals, 161 private clinics, and 35 private drug establishments.
Trial Design and Period
A two-arm parallel group, cluster randomization control trial was employed to include the health institutions. Baseline data were collected from April 1 to 30, 2023. An eight-month intervention was implemented from July 1, 2023, to February 29, 2024. The end-line data were collected from April 1 to 30, 2024. The cluster design was developed to enable random assignment of the groups at the institutional level while still taking the individual level into account. Therefore, the possibility of experimental contamination between subjects were minimized through selection and allocation of participants in two groups from the different districts. 37
The Participants
The source population comprises all districts, functional public health facilities, and all health workers (HWs) serving in the Zone, as described in the study setting section. The selected health institutions and the randomly selected HWs from various departments of Gofa Zone were considered as the study population.
Regarding eligibility, functional health facilities and administrative institutions (district health offices) were included in the study. The HWs serving in HMIS units, outpatient departments (OPD), maternal and child health (MCH) departments, performance management team (PMT) members, managers, and health extension workers (HEWs) were included. Conversely, HWs (n = 13) who were lost to follow-up were excluded from the endpoint data collection. Newly established, non-functional, and privately owned health facilities were not be considered. Moreover, HWs (n = 6) who intended to leave their current workplace within the next 8 months were excluded from the initial recruitment process.
Sample Size Determination
The study has assumptions of confidence level of 95%, non-response rate of 10%, 38 intervention to control ratio of 1:1 and power of 90% to determine the sample size.
Sample size was estimated based on 27% of unexposed with the outcomes and 57% exposed with the outcomes. 39 The study had a cluster design with an Intraclass Correlation Coefficient (ICC) of 0.35 and an average cluster size of 4.3, leading to a design effect of 2.16. 40 The final sample was 299 but we used 304 health workers (154 interventions and 150 controls), following intervention to control ratio of 1:1. Calculations used OpenEpi version 3.01 software. 41
Sampling Procedures and Randomization
Sampling Procedures
We conducted a multistage stratified cluster sampling technique. Four and 2 districts were selected from 7 rural and 4 urban districts of the zone, respectively. Based on this, all 18 HCs, 2 hospitals, and a proportionally allocated sample of 46 HPs from the corresponding HCs were selected, resulting in a total of 72 health institutions. Based on this, 37 public health institutions (24 HPs, 9 HCs, 1 hospital, and 3 districts) were selected from intervention arm as well as 35 institutions (comprising 22 HPs, 9 HCs, 1 hospital, 3 districts) were assigned from the control arm. The risk of experimental contamination between the intervention and control institutions was minimized by inclusion of districts and health facilities that are separated by geographical distance (as a buffer zone) in the groups.
Randomization
Sequence Generation
The study stratified districts based on location (urban or rural) and geographical proximity, dividing them into two blocks. The blocks were randomized to either the intervention or control group. The stratified block randomization process aimed to reduce contamination risk, with physical features serving as buffers. Even though some of the control and intervention districts share borders, this connection do not pose a serious risk of contamination because the health facilities themselves are not located closer to each other.
Allocation Concealment
To reduce selection bias and ensure unpredictability in the group assignments, an independent researcher from Arbaminch University in Ethiopia, who was unaware of the districts’ allocation to the intervention or control groups, used sealed envelopes to randomly assign the blocks to each group.
Blinding
The study team aimed to reduce potential bias in the findings by masking assessors regarding which groups received the intervention. Their independence was also assured, as they were recruited from districts not selected in the study. It was not possible to blind the program implementers or the participants because the intervention was openly delivered. However, efforts were made to prevent the control group from knowing what the intervention group received.
Variables
Outcome Variable
As indicated in the Table 2 of result section, the study assessed 16 dimensions of the outcome variable, information utilization using Likert scale metrics ranging from ‘never = 1’ to ‘always = 5.’ The responses for each respondent were first averaged, 42 and these averages were then used to calculate the overall mean for the final analysis. Values below the mean (2.29 and lower) were categorized as ‘poor’, while those above or equal to the mean (2.30 ) were categorized as ‘good’. 40 The same mean cut-point value is applied to both baseline and end-line data to maintain a consistent criterion for categorization, thereby enabling valid comparisons over time.
