
Abstract
Background:
Malaria remains a public health priority In Zimbabwe, with approximately half the population at risk.
Aim:
This study aimed to review the literature to synthesise historical and current evidence regarding the impact of climate change on malaria transmission and management.
Methods:
Guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for a scoping review framework, a systematic search was conducted across multiple databases and websites, and 22 literature sources were included based on topic relevance and alignment to the inclusion criteria.
Results:
Most reviewed studies have consistently demonstrated that climate change is shifting the geographic distribution, trends, timing, and intensity of malaria transmission in Zimbabwe. However, others have emphasised the key role of non-climatic human, ecological, and health system factors and intervention coverage in shaping malaria transmission dynamics. Overstretched health systems and the uncertain effectiveness of existing interventions in a changing climate pose significant challenges to malaria management. This review identified key gaps, including the lack of longitudinal data, limited use of localised predictive modelling, and a limited focus on climate-parasite dynamics.
Conclusion:
There is a growing need for climate-informed programming, emphasising the need for improved local funding, multi-sectoral collaboration, community engagement, and building climate-resilient health systems.
Plain English Summary
This review examined research on how climate change affects malaria in Zimbabwe. Mosquitoes spread malaria, and their breeding and survival are strongly affected by temperature, rainfall, and humidity. The findings showed that increasing temperatures and changing rainfall patterns make some parts of Zimbabwe more suitable for malaria, even in areas that were not previously at risk. Some studies have also associated floods and droughts caused by extreme weather events, such as cyclones, with more malaria cases. However, some studies have provided different views. Other researchers have stated that factors such as poverty, health services, and access to preventive methods and medicines also play a major role in the decrease or increase in the number of people who fall sick from malaria. This review found that Zimbabwe’s current malaria control programs are facing new challenges because of the changing climate. There is also a lack of long-term data and climate-informed health plans. In summary, climate change makes controlling malaria in Zimbabwe difficult, and there is a need for new and more flexible strategies to keep people safe, especially in rural and hard-to-reach areas.
Highlights
Climate change is the reshaping of the malaria transmission dynamics in Zimbabwe.
This review identifies changes in the distribution, timing, and intensity of malaria outbreaks.
This study revealed that other non-climatic factors also influenced malaria transmission.
Gaps that hindered the successful management of malaria were identified.
Strategies to improve the management of malaria have also been identified in a changing climate.
Introduction
The changing climate of the Earth poses a massive and inevitable challenge to malaria control and management efforts worldwide. 1 Climate change is becoming an increasingly significant factor in determining the global burden and distribution of malaria. 2 Studies have revealed that malaria transmission is highly sensitive to climatic factors, particularly temperature, rainfall, and humidity, which influence the vector and parasite lifecycles.3,4 Vector mosquito breeding, survival, biting behaviour, and Plasmodium parasite development are influenced by rising temperatures, shifts in rainfall patterns, and changes in humidity. Its influence on vector behaviour has the potential to render the existing vector control strategies ineffective. For instance, vector control in the form of Indoor Residual Spraying (IRS) and insecticide-treated nets (ITNs) may lose its effectiveness if vectors change their resting and biting behaviours or if vector populations are ready to enter new geographical areas that were historically non-endemic for malaria transmission. 5
Sub-Saharan Africa (SSA) has the highest malaria burden, especially in pregnant women and children under the age of 5 years. According to the 2022 World Health Organization (WHO) Malaria Report, this region accounts for approximately 95% of global malaria cases and 96% of malaria deaths. 6 Zimbabwe is among the SSA countries in which the disease remains endemic, particularly in rural communities which are defined by the Zimbabwe National Statistics Agency (ZIMSTAT) as areas under traditional leadership and outside the jurisdiction of town boards and municipalities.7,8 These areas are primarily characterised by low population density, dependence on agriculture, and inadequate infrastructure which increase their vulnerability to malaria transmission under changing climatic conditions.
Malaria remains a public health priority in Zimbabwe, with half of the population already at risk of contracting the disease. 9 The country has committed to a malaria elimination strategy that emphasises enhanced surveillance, prompt radical treatment, vector control, and foci response as outlined in the National Malaria Elimination Strategic Plan (2021-2025). 10 Climate change in Zimbabwe may work against the country’s malaria elimination efforts. 11 Extreme weather events, such as El Niño, can create favourable environments for malaria transmission in previously non-receptive areas, straining the country’s under-resourced health system. 12 The increased burden of malaria on previously malaria-free populations may overwhelm health services, leading to delayed diagnosis and treatment. Zimbabwe’s health system continues to face resource constraints such as shortages of diagnostic supplies, essential medicines, and trained personnel. 13 Remote rural communities are characterised by infrastructure gaps, including poor road networks, inadequate health facilities, and limited communication systems. 14 These limitations compromise the capacity of the health system to effectively respond to and adapt to the changing epidemiological landscape of malaria.
Although scholars have increased their efforts to examine the malaria-climate nexus in Zimbabwe, existing research is fragmented and methodologically diverse. Studies lack coherence and differ significantly in their design, scope, focus, and quality. The approaches range from localised ecological studies to broad national policy reports, often utilising varying data sources and analytical frameworks. To date, no comprehensive review has systematically contextualised the impact of climate change on malaria transmission and management in Zimbabwe by integrating evidence from both peer-reviewed and grey literature sources. Consequently, malaria planners in regions with unstable malaria transmission lack timely and reliable evidence to guide interventions. Furthermore, complexities arise in Zimbabwe’s malaria research ecosystem because of contradictory findings from studies linking malaria transmission and climatic variables.11,15 A scoping review of the literature is needed to address these gaps by mapping the existing literature, identifying key themes, and informing climate-resilient malaria interventions in Zimbabwe.
This review aimed to synthesise historical and current evidence regarding the impact of climate change on malaria transmission and management in Zimbabwe. Table 1 lists the specific objectives and review questions.
Specific Objectives and the Corresponding Research Questions.

