
Abstract
Hybrid professionals in healthcare organizations play a critical role, the characteristics, processes and implications of which have been thoroughly studied by scholars in the field. However, not as much attention has been paid to the conditions under which such roles might be taken by professionals entering the ground of management. This gap results into a lack of conceptual clarity and eventually ends being an obstacle in framing and ameliorating the tools needed to act such a role in its different phases. This is a research area worthy of a finer-grained understanding: the ability of organizations to effectively support role hybridization, in fact, is a requisite for professionals-managers' willingness to stay in the role and cope with the complexity that such a two-fold position entails, no matter what. Based on the results of a scoping literature review, this paper presents the enabling conditions for hybrid professionalism in healthcare, and proposes a classification of them into categories corresponding to different facets of hybrid role-taking: opportunities for interaction with management, tools supporting sense-making, and provision of delegation and autonomy. For each of these categories, organizational and management tools discussed in the literature are presented. The results of the study provide a road-map of the enabling conditions for hybrid professionalism that aims to be of practical convenience for managers and policy-makers in health care. Eventually, suggestions for organizational design and personnel management, as well as directions for further research, are highlighted.
Introduction
Despite the reforms of the last decades which introduced managerial approaches in healthcare, still many professionals find uneasy to take up managerial responsibilities over staff and resources. “Two-way window” positions 1 are indeed intertwined with complexity. Therefore, for both research and practice it is crucial to understand how the social and organizational context can support the process of healthcare professionals’ managerial role-taking, in order to find arrangements that can help them navigating ambiguity. Through a scoping literature review, this paper aims at identifying and classifying the main enabling conditions supporting the development of hybrid medical managers, by embracing an understanding of hybrid management as dynamic. 2 Although the debate on hybrid professionalism is relentlessly gaining ground in all fields of organization and management studies,3,4 much of the scholarly attention is directed towards either macro-level institutional logics or micro-processes of identity work, with the meso-level discourse end up being the underdog. 5
In order to contribute filling this gap, we start by presenting the theoretical background on healthcare hybrid professionals and the enabling conditions for these roles, while in the following paragraph the methods are illustrated. After presenting a synthesis of the literature we propose a framework of the enabling conditions for hybrid managers, which is later discussed with regard to its implications for healthcare management and research in this field.
Hybrid professionalism
Hybrid managers are professionals involved in intermediate layers of hierarchy within an organization, responsible for staff or resources and with the potential to negotiate and merge professional and managerial cultures, values, and identities.6–8 The rise of hybrid managers was part of the process which brought managerial values and practices into professional settings, which have challenged the classical forms of organising professional work. Traditionally, healthcare professionals were granted high degrees of autonomy, necessary to apply specialized and tacit knowledges to highly complex cases at the service of citizens. Their work was subject to professional values and social norms of behaviour, and supervised by the professional community, therefore it did not require external forms of appraisal and control.9,10 However, political, economic and social forces have put pressures over public professionals questioning whether what they do and how they do it is still capable to respond to societal and individual needs. Starting from the 1980s, New Public Management reforms in healthcare, as well as in other public professional fields like education, justice, social services, have increasingly required professionals to consider efficiency alongside effectiveness, and to openly report performances and be accountable to the public rather than (only) to the profession. 11
Research on hybrid roles found that they are capable to balance intrapersonal and interpersonal conflicts and to reconcile the two apparently conflicting worlds.7,8 They have the potential to bridge the gap between colleagues and administrators, maintaining the professional status and legitimacy but being “loyal” and committed towards the organization and its top management.12,13
Recently, scholars have moved forward and suggested to look beyond hybridity as a juxtaposition of contrasting logics or practices, rather underlying that organizing becomes an intricate part of professional work3,14,15 and that managerial and professional mindsets could indeed end up being “overlapping discourses”. 16 Several authors have hence argued that a “new professionalism” was born, characterized by a focus on coordination, quality improvement and accountability to external stakeholders. 17 In the same line, Salvatore and colleagues 18 showed that, contrary to traditional approaches stressing the clash of cultures, professionals’ identification with their organization and their profession can in actual fact correlate. Individual responses to such combination can indeed diverge remarkably, depending on multiple configurations that can arise from both individual agency and organizational level factors. 19
Enabling conditions for hybrid professionals
In light of this variability, it is paramount to understand in depth the factors that support or hamper the process of professionals’ managerial role-taking. In fact, crafting a hybrid-role identity is not an individualistic process, but depends to a great extent - as any other working experience within an organization - on the efficacy of relational and social interactions with others, whatever the organizational articulation. 20 As “the organizational context makes some actions easier, and therefore more likely, and other actions harder, and therefore less likely”, 21 thus leading to the creation of organizational routines, in this study we focus on those conditions making easier - or more likely - for professionals-managers to exert effectively their hybrid role. To do this, we take a view defining such supporting conditions as enabling, i.e. social structures opening up possibilities for actions. More properly, our view encompasses the set of social structures, within the organization, which makes a given actor more likely to settle on some possibilities out of those it enables, defined by Cardinale 22 as “orienting”. Following a well-established habit in the management literature, we keep these factors labelled as “enabling conditions,” rather than the niche (although more accurate) “orienting” wording.
