
Abstract
Strengthening data quality in the routine health information system is vital for the performance of health service outcomes. However, implementation of the routine interventions to improve data quality in the existing health system has been found inadequate two in Ethiopia. This study was aimed to examine the effect of Augmented Capacity Development Interventions (ACDI) on the performance of data quality in the routine health information system. A arm, parallel group, cluster-randomized control trial was implemented from July 1, 2023 to February 29, 2024. Baseline data were collected from April 1–30, 2023, and end-line data from April 1–30, 2024. The cluster design was employed as it allows for minimizing information contamination. The study included 72 health institution clusters and 304 health workers (154 intervention and 150 control arms). The implemented interventions include training, supportive supervision, mentorship, and recognition. General Linear Mixed Model was applied for analysis. The mean score for data quality perception improved from 2.32 at baseline to 3.13 at end-line (95% CI: 3.05, 3.21; P < .001). The data quality practice has significantly improved after the implementation of the ACDI packages (β = .17; 95% CI: 0.05, 0.30; P = .007), ease of data management (β = .14; 95% CI: 0.07, 0.22; P < .001), information use (β = .15; 95% CI: 0.08, 0.23; P < .001), and the combined effects of encouragement and training (β = .44; 95% CI: 0.23, 0.65; P < .001) were significant predictors of the change in the data quality. The ACDI packages implemented in this study effectively influenced data quality improvement. Key predictors of data quality practices included an encouraging system, ease of data management, written guidelines, supportive supervision, and training. Therefore, the interventions are recommended to be adapted and scaled up.
Keywords
● Routine data quality interventions have been ineffective in health systems. The performance of existing health system interventions in improving data quality has been found to be weak in the developing world.
● Capacity development efforts improved data quality performance. The interventions implemented in this study, including training, supportive supervision, mentorship, recognition, and monitoring and evaluation, contributed to enhancing data quality practice.
● Capacity Development Efforts are recommended strategies to improve data quality. Providing training for all groups of managers and health workers, integrating RHIS training with encouragement system, enhancing the data management skills of health workers and cultivating a culture of information use are suggested interventions to improve data quality practice in health institutions.
● Scale up the interventions. The ACDI strategies implemented in this study could be adapted and implemented in the region or in comparable settings with limited resources to strengthen data quality practices.
Introduction
Routine health information system (RHIS) is the process of collection, interpretation, utilization, and dissemination of routine health data targeted to improve health system performance and health service outcomes. 1 Data quality in health is a multifaceted concept commonly expressed in the dimensions of data accuracy, completeness and timeliness to generate reliable information for decision making process. 2 The ultimate purpose of a RHIS is to produce quality information to be presented for an evidence-based decision making process. 3
In low- and middle-income countries, as revealed by scientific evidence, the overall health data quality was much below the expected national standard.4 -6 In these countries, the performance of routine health data is challenged by poor data management skills, lack of commitment from managing bodies, shortage of monitoring and evaluation system, inadequate infrastructure, and shortage and high turnover of skilled staff.7 -9 Therefore, the performance of existing health system interventions to enhance data quality in RHIS has been found to be ineffective in the developing world. 10
Most studies in developing nations reported that the rate of routine data quality was far below the World Health Organization (WHO) standard of 90%.10 -12 The completeness rate of District Health Information Software, version 2 (DHIS2) data was only 60% whereas under-reporting ranges between 10% to 60% according to a study in Nigeria. 10 Data quality assessment in Mali indicated that the rate of data accuracy at the health facility level was 45% and timeliness of 27%. Data accuracy was 68% at the regional and 54% at the central levels. 12
In the Oromia region of Ethiopia, data timeliness was 70%, completeness was 86%, and accuracy was 48%. 13 In Southern Ethiopia, ANC 4 visits, postnatal care, and full immunization were over-reported by 24%, 21%, and 16%, respectively. 14
There is no individual intervention that could be operated separately to enhance the quality of data in RHIS, but the implementation of the combination of interventions is recommended to assure high quality of health data. 15 A survey in Pakistan revealed that data accuracy has increased from 40% to 75% after implementation of DHIS platform as intervention.16,17 A study in Nigeria revealed improvements in data quality metrics after implementation of interventions. Accordingly, report completeness rate has improved from 72% to 82%, timeliness increased from 60% to 72%, the report content completeness increased from 62% to 68%. 10
A study in Northwest Ethiopia reported that data consistency has improved from 84.0% to 99.5%, data recording completeness from 69% to 96%, and that of report timeliness increased from 66% to 100% after implementation of intervention packages comprising training, supportive supervision and feedback provision. 18 However, the study addressed only one primary hospital of the area where its representativeness is debatable.