The Intervention
The study implemented ACDI strategies to enhance data use in RHIS among selected health institutions, improve knowledge, practice, and skills of the managers and experts. The intervention was implemented over an 8-month period, involving 304 study participants across 72 health institutions. It targeted a total of 304 individuals, including selected staff and leaders from OPD (n = 33), MCH (n = 86), HMIS (n = 23), laboratory (n = 18), dispensary (n = 22), and emergency (n = 22) departments, as well as managers of the institutions (n = 26), other PMT members (n = 28), and HEWs (n = 46) from HPs.
Training
The training process was led by intervention team, who had received initial master training and was assigned to deliver the intervention. Training manuals were adapted by these subject matter experts and delivered with the aim of improving data quality and information utilization. The training covered several important topics, including data recording and reporting procedures, the health data quality training module, the information utilization manual, the information revolution roadmap, the HMIS indicator reference guide, and the PMT guideline. Training health workers aimed to enhance their skills and confidence in data management, analysis, visualization, and interpretation, thereby promoting data quality, evidence-based decision-making, and more accurate, timely, and effective use of digital health systems and information within the organization. It also helps to increases their knowledge of data demand and the importance of a data-driven decision-making system. At the beginning of the intervention process, a 6-day initial training for the intervention participants was organized on six relevant modules. These initial training was organized in each of the three intervention districts, targeting the institutions and their respective study participants. Then, assessment-based on-the-job training forums were conducted every 2 months by the intervention team, along with evaluative workshops held at each of the intervention institutions.
Supportive Supervision and Feedback
The supervisory assessments were conducted by experienced experts trained in supervisory skills. During the checklist based assessment process, the culture of information use such as data analysis, data display or visualization, PMT implementation, planning, and performance evaluation was assessed. Guidance and capacity building support were provided in each department of the institutions with the selected intervention participants. Gaps in skills, knowledge, and other areas of data management and information use were identified, and underlying reasons were explored. Tailored on-the-job guidance was designed to address the identified gaps for improvement and strengthen routine practices. Supportive supervision was boosted by reflective oral and written feedback, which helped guide corrective actions among health workers. Joint action plans were designed, progress on previous actions was evaluated, and improvement areas identified based on the assessment findings were highlighted. During the joint supervisory meeting, the checklists were completed, and the findings from the supervision were later communicated through oral feedback sessions held during learning workshops and mentorship process. Monthly checklist guided self-assessments were also implemented by the intervention participants.
Furthermore, the checklist-based supervisory visits are both supportive and primarily facilitative in identifying technical gaps to inform subsequent evaluative workshops meetings and mentorship sessions. Checklist-based supervisory assessments of the data management process were conducted for 1 day every 2 months in each of the 70 intervention health institutions. Overall, a total of four supportive supervision visits were conducted at each intervention institution during the implementation period.
Mentorship
Eight experts were deployed to conduct both the supervisory visits and the mentorship process. These experienced mentors, trained in mentorship skills and data management processes, developed the mentorship modules and led its implementation, with the intervention participants serving as the mentees. The mentorship process is competency based and was guided by findings from checklist-based supervisory assessments, which identified initial and subsequent skill gaps, performance levels, and training needs. During the mentorship, mentors provided hands-on support, coaching, and practical demonstrations, skill support and facilitated discussions on how data is used in decision-making. They also encouraged mentee participation and reflection on routine practices within data-driven decision-making platforms. The mentorship process covered key areas such as data quality assessment, analysis, visualization, decision-making, feedback utilization, and integration into performance reviews, emphasizing practical skills and fostering a culture of routine data use. The mentorship program was held quarterly in each session, with each session lasting 1 to 2 days at each health institution.
Monitoring and Evaluation
In this project, every 2-month review meetings or learning workshops on supervision findings were organized to address data quality and information utilization across all intervention institutions. Monitoring was conducted to ensure the correction and implementation of supervision feedback. Furthermore, Data Quality Assessment (DQAs) of monthly reports and regular review meetings were established and implemented using a data monitoring logbook. A strong monthly data review process, prior to submission to the next reporting level, was assured by revitalizing or establishing a specific PMT platform in each institution and department.
