
Abstract
Objective
In this study, we aimed to assess the epidemiological profile and associated risk factors of malaria in Boset District using clinical records from the Boset District Health Office Central Surveillance Unit, East Shawa Zone, Oromia, Ethiopia.
Methods
This health facility-based retrospective cross-sectional study included clinical malaria data for 5 years (2016–2020) recorded at all public and private health facilities in the district.
Results
The present study revealed an overall malaria slide positivity rate of 12.4% (21,059/169,986), ranging from 23.3% to 5.3% during 2016–2020 in Boset District. Malaria cases were recorded in all age groups, but individuals aged 15 years and above accounted for a higher (56.2%) average proportion of malaria cases. Concerning the relative proportion of malaria parasite species, Plasmodium falciparum was slightly predominant (58%) over P. vivax (42%).
Conclusion
The present study revealed a declining trend in malaria cases over the 5-year study period in Boset District. Scaling up the available malaria prevention strategies and control measures is recommended to achieve malaria pre-elimination.
Introduction
Malaria is a life-threatening infectious disease caused by the protozoan parasite Plasmodium. Despite the significant reduction in malaria cases achieved by 2020, over 241 million cases of malaria and 627,000 malaria-attributable deaths occurred worldwide in the same year, among which 95% of cases and 96% of deaths occurred in Africa. 1 Although there has been a considerable decline in malaria incidence since the year 2000, the disease remains a public health threat in areas where malaria is endemic, especially in Sub-Saharan African countries, which experienced an expansion of malaria in 2019 in comparison with 1990. 2
Plasmodium falciparum and Plasmodium vivax are among the five Plasmodium species known to infect humans, with a high prevalence and wide distribution in Ethiopia. It has been reported that 60% and 40% of all reported malaria cases are caused by P. falciparum and P. vivax, respectively. 3 Studies have found that malaria is among the 10 leading causes of morbidity and mortality in children under age 5 years in Ethiopia. 4
Malaria transmission is very heterogeneous, seasonal, and unstable across Ethiopia,5,6 and transmission intensity varies according to landscape and climate. Transmission peaks bi-annually from September to December and from April to May, coinciding with the main harvest seasons. 5 Studies have reported that certain variables are strongly associated with the transmission of malaria elsewhere in the world. Human-induced risk factors, such as water resource developments and the presence of dams, have been reported to intensify malaria transmission in lowland and midland ecological settings of Ethiopia. 7 Accordingly, studies have revealed that the mean monthly malaria incidence is generally higher in villages near dams than in those further from a dam. 8 Similarly, studies in the Tigray Region of northern Ethiopia report that the overall incidence of malaria in villages close to a dam is higher than that in communities far from a dam. 9
Recent studies report that Ethiopia has achieved the target 50% reduction in malaria incidence, which is among the Millennium Development Goals. 10 The country is on track for a further 40% reduction in malaria incidence (along with Rwanda, Zambia, and Zimbabwe) and malaria mortality rates (together with Zambia) by 2020. 11
Despite the substantial reduction in malaria morbidity and mortality in Ethiopia since 2001, the case incidence remains high, 12 and malaria remains the main cause of morbidity in the country, with 3,331,599 confirmed cases and 59,370 hospital admissions in 2012 to 2013. 13 Although its prevalence is relatively low compared with other African nations, the disease remains the leading cause of outpatient morbidity and is among the leading causes of inpatient morbidity. Recent studies have shown that malaria results in considerable adverse effects on the health and socioeconomic development of Ethiopia. 14 Despite the country’s commitment to its control program, malaria remains a huge challenge to the public health and economic sectors. The prevailing, conducive weather conditions coupled with tremendous socioenvironmental changes are believed to contribute to the surge in malaria throughout most areas of the country. Most importantly, irrigation schemes and water harvesting projects in malaria-endemic areas of Ethiopia represent serious challenges not only in terms of the establishment of year-round transmission but also for the occurrence of sudden outbreaks of disease.