Limited previous intervention studies were available on data quality in RHIS. Even though few studies were conducted previously, the interventions implemented were not comprehensive, with many focusing on just a few packages, such as training and guideline provision. These studies were done only on a single or very few facilities or districts; therefore, their representativeness is questionable. Still, other studies had design-related limitations such as a lack of control groups and inability of considering variation of the nature of the outcome among health institutions.
Therefore, this study aimed to evaluate the effect of Augmented Capacity Development Interventions (ACDI) on the performance of data quality in the RHIS among health workers in public health institutions of Gofa Zone, Southern Ethiopia region.
Methods
Study Setting
The study was carried out in health institutions of Gofa Zone, South Ethiopia region. According to the central statistical agency of Ethiopia, the current population of the Zone is approximately 713,854. Among these, 357,359 (50.1%) are men, and 356 495 (49.9%) are women, with a total of 145,684 households. A total of 1510 health professionals are deployed in 11 districts, 2 governmental hospitals, 26 health centers, 179 health posts.
Trial Design
A two arm, parallel group, cluster randomized controlled trial design was adopted. This design was selected in order to minimize experimental contamination between groups as the intervention was implemented at group level. The baseline data were collected from April 1 to 30, 2023. The intervention was implemented from July 1, 2023 to February 29, 2024. The end-line data were collected from April 1 to 30, 2024.
The Participants
The source population comprised all districts, public health facilities, and health workers existing in the zone. Randomly selected health institutions and health workers constituted the study population.
Eligibility
Inclusion Criteria
Administrative district health offices and functional health facilities, including hospitals, health centers, and health posts were included. All health workers, including those serving in different departments, health posts, and heads of health institutions were included in the study.
Exclusion Criteria
Newly established (2 health posts) and privately owned health facilities were not considered in this study. The health workers who were not available during baseline data collection (5 health workers) and who intended to leave the institution within 8 months prior to the baseline data collection (6 health workers) were also excluded.
Sample Size Determination
The study applied the assumptions of confidence level of 95%, marginal error of 5%, and intervention to control ratio of 1:1 to determine the sample size. The sample size was calculated by considering the percent of data quality in comparison group of 33%. 19 Power of 90% was assumed to detect 30% difference in rates between the two groups. Since the study was a cluster design, Intra-Cluster Correlation Coefficient (ICC) of 0.35 and average cluster size of 4.3 were utilized from previous related study. 20 The ICC affects sample size by accounting for similarity within clusters and ensuring adequate statistical power. It is usually informed by prior studies, or if these are unavailable, by pilot data or expert judgment, with a conservative estimate chosen to avoid underestimating the design effect. In this study, the design effect of 2.2 and non-response rate of 10% was considered. Therefore, a total of 309 health workers of both groups were targeted to be recruited from 72 health institutions including 6 districts, 2 hospitals, 18 health centers and 46 health posts. However, in the baseline, 5 respondents were non-respondents, and 13 were lost to follow-up in the endpoint data collection.
Sampling Procedures and Randomization
A multistage stratified cluster sampling technique was employed to select study institutions. The zone has 11 districts (7 rural and 4 urban). First, the rural-urban stratification of the districts was implemented. Then, 4 from 7 rural districts (Demba Gofa, Zalla, Gezegofa and Melokoza) and 2 (Sawla and Laha) from 4 urban districts of the zone were selected by simple random sampling technique. The districts were selected with all their respective health facilities. Based on this, 18 health centers and 2 hospitals from selected districts were considered for the study. Additionally, a total of 46 health posts were proportionally allocated from each of the corresponding health centers. Regarding the groups, 2 randomly selected rural districts, Geze Gofa and Demba Gofa, as well as 1 urban district (Sawula) with all their respective facilities were included under intervention group. Therefore, a total of 37 health institutions clusters were included under the intervention institutions that constituted 24 health posts, 9 health centers, 1 hospital, 2 rural and 1 urban district. On the other hand, 2 randomly selected rural districts (Zalla and Mello Koza) and 1 urban district (Laha) with their respective health facilities including 22 health posts, 9 health centers and 1 hospital were the part of overall 35 control institutions. It is based on the intervention to control ratio of 1:1. Regarding the selection of health workers, the heads of the health institutions and departments along with randomly selected participants from the Outpatient Department (OPD), Maternal and Child Health (MCH), emergency, dispensary, laboratory, Health Management Information System (HMIS) departments and office management were included. Health workers were recruited at baseline, before the randomization of clusters into groups was carried out.