Regarding evaluation, review meetings were held every 2 months throughout the 8-month intervention period. Each workshop lasted 1 day and was conducted in each institution, except for the initial training session. Sessions concluded with the development of an improvement plan to be implemented in the following months to enhance information utilization for decision making.
Recognition
This project involved individual and organizational certification of outstanding performance, appreciating the health workers, departments and institutions by using verbal communication, encouraging the workers to share their successful experience for other institutions, promoting and scaling up their effective intervention approaches. The recognition process was practiced along with learning workshops.
In conclusion, we describe the intervention as ‘augmented’ because substantial modifications were made to conventional routine practices. In this study, the key aspect of the intervention approach that justifies the term ‘augmented’ is the combination of multiple interventions, in contrast to the routine process, which lacks integration of various capacity-building efforts to achieve effective improvement in the RHIS data use. The intervention institutions received all the stated interventions, while the control institutions were given the training modules at the end of the study period. Different standard operating procedures were developed to guide the implementation of each intervention package and its corresponding action points.
Data Collection Procedure
A 3-day intensive initial training was delivered to eight data collectors and three supervisors on data collection protocol. One-day endline data collection training was also conducted. The data were collected with a structured, pre-tested, and standardized questionnaire customized from Performance of Routine Information System Management (PRISM) assessment tools. 43 The Kobo Toolbox was used for data collection process.
Statistical Analysis
Data were exported to Stata 17 for analysis. Descriptive statistics including frequencies, proportions, mean, and standard deviation were computed. The 95% confidence interval was used with P-values.
Regarding the model structure, a General Linear Mixed Effects Model was applied to assess the effect of the intervention over time, accounting for repeated measurements (baseline and end-line) within individual health workers and clusters. We used the intention-to-treat (ITT) approach to handle missing data from 13 participants who were lost to follow-up. This helped us maintain the advantages of randomization and reduce the risk of bias that might arise from participant dropouts. We assumed that the data were missing at random (MAR), based on the nature of the dropouts. Therefore, we applied the default estimation method of the General Linear Mixed Effects Model, restricted maximum likelihood estimation, which leverages all available data points without the need to explicitly impute missing values.
While preparing the manuscript, we carefully adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines, including the extension for cluster randomized trials, to ensure the trial was reported in a clear and standardized manner (Supplemental Material).
Results
Flow Chart
A total of 11 districts in the zone were found to be eligible for inclusion. We used districts as the cluster units for randomization and intervention as well as both health institutions and health workers as units of analysis. Among these clusters, 3 districts were allocated to each of the treatment groups, along with a total of 304 health workers. At end-line, 70 clusters and 291 health workers remained for follow-up and were included in the analysis, as 13 (4.2%) participants and 2 clusters were lost to follow-up for various reasons. However, all 72 clusters and 304 health workers involved at baseline were included in the final analysis, as an ITT approach was applied (Figure 1).

Flow diagram illustrating the progress and involvement of cluster health institutions and health workers throughout the trial process in Gofa Zone, South Ethiopia, 2024 (n = 304).
Participant Characteristics
A total of 304 health workers used for the final units of analysis where 154 participants were in the intervention group and 150 in the control group at baseline. At end-line, 147 and 144 participants remained in the respective group. At the baseline, a total of 194 (63.8%) were males and 239 (78.6%) were selected from urban health institutions. Ten males and 3 females, a total of 13, were lost to follow-up at the end-line. Regarding the current job of the participants, 94 (30.9%) were department leaders and 49 (16.1%) were head of health institutions at the baseline. On the other hand, the study participants have a mean age of 30.07 years with Standard Deviation (SD) of 3.77 and the average work experience of 6.69 years (Table 1).
Characteristics of Study Participants in Public Health Institutions of the Gofa Zone, South Ethiopia Region, 2024 (n = 304).

Abbreviations: SD = Standard Deviation, IQR = Interquartile range, n = sample size, DQA, data quality assessment; HMIS, health management information system; IQR, interquartile range; MCH, maternal and child health; n, sample size; OPD, outpatient department; PMT, performance monitoring team; RHIS, routine health information system.