Methods
Study Setting
This scoping review focused on Zimbabwe. Landlocked countries located in Southern Africa are increasingly experiencing the negative health impacts of climate change, particularly vector-borne diseases such as Malaria. 16 It is located between latitudes 15°30′ and 22°30′ south and longitudes 25°00′ and 33°10′ east, covering a total surface area of 390 747 km2, with a total population of approximately 16.9 million people. 8 The country’s climate varies by region and season, but the southern and eastern parts are more vulnerable to extreme climate events, such as cyclones, droughts, and floods. Over the years, Zimbabwe has experienced a subtropical climate with a rainy season from November to March, which coincides with a period of high malaria transmission.17,18 However, in recent years, the country has experienced notable changes in rainfall patterns, protracted dry spells, and warming.
Zimbabwe’s vulnerability to the health impacts of climate change is shaped by historical, environmental, socioeconomic, and infrastructural factors. 1 Malaria transmission has traditionally been seasonal and concentrated in low-veld regions. 19 However, the previously malaria-free areas of Masvingo, Matabeleland South, and Midlands provinces have reported sporadic local transmission. For instance, Matabeleland South Province and Beitbridge District which had nearly achieved elimination by 2015, recently experienced sustained local malaria transmission linked to climate variability and cross-border movement.20,21 While enhanced surveillance may partially explain new detections, the spread of vectors into those areas driven by climate change suggests genuine ecological expansion rather than improved screening.
Study Design
The review was guided by a pragmatic paradigm, adopting the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) framework to ensure transparency, rigor, and repeatability. 22 The pragmatic approach centres on flexibility and practicality and prioritises solutions to real-world problems. 23 This approach captures multiple perspectives and types of evidence to provide a comprehensive understanding of the complex interplay between malaria and climate change. Inclusion criteria and search strategies were developed using the Sample, Phenomenon of Interest, Design, Evaluation, Research type (SPIDER) framework. This approach allowed for a comprehensive mapping of the existing literature on the impact of climate change on malaria transmission and management in Zimbabwe to inform policies and practices.
Inclusion Criteria
✓ Studies focusing on Zimbabwe or included as part of a broader analysis
✓ Focused on any population group in Zimbabwe (e.g. under 5s, rural population, general population)
✓ Studies published between January 2000 up to September 2024
✓ Empirical studies (quantitative, qualitative, mixed methods), modelling studies, reviews, and policy or technical reports.
✓ Studies done in English only
✓ Authors reviewed articles from reputable databases, conference papers, peer reviewed discussion articles, government reports, NGO reports, and policy briefs.
✓ Previous studies that addressed the relationship between climate change and malaria transmission and/or management
✓ Studies with full text accessible through open access or institutional databases are available to the authors.
Exclusion Criteria
Studies focusing on diseases other than malaria or non-climatic environmental issues.
Studies not focusing on Zimbabwe.
Studies published before January 2000 and after September 2024
Studies fully or partially done in languages other than English.
Journal and discussion articles that are not peer-reviewed, research protocols, newspaper articles, commentaries, editorials, or opinion pieces.
Data and Information Sources
This review used peer-reviewed journal articles, discussion articles, conference papers, and relevant reports as primary sources of data and information. The search began with reputable academic databases, including PubMed, Web of Science, African Journals Online, EBSCO, Cochrane Library, and Science Direct, from January 2000 to September 2024. The selected databases are known for their extensive collection of multidisciplinary peer-reviewed research articles covering historical and current scientific evidence on key topics including malaria. The review covers gaps left by traditional academic publications by including gray literature from conference papers, discussion articles, government reports, NGO reports, policy briefs and documents. The inclusion of government and non-governmental organisations as part of the gray literature helps contextualise the review to local settings.
Search Strategy
Google Advanced Search Engine was used to access relevant studies from PubMed, Web of Science, African Journals Online, EBSCO, Cochrane Library, and ScienceDirect. The keywords used for the systematic search were climate change, Malaria Transmission, Optimal control strategy, and Zimbabwe. Electronic databases were searched using the data collected between January 2000 and September 2024. The following search string was used: (“climate change” OR “climate variability” OR “climate factors” OR “environmental factors” OR “extreme weather events” OR “extreme weather event” OR “heatwave” OR “drought” OR “flood”) AND (“malaria transmission” OR “malaria incidence” OR “malaria control” OR “malaria management” OR “mosquitoes” OR “mosquito” OR “parasites” OR “parasite” OR “Anopheles” OR “Plasmodium”) AND (“rainfall” OR “temperature” OR “humidity” OR “landcover”) AND (“sub-Saharan Africa” OR “SSA”) AND (“vulnerable population” OR “vulnerable populations” OR “children” OR “pregnant women” OR “displaced persons” OR “refugees” OR “poverty” OR “socioeconomic status” OR “general population”) AND (“quantitative study” OR “quantitative analysis”) AND (“peer-reviewed” OR “research articles”) AND (“open access”) AND (“2000/01/01”[Date – Publication]: “2024/09/30”[Date – Publication]) AND (English[Language]) to search for eligible literature sources in the selected databases. Citation mining was used to ensure a comprehensive search. The process involved screening the reference lists of the included sources and identifying the articles that cited these studies.
In addition to a peer-reviewed literature search, a structured gray literature search was undertaken to identify government reports, policy briefs, publications from non-governmental organisations, conference papers relevant to malaria, and climate change in Zimbabwe. Targeted searches were performed across relevant websites for MOHCC, WHO, ZIMSTAT, and NGOs, such as UNDP. Boolean strings such as “climate change,” “malaria, and “Zimbabwe were searched using the Google Advanced Search engine. Policy documents were manually searched by government departments such as MOHCC, EMA, and the Ministry of Environment, Climate, and Wildlife. Citation mining was performed on the identified gray literature sources that could not easily be found through structured searches.