Allocation Sequence, Concealment and Blinding
Sequence Generation
Before the implementation of the randomization process, districts were first stratified by location type (ie, urban or rural). Then, to reduce the risk of experimental contamination, districts were allocated using the block randomization procedure. Three (1 urban and 2 rural) adjacent and contiguous districts were grouped into 1 block and the other 3 (1 urban and 2 rural) districts were sorted in to the other block. Finally, the blocks were randomly selected and allocated into either intervention or control groups. The 2 blocks of the districts were separated geographical buffers of unselected districts, special zones and rivers. Although there is still some territorial connection between certain control and intervention districts, the risk of contamination is not significant, as there is no physical proximity between the clusters.
Allocation Concealment
In order to minimize the selection bias and ensure unpredictability, the assignment of the blocks to the either arm has been done by an independent researcher from Arbaminch University of Ethiopia, who was unaware of the study group assignments, applied sealed envelopes for the group allocation.
Blinding
In order to avoid any bias on study results, the outcome assessors were withheld about the interventions provided as they were deployed from unselected districts. The blinding of program implementers and study participants was not possible as they provide and receive the open-level trial. However, the control groups were kept unaware of what the intervention groups received.
Variables
Outcome Variables
Data quality is a multidimensional construct expressed in terms of timeliness, accuracy, and completeness.
Completeness was explained by report completeness and completeness of indicator data.
Timeliness of reporting was determined by analyzing health institution summary reports that were remitted to the next level within a predetermined reporting period based on the Ethiopian national reporting schedule. 25 Report timeliness was also calculated only for districts and health centers.
Data Quality Practice
Data quality practice is the primary outcome in this study. It is a composite construct measured by the level of agreement on 11 items using a Likert scale format, where a score of 5 represents ‘Strongly Agree’, 4 represents ‘Agree’, 3 represents ‘Neutral’, 2 represents ‘Disagree’, and 1 represents ‘Strongly Disagree’. In this case, the perception of respondents about how their institution performs in terms of data quality is assessed.
The items used to measure this construct include: provision of quality healthcare and generation of sufficient data, quality of documentation, accuracy in data compilation, effectiveness of data communication; efficiency of data collection, sharing, and reporting systems; appropriateness and accuracy of data for quality decision-making, timeliness of reporting, assurance of completeness of information in records and reports, conducting data quality reviews before reporting, and promotion of integrity in data management.
The 11 item scores for each respondent are averaged to produce a single value, and finally, the mean of these scores is computed, treating the variable as continuous.
Predictors like perceived ease of data management, level of information utilization, supervision quality and perceived level of job satisfaction were also computed using the same procedure as data quality practice.
The Intervention
The study implemented the Augmented Capacity Development Interventions (ACDI) packages that were targeted to improve data quality in RHIS among selected health institutions. The following interventions were implemented to improve the knowledge, practice, and skill of the experts and the system to produce quality data.
Training
Training process was led by intervention team members, who had received initial master training and were assigned to deliver the intervention. The training of the intervention community members, selected staff from different departments, comprising HMIS officers, managers, Performance Monitoring Members (PMT) members, and health extension workers was carried out. The training was organized in their respective institutions. At the beginning of the intervention process, a 6-day initial training for the intervention community was organized on 6 relevant modules. Then assessment-based on-the-job training workshops were conducted in every 2 months by the intervention team.
Supportive Supervision and Feedback
In this study, checklist based supervisory assessment and action oriented oral and written feedback system on data management process were implemented for 1 day per every 2 month period. A total of 4 supportive supervision visits were delivered for each intervention institution during the 8 month implementation period.
Mentorship
The mentorship program was organized in every 3 months each for 1 to 2 days. Trained experts, from the members of the intervention team, were the mentors and the intervention communities were the mentees. Close observation, guidance and spot assistance based on initial and subsequent assessment findings were addressed and forwarded for discussion.
Monitoring and Evaluation
In this project, every 2-month review meetings and learning workshops based supervision findings were organized following the second day of the supervisory assessments. Monitoring was implemented in an ongoing process by the institution representatives for the correction and implementation of supervision feedbacks as part of self-assessment.
Recognition
This project involved individual and organizational certification of outstanding performance, appreciating the workers, departments and institutions by using verbal communication, encouraging the workers to share their successful experience for other institutions, promoting and scaling up their effective intervention approaches. The recognition process was practiced along with learning workshops.
We state that the intervention is augmented, as substantial modifications were made to conventional routine practices. Overall, the intervention institutions have received all the stated interventions while the control institutions were given the training modules at the end of the study period. Different Standard Operating Procedures (SOPs) were established for the implementation of each intervention packages and corresponding activities (Figure 1).