Although some studies have shown how the development of professional identities and roles is relational, most research tends to look at contexts in which interactions take place within the professional community in the process of developing the professional, rather than the hybrid, identity. Among these, Pratt and colleagues 23 have analyzed the importance of socialization and role modelling when young doctors’ identities are developed. However, existing literature offers limited understanding of the conditions for the development of hybrids and the role of the social/organizational context in this process. Therefore, as argued by Denis and colleagues 24 it is necessary to overcome the focus on hybrid professionals’ response strategies that has prevailed in the literature and, following Noordegraaf, 7 to explore the relational dimension of healthcare professionalism, and its links with the outside world, organizational rationales and other professions. On this regard, Giacomelli 5 identified the “enabling conditions” and managerial levers as one of the perspectives through which the literature has looked at hybridization. In this review, however, different forms of enabling conditions are not untangled, as the scientific debate on this dimension is reported to be underdeveloped if compared with other lines of investigation (institutionalism and identity work).
Hence, understanding the factors enabling professionals and their hybridization is highly relevant not only for theory on hybrid professionalism, but also for practice, as it allows to understand if and how the process of managerial role-taking might be supported. As strategies to reconcile dual-logic dilemmas depend massively on context, identifiying specific managerial and organizational tools can help professionals-managers in “mak[ing] decisions by providing them with evidence and agreed-on criteria, thus relieving them from having to weigh the different considerations based only on their own values and knowledge”. 25 This is the reason why one of the aims of this work is also to favour the contacts between organization studies literature with the world of health services and policy research.
Hybrid professionals in healthcare
Numerous types of hybrids have been introduced in healthcare over time, both in the medical profession, with doctors being assigned different forms of managerial responsibilities, as clinical directors, medical directors, network managers,26,27 as well as in the nursing profession, 28 where nurses have been covering more and more management issues, from traditional line management responsibilities (in the form of training, organizing and monitoring the work of other nurses to deliver patient care) to an increasing expansion towards budgetary management and leadership roles. 29 As a matter of fact, case treatment calls for greater collaboration with other internal organizational constituencies to increase continuity of care, quality and speed; external stakeholders call for accountability, transparent performance reports and risk management; financial pressures require the definition of criteria for case prioritization, decisions regarding end of treatments, health technology assessment, etc.
As illustrated by Braithwaite and colleagues, 30 medical managerial hybrids have the potential to promote clinical governance, develop multi-disciplinary and inter-professional collaboration and reorganize services to achieve cost savings without compromising the quality of care. They can do it more effectively than general managers, who lack the understanding of clinical problems and the status and legitimacy among the professional community. Furthermore, they have the ethical drive to serve patients and their needs, and can understand the relevance of patient centeredness and new expectations from patients and their families. For these reasons, medical management has become a very fashionable topic for health policy-makers across a number of countries and the development of medical management competences is by now one of the goals of healthcare reforms across the globe. 31 Following the US example, firstly in the United Kingdom and then in a number of Western countries, medical managerial roles were introduced at the top of organizations and in intermediate layers. 32 Accordingly, a great effort has been placed on developing management training programs for doctors and (more recently) for medical students, due to the initiatives of Departments of Health, medical societies and medical faculties. Managerial training, in fact, has proven to make professionals interact better with the top management of health care organizations, by providing two-way vocabularies of practice (for instance, that of performance information) that let them speak the same language. 33
However, despite the political enthusiasm that brought the introduction of professional-managerial roles into most healthcare systems, staying in a hybrid position can be uneasy, and not all professionals are capable or willing to perform in these roles. Being a professional-manager does not automatically mean becoming a professional capable to bridge the gaps between the worlds of one’s profession and management and to incorporate new values into the traditional professional culture; accordingly, the responses of professionals to management and the practice of medical (or nursing) management greatly vary. 8 Many times, professionals resisted management as looked at “managerialization” as a threat and an impoverishment of medical culture, therefore being unable to find meaningful combinations of management and professionalism. 34 Other times professionals adopted subtle strategies of resistance, as they retained those external facets typical of formal management roles, but did not conform to managerial practices substantially.35,36 Often doctors accepted formal management responsibilities just to gain a new source of power to pursue self-interest, 37 without really engaging in management and making it more difficult for executives to coordinate their behaviours. In a number of instances, however, medical professionals succeeded in negotiating and merging professionalism and management, making these values compatible, and developing hybrid identities.1,4,38
Methods
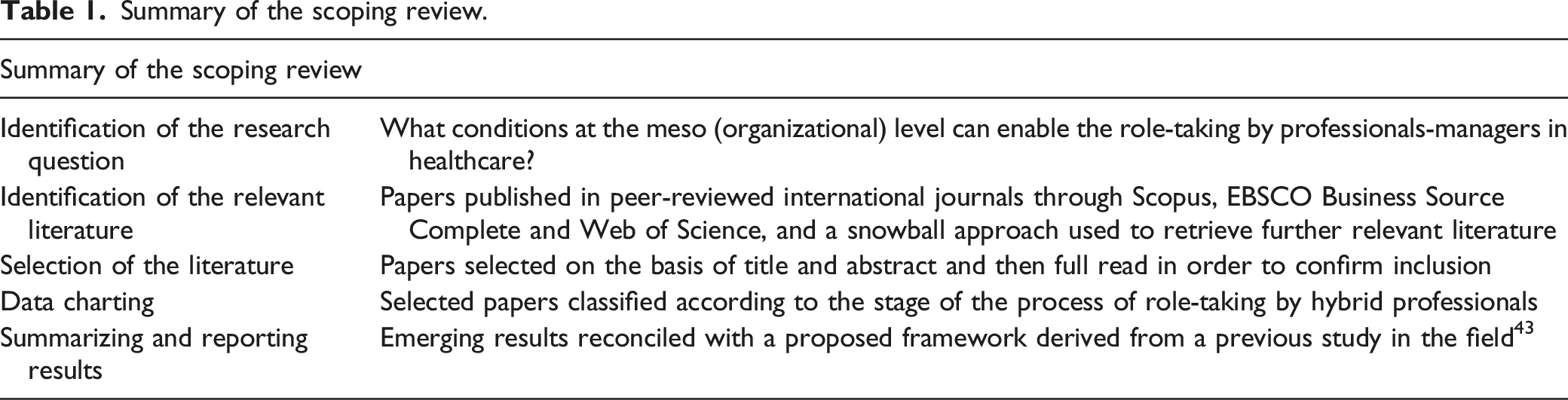
In order to achieve the above-mentioned goal, we carried out a scoping literature review 39 starting from the results of a previous study 5 which identifies contributions in the field of public management regarding the enabling conditions of hybrid professionalism.