Information Utilization
A total of 16 dimensions were adapted to compute the overall status of information utilization. The average information utilization score at baseline among participants, measured on a scale ranging from 1 to 5, was 2.29 (95% CI: 2.27, 2.32; SD = 0.20; P = .442) with the intervention group mean score of 2.33 (95% CI: 2.28, 2.37; SD = 0.26) and the control group average score of 2.27 (95% CI: 2.25, 2.29; SD = 0.13)
On the other hand, the mean end-line mean score of the outcome variable was 2.65 (95% CI: 2.55, 2.75; SD = 0.86; P = .005). In this case the intervention group has a mean score of 3.02 (95% CI: 2.85, 3.15; SD = 0.91) and that of the control group has a mean score of 2.27 (95% CI: 2.25, 2.29; SD = 0.61) (Table 2).
The Description of Intervention and Control Group Characteristics Related to the Dimensions of Information Utilization Among Study Participants in Public Health Institutions of Gofa Zone, South Ethiopia Region, 2024 (n = 304).

The overall (repeated measure) mean score of information utilization was 2.47 (95% CI: 2.42, 2.52; SD = 0.64; P (adjusted) < .001), with the intervention group having a mean of 2.66 (95% CI: 2.58, 2.75; SD = 0.74) and the control group a mean of 2.27 (95% CI: 2.22, 2.32; SD = 0.43).
Proportion of Information Utilization
The proportion of respondents with good information utilization was 52.0% (95% CI = 46.37, 57.53; P (adjusted for clustering) = .734) at baseline. This value significantly increased to 64.3% (95% CI = 58.63, 69.61; P = .005) at the end-line.
The baseline good information utilization among the intervention group of 55.2% (95% CI = 45.99, 61.47; P = .540) has significantly improved to 82.3% (95% CI = 75.51, 87.85; P < .001) at the end-line as compared to control groups (Figure 2).

The proportions of good information utilization among the studs groups over time in public health institutions of Gofa Zone, South Ethiopia region, 2024 (n = 304).
Overall (repeated data), good information utilization was observed after the implementation of the intervention, with a significant increase among participants to 58.2% (95% CI: 54.2, 62.1; P < .001), with the intervention group scoring good information utilization rate of 68.8% (95% CI = 63.16, 73.90; P < .001). On the other hand poor information utilization accounted for 41.8% (95% CI: 37.9, 45.9, P < .001).
Information Utilization and Associated Factors
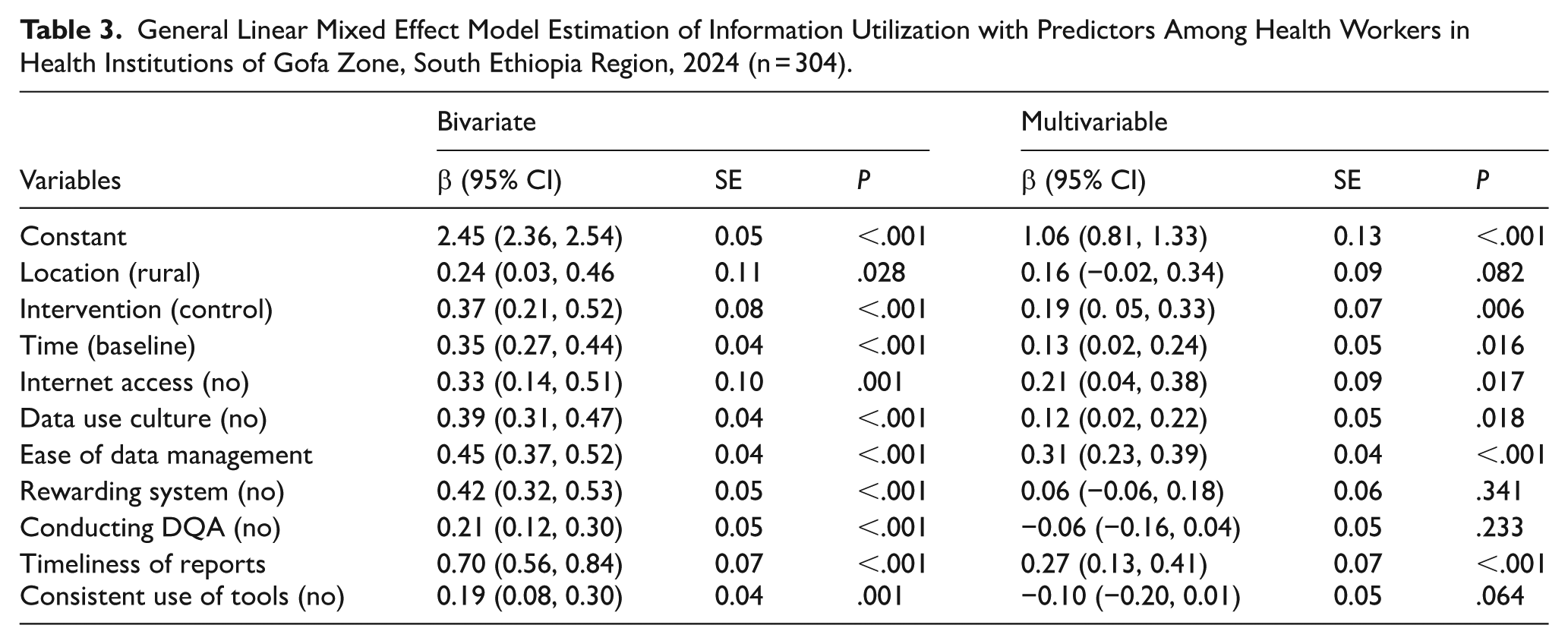
In the bi-variable analysis, variables such as the respondents’ location, the intervention, time, availability of internet access, culture of data use, ease of data management, availability of a rewarding system, conduct of DQA, timeliness of reports, and consistency in using standard recording and reporting tools were significantly associated with information utilization.