Schematic overview of the ACDI framework for improving data quality in RHIS.
Data Collection Tools and Procedures
A total of 8 data collectors and 3 supervisors were deployed for data collection after 3-day intensive training at the baseline. The questionnaire was designed in English version and translated to the Amharic language for better understanding of respondents. The data were collected with a structured, pre-tested, and standardized questionnaire customized from Performance of Routine Information System Management (PRISM) assessment tools. 26
Although the questionnaire was standard, it was pretested on 33 health workers from Uba Debretsehay, an adjacent district with similar characteristics to the study sites, to ensure clarity, relevance, and reliability. The pretest helped identify unclear or inconsistent items, assess the understandability and acceptability of the questions, and determine the average time required to complete the questionnaire. Internal consistency was confirmed using Cronbach’s alpha, with all variables above 0.70. Specifically, data quality practice scored 0.75, data accuracy 0.74, data completeness 0.89, information use 0.82, data management skill 0.79, data use culture 0.75, and data accuracy perception 0.93.
The same questionnaire was used for baseline and end-line, but the end-line data collection included only necessary questions, excluding less relevant items like socio-demographic characteristics. The data were collected using face-to-face interview questionnaires, document review templates, physical observation checklist that were also used for organizing surveys, reviewing documents and conducting observations. An electronic data collection process has been implemented using the Kobo Toolbox.
Quality Control
Data collectors and supervisors have received an intensive training on data collection protocol during both baseline and endline data collection. We have adapted a standard PRISM assessment tools 26 in designing the questionnaire for the study. During the manuscript writing process, we thoroughly followed the Consolidated Standards of Reporting Trials (CONSORT) with Extension to Cluster Randomized Trials to ensure a standard reporting process. 27 The guideline was adopted from the EQUATOR Network to promote transparency and completeness, and all recommended items were completed and submitted as a Supplemental File.
Statistical Analysis
Data were exported to Stata 17 for analysis. Descriptive statistics including frequencies, proportions, mean, and standard deviation were computed. The 95% confidence interval was used.
Repeated measures analysis was conducted using a General Linear Mixed Effects Model regression. Variables with a P-value of less than .25 in the bi-variable analysis were entered into the multivariable regression analysis. A P-value of less than .05 in the multivariable regression analysis were reported to identify predictor variables significantly associated with the outcome variable. 28 We applied the intention-to-treat (ITT) approach to account for missing values from 13 participants lost to follow-up, in order to preserve the benefit of randomization and prevent bias caused by dropouts.
Results
Participant Flow
During the baseline data collection, a total of 304 participants (154 intervention and 150 control) were surveyed from 72 health institutions (37 intervention and 35 control). However, for the end-line data collection, a total of 291 health workers participated, resulting in a loss to follow-up of 13 (4.2%) participants. On the other hand, 70 health institutions were included in the final data collection, as 2 health extension workers from 2 institutions (health posts) were lost to follow-up (Figure 2).

Flow diagram illustrating the selection procedure for health workers in public health institutions of Gofa Zone, Southern Ethiopia, 2024.
Characteristics of the Study Participants
About half (50.5%) of the participants who completed the follow up were from the intervention institutions. Among the 291 study participants who completed the follow up, 184 (63.2%) were males and 227 (78.0%) were from rural health institutions. The average age of the total participants was 30.05 years (SD = 3.81), while the median work experience was 6.16 years (SD = 3.70). At baseline, 73.3% of the intervention group and 59.1% of the control group had a Diploma, compared with 59.9% and 72.9% at end-line, with no significant differences between groups at either time point. Overall, no significant baseline differences were found in any predictor variables between the intervention and control groups (Table 1).
Characteristics of Study Participants Among Health Institutions of Gofa Zone, South Ethiopia Region, 2024.

MCH = maternal and child health; HMIS unit = health management information system unit; OPD = outpatient department; PMT = performance monitoring team; SD = standard deviation; DQA = data quality assessment; RHIS = routine health information system.
Data Quality Dimensions
Report Completeness and Report Timelines
At the beginning of the study, the average report completeness of the health institutions was 96.17% (95% CI: 93.40, 97.50; P = .065), with the intervention institutions at 98.75% and the control institutions at 93.58% and showed no significant difference between groups at baseline. By the end of the study, no significant change was observed over time, with report completeness at 92.70% (95% CI: 85.20, 100.20; P = .146), with the intervention institutions at 98.12% and the control institutions at 87.28%. However, the overall average report completeness showed a significant difference between the groups, with a rate of 94.43% (95% CI: 90.60, 98.27; P = .041), corresponding to a practical mean difference of 8.01% between the intervention group (98.44%) and the control group (90.43%) (Figure 3).