A scoping literature review is considered appropriate when the object of analysis is broad and, thus, it is difficult to define the boundaries of the review. 39 Here, the object of analysis (i.e. the enabling conditions for hybrid professionalism) would have not been clearly identifiable in the search strategy phase as it is an ex post classification of quite differentiated contents, namely all those structures opening up possibilities for actions or making a given actor more likely to settle on some of those possibilities. Therefore, we built on the papers identified by a previous study 5 as the starting point of the scoping review and then extended it according to a snowball approach, that is explained below. Furthermore, our aim was to develop a framework for classifying practices in healthcare management to support professionals taking up a managerial role, rather than assessing the quality of research in a specific field (for which a more suitable approach would have been a systematic review). A scoping approach, on the other hand, is deemed particularly fit-for-purpose when there is a need to map ‘the key concepts underpinning a research area and the main sources and types of evidence available’. 40 Adopting a scoping review is considered as a useful method in the management field, ‘when there is the need for analysing broader areas of research and it is not easy to set precise boundaries in advance’ 41 and has recently been adopted in other studies in health services. 42
We focused on papers examining what conditions at the meso level of organization - in between institutions and individuals - can enable the effective role-taking by professionals-managers in healthcare. To this end, we first included papers identified in a previous systematic literature review as resonating with the dimension of the enabling conditions 5 ; we then replicated the search strategy adopted in that review in order to complement its results with the contributions published from 2018 on (i.e. the timeframe not covered by the original review). Lastly, we included further relevant contributions citing or cited by the resulting papers. Overall, we selected 34 papers published in international peer-reviewed journals (details can be found in the Appendix).
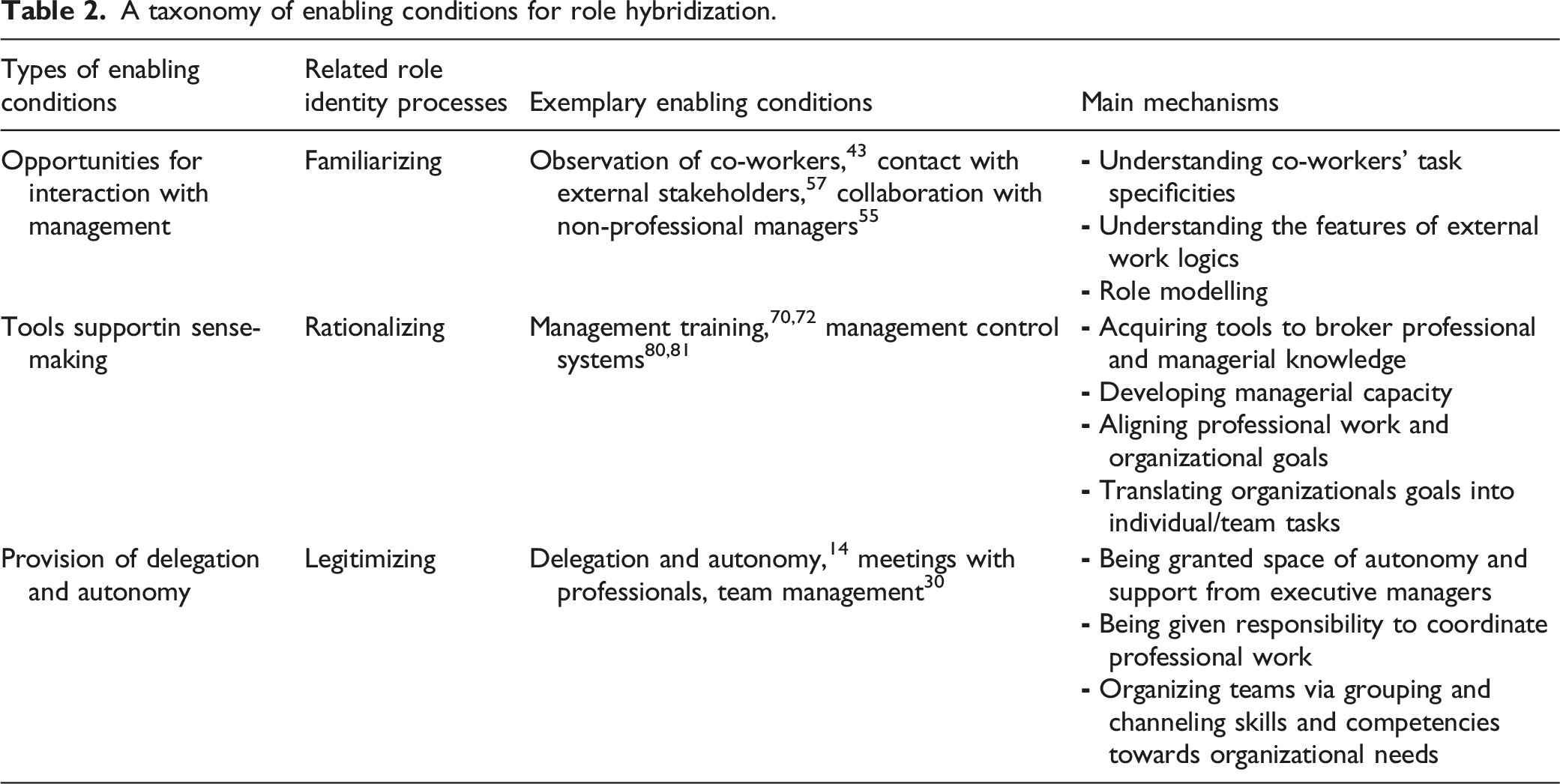
We then classified the emerging results in clusters, each representing a different set of conditions enabling the effective exertion of a hybrid role.We eventually reconciled the emerging results with the taxonomy proposed by Sartirana and colleagues 43 ; which we found relevant for understanding how processes of identity work are enacted by hybrid professionals in the healthcare sector. We used the distinction between these processes, namely familiarizing, rationalizing and legimitizing, as a theoretical complement for developing our framework and reinforce a theoretical connection with our inductive analysis. Sartirana and colleagues 43 define familiarizing as the acquisition of knowledge of managerial practices, rationalizing as the understanding new meanings of the professional self, and legitimizing as the development of social and cultural capital providing hybrids with credibility. As these three processes have a strong relational dimension, Sartirana and colleagues 43 identified various dynamics of interaction with organizational actors that can support hybridization. In particular, based on their interviews in a Dutch teaching hospital, they found observation of co-workers and feedback exchange, discussion with senior hybrids and external experts, and receiving back up by executives, as enabling factors for the three processes of identity work, respectively. In revising the literature, we found that this framework, developed to understand the factors supporting hybrids in a specific context (clinical directors in a tertiary care facility with a managerialized culture) had the potential to be broadened and used to classify existing literature on the enabling conditions for hybridization, irrespectively of the geographical/organizational setting. Therefore, we identified categories with the potential to embed groups of coherent enabling conditions, namely: opportunity for interaction with management, tools supporting sense-making, and provision of delegation and autonomy.
Summary of the scoping review.