Most areas in the East Shawa Zone, including Boset District, are among major centers with year-round irrigation farming of vegetables and fruits. Surface irrigation creates an environment conducive to mosquito breeding and proliferation, leading to stable transmission of malaria infection throughout the year. 15 Despite the favorable weather conditions and presence of irrigation farming, both risk factors for stable malaria transmission, there are limited reports with regard to the malaria prevalence and associated risk factors in Boset District, East Shawa Zone. Therefore, in this study, we aimed to assess trends in the malaria prevalence in Boset District.
Methods
Description of the study area
This study was carried out in Boset District, East Shawa Zone, Oromia Regional State, Ethiopia. Olanchiti is the main town in the district, with latitude and longitude 8°40′N 39°26′E and an elevation of 1436 meters above sea level. Olanchiti is located 25 km from Adama Town, in the middle of the Great Ethiopian Rift Valley, along the road from Addis Ababa to Dire Dawa (Figure 1). According to population projection data of the Central Statistical Agency, the total population of Boset District was estimated to be 189,795, with a 22.5% and 77.5% urban and rural population, respectively, in the year 2017. 16 The district receives between 621 mm and 1012.7 mm of annual rainfall and has an annual temperature of 14.3°C to 31.8°C, with heavy rains during the months of June to September and short rains in April and May. Boset District is a malarious area in this region. Malaria is a leading cause of morbidity and mortality, being among the 10 leading diseases reported in local health facilities. According to the Health Office of the district, there are currently 33 public health posts, 7 health centers, and 1 primary hospital (Olanchiti Hospital) in this area. The outpatient