Screening Process
References retrieved from the selected databases were exported into Rayyan software in compatible formats (for example RIS, Bib Tex, EndNote). Rayyan software is a free web-based tool used to screen and select studies in systematic and scoping reviews using features such as blinding, tagging and filtering. 24 The next step was a two-stage screening process which started by screening titles and abstracts against the inclusion and exclusion criteria, followed by a thorough examination of the full texts to determine their alignment with the inclusion and exclusion criteria. Three reviewers conducted an article review to identify articles that were relevant for the final consideration. A blinding screening approach was implemented in the Ryyan software, ensuring that the reviewers were not influenced by each other’s decisions. Each article was classified as either “include,” “exclude” or “maybe.” Initially, each reviewer independently assessed the literature sources using predetermined inclusion and exclusion criteria. In cases of disagreement, the reviewers discussed the basis of their decisions, referring back to the review objectives and the inclusion/exclusion criteria.
In contrast, gray literature sources were manually screened owing to their diversity in formatting and lack of standard indexing. Two independent reviewers performed the screening in two steps. The first step assessed titles and executive summaries for relevance to climate change, malaria, and the Zimbabwean context, followed by full-text appraisal for alignment to the predefined eligibility criteria. Similar to peer-reviewed sources, a disagreement during screening of gray sources was resolved through discussion and consensus, with a third review being called to make a final decision if the first two reviewers remained in disagreement.
Data Extraction
A structured and systematic data extraction process was implemented to ensure that all relevant evidence was accurately captured for the analysis. A data extraction form was designed in Microsoft Excel using the Joanna Briggs Institute (JBI) guidelines to capture all relevant information from each of the included evidence source. 25 In addition, the inclusion and exclusion criteria, research questions, and objectives (Table 1) guided the development of the data extraction flowchart, which enabled the collection of relevant data. Two independent reviewers were assigned to each study to extract the data separately, using a step-by-step data extraction flowchart (Appendix A). The reviewers piloted a draft data extraction form for ten of the selected studies before applying it to the rest of the studies to ensure clarity and consistency. The pilot test results were used to refine the form before use. The reviewers read the full text of each assigned study and completed a data extraction form. Disagreements arose most notably in appraising study eligibility, determining study characteristics, and categorising the information reported in the included studies. A structured consensus process was followed when discrepancies arose during data extraction. Initially, a joint meeting was conducted, in which each reviewer independently justified their decision. The reviewers further discussed the main disagreement points guided by the review objectives and predefined eligibility criteria. If consensus could not be reached through a joint discussion, a third reviewer was engaged in the final decision.
Quality Appraisal
The use of multiple diverse databases coupled with gray literature ensures that adequate relevant evidence is captured. The quality of the included studies was appraised using the Mixed Methods Appraisal Tool (MMAT) version 2018. The MMAT is a validated instrument suitable for the quality assessment of scoping reviews, owing to its versatility across various study designs. 26 The tool was applied across all included studies, irrespective of the study design, except for gray literature, which was assessed using a separate appraisal checklist. Each included study was assessed by two independent reviewers by applying MMAT’s five core criteria appropriate to its design category. These criteria are:
(1) Clarity of the research questions.
(2) Appropriateness of the data collection methods.
(3) Relevance of sampling methods.
(4) Appropriateness of the data analysis methods.
(5) Coherence of the study data, interpretation, and conclusions.
Prior to the formal appraisal process, reviewers independently familiarised themselves with the MMAT 2018 user guide and discussed the agreed criterion to come up with a common interpretation. Disagreements emanating from the assessment were resolved by discussion and consensus. A third reviewer was engaged in cases where a consensus could not be reached. Although not mandatory in scoping reviews, quality assessment was conducted to enhance the rigor and interpretability of the study findings, particularly considering the methodological diversity of the included studies. 27 While MMAT could not be applied to gray literature sources because of their lack of formal methodological structure, inclusion was based on five appraisal dimensions adapted from previous public health scoping reviews. 28 These dimensions include source credibility, content relevance, content appropriateness, cross-validation, and transparency. These were considered to ensure the integrity and relevance of the included evidence sources.
Analysis and Synthesis
The extracted data were analysed using a descriptive and thematic synthesis approach in line with scoping review questions and objectives. Frequencies and percentages were used to summarise quantitative data, whereas qualitative data were synthesised using a narrative and thematic approach to identify key themes and trends. Microsoft Excel 2019 was used to manage and analyse the data. Data were analysed independently by two reviewers, and conflicts were resolved through discussion and consensus.
Results
Overview of Selected Sources
The database search yielded 1059. After removing duplicates, 889 records were retained for title and abstract screenings. An additional ten literature sources were identified from the cited literature sources and websites. Following the title and abstract screening process, 867 sources were excluded because they did not meet predefined inclusion criteria. The reasons for exclusion included studies not focusing on Zimbabwe, not malaria-or climate change-related, and lacking relevance to malaria transmission and management. The 32 remaining sources were sought for retrieval, and nine full texts could not be accessed through open-access sources. However, the full texts for two of these studies were successfully accessed through author correspondence. A total of 25 full-text articles were assessed for eligibility, and 22 studies met the eligibility criteria and were included in the final analysis. A PRISMA-ScR flow diagram illustrating the study selection process is shown in Figure 3.
Characteristics of Included Studies
Most (17 of the 22) included studies have analysed malaria and climate data between 2000 and 2020.1,2,15,16,19,20,29 -41 However, none of the included studies analysed more recent trends from 2021 to date, whereas others (6 of the 22 included studies) have focused on more historical datasets dating back to 1980.11,37 -39,42,43 The primary justification for the selected timeframes was data availability and the need to assess temporal trends and correlations between climate change and malaria transmission. The reviewed studies were conducted across a range of geographic settings, with a strong focus on malaria-endemic and pre-elimination regions in Zimbabwe, including rural districts such as Chimanimani, Mount Darwin, Gwanda, Buhera, and Mutasa15,29,31,44 (Figure 1). Only a few included sources (2 of the 22) have provided comparative insights into the climate-malaria nexus between Zimbabwe and other countries in sub-Saharan Africa.2,41 Data availability, historical malaria burden, and projected or observed environmental changes affecting malaria transmission were the most frequently (10 of the 22 included) mentioned reasons for selecting specific study areas.2,20,32,34 -36,39,41,42 Table 2 summarises the characteristics of the studies included in this review.

Map of geographic scope and focused areas of research studies.