Results of the literature review: The enabling conditions for hybrid professionals in healthcare
Hybridization processes have been studied thoroughly in the healthcare domain, mostly dwelling into either the underpinning sets of values, i.e. the institutional logics,44–46 or the identity work dimension,47–49 leading to patterns of variously mixed combinations of professional and managerial identities 50 . Less attention has been paid to how meso-level organizational factors mediate the macro-level circumstances into the microprocesses of role identification. 19 However, professionalism operates ‘both as an ideology or a belief system at the macro level and as a control mechanism of individual practitioners at the micro level’ 51 : hence, the role of organizational design choices and managerial tools is likely to represent a valuable key to interpreting the effectiveness of role-taking by the hybrid managers in healthcare. We focus on such meso-level set of interventions, that we label organizational enabling conditions, 5 and briefly present the findings of the extant research in the field in order to propose an interpretative, practice-oriented taxonomy.
A taxonomy of enabling conditions for role hybridization.
Seemingly, complexity factors such as differentiated professional groups’ priorities, 52 nuances of the local context 53 or the specific administrative tradition 54 should be always accounted for, and extreme caution have to be paid towards easy-way ‘to-do list’ approaches.
Opportunities for interaction with management
Quite broad evidence has been collected about the factors that enable professionals to interact with management, first of all with regard to the process of learning through feedback exchange and observation of co-workers 43 and frequent collaboration between professional and non-professional managers.55,56 Although existing research on professional identity have looked at the role of interdependencies of hybrids mainly within their professional community, 1 scholars have recently hihglighted the importance of the interactions between professionals and business managers in the creation of hybrid identities: indeed, interactions occurring in private relational spaces can ease the questioning of the consolidated professional self and allow for identity change 57 and eventually letting go with traditional identities. 49 For instance, Reay et al. 57 acknowledged the gap in current literature in which “the importance of interactions between professionals and others has been relegated to the background”, showing the potential for change to be orchestrated by others, i.e. business managers, who supported doctors in incorporating managerial values. They found that business and nurse “managers purposefully planned opportunities for interaction, engaging in strategically oriented meetings and conversations that set out a pathway toward a new physician role identity”. 57 When broadening their network, hybrid managers accordingly broaden their working repertoire, as they have the chance to ‘derive a broader strategic picture of the organization’ and ‘progressively abandone[d] short-term, tactical and specialty-oriented approaches to management’. 43 Furthermore, thanks to interactions with the members of the division management team, professionals can see the complementarities between clinical and managerial work in fields like care pathways, ICT innovations, and receiving feedbacks they can identify thise managerial practices and styles that can be more effective to run a professional organization. 43
From an organizational design standpoint, facilitating social interactions across professional groups is relevant for engaging in management also those professionals that can be more reluctant towards hybrid roles: the Covid-19 pandemic has shown that, when professionals are exposed to work environments they are not used to (that is the case, for instance, of specialized clinicians assigned to Covid-dedicated wards, during the peaks of the emergency in 2020), traditional professional barriers tend to loosen and melt, easing the integration of skills towards common goals. 58 When organizational structures and work practices favouring “professional melting” are in place, a reconfiguration of professional identities towards novel organizational values can be enabled.