Report completeness among health institutions in Gofa Zone, Southern Ethiopia, 2024 (n = 24).
Regarding report timeliness, the result significantly improved from 53.30% (95% CI: 34.10, 72.60; P = .627) at baseline to 76.50% (95% CI: 63.20, 89.50; P = .003) at end-line, showed a practical improvement of 23.20% over time. Although the overall comparison between groups was not statistically significant, the overall mean timeliness was 64.91%, with 73.33% in the intervention group compared to 56.50% in the control group, corresponding to a practical average difference of 16.83% (Figure 4).

Report timeliness among health institutions in Gofa Zone, Southern Ethiopia, 2024 (n = 24).
Data Accuracy and Data Completeness
Data completeness in health institutions showed minimal change over time, from a baseline of 93.57% to an end-line score of 93.40% (95% CI: 90.51, 96.28; P < .001). Overall, the treatment groups demonstrated a practical difference of 93.52, with an average of 99.14% in the intervention institutions compared to 87.89% in the control institutions, corresponding to a mean difference of 11.25%.
On the other hand, data accuracy increased from 89.40% at baseline to 95.63% at end-line (95% CI: 92.82, 98.45; P = .060), which reflected a practical improvement of 6.23% in the mean scores. Similarly, although there was no statistically significant difference between groups, the intervention institutions averaged 95.50% compared to 92.53% in the control institutions, corresponding to a mean difference of 2.97% (Figure 5).

Data completeness and accuracy among treatment groups in health institutions of Gofa Zone, Southern Ethiopia, 2024 (n = 72).
Data Quality Practice Score
At baseline, the mean score for data quality perception was 2.32 (95% CI: 2.25, 2.35; SE = 0.02), with 59.5% of respondents scoring at or above the average, categorized as having a ‘good’ perception of data quality practice. At end-line, 77.3% of respondents had a good perception, with a mean score of 3.13 (95% CI: 3.05, 3.21; P < .001), thereby reflected a practical improvement of 0.81 in the mean score (Figure 6).
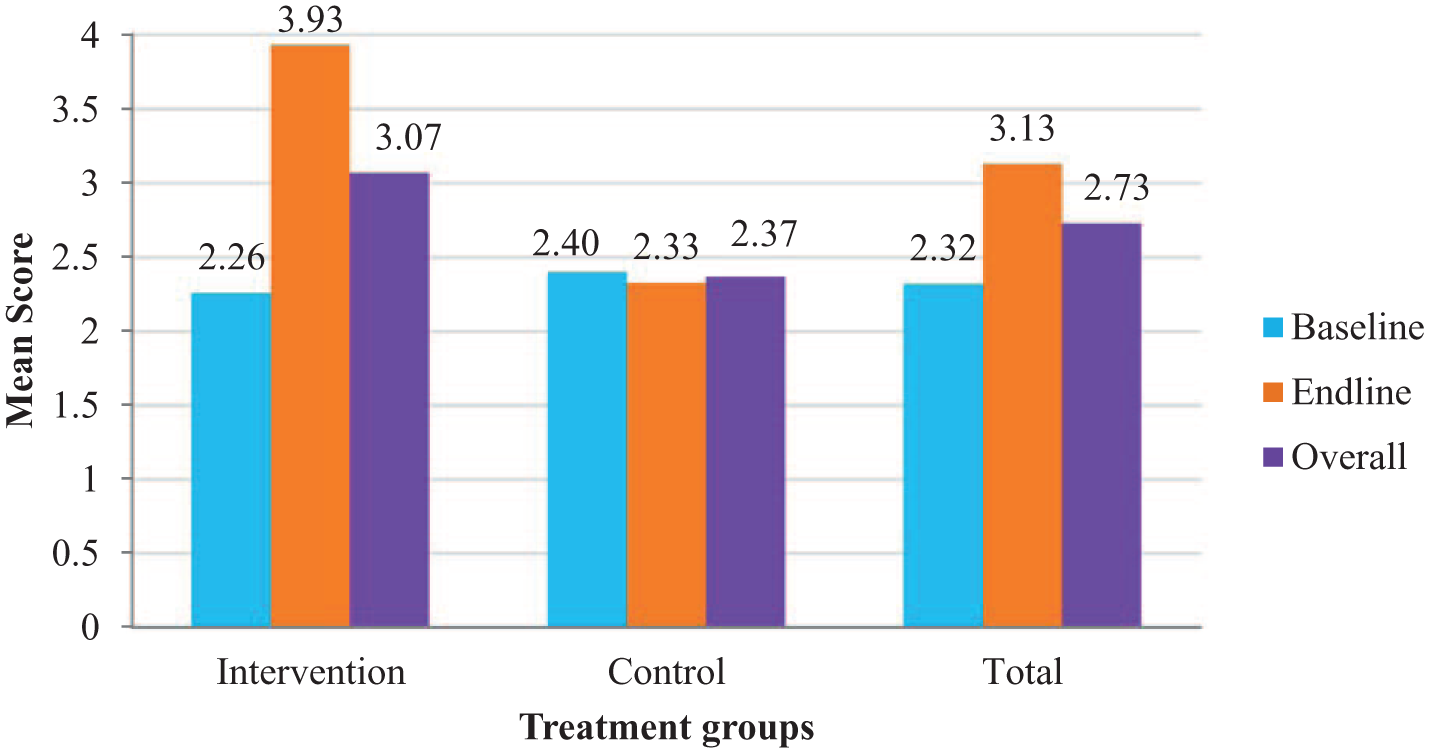
The mean of data quality practice score from baseline to end-line in the treatment groups among health workers in public health institutions of Gofa Zone, Southern Ethiopia, (n = 304).