Characteristics of Included Studies.

The reviewed evidence sources reflect a cross-sectoral mix of funders, ranging from Non-Governmental Organisations (NGOs), academic institutions, research institutions, governments, and international organisations. A considerable proportion of the studies (7 of the 22) reported their sources of funding were academic and research institutions including universities, commonly through collaborative research or postgraduate student research support.2,9,11,15,29,31,34 Government funding (3 of the 22 included) mainly targeted policy and strategic documents through the Ministry of Health and Child Care and the Ministry of Environment Water and Climate.16,32,37 Limited evidence sources (4 of the 22) acknowledged funding from international agencies and partners such as the United Nations Development Program (UNDP), USAID, World Health Organization (WHO), Malaria Consortium.1,33,34,42 Only four of the included studies mentioned not receiving any external funding, and they conducted using their own resources.30,36,42,44
Methodological Approaches
Study Designs
Predominantly (9 of the 22 included), literature applied quantitative modelling study designs, which analysed historical malaria and climate data to assess trends, correlations, associations and in some cases predict into the future.11,30 -33,35,39,42,43 Ecological and time-series approaches have been applied in six of the included studies by integrating GIS and remote sensing to map spatial patterns and identify malaria hotspots.2,11,32,33,35,41 The simulation of malaria risk under climate change scenarios has mostly been performed using statistical, or predictive models, including ecological niche and Bayesian analysis.9,19,32,33,42,43 Only 2 of the 22 studies conducted narrative and systematic reviews to synthesise the existing evidence in Zimbabwe. A systematic review of the literature conducted in Uganda and Zimbabwe highlighted climate change as a context-specific challenge for sustaining malaria prevention strategies, while a narrative review conducted in Mutare and Mutasa districts explicitly discussed climate change as one of the emerging challenges hindering malaria elimination.41,44 Similarly, a minority of studies have adopted qualitative (2 of 22)29,34 and mixed-methods approaches (2 of 22)36,38 to gain a more comprehensive understanding of the malaria climate relationship. None of the 22 included studies explicitly mentioned the use of mathematical models and machine-learning techniques to model malaria transmission in the context of climate change.
Measures of Malaria Transmission
Malaria incidence, typically reported as cases per 1000 population, was the most reported (12 of the 22 included) measure of transmission.2,16,19,29,31,35,39 -43,44 Some studies (2 of 22), particularly cross-sectional surveys, used prevalence rates to estimate the proportion of infected populations at a given place and time.32,36 Two qualitative studies applied perceived prevalence to explore local perceptions of climate change and its impact on malaria transmission.15,38 Case counts and malaria risk levels were sparse (2 of the 22 included) and were used in spatial analysis and modelling studies to predict high transmission areas.33,37 Four of the 22 included evidence sources reported no formal epidemiological measures but referred to the general risk of malaria transmission.1,11,30,37
The reviewed evidence indicates that the malaria incidence varies markedly across districts and ecological zones. For instance, malaria incidence ranged between 18 and 43 cases per thousand people per year from 2005 to 2015, with seasonal peaks aligned with the rainy season. 35 A study in Buhera district showed micro-spatial clustering of cases around wetlands and irrigation schemes, with malaria incidences fluctuating between 25 and 48 cases per thousand population. 31 Similarly, climate variability and low vector control coverage have been reported as drivers of localised outbreaks in Mutare and Mutasa districts, with prevalence rates exceeding 20% during peak periods. 44 Qualitative enquiries in the Chimanimani and Mount Darwin districts reinforced the quantitative findings, with residents perceiving increased prevalence linked to warmer temperatures, altered rainfall patterns, and deforestation.15,38 Similarly, gray literature sources, including the Third National Communication to the United Nations Framework Convention on Climate Change (2017) and the Zimbabwe Human Development Report (2017), have warned that climate change may expand malaria transmission to traditionally low-risk areas.1,39
Climate Change Variables
The reviewed evidence sources assessed a range of climate change variables to understand their impact on malaria transmission and management. Temperature (minimum, maximum, and average) and rainfall were the most frequently (19 of the 22 included) assessed variables considering their direct influence on vector breeding and parasite development.1,2,11,15,19,29 -40,42,43 Three articles included humidity and seasonality to explore their influence on observed malaria trends.15,29,43 Three evidence sources considered the effects of extreme weather events, such as droughts, cyclones, floods, and droughts, on malaria transmission.34,37,38 In addition, about half of the included sources employed remote sensing indicators such as the normalised difference vegetation index (NDVI), Land Surface Temperature (LST), proximity to water bodies, and evapotranspiration to model interactions between climate and malaria transmission risk.11,19,30 -33,39,40,42,43 GIS-based modelling identified statistically significant associations between rainfall patterns, warming temperatures, and malaria incidence.42,43 Climate suitability modelling by Ebi et al 11 further indicated that changes in temperature and precipitation could modify the geographic distribution of malaria in Zimbabwe. Their findings projected that the highlands become more suitable for transmission, whereas the Lowveld and areas with low precipitation show varying degrees of change, depending on climate sensitivity and greenhouse gas emission stabilisation scenarios.