department of the hospital provides six main types of services: those for children under age 5 years and age 5 to 14 years (one program for each age group), services for patients aged ≥15 years, emergency services, and chronic disease evaluation and treatment. Inpatient department services include pediatrics, gynecology and maternity, internal medicine, and surgery. In addition to public health facilities, there are eight private health posts and clinics.
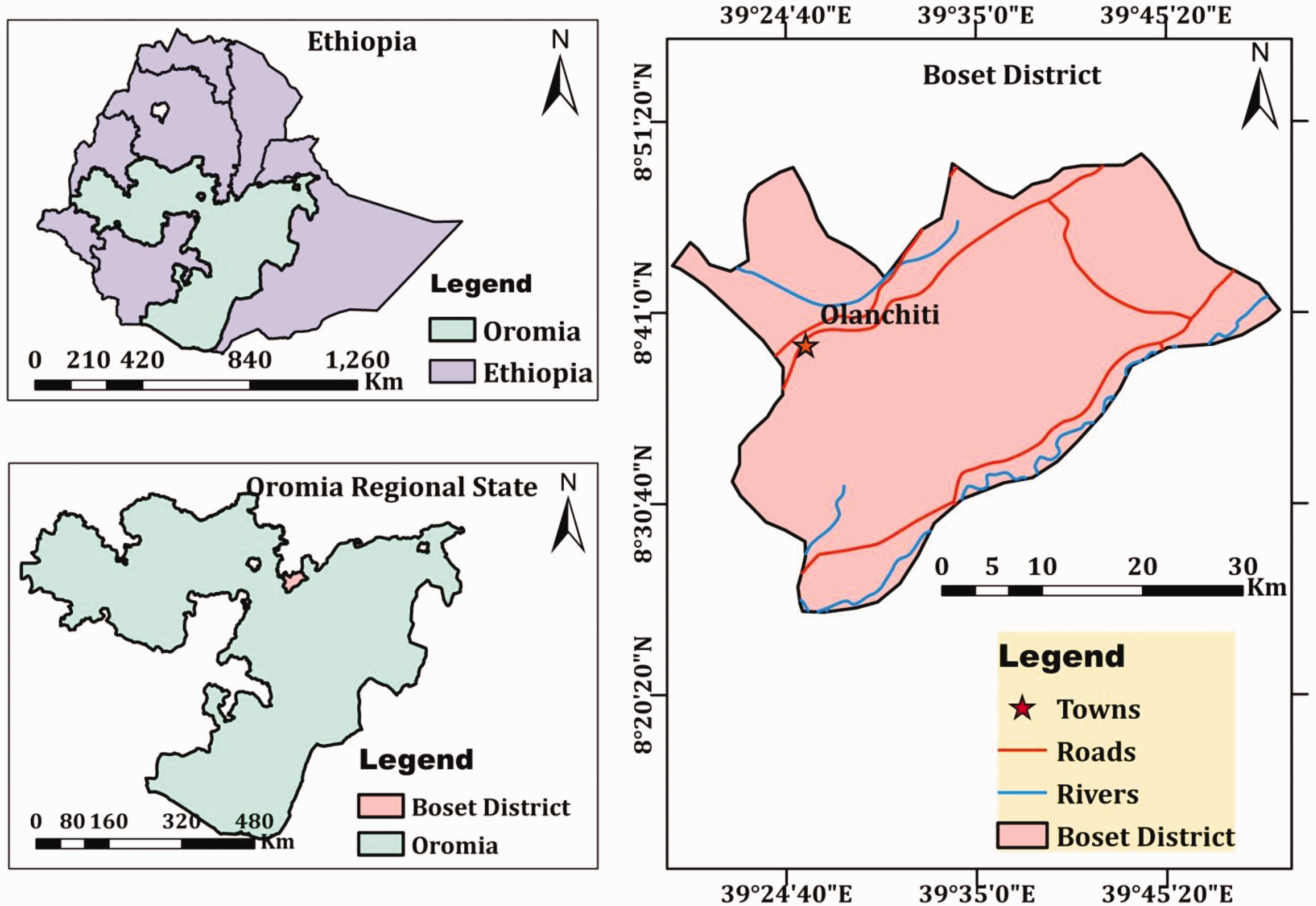
Map of study area, Boset District and Olanchiti Town (developed using Arc-GIS Desktop version 10.3.1; Esri, Redlands, CA, USA).
Study design and data collection
We conducted a retrospective study to analyze the malaria trends in Boset District, East Shawa Zone, using malaria data over 5 years (2016–2020) recorded in the surveillance database of the district. The data source was malaria cases confirmed microscopically and/or via rapid diagnostic test (RDT) in public and private health facilities as per the national guidelines for parasitological diagnosis of malaria. The extracted data were part of a report compiled by the zonal Health Office Central Surveillance Unit via district health offices, organized and managed using a health management information system. The present study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations for reporting observational studies. 17
Ethical approval
The data for this research were accessed after ethical approval was received from the Adama Science and Technology University (Certificate Ref. No. RECSoANS/BIO/04/2020. September 2020). Informed consent was not needed as there was no direct interaction with study participants. Only the data of treatment seekers was accessed.
Data analysis