Data Quality and Associated Factors
In the bi-variable analysis, treatment group, time, encouraging system for good performance, ease of data management, level of information use, availability of written guideline on RHIS, receive supportive supervision on RHIS, training on RHIS, the combined effects of encouraging system for good performance and training on RHIS, availability PMT system, receive feedback on RHIS, consistently use standard tools, and availability of rewarding system were significantly predicted the change in the data quality practice. However, in multivariable analysis predictors like treatment group, time, encouraging system for good performance, ease of data management, level of information use, availability of written guideline on RHIS, consistently use standard tools and the combined effects of encouraging system for good performance and training on RHIS, were significantly predicted the change in the data quality practice among the treatment groups.
General Linear Mixed Effect Model Estimation of Data Quality Practice Score with Predictors Among Health Workers in Health Institutions of Gofa Zone, South Ethiopia Region, 2024 (n = 304).

Model Fitness
Comparing Akaike’s Information Criterion (AIC) and Bayesian Criterion (BIC) between the null and final models provided an indication of model fit. Lower values of the information criteria from the null to the final model suggested better-fitting models. On the other hand, the ICC measured the proportion of the total variance explained by the grouping factor. A higher ICC value (>5%) indicated that the grouping factor has a significant impact on the outcome variable (Table 3).
Model Fitness in the Mixed Linear Effect Model Analysis Among Health Workers in Public Health Institutions of the Gofa Zone, Southern Ethiopia, 2024 (n = 304).

AIC = Akaike’s information criterion; BIC = Bayesian criterion; ICC = intraclass correlation coefficient.
Discussion
The aim of this study was to evaluate the effect of capacity development interventions on the performance of data quality in the RHIS among public health institutions. At baseline, report completeness, timeliness, data completeness, and accuracy were well balanced across groups. By end-line, timeliness and data completeness improved over time, while report completeness and data completeness showed significant improvement in the intervention groups compared to the control groups. In the regression analysis, the overall data quality score changed from baseline to end-line and demonstrated a significant difference among the groups. The intervention groups, time, encouragement for good performance, availability of written RHIS guidelines, and perceptions of ease of data management and information use were significant predictors of data quality practices. In addition, the combined effects of training and the encouragement system for good performance, showed significant changes from baseline to end-line and between the intervention and control groups.
Regarding data quality dimensions, report timeliness improved from baseline to end-line among the treatment groups, even though it did not meet the national MOH standard of 90%. This result aligns with a study conducted at Metema Primary Hospital in Northwest Ethiopia, where report timeliness significantly increased following the implementation of intervention packages such as training, supportive supervision, and feedback, 18 and Philippines, 29 and Uganda. 30 The interventions we applied; such as training, supervision, mentorship, motivation, and monitoring and evaluation on RHIS, might have helped build the capacity and knowledge of health workers, motivate staff, and enhance data flow and submission processes.
Similarly, data completeness also showed significant improvement following the implementation of the interventions overtime among the treatment groups. A similar finding was reported in the Oromia region of Ethiopia, where data completeness increased from 42% before the intervention to 100% post-intervention. Another study in Nigeria, 10 and Malawi 31 also reported improvement in changes in data completeness. A possible explanation for the association could be the strategies we implemented, such as standardizing data collection and reporting tools, training staff, validating data, conducting regular supportive supervision, offering timely feedback, and closely monitoring performance, all of which may have impacted overall performance. Together, these actions could also have strengthened the data management process, leading to more complete and reliable health data in source documents and reporting formats, which may have contributed to improvements in data completeness and overall data quality.