On the other hand, the intervention, time, availability of internet access, culture of information use, ease of data management, and timeliness of reports significantly improved information utilization among the treatment group compared to the control group in multivariable analysis.
The intervention and time: the mixed-effects model revealed a significant overall effect of the intervention on information utilization (β = 0.19, 95% CI: 0.05, 0.33, P = .006), after adjusting for clustering and repeated measures. This suggests the intervention group had greater improvement compared to the control group. At the start of the study, the two groups had similar characteristics but significant improvement is observed in the intervention group over time from baseline to end-line (β = 0.13, 95% CI: 0.02, 0.24, P = .016).
Availability of internet service: health institutions with internet access showed significantly better information utilization scores in intervention institutions than in controls (β = 0.21, 95% CI: 0.04, 0.38; P = .017). This suggests that internet access may be an enabling factor for better performance of information utilization in RHIS.
Culture of information utilization and Ease of data management: culture of information utilization in intervention health institutions was found to be significant indicator of information utilization as compared to control health institutions (β = 0.12; 95% CI: 0.02, 0.22; P = .018). On the other hand, ease of data management is a significant predictor of information utilization after the implementation of intervention packages (β = 0.31, 95% CI: 0.23, 0.39; P < .001).
Timeliness of reports: a unit increase in timeliness of reporting increases information utilization by 0.27 units in intervention health institutions compared to control institutions (95% CI: 0.13, 0.41; P < .001) (Table 3).
General Linear Mixed Effect Model Estimation of Information Utilization with Predictors Among Health Workers in Health Institutions of Gofa Zone, South Ethiopia Region, 2024 (n = 304).
Model Fitness
The ICC for the null model was 0.209, indicating that 20.9% of the total variance in the outcome was attributable to differences between health institutions. This justifies the reasonable use of a mixed-effects model to account for clustering and repeated measures. The final model had a lower Akaike Information Criterion (AIC = 880.32) and Bayesian Information Criterion (BIC = 941.76) compared to the null model, indicating a better fit model (Table 4).
The Model Fitness in the Mixed Linear Effect Model Analysis Among Health Workers in Public Health Institutions of the Gofa Zone, Southern Ethiopia, 2024 (n = 304).

Abbreviations: AIC, Akaike information criterion; BIC, Bayesian information criterion; ICC, intraclass correlation coefficient.