Tools supporting sense-making
Once the competencies and practices of interaction across professional groups and between professions and management have been developed, the following cluster of organizational conditions and circumstances needed for enabling hybrid roles concerns the process by which professionals-managers make sense of their hybridity. Sense-making is inherently linked to the need to unravel a situation of uncertainty and ambiguity 59 : the underpinning rationale is that the actions of managers are founded upon the meanings of situations and information they face. When such situations are ambiguous, as in the case of hybrids, individuals need to develop their situated understanding of reality into a more organised perception 60 which can help them navigating ambiguity. This process is usually retrospective, as one makes sense largely from reflections on previous experiences 59 : the basic idea, in the words of Weick himself, is “that reality is an ongoing accomplishment that emerges from efforts to create order and make retrospective sense of what occurs”. 61 On this regard, based on the available literature in the field, we argue that organizational enabling conditions which help hybrids interpreting and organizing role-related ambiguity can be grouped into two main clusters: management training and management control practices.
When lacking sound management skills and competencies, hybrids’ understandings and enactment of their roles tend to draw solely on professional norms, organizational formal rules and practical routines,62,63 leading to a passive transposition of the external requirements of the context. However, when training about managerial competencies is in place but it follows a polarizing approach to the professionalism-managerialism dyad, this may ultimately fail to produce the desired results: as observed by Kuhlmann and von Knorring 64 with regard to managerial education for clinicians, ‘if the values of professionalism being necessarily opposed to those of management and markets is what is taught, medical education will not help young doctors to connect medicine and management’ (ibidem). Once overcome a dialectic approach opposing profession to management, investing thoroughly in management training - besides supporting professional self-efficacy65,66 and triggering effects referred to as informative and capacity-building 67 - can indeed be supportive in giving the hybrids ‘translational’ 48 capacity and making them broker different sources of knowledge: 68 understanding the ‘words of management’ can indeed facilitate hybrids’ in acting as a credible partner towards both the professional community and the top management. 33 Nowadays, professionals feel more and more “ready to play the role of manager” 69 mainly due to the formal training requirements put in place in several national contexts to take-on managerial roles. Still, within training programs for healthcare professionals, technical skills such as planning, organization and resource management outnumber interpersonal and decision-making skills. 70 Moreover, it should be noted that medical and nursing schools still lack offering adequate management and leadership training 71 and the burden of providing professionals with managerial skills still falls mainly on healthcare organizations. 69 This is highly dependent on contingent factors shaping the modes of training for healthcare professionals, with striking differences both across national systems and - sometimes - also at an intra-national level: such factors include, just to name a few, the existence (or not) of a leadership competency framework, the institutional location (national or regional) of professional education and training, the availability (or unavailability) of extra-currucular training, and the nature of the provider in charge of it. 72 Hence, a multifaceted approach to developing managerial capacity in healthcare is needed, and undoubtedly requires to consider ‘a bundle of different interventions and strategies’ which should be tailored to the given context. 73
On the other hand, one of the competencies required nowadays to professionals-managers to take on their hybrid role is evidence-informed decision making33,74,75: this has much to do with the nature of performance information as boundary object, as it ‘enables alliances between actors helping them to highlight their own interests’ and find compromises. 76 Shand and Callen 77 also take this view and discuss what kind of information is needed for hybrids: information is shown to support effectively the hybrid role of the professionals-managers in healthcare when is timely, graphically interpretable and comparative. Recent research in the field has shown indeed that information framing can be a powerful tool to align professionals’ behaviors towards common – typically patient-centered – goals.78,79 With regard to management control, Macinati and colleagues80,81 discuss also that the procedural factors can influence hybrids’ role enactement: participative budgeting practices can indeed enhance hybrid managers’ self-efficacy by supporting their belief to “have the capability and resources to perform successfully in managerial tasks”. 80
Provision of delegation and autonomy
Once having made sense of the hybrid role through managerial training and management tools, professionals-managers are called upon to exercise it by spreading its potential throughout the organization. Legitimacy concerns social actors being empowered to act on accepted grounds and relieved of justifying their choices and actions. 82 This is even more crucial for hybrids, as their role acts in contested fields where the sources of legitimacy are tensional because of controversial norms, values, and beliefs. 83
Various forms of enabling conditions were found by the literature. Healthcare organizations can set up roles and organizational practices that support hybrid managers in performing their manageriale role. First of all, as shown by Sartirana and colleagues; 43 organizational leaders can reduce hybrids’ perception of being just a “first among equals” by providing them with effective delegation of managerial responsibilities, as well as autonomy in decision making. This is particularly relevant for hybrids who reduce the involvement in clinical practice, therefore compromising the main source of legitimacy and status within a professional organization.