In this study, the overall ACDI intervention recorded a significant difference among the treatment groups, with greater improvement observed in the intervention groups compared to the control groups. Similarly, the intervention was found to be effective from baseline to end-line. Studies in the Oromia region of Ethiopia, 2 Amhara region of Northwest Ethiopia, 18 Tanzania, 32 low- and middle income countries, 33 showed improvement in the performance following the implementation of a combination of interventions, rather than single interventions. The combination of interventions greatly impacts helping to address multiple dimensions of data quality. 34 Training provides the essential knowledge and skills necessary for accurate data collection and reporting.19,35 Supportive supervision ensures consistent, on-the-ground guidance to address challenges and reinforce correct practices. 7 Feedback highlights errors or weaknesses, offering opportunities to correct and improve data practices in real time. 5 Review meetings serve as platforms for teams to assess performance, share lessons learned, and engage in collaborative problem-solving. Motivation creates a culture of accountability and encourages individuals to take ownership of the quality of the data they produce. 36
Encouragement for good performance in RHIS was among the predictors that significantly improved after application of the implementation in this study. Studies in Ethiopia and other parts of the globe have indicated that data quality practice is highly associated with institutional management support and encouragement.13,37 Our intervention has involved the heads of institutions and departments, whose encouragement and support could have made staff more effective and dedicated by addressing resource limitations and creating a supportive work environment in which staff feel safe to try new approaches and perform better through boosted morale.
As indicated in this study, when training is combined with encouragement from managing bodies, there is a statistically significant improvement in the perceived quality of routine data. Some descriptive studies have revealed the association of training and data quality practice.19,38 A study in Ghana has revealed that a combination of interventions is necessary to achieve the intended outcome of data quality. 39 Giving training to the healthcare workforce, especially to the heads of health institutions and leaders of departments, help them gain a deeper understanding of the importance of data quality in healthcare decision-making. 40 This awareness encourages a culture of prioritizing accurate, reliable, and consistent data at all levels of the institution. The motivation system helps improve data quality practice performance by increasing effort and accountability.
The perceived ease of data management skills and processes is a significant predictor of data quality practices that improved from before to after the intervention in the study. A study in in Oromia Special Zone, Amhara region of Ethiopia indicated a significant relationship between competency and data quality in RHIS. 41 Another study in Massaguet district of Chad also indicated an association between the presence of a health technician and staff dedicated to data management and data quality in the HMIS. 42 The perceived ease of data management skills and processes influences user engagement and motivation. 43 When health workers and managers perceive data management processes as easy to understand and perform, they are more likely to engage consistently in proper data recording and reporting, feel confident in handling data, be motivated to ensure accuracy and completeness, and complete records on time while avoiding errors. 44
The perceived level of information utilization is one of the predictors of data quality that showed improvement from baseline to end-line among the groups. A PRISM framework analysis revealed that organizational and behavioral determinants, such as data use, are key factors influencing data quality. 45 The likely explanation for this association is that using data in decision-making fosters accountability and ownership among health workers and managers by reinforcing their responsibility for producing quality data. Regular data reviews help identify and correct errors, thereby strengthening validation practices. This promotes a culture of continuous data quality improvement, motivates accurate reporting, and drives ongoing improvement through targeted actions based on identified gaps. 46
Using written guidelines in RHIS is an independent predictor of improved data quality practice in the study. As indicated by the Health Metrics Network, written guidelines promote standardization of data collection and reporting by ensuring uniform methods, definitions, and indicators, thereby minimizing errors and inconsistencies. 3
Consistency in using standard tools was a significant predictor of data quality practice in the study. A qualitative study conducted in Eastern Ethiopia revealed that the lack of standard forms was one of the barriers to data quality. 36 According to a report in South Africa, the standardization of routine data collection and reporting tools strengthens the system, supports a nationwide common platform, and reduces fragmentation in the health information data management system. 47 A possible explanation for the association of standardization tool utilization and data quality is that consistency in using documentation tools in RHIS is an important process that supports the regular, standardized, and systematic use of approved tools. These tools include registers, tally sheets, reporting forms, and electronic health records by health workers during service delivery, data recording, and reporting.48,49
Strengths and Limitation of the Study
Strength of the study is the use of a cluster RCT, which helps minimize experimental contamination by randomizing entire groups rather than individuals, reducing bias from cross-group interactions. Cluster randomized controlled trials are practical for group-level interventions and allow analysis of nested data structures, making them highly suitable for evaluating organizational-level interventions. They are cost-effective, ethically sound, help control for group-level confounders, and allow for long-term impact measurement.