Data collection was followed by proper data organization, analysis, and interpretation. Retrospective data were qualitatively and quantitatively analyzed to check the frequency and strength of the associations among variables using IBM SPSS version 20 (IBM Corp., Armonk, NY, USA). Results were considered statistically significant with p < 0.05.
Results
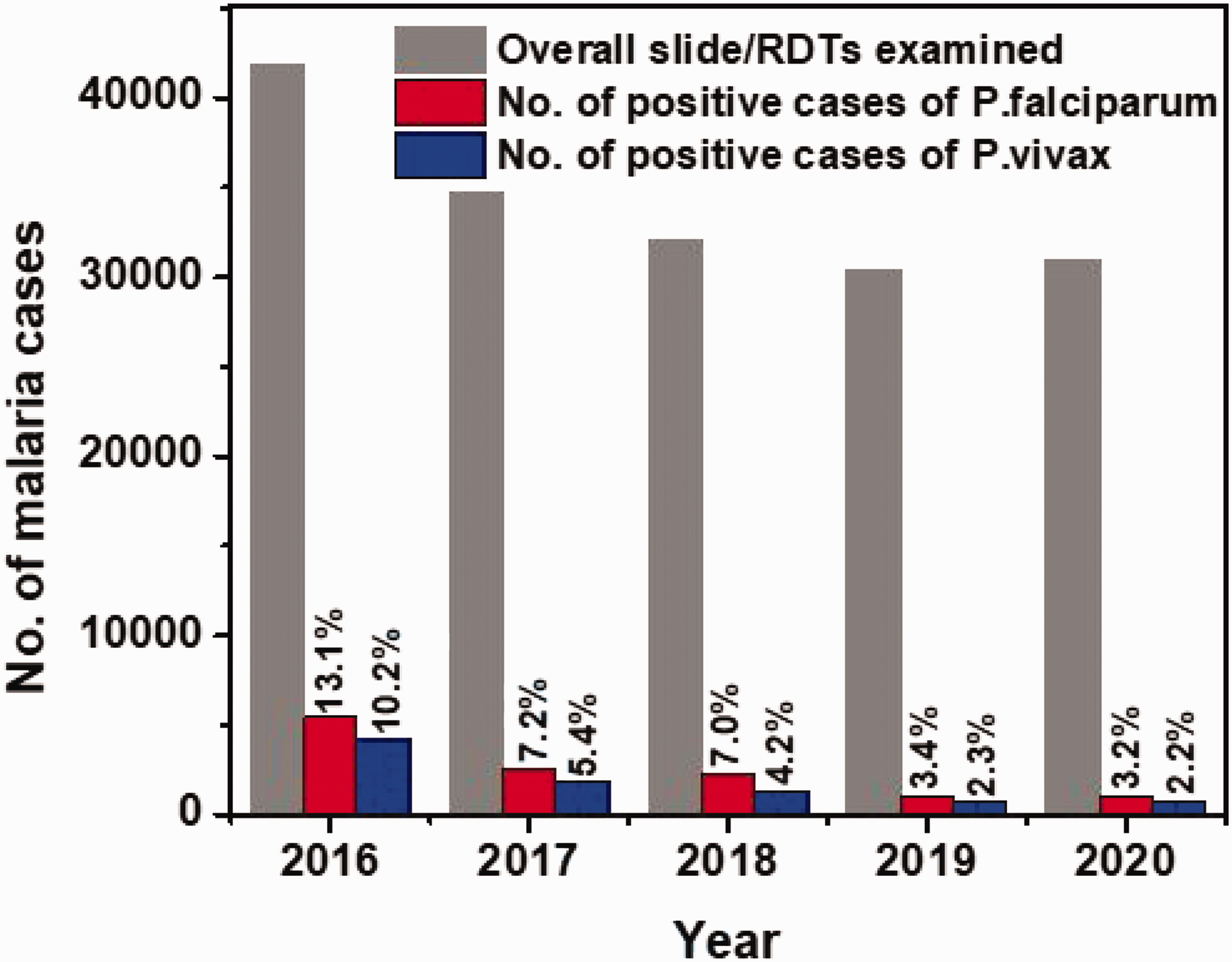
Among an overall 169,986 examined slides and/or RDTs, 21,059 (12.4%) malaria-positive cases were recorded during 2016 to 2020 in all public and private health facilities of Boset District. Among positive cases, 12,025 (57.1%) and 9034 (42.9%) were among male and female individuals, respectively. The data for mixed infection were incomplete and inconsistent between public and private health facilities; therefore, these data were excluded. The malaria trend in the district over the 5-year study period revealed a sharp decline in the slide positivity rate (SPR) from 23.3% (9728/41,815) in 2016 to 5.3% (1657/30,989) in 2020 (Figures 2 and 3).

Yearly trends of suspected and positive malaria cases in Boset District, Central Ethiopia, 2016 to 2020.
Malaria suspected cases versus the slide/rapid diagnostic test positivity rate by parasite species in Boset District, Central Ethiopia, 2016 to 2020.
As shown in Table 1, a higher SPR (14.0%) was observed in public facilities than in private health facilities (13.9%) and Olanchiti Hospital (7.5%).
Distribution of malaria cases in Boset District, Central Ethiopia, 2016 to 2020.

*Public health facilities refers to all public health centers and public health posts.
P., Plasmodium; RDT, rapid diagnostic test.
As shown in Figure 4, the malaria SPR by sex and age showed a considerable decrease over the 5-year period. With regard to age profile, the SPR was significantly higher for the age group ≥15 years (56.2%) than for other age groups (p < 0.01), as shown in Figure 5.

Percentage distribution of malaria-positive cases by sex and age in Boset District, Central Ethiopia, 2016 to 2020.