Discussion
The aim of this study was to examine the effectiveness of intervention packages on information utilization for decision-making in the RHIS. The proportion of participants with good information utilization increased significantly from 55.2% at baseline to 82.3% at the end-line among the intervention groups. The intervention, time, availability of internet access, culture of information use, ease of data management, and timeliness of reports were significant predictors of information utilization in the treatment group compared to the control group.
The sets of ACDI intervention packages implemented in this study, including training, supervision, feedback, mentorship, monitoring and evaluation, as well as motivation, positively impacted the level of information utilization in the intervention health institutions. A positive change was also observed from baseline to end-line over the 8-month study follow-up period. Similar finding was reported in studies conducted in North Shewa Zone, Amhara Region, Ethiopia, in 2022 following the implementation of district health management team packages.44,45 Combining interventions in cluster trials can be highly valuable, as in many real-world settings, RHIS interventions are not implemented in isolation. These interventions often have a synergistic effect when implemented together, amplifying the overall impact on RHIS performance. Moreover, according to the PRISM framework, RHIS improvements typically require addressing multiple underlying factors including technical, behavioral, and organizational; which should be tackled simultaneously. 46 Additionally, we increased the frequency and intensity of the interventions to help modify routine practices in RHIS programs, aiming to accelerate the desired change in outcomes. This approach might have brought new insights into how effective RHIS performance can be rapidly achieved in the intervention clusters. 6
In this study, internet availability has a significantly higher impact on change in the use of routine data in RHIS in the intervention groups as compared to the control groups. A study in Hadiya Zone, Southern Ethiopia, reported that internet availability was a facilitating factor for information utilization practices in District Health Information System (DHIS2). 47 A qualitative study also highlighted the role of internet resources in supporting health decision-making. 48 Internet availability plays a vital role in improving RHIS performance. With reliable connectivity, health professionals and managers can access real-time data, enabling them to make timely and informed decisions. Platforms like DHIS2 support standardized data entry and reporting, reducing errors from manual processes and improving data accuracy and reliability. In addition, internet access encourages communication and collaboration among health workers, making it easier to share best practices and solve problems together. 49 Finally, strong connectivity is essential for linking various health information systems, offering a more complete picture of health data across different levels and sectors. 48
The culture of information use reflects the habit of using data shaped by the shared values, beliefs, norms, and practices within an organization or health system to support evidence-based decision-making, planning, monitoring, and evaluation. 50 This study revealed that strengthening the culture of information use significantly enhances information utilization in the RHIS. A study from public health centers in Addis Ababa, Ethiopia, highlighted that fostering a culture of information use plays a key role in supporting data-driven decision-making among managers. 51 A similar finding was also reported in health facilities in the Harari 52 and Amharia 53 regions of Ethiopia. A strong culture of information use creates an environment where decisions are consistently guided by data rather than traditional practice. 54 Moreover, a culture that values information motivates health workers and leaders to collect and report data that are accurate, complete, and timely because they see that the data are actually being used. 55 When staffs participate in reviewing and interpreting data, they build their skills and become more actively engaged in the RHIS process. 8
In this study, ease and skill of data management is a significant predictor of information utilization in RHIS. A study conducted in health centers in the Oromia Special Zone of Ethiopia reported a similar finding, highlighting data analysis skills as a key factor influencing information use. 39 A study from Northwest Ethiopia also found that health information utilization was linked to health professionals’ skills in checking data quality. 26 Health workers with strong data management skills are better equipped to collect, record, and enter data accurately, which helps ensure the reliability of the information. 56 They can also make sense of the data by creating summaries, graphs, or indicators that turn raw numbers into useful insights. 57 When data is managed well, reports are prepared and submitted on time, supporting timely feedback and informed decisions. 54 Regular checks on data quality also boost its credibility, building trust and encouraging its use in planning services, allocating resources, and improving program performance. 58
Timeliness of reports was one of the predictors that improved data utilization in the intervention institutions from baseline to end-line. A similar finding is reported from Ethiopia where the healthcare providers who submit reports timely were more likely to utilize routine health information. 39 Timeliness of reports is an important aspect of data quality in RHIS and is closely linked to better data utilization. 59 When reports are submitted on time, they offer up-to-date and relevant information that supports regular monitoring of health services, disease patterns, and program performance. 60 This allows health professionals to make timely and well-informed decisions, such as reallocating resources or addressing service delivery gaps. Consistently timely reporting also strengthens trust in the system and encourages more frequent use of data for planning and oversight, supporting a culture of informed decision making. 61
Strength and Limitation of the Study
The unique aspects of the cluster randomized design contribute significantly to the effectiveness of interventions. First, delivering interventions to entire clusters is often more feasible and tends to be better accepted by participants. This design also helps minimize contamination between intervention and control groups, thereby preserving the integrity of the comparison. In addition, it is particularly well-suited for evaluating multi-component interventions that target health systems, as it enables the assessment of combined effects across different levels of health institutions. The design effectively accounts for group-level influences, an important consideration in settings where information use is strongly shaped by institutional factors.