Data Sources and Tools
Many studies (15 of the 22) primarily relied on secondary data collection.1,2,11,19,30 -33,35,37,39,41 -43,44 Epidemiological data for malaria was frequently collected from the District Health Information System (DHIS-2) database, while climate data from the Meteorological Services Department (MSD), and global datasets.19,31 -33,35,36,42,44 Remote sensing and GIS tools are often (7 of the 22 included) used to collect environmental variables such as NDV, proximity to water bodies, road networks, slope, and elevation.30 -33,35,42,43 In limited evidence sources (4 of the 22 included), qualitative interviews and literature reviews were incorporated in studies to capture community perceptions and policy insights.15,29,34
Data Aggregation
Predominantly, (16 of the 22) included literature aggregated malaria transmission and climate data at monthly or annual levels.2,11,16,19,29,32 -37,39,41 -43,44 Annual aggregation was employed in ten included studies that either examined long-term trends or conducted retrospective reviews over many years.2,16,32,33,36 -39,42,44 A few evidence sources (two of the 22 included) applied seasonal aggregation to environmental and epidemiological variables to assess changes in malaria transmission patterns.29,38 Weekly aggregation was used in only one study, which was highly localised and focused on short-term outbreaks. 40
Special Populations
Most of the included sources (13 of the 22) focused on the general population without categorising them into specific groups, with the remaining nine targeting special populations. Special populations highlighted in the reviewed studies included children under five, pregnant women, and people living in highlands or newly malaria-prone areas, who were identified as particularly vulnerable to malaria under changing climatic conditions.1,34,40,42,43 Limited evidence sources (4 of the 22 included) deliberately focused on rural and low-income communities with limited access to healthcare and vector control interventions.15,34,36,38
Impact of Climate Change on Malaria Control/Elimination Strategies
The reviewed literature (17 of the 22 included) consistently confirms the existing and evolving relationship between climate change and malaria transmission which creates uncertainty regarding the sustainability of the existing control and elimination strategies.1,2,11,15,29 -31,33 -36,38 -40,42,43,44 Table 3 provides a detailed summary of climate change outcomes and their impacts on malaria transmission and management strategies.
Summary of Climate Change Outcomes and Impacts on Malaria Transmission and Management.

Impacts on Malaria Epidemiology
A substantial proportion (16 of the 22) reviewed sources identified climate impacts on malaria epidemiology through various methodological approaches including formal epidemiological trend analysis, modelling and community perceptions.2,11,15,19,29,31,32,34 -40,42,44 Notably, 19 of the reviewed literature sources indicated a shift in the spatio-temporal patterns of malarial transmission.2,11,15,16,19,29,32 -44 Longer and less predictable malaria transmission seasons, emergence of malaria in highlands and previously non-endemic communities, and outbreaks after extreme weather events such as floods, were noted in half of the reviewed evidence sources.11,15,29,34 -36,38,40 -43 In addition, two of the included studies observed shifts in sociodemographic characteristics of the affected population, such as age and increased burden among previously non-exposed populations.36,40
The reviewed sources consistently revealed spatial heterogeneity of malaria cases across Zimbabwe.1,2,16,19,32 Malaria hotspots were concentrated on the Eastern and Northern parts of Zimbabwe (Figure 2). The high-risk districts included Mutasa, Chimanimani and Buhera in Manicaland Province; Mount Darwin and Muzarabani in Mashonaland Central; Mwenezi and Chiredzi in Masvingo and Hwange in Matabeleland North.16,42,45 Other Districts such as Gwanda and Mberengwa continue to experience local transmission even though they have transitioned to malaria elimination.16,20 Highland or urban districts such as Harare, Bulawayo, Zvishavane, Gweru and Zvimba were mostly classified under low-risk areas.11,30,32 Figure 2 shows the synthesised malaria hotspot map, based on evidence from included data sources (Figure 3).

Map of malaria risk hotspots in Zimbabwe based on included literature.
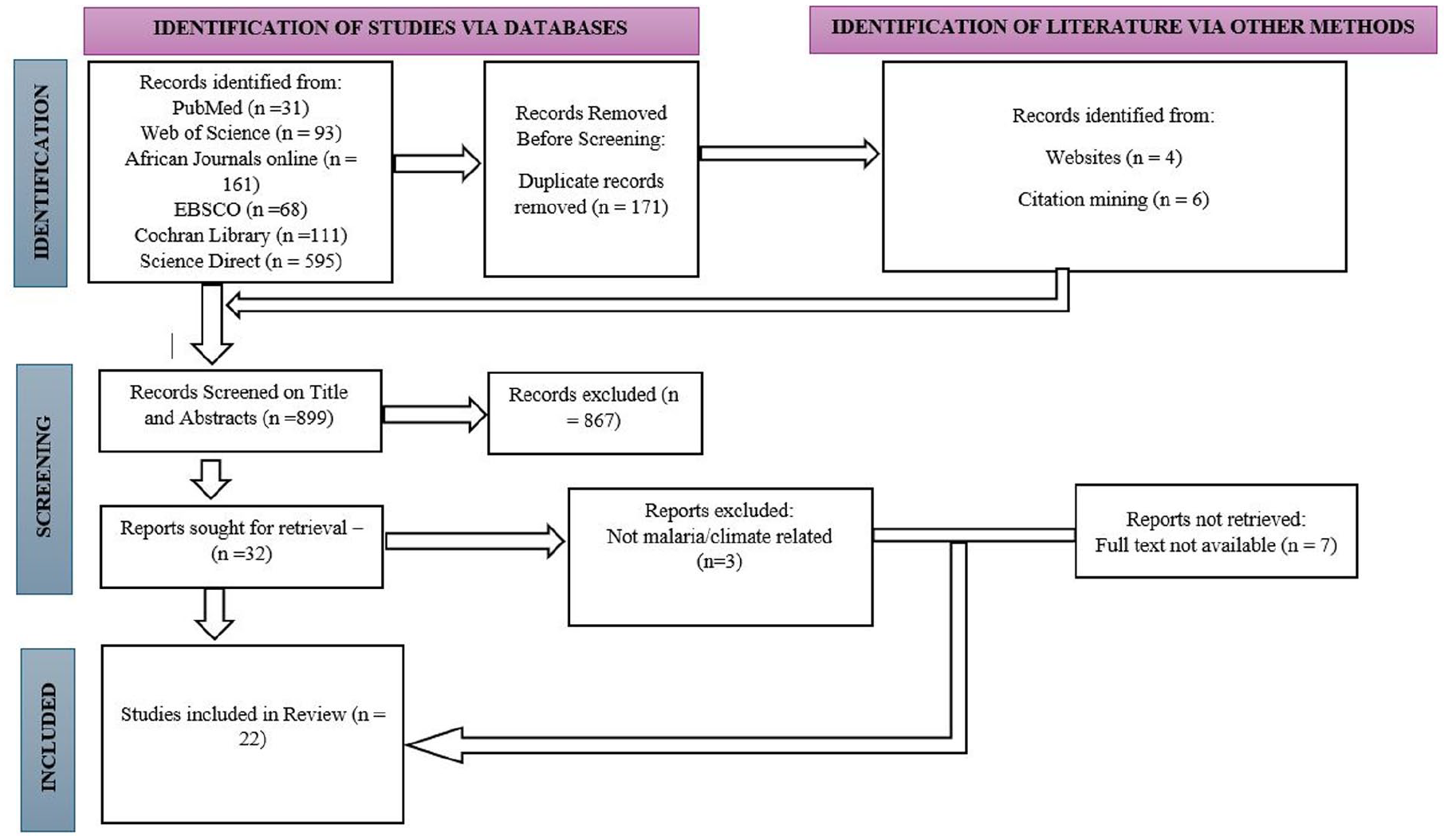
PRISMA-ScR flow diagram for the study selection process.