Furthermore, organizations can provide opportunities for hybrids to be recognized by professional peers. This happens typically via forums 84 which allow the transfer, translatation and transformation of knowledge across functional and professional boundaries. 85 The usual form of such organizational forums, widely discussed in literature, are meetings with colleagues: regular meetings can act as “managerial vehicles” 30 and be a valuable mechanism for legitimizing the position of hybrid managers. Since the lack of proper interaction between frontline professionals and managerial positions cannot prevent a certain perception of organizational detachment from arising, team autonomy recognition could act as a buffer for professionals who perceive an uncongenial workplace and still channel individuals’ commitment to patient care. 56
Finally, quality and accountability standards can also be leveraged on for legitimacy purposes by specific professional groups: this is the case of those professions engaged in a long “battle for recognition”, 86 which could make use of evidence-based practices in order to pursue a dual interest, that of benefiting patients and strengthening legitimacy both for the profession per se and for the managerial status arranged to professionals in the occupational group.
Discussion
Most existing literature has seen professionals as passively influenced, in an overly deterministic way, by traditional professionalism, 34 with its strong institutionalized pressures of normative socialization. 9 In this scenario, professionals in hybrid roles would be called to exert agency acting as “heroic” individuals in a lonely strive to reconcile alternative logics, 87 and they can succeed or not. However, an organizational context providing opportunity for engagement in management is necessary for enabling hybrids’ capacity and willingness towards the reshaping of individual identities. Therefore, we need to look beyond individual hybrids towards the organizational context in which hybridization processes are embedded.
In this review we have identified those contributions that presented evidence on the conditions for the development and effective enactment of hybrid roles, and developed a framework aimed at classifying this literature. We draw on the work of Giacomelli, 5 in which the enabling conditions perspective was identified as a quite niche line of research in the field: we follow in the wake of this study to provide a more grounded classification, which basically aims to zoom in on the image and add some details, within a field that is less unexplored than it seems, but in which the contributions were probably unorganized.
When analyzing the literature, we used as starting point a taxonomy originally developed to classify forms of social interactions accompanying the processes of hybridization of clinical directors in public training hospitals. Although Sartirana and colleagues 43 claim that “as a single case study of professional managerial hybrids in a Dutch hospital, our study may have limited empirical generalizability” (ibidem: 1208), we have shown that it can be adopted as a more encompassing framework to classify the existing – although still limited – literature on the topic, across countries and health systems.
Furthermore, we believe this adds value to the academic debate, as it shows not only that the development of professional identities is inherently relational, but so are the processes through which the organization influences it. All the organizational and management tools highlighted here, in fact, are characterized by a strong relational orientation, and it could not be otherwise: especially in a highly institutional context such as the healthcare, where individuals themselves are carriers of different institutional logics, 88 the form of social interactions can be substiantially reflected into the organizational arrangements. As obvious as it may seem, value creation in healthcare does not respond to compartmentalization, and this is now taken for granted in managerial practice, where terms such as “value-based healthcare” and “patient-centered medicine” are routine. Moreover, the recent experience of the Covid-19 pandemic has accentuated the need to overcome the traditional rigidity of professional organizations, in favor of a more interdisciplinary and multidisciplinary model. 89 However, academic research in the field of hybrid professionalism seems to struggle to expand on the organizational level of the discourse, beside those - well developed - of macro institutional logics and identity work micro-processes.
Indeed, this work shows the importance of a contextual understanding of hybridization processes, and this is relevant for supporting this transition. It is necessary to contrast the “standardization” of medical management policies internationally, which strives to implement NPM-inspired reforms with similar hospital organizational structures and managerial roles across (sometimes very) different countries. Change, and especially that carried out in complex public professional organizations, cannot be achieved by reforms alone, but requires careful and contextualized implementation processes. It is necessary to avoid managerialistic perspectives in health policy, in some cases supported by the action of external agents, which risk to be conducive to a standardization of organizational structures and managerial tools, irrespectively of local contexts.
Implications for practice in healthcare
We have seen that the enactment of a range of support strategies can favour hybridization and overcome the traditional reluctance of professionals to engage with management. Following is a number of implications for health policy-makers and managers.
First of all, a number of interventions in hospitals’ organizational structure and management systems can support the rationalization process of hybid identities. It is the case, for instance, of proper design of physical layouts and workplace innovations, 90 as hospitals in which outpatient services, wards and operating theatres are shared, spaces are designed to favour interdisciplinary and interprofessional encounters, horizontal pathways or care centres are formalized, multidisciplinary teams meet regularly, greatly support the early nurturing of organizational competencies among doctors. Also, the presence of quality programs and standards of practice, as well as the availability of clinical indicators and patient satisfaction data, makes evident the alignment between managerial decisions and professional priorities.
Further, appropriate selection mechanisms should be in place to identify candidates for formal managerial positions. Assessment schemes, appraising not only clinical competence but also managerial experiences or potential should be used. Also, job interviews might include a presentation of a strategic plan for the directorate/division, in order to appraise managerial competencies and identify clear performance indicators for the mandate. At the same time, appropriate support for formal doctors-in-management roles should be provided. Too often non-medical staff working in hospitals and supporting doctors have inadequate professional background, with an administrative education but without the managerial capabilities and the diverse professional experiences necessary to govern the large endowments of resources which exist in hospitals. The presence of management teams supporting hybrid roles, providing them support, feedback, as well as operational assistance, is paramount. Open feedback provision is greatly favoured by hospital cultures, where the value of different professions is acknowledged, i.e. where nurses or administrative staff are provided with the legitimacy to interact with doctors at the same level, and where new ideas as well as problems can be openly reported and discussed. Formal training programs in management for high calibre professionals, which are already in place in several countries, can also be effective for providing knowledge of managerial tools, time for thinking on professional practice as well as exchange of experiences with colleagues. However, coaching and mentoring programs allowing deeper personal reflection and sensemaking appear even more effective to accompany professionals in their identity transition over time.