However, there is geographic contact between some of the intervention and control districts in this study, making them vulnerable to contamination, even though the health institutions are located far apart. In the sample size calculations, we assumed equal cluster sizes; however, in practice, the cluster sizes were not equal.
Conclusion
This study demonstrates that the implementation of ACDI over time has led to a significant improvement in information utilization among the intervention clusters compared to the control clusters. Availability of internet access, culture of information use, ease of data management, and timeliness of reports are factors significantly improved information utilization among the treatment group compared to the control group. Collaborating with telecom stakeholders to expand internet infrastructure in health facilities, promoting a culture of information use, and building the capacity of health workers in data management and timely reporting are potential strategies for improving information utilization within the RHIS. These findings suggest that the intervention is effective in enhancing information use in the RHIS and provide evidence to support the adaptation of this strategy in similar settings.
Supplemental Material
sj-docx-1-his-10.1177_11786329251381429 – Supplemental material for Effect of Augmented Capacity Development Interventions (ACDI) on Information Utilization for Decision-Making in the Routine Health Information System in Public Health Institutions of Gofa Zone, Southern Ethiopia: A Cluster Randomized Controlled Trial
Supplemental material, sj-docx-1-his-10.1177_11786329251381429 for Effect of Augmented Capacity Development Interventions (ACDI) on Information Utilization for Decision-Making in the Routine Health Information System in Public Health Institutions of Gofa Zone, Southern Ethiopia: A Cluster Randomized Controlled Trial by Bedilu Kucho Doka, Keneni Gutema Negeri, Abebaw Gebeyehu Worku and Dejene Hailu Kassa in Health Services Insights
Footnotes
Acknowledgements
We would like to thank Hawassa University, College of Health and Medical Sciences, School of Public Health, and the former Southern Nations, Nationalities, and Peoples’ Regional Health Bureau for providing us with the opportunity to conduct this study. We also extend our appreciation to the Doris Duke Charitable Foundation (DDCF) for funding the data collection process of this study.
Correction (November 2025):
This article has been updated to include the “Acknowledgments” section heading in the end matter.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. Before implementation of the intervention, the an official ethical approval letter has been received from the Institutional Review Board of the College of Health Sciences, Hawassa University with the Reference No. of IRB/183/14 and date 08/06/2022. Permission letters were obtained from the SNNP Regional Health Bureaus. Further permissions were secured from each zonal health department, district health offices and health facilities during the initial data collection process. The study protocol was registered on 14 December 2022 at the Pan African Clinical Trial registry with ID number of PACTR202212472091194.
Consent to Participate
Written informed consent was obtained from all subjects involved in this study. Participants were informed that their involvement in the study was completely voluntary and that their confidentiality would be strictly protected. They were informed that they could choose to stop participating at any time without willing to provide a reason. They were also assured that no personal identifiers would be collected, and only the research team would be aware of their participation in the study.
Consent for Publication
Not applicable.
Author Contributions
BK, KG, AG, and DH designed the study, performed the analysis, interpreted the results, and wrote or revised the manuscript. All authors agree to be accountable for the content of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The fieldwork of this study was supported by the Doris Duke Charitable Foundation (DDCF) through grant to Hawassa University (Grant Number: 2017187). The funder supported the fieldwork component of the study. The funder had no role in the design of the study, data collection, analysis, write-up or publication of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study can be obtained from the corresponding author upon reasonable request by authorized body.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.