Impact on Existing Interventions
Approximately half of the reviewed literature acknowledged that malaria control and elimination have been effective to some extent in reducing the burden of malaria in Zimbabwe over the past few decades.1,2,16,19,31,32,34,36,40,41,44 However, most of the reviewed sources either partially or did not directly assess the effectiveness of existing interventions (for example, insecticide-treated nets, indoor residual spraying, and antimalarial drugs) under changing climatic conditions. The few studies (3 of the 22 included) that assessed the impact of climate change on current interventions concur that climate change limits its impact and compromises sustainability.15,40,44 Six of the included evidence sources documented vector behaviour and distribution changes in response to climate change as limiting factors for the effectiveness of existing interventions.16,32,36,39 -41 Five of the included literature sources revealed that vector Anopheles mosquitoes are no longer limited to traditional hotspots, but there is increasing breeding in new areas, leading to higher burden in previously non-endemic areas.32,36,39,40,44
Limited reviewed sources (3 of the 22) that focus on the link between the parasite and climate change have revealed that Plasmodium falciparum is the dominant species in Zimbabwe.11,16,40 Despite the lack of adequate evidence linking the prevalence of the parasite directly to climate change, one reviewed study indicated that there is increased persistence in climate-favourable areas, while other species remain rare and unchanged. 40
Impact on Health Systems
The literature sources in this review identified various ways in which health systems are affected by the impact of climate change on malaria control and management. Over half of the included sources revealed that an increase in malaria burden, longer transmission seasons, and outbreaks in previously non-endemic areas overstretch the health service delivery system, including a shortage of medicines, diagnostic supplies, and trained human resources.1,2,11,15,19,34,36 -40,42 Two evidence sources indicate that health facilities in newly affected geographical settings or high-altitude areas are ill-prepared for emerging cases, resulting in delayed diagnosis and treatment.36,42 Additionally, 3 of the 22 sources reported that extreme weather events such as floods drive unpredictable outbreaks, malaria outbreaks, disruption of planned interventions, straining of essential routine services, and increasing operations.19,37,42
Two studies found that limited resource settings, particularly in rural communities, were the most affected.1,19 In a moderate proportion of the included literature sources (9 of the 22), climate change has been found to exert a direct impact on health systems, particularly on time-case detection, management efforts, and critical resource allocation.1,15,32 -34,38 -40,44 Two of the reviewed studies revealed that floods in Chimanimani and Mutasa districts created extensive breeding sites, resulting in localised outbreaks that overstretched the health systems’ capacity to diagnose and treat malaria cases. 15 In addition, the Zimbabwe Human Development Report (2017) highlighted that droughts and floods as a result of climate change disrupt health service delivery, reduce access to clean portable water, and increase the risk of water- and vector-borne diseases such as cholera and Malaria. 1
Strategies for Optimising Malaria Management Under Climate Change
The reviewed evidence sources have proposed various strategies to optimise the management of malaria in the context of climate change. The strategies were synthesised into seven main thematic areas: surveillance and early warning, health system capacity and resilience, vector control interventions, infrastructure resilience, community engagement, technological innovation and policy, and planning and governance. Table 4 provides a detailed summary of these thematic areas along with their corresponding strategies and relevant evidence sources.
Strategies to Optimise Malaria Management Under Climate Change.

Research Gaps and Weaknesses in the Literature
Most of the included studies revealed gaps and limitations affecting the robustness of their findings. The highlighted gaps span geographic scope, methodological approaches, data availability, and the quality and utilisation of findings to inform policy and practice.
Geographical gaps: Over half of the included (12 of 22) studies have focused on six specific districts in Zimbabwe, particularly Gwanda, Chimanimani, Mutasa, Mutare, Mount Darwin and Masvingo.15,29 -31,33 -36,38 -40,44 Matabeleland South (4 of 22), was the most frequently studied province among the 22 included sources, followed by Manicaland (3 of 22), Masvingo (2 of 22) and Mashonaland Central (1 of 22). As shown in Figure 1, no district- or ward-focused studies have been conducted in other highly burdened districts of Zimbabwe, such as Binga, Gokwe North, Mbire, and Muzarabani. Key elimination districts such as Mberengwa, Mutoko, Beitbridge, Zvimba, Gutu, Seke, Sanyati and Gokwe South were not represented in the reviewed literature.
Methodological gaps: Only a few studies (2 of 22) have utilised mixed-method approaches to enhance rigour.15,36 In four instances where, predictive models were used, they were built on various assumptions, such as that vector climate relationships remain constant over time, and the effectiveness of vector control interventions does not change over time.11,31,33,42
Data quality and availability: A considerable number of included evidence sources (9 of 22) revealed a lack of longitudinal, validated, and spatial data which compromised generalisability and the ability to predict in the future.1,15,16,29,31,33,37 -39 Furthermore, the aggregation of epidemiological and climate data at the district or national level by 10 of the 22 included literature sources may not adequately reveal localised malaria transmission patterns in the context of climate change.2,11,16,19,30,32,37,41 -43
Limited use of localised predictive modelling approaches: Included studies that applied predictive modelling focused on national or district-level data which may obscure local transmission dynamics.11,32,33,42,43 The use of coarse environmental and epidemiological data at district and national levels may not be representative of the situation at the local level.