Combining general linear mixed models with ITT enhances statistical power, minimizes bias, handles missing data, improves generalizability, ensures ethical transparency, addresses confounding, and provides accurate, real-world effect estimates.
Although buffer zones were in place, a limitation of the study is the geographical proximity of some districts, which may still have increased the risk of contamination. Therefore, despite efforts to keep the control group unaware of the intervention, some information transfer might have been inevitable. During sample size calculations, the assumption of equal cluster size was considered, but in practice, the number of health workers selected varied among different cluster.
Conclusion
The ACDIs strategies implemented in this study were found to be highly effective in influencing and bringing about the desired changes in data quality improvement. An encouraging system for good performance, ease of data management, perceived level of information use, and availability of written RHIS guidelines were significant predictors of data quality practices. Moreover, the joint effects of an encouraging system and RHIS training, were also significant. Providing training for large groups of managers and health workers, and integrating RHIS training with encouragement system are recommended strategies to improve data quality in health. Enhancing the data management skills of health workers and cultivating a culture of information use are also recommended interventions. Therefore, the ACDI strategies could be adapted and implemented in the region or in comparable settings with limited resources to strengthen data quality practices.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251399390 – Supplemental material for Augmented Capacity Development Interventions (ACDI) Improved Data Quality Performance in the Routine Health Information System (RHIS): A Cluster Randomized Trial
Supplemental material, sj-pdf-1-inq-10.1177_00469580251399390 for Augmented Capacity Development Interventions (ACDI) Improved Data Quality Performance in the Routine Health Information System (RHIS): A Cluster Randomized Trial by Bedilu Kucho Doka, Abebaw Gebeyehu Worku, Keneni Gutema Negeri and Dejene Hailu Kassa in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580251399390 – Supplemental material for Augmented Capacity Development Interventions (ACDI) Improved Data Quality Performance in the Routine Health Information System (RHIS): A Cluster Randomized Trial
Supplemental material, sj-pdf-2-inq-10.1177_00469580251399390 for Augmented Capacity Development Interventions (ACDI) Improved Data Quality Performance in the Routine Health Information System (RHIS): A Cluster Randomized Trial by Bedilu Kucho Doka, Abebaw Gebeyehu Worku, Keneni Gutema Negeri and Dejene Hailu Kassa in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We are grateful to Hawassa University, College of Health and Medical Sciences, School of Public Health and former Southern National Nationalities and Peoples Regional Health Bureau for giving us the opportunity to conduct this study. We would also like to thank the Doris Duke Charitable Foundation (DDCF) for financially supporting the data collection process of this study.
Ethical Considerations
Ethical approval of the protocol for this study was received from the institutional Review Board of the College of Medicine and Health Sciences, Hawassa University with the Reference No. of IRB/183/14 and date 08/06/2022. Approval letter was received from former Southern Nations, Nationalities and Peoples Region (SNNPR) Health Bureau. Permission letter was also obtained from the Gofa Zone Health Department, District Health Offices and each of respective health facilities. The study protocol was registered on 14 December 2022 at the Pan African Clinical Trial registry with ID number of PACTR202212472091194. The control institutions have received ACDI manuals after endpoint data collection.
Consent to Participate
All procedures were conducted based on the voluntary participation of the study participants in compliance with the Helsinki Declaration of ethical principles. Written informed consent was obtained from each study participant at both data collection points. Information about the study was clearly explained, and participants were assured of their anonymity, the confidentiality of their responses, and their right to withdraw at any stage.
Authors’ Contributions
BK involved in designing the study, data collection, data analysis, data interpretation, and manuscript write up. DH, AG, and KG were participated in the design of the study, critically reviewed and revised the manuscript. All authors have approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study would not be possible without the financial support of Doris Duke Charitable Foundation (DDCF) under grant number 2017187. The mission of the Doris Duke Charitable Foundation is to improve the quality of people’s lives through grants supporting the performing arts, environmental conservation, medical research and child well-being, and through preservation of the cultural and environmental legacy of Doris Duke’s properties. The funder had no role in the design of the study; the collection, analysis, or interpretation of data; the writing of the manuscript; or the decision to submit the manuscript for publication. All aspects of the research and publication process were conducted independently by the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets utilized in this study are available from the corresponding author and provided at the reasonable request of authorized personnel.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.