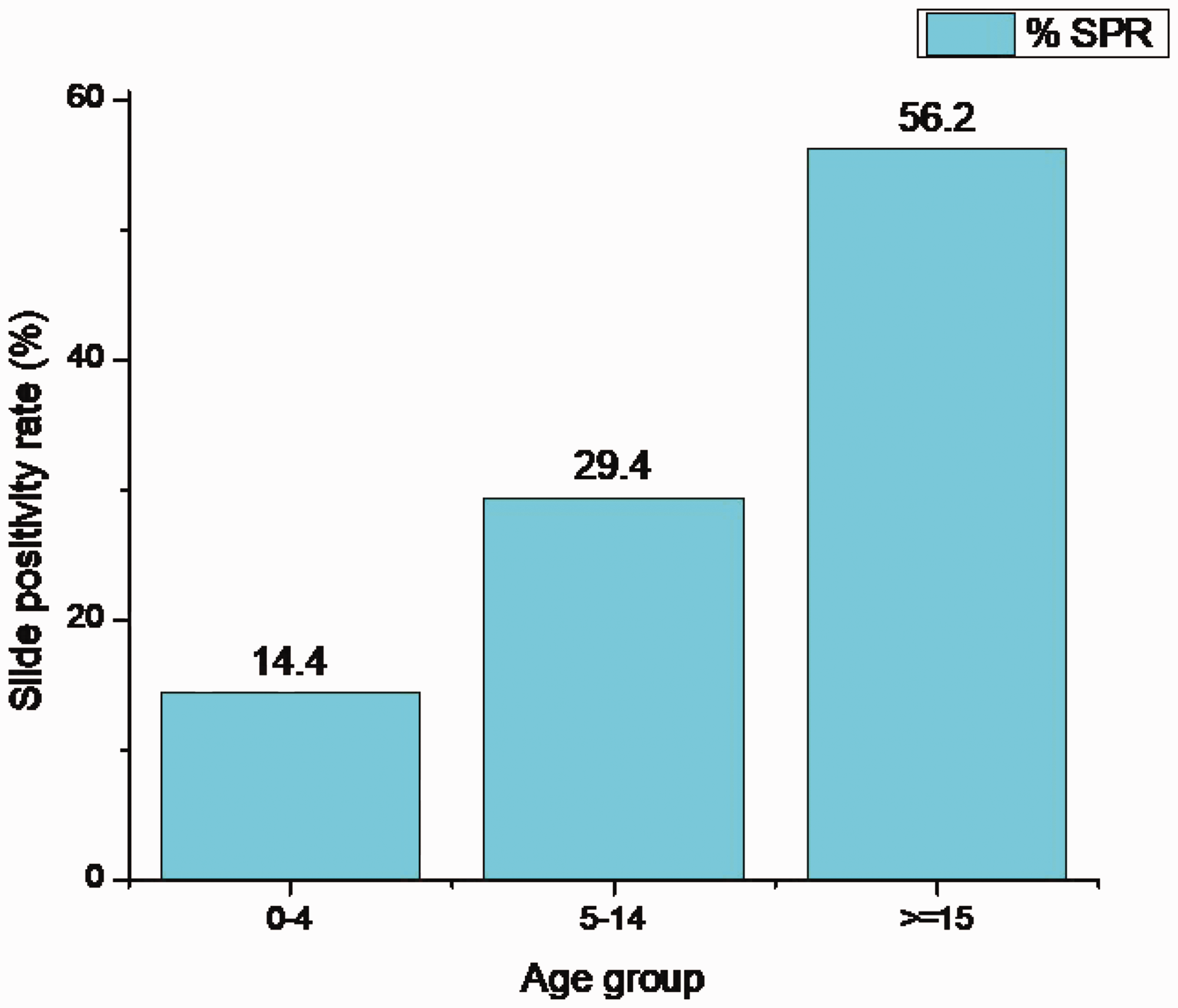
Distribution of malaria slide positivity rate (SPR) by age in Boset District, Central Ethiopia, 2016 to 2020.
As for the relative proportion of malaria parasite species among positive cases in Boset District, P. falciparum showed a slight predominance (58%) over P. vivax (42%) (p < 0.04), with an SPR of 7.2% and 5.2%, respectively. Both species showed a declining trend in the SPR during 2016–2020 (Figure 6).