Lack of adequate representation of vulnerable populations: Most of the included studies (13 of 22) focused on the general population, with relatively fewer (9 of 22) focusing on vulnerable populations, such as children under the age of five, pregnant women, and hard-to-reach communities.
Limited focus on climate-parasite dynamics: A few studies (1 of 22) have examined how climate change affects Plasmodium parasite development, survival, and transmission. 40 Understanding how climate change influences parasite biology is critical, as it has a bearing on the transmission intensity and seasonality.
Discussion
Overview of Key Findings from the Study
This scoping review synthesised existing evidence on the impact of climate change on malaria transmission and management in Zimbabwe. This was achieved through (1) identification and documentation of literature sources; (2) examination of how studies have been conducted; (3) determination of the impact of climate change on malaria control and elimination strategies; and (4) gathering and analysing proposed strategies to optimise the elimination, management, and prediction of malaria. The reviewed articles employed diverse methodologies, most of which employed quantitative modelling and GIS-based approaches, relying on retrospective health system records and climate datasets collected at the ward, district, provincial, and national levels.
The studies in this review adopted a range of methodological approaches, including qualitative enquiries, GIS-based risk stratification, climate suitability modelling, spatial and spatiotemporal analysis, micro-spatial mapping of cases, and literature reviews. Most studies relied on secondary epidemiological and meteorological data from district and national health systems, with limited fine-scale local malaria data at the community and ward levels. The analysis at district, provincial, and national levels was valuable in providing trends and generalised risk maps; however, they lacked the resolution to adequately capture local malaria transmission and management dynamics under climate influence. Consequently, the heavy reliance on course-scale analyses raises questions regarding the reliability of such models in guiding interventions at the community level, where micro-climatic and anthropogenic environments are unique.
The reviewed literature has consistently demonstrated that climate and environmental changes affect vector breeding, parasite development, geographical distribution of cases, and the timing and duration of malaria transmission seasons.11,34,42 Shifts in rainfall patterns can create new and more persistent malaria vector breeding sites in previously non-endemic settings, while warmer minimum temperatures have been reported to shorten the extrinsic incubation period of Plasmodium parasites within vectors. 43 Additionally, warmer conditions accelerate vector mosquito breeding cycles, resulting in increased vector densities.11,42 By shortening the life cycle and increasing the longevity of vector mosquitoes at optimum temperature ranges between (25-30°C), warmer temperatures facilitate the development of more vector mosquito generations, elevating the risk of malaria transmission. 46
Studies in this review concur that climate change limits the effectiveness and threatens the sustainability of malaria control and elimination interventions.15,40,44 Unpredictable rainfall patterns and prolonged droughts can disrupt indoor residual spraying schedules and reduce the availability of water required to sustain the activity, whereas flooding events can create new vector breeding sites, resulting in reintroduction in previously cleared areas. Loss of household income during drought and flood periods limits community access to treated mosquito nets. Extreme weather events and changing climate conditions have been noted to exert pressure on fragile local health systems and previously non-endemic geographical settings, which are ill-prepared to increase malaria burden. These findings highlight the role of climate-related shocks in not only increasing risk but also exposing and amplifying health system weaknesses, undermining progress towards the malaria elimination goal.
Importantly, the limited studies in this review have highlighted the equally important role of non-climate factors, such as socio-economic status, land use, and urbanisation, underscoring the multifaceted nature of malaria transmission in Zimbabwe.1,15 Socioeconomic factors, such as poverty levels and occupation, influence household vulnerability by restricting access to prevention and treatment services. For example, low-income households may fail to afford preventive tools and build quality houses that prevent mosquito entry or relocation to low-risk areas, while limited education restricts the ability to invest in preventive measures by reducing awareness of their importance and proper use.
The review identified six key thematic areas to optimise the elimination, management, and prediction of malaria in the context of climate change. These include (1) strengthening surveillance and early warning systems, (2) building health system resilience capacity, (3) vector control interventions, (4) technological innovation, (5) community engagement, (6) infrastructure resilience, and (7) policy planning and governance. These interconnected areas demonstrate the need for a coordinated strategy for malaria management under climate change.
Comparison with Existing Literature
Our scoping review findings align with the global and regional evidence base, which indicates seasonal and geographical shifts, increased burden in previously non-endemic settings, outstretched health institutions, and uncertainty of existing interventions under climate change scenarios.47 -51 For example, multiple studies conducted across Africa have predicted that climate change will significantly alter the epidemiology of malaria across the continent, with potential transmission expansion in Southern and Eastern Africa and Contractions in Western Africa.51 -53 A few reviewed studies have brought a divergent but important perspective, revealing the role of non-climatic factors, such as socioeconomic conditions, land use, and health system factors. This aligns with evidence from some studies conducted globally and in Africa, suggesting that the negative impacts of malaria transmission will potentially be offset by urbanisation, enhanced public health interventions, and improved socioeconomic conditions, which have contributed to the observed declining malaria burden despite the changing climate.45,54,55 Overall, the review findings underscore the importance of prioritising both climatic and non-climatic factors in the control and management of malaria in the context of climate change.
Implications for Policy and Practice
The results of this review have important implications for malaria policies and practices in Zimbabwe, particularly in the context of climate change. Considering that climate variability directly shapes the epidemiology of malaria, national- and sub-national-level malaria programming must integrate climate intelligence into routine surveillance, monitoring, and early warning systems. For example, real-time climate data on temperature and rainfall from the Meteorological Services Department or Ministry of Lands, Agriculture, Fisheries, Water, and Rural Development cold are linked with local health facilities malaria case trends to anticipate outbreaks and timely deployment of interventions such as Larval Source Management and deployment of insecticide-treated nets in malaria pre-elimination and control areas. Malaria data analysis should therefore move beyond case reporting to include climate and anthropogenic variables and improve forecasting accuracy and resource allocation. Furthermore, multi-sectoral collaboration between the Ministry of Health and Care, Meteorological Services Department, and other key government sectors must be strengthened to ensure a coordinated response to climate-related malaria risks. Effective collaboration should move beyond information sharing to include the development of systems that integrate climate and health data, joint training and intervention planning, and the harmonisation of sectoral policies. Importantly, the operational capacity of the health workforce in low-risk and previously non-endemic settings must be strengthened through targeted training on climate-sensitive diseases, such as malaria. Training must focus on updated diagnostic skills and treatment protocols aligned with evolving disease transmission patterns. Such training must be complemented by major investments in climate-resilient infrastructure. There is a need to construct flood-resistant health facilities in flood-prone communities, such as the Chimanimani and Mutasa districts. In addition, improved storage facilities for critical antimalarial medicines must be adapted to withstand extreme heat.