Hospital top managers should also be willing to invest in hybrid professional-managerial roles, delegating some of the leverages of power to intermediate organizational layers. Although this entails taking up the risk of slowing down processes or being exposed to opportunistic professional behaviours. However, having direct communication channels, providing professionals with autonomy, human and financial resources, as well as support and backing in “uneasy” decisions, appears necessary for favouring an effective hybridization and legitimizing new roles within the professional group and the organization. At the same time, it is necessary to create alternative career trajectories for those high value professionals who are incapable or unwilling to take up a managerial position. In many health systems managerial roles are the only career steps which can provide doctors with adequate financial reward and status. It is necessary to devise professional career advancements, provided with internal and external visibility, as well as salary increase, available for those professionals that are not suited or not willing to become managers.
However, some implications can be drawn also for professionals and professional associations. Although hybrid management is well developed worldwide, still professionals – and most notably their organized groups – tend to see managerialization as a threat. A cultural shift should be done thanks to the understanding that hybrid management is not about dismantling professionalism, but rather about reconfiguring it. In particular, issues like safety, quality and patient centeredness can be seen as both managerial and professional problems: finding new work processes capable to effectively address these issues can become a relevant point in the agenda of all doctors.
This can be done in many different ways. First of all, health education reforms should introduce training of management and organizational capabilities in schools and residency programs. This responds to the professional need of aligning medical education with the shifting health needs and socio-economic demands. On one side, it is necessary to favour the development of educational training programs capable to develop soft skills, teamworking, interprofessional collaboration.
At the same time, it is necessary to foster an “organizational” sensitivity, supporting medical students in the development of an understanding of the overall process of patient care, interdisciplinary and not necessarily hospital based. An interesting avenue, as also suggested by Plochg and colleagues, 91 is to favour the incorporation in training programmes of “values” from the field of public health in the conventional set of professional values of hospital doctors. This would require to move from disease-oriented services to person-oriented services, and to think at new forms of organizing health services that consider multimorbidity rather than individual diseases and disciplines.
Training on-the-job in organizational issues is also extremely relevant, and it is an interesting area for educational innovation. Effective experiences should be spread, like the one reported by Noordegraaf and colleagues 92 in which medical residents of different specialties within a hospital meet periodically to report organizational problems and discuss possible solutions, in order to engage as soon as possible in management of people and resources.
Future directions for research
First of all, despite the relevance of hybrid roles, it is necessary to further explore the new forms in which management and professionalism are accommodating. Hybridity itself is not a homogenous concept. In the past, the focus had been placed on hybrid roles, filled by hybrid managers provided with resources and responsibilities. Increasingly, the focus is shifting towards hybrid processes and hybrid work practices, in which organizational and professional action not only coexist but coincide, and in which the focus is placed on connectivity within the organization, engagement with stakeholder as well as adherence to standards of practice. As a matter of facts, in the last years a number of hospitals started introducing reforms towards process based and patient-centered structures, as well as resource sharing, that were welcome by doctors in management and clinical directors more than vertical managerial approaches typical of the previous years. Also, favoured by new hospital layouts, new forms of medical management, which can be referred to as disease management, 93 are now present in daily work processes including quality management, safety procedures, multidisciplinary work, patient centered work design. Accordingly, international scholars started to suggest theoretical development to the notion of hybridity. In the last years the contributions of Martin and colleagues 17 and especially Noordegraaf, 3 who introduced the concept of “organizing professionalism”, have been picturing a different and promising view to study hybridity in relation with the organizational contexts.
Further, the study of hybridization “in context” might benefit from more interactions between the literature on professionalism and identity with leadership research, and especially the studies on plural leadership and co-leadership in contexts characterized by institutional complexities. A recent promising research developed by Gibeau and colleagues 94 on medical-managerial co-leadership, hinting at logics combining professionalism and managerialism, echoes the concepts of reconfigured and redefined professional work used in other literature.
Attempts to develop studies linking theories of professionalism and research into human resource management practices could also be worthwhile. We still know very little about the impact of HRM in professional organizations, characterized by status hierarchies and power, and the role of legitimacy and occupational status as a constraint or a source of motivation has not been studied in the context of the Ability-Motivation-Opportunity perspective. 95 With reference to skill-enhancing and motivation-enhancing practices that can support professionals in taking up the managerial hybrid role, the work by Currie and colleagues 52 represents - at the best of the authors’ knowledge -a stand-alone example under this respect. It would be extremely interesting to dispose of more research studying the impact of practices like training systems, talent management, incentives as well as career development systems, in supporting professionals, both in the early experiences with managerial engagement as well as when they take up hybrid managerial roles. Of course, this requires an approach to human resource management capable to take into consideration the context and to balance methodological rigour with relevance.
Eventually, it would be interesting to broaden existing understanding of hybrid professionalism across different countries and health systems. More comparative studies should be developed to explore convergence and divergence in the adoption of medical management models and the ways in which similar organizational structures and roles are translated, becoming ‘dis-embedded from their original context and re-embedded in the context of adoption’. 31 Future research may investigate these arguments also in other domains within healthcare, e.g. non-hospital doctors and nurses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Note
Database of the selected papers (records displayed by first author’s alphabetical order).