At the community level, Social Behaviour Change (SBC) strategies must be redesigned to resonate with emerging malaria risks in places that were previously considered safe. Messaging should account for shifts in community perception of vulnerability. The planning of community awareness programs on malaria and climate change must go beyond basic sensitisation, create ownership, and foster adaptive practices such as environmental manipulation to reduce breeding sites around local irrigation schemes.
Research Gaps and Future Research Directions
From a research perspective, this review underscores the urgent need to go beyond the general analysis of climate malaria correlations and conduct granular multidisciplinary studies that examine causal pathways and evaluate the effectiveness of interventions in a changing climate. Future work must prioritise fine-scale analysis at district and ward levels to better capture context-specific climate-driven malaria transmission dynamics. Finally, strengthening local research capacity and providing sustained local funding are essential to ensure that Zimbabwe creates its own climate-malaria evidence base. Overreliance on external funding models and risks producing generalised evidence that may not reflect local realities or align with national malaria research priorities. Despite the invaluable contributions of this review to the management of malaria under climate change scenarios, several key gaps were identified, including limited geographical coverage, insufficient and poor-quality data, overreliance on generalised assumptions in predictive models, and inadequate use of robust multi-method approaches. Future models should use high-resolution, locally validated data, calibrate model parameters with historical surveillance data, and integrate ensemble approaches to reduce uncertainties. Ensemble approaches reduce uncertainties by integrating the outputs from multiple predictive models instead of relying on a single set of assumptions. 56 Future research should focus on multidisciplinary approaches that link malaria with both climatic (e.g. temperature, rainfall, and humidity) and non-climatic factors (e.g. health-seeking behaviour, population density, and vector control). Furthermore, there is a need to consider more robust methodologies, including multi-method approaches at the granular level, to enhance the rigor and applicability of the study findings.
Strengths and Limitations of the Review
This scoping review approach provides a broad and inclusive overview of the existing literature on the impact of climate change on malaria transmission in Zimbabwe. A key strength of this review lies in its integration of evidence from both peer-reviewed and gray literature sources, offering a uniquely comprehensive synthesis of how climate change affects malaria transmission and management in Zimbabwe, an area previously lacking in contextualised and inclusive analyses. The selection of reputable databases and gray literature in the form of Ministry of Health and Child Care, United Nations, Government Agencies and Non-governmental organisations reports ensures that the review captures evidence from sources not published in traditional databases. In addition, the review applied a well-defined and transparent framework which included a clear search strategy and predefined inclusion and exclusion criteria. The application of a rigorous two-stage screening process and the MMAT for quality assessment ensured the validity and reliability of the findings.
The following limitations should be considered when interpreting the findings of this study. First, normally studies with statistically significant results or positive findings are more likely to be published, which creates a publication bias in the review. This review attempts to address this limitation by including gray literature that applies to the Zimbabwean context. Second, language, regional, and temporal restrictions in this review may have excluded relevant research published in other languages, conducted in excluded settings, and published outside the predefined timeframe. Third, the variability of the included studies in design and quality requires a cautious approach for the interpretation and generalisation of the review findings. Fourth, despite efforts to retrieve full text, seven potentially relevant articles could not be accessed, which may have influenced the completeness of the available evidence. Fifth, the included studies were heterogeneous in design, methodology, and reporting, which limits the ability to draw causal conclusions, and the interpretation remains descriptive. Finally, the inclusion of gray literature together with peer-reviewed articles, despite broadening the scope of the review, may have introduced variability in quality.
Conclusions
This scoping review highlights that climate change is reshaping malaria transmission in Zimbabwe, overstretching fragile health systems in previously non-endemic settings, and creating uncertainty over the effectiveness of existing interventions. While most studies agree on the role of climatic factors, such as temperature, rainfall, and humidity, in malaria transmission, others have emphasised the importance of non-climatic factors, including socioeconomic status, urbanisation, and vector control coverage. The synthesis of available evidence proposes seven strategic areas to effectively control and manage malaria in the context of climate change: climate-informed surveillance and early warning, building health system capacity and resilience, enhancing vector control interventions, infrastructure resilience, technological innovation, community engagement, policy planning, and governance. This review’s findings have substantial implications for policy, planning, and research. The integration of climate intelligence into national and subnational planning, surveillance, and response is vital. It is equally important to build community resilience through community engagement and strengthening local health systems in response to climate stress. Research should cover more geographical settings and more robust methods should be employed to inform malaria programming under climate change scenarios.
Footnotes
Appendix A: Data Extraction Flowchart
This flowchart provides a step-by-step visual representation of the data extraction process, ensuring clarity in criteria and consistency in evaluation for each literature source.
Ethical Considerations
This scoping review did not require human participation as it focused on analysing and synthesising existing data. This review was part of a PhD study approved by the Institutional Review Board (IRB) at the National University of Science and Technology (ethics number NUST/IRB/2024/118).
Authors Contributions
TC took the lead in conducting this scoping review in the partial fulfilment of the DPhil in Environmental Health degree at the National University of Science and Technology. WNN, AM, and MD provided an overall mentorship and reviewed protocols. GNN reviewed and participated in screening and reviewing literature sources. WNN conceptualised the research idea, reviewed it, and provided substantial input to the draft of the manuscript. All authors have read and adopted the manuscript for final submission to a journal and have agreed to its publication. WNN is responsible for the overall content of the guarantor.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article and its supplementary files. Further details or clarifications are available from the corresponding author upon reasonable request.