Authors
Title
Year
Journal
Aufegger L., Alabi M., Darzi A., Bicknell C
Sharing leadership: Current attitudes, barriers and needs of clinical and non-clinical managers in UK’s integrated care system
2020
BMJ leader
Bartram T., Stanton P., Bambe, G. J., Leggat S. G., Ballardie R., Gough R
Engaging Professionals in Sustainable Workplace Innovation: Medical Doctors and Institutional Work
2020
British journal of management
Bellé N., Giacomelli G., Nuti S., Vainieri M
Factoring in the human factor: experimental evidence on how public managers make sense of performance information
2021
International public management journal
Braithwaite J
An empirically-based model for clinician-managers' behavioural routines
2004
Journal of health organization and management
Burgess N., Currie G
The knowledge brokering role of the hybrid middle level manager: the case of healthcare
2013
British journal of management
Burgess N., Strauss K., Currie G., Wood, G
Organizational ambidexterity and the hybrid middle manager: the case of patient safety in UK hospitals
2015
Human resource management
Correia T., Denis J.L.
Hybrid management, organizational configuration, and medical professionalism: Evidence from the establishment of a clinical directorate in Portugal
2016
BMC health services research
Currie G., Burgess N., Hayton J.C.
HR practices and knowledge brokering by hybrid middle managers in hospital settings: the influence of professional hierarchy
2015
Human resource management
Currie G., Finn R., Martin, G
Accounting for the ‘dark side’ of new organizational forms: The case of healthcare professionals
2008
Human relations
Dwyer D
Experiences of registered nurses as managers and leaders in residential aged care facilities: a systematic review
2011
International journal of evidence-based healthcare
Ernst J
The curse of bureaucratisation or the blessings of professionalisation? Nurses’ engaged adoption of quality management in hybrid managerial positions
2019
Scandinavian journal of management
Fanelli S., Pratici L., Zangrandi A
Managing healthcare services: Are professionals ready to play the role of manager?
2021
Health services management research
Fung KK.W.
Physician managers in Hong Kong public hospitals
2020
Journal of health organization and management
Giacomelli G., Ferré F., Furlan M., Nuti S
Involving hybrid professionals in top management decision-making: How managerial training can make the difference
2019
Health services management research
Gilbert M.H., Dextras-Gauthier J., Fournier P.-S., Côté A., Auclair I., Knani M
Organizational constraints as root causes of role conflict: The situation of physician-managers and their responses
2019
Journal of health organization and management
Hartley K
Untangling approaches to management and leadership across systems of medical education
2016
BMC health services research
Jacob R. R., Duggan K., Allen P., Erwin P. C., Aisaka K., Yang S. C., Brownson R. C
Preparing public health professionals to make evidence-based decisions: a comparison of training delivery methods in the United States
2018
Frontiers in public health
Keijser W., Poorthuis M., Tweedie J., Wilderom C
Review of determinants of national medical leadership development
2017
BMJ leader
Kendrick M., Kendrick K.B., Taylor N.F., Leggat S.G.
A qualitative study of hospital clinical staff perceptions of their interactions with healthcare middle managers
2021
Journal of health organization and management
Kuhlmann E., von Knorring M
Management and medicine: why we need a new approach to the relationship
2014
Journal of health services research & policy
Lega F., Prenestini A., Rosso M
Leadership research in healthcare: A realist review
2017
Health services management research
Liang Z., Leggat S.G., Howard P.F., Koh L
What makes a hospital manager competent at the middle and senior levels?
2013
Australian health review
Macinati M.S., Bozzi S., Rizzo M.G.
Budgetary participation and performance: The mediating effects of medical managers' job engagement and self-efficacy
2016
Health policy
Macinati M.S., Nieddu L., RizzoM.G.
Examining the role of value congruence, professional identity, and managerial job engagement in the budgetary participation-performance link
2020
Health care management review
Nuti S., Noto G., Vola F., Vainieri M
Let’s play the patients music: A new generation of performance measurement systems in healthcare
2018
Management decision
Nzinga J., McGivern G., English M
Hybrid clinical-managers in Kenyan hospitals: Navigating between professional, official and practical norms
2019
Journal of health organization and management
O'Riordan C., McDermott A
Clinical managers in the primary care sector: do the benefits stack up?
2012
Journal of health organization and management
Quartz-Topp J., Sanne J.M., Postges H
Hybrid practices as a means to implement quality improvement: a Comparative qualitative study in a Dutch and Swedish hospital
2018
Health care management review
Ravaghi H., Beyranvand T., Mannion R., Alijanzadeh M., Aryankhesal A., Belorgeot V.D.
Effectiveness of training and educational programs for hospital managers: A systematic review
2021
Health services management research
Reay T., Goodrick E., Waldorff S.B., Casebeer A
Getting leopards to change their spots: Co-creating a new professional role identity
2017
Academy of management journal
Sartirana M., Currie G., Noordegraaf M
Interactive identity work of professionals in management: A hospital case study
2019
Public management review
Sarto F., Veronesi G., Kirkpatrick I
Organizing professionals and their impact on performance: The case of public health doctors in the Italian SSN
2019
Public management review
Shand S., Callen J
Management information needs of clinician managers in a metropolitan teaching hospital
2003
Health information management
Williams S.J., Radnor Z., Aitken J., Esain A., Matthias O
Transferring, translating and transforming knowledge: The role of brokering in healthcare networks
2021
Journal of health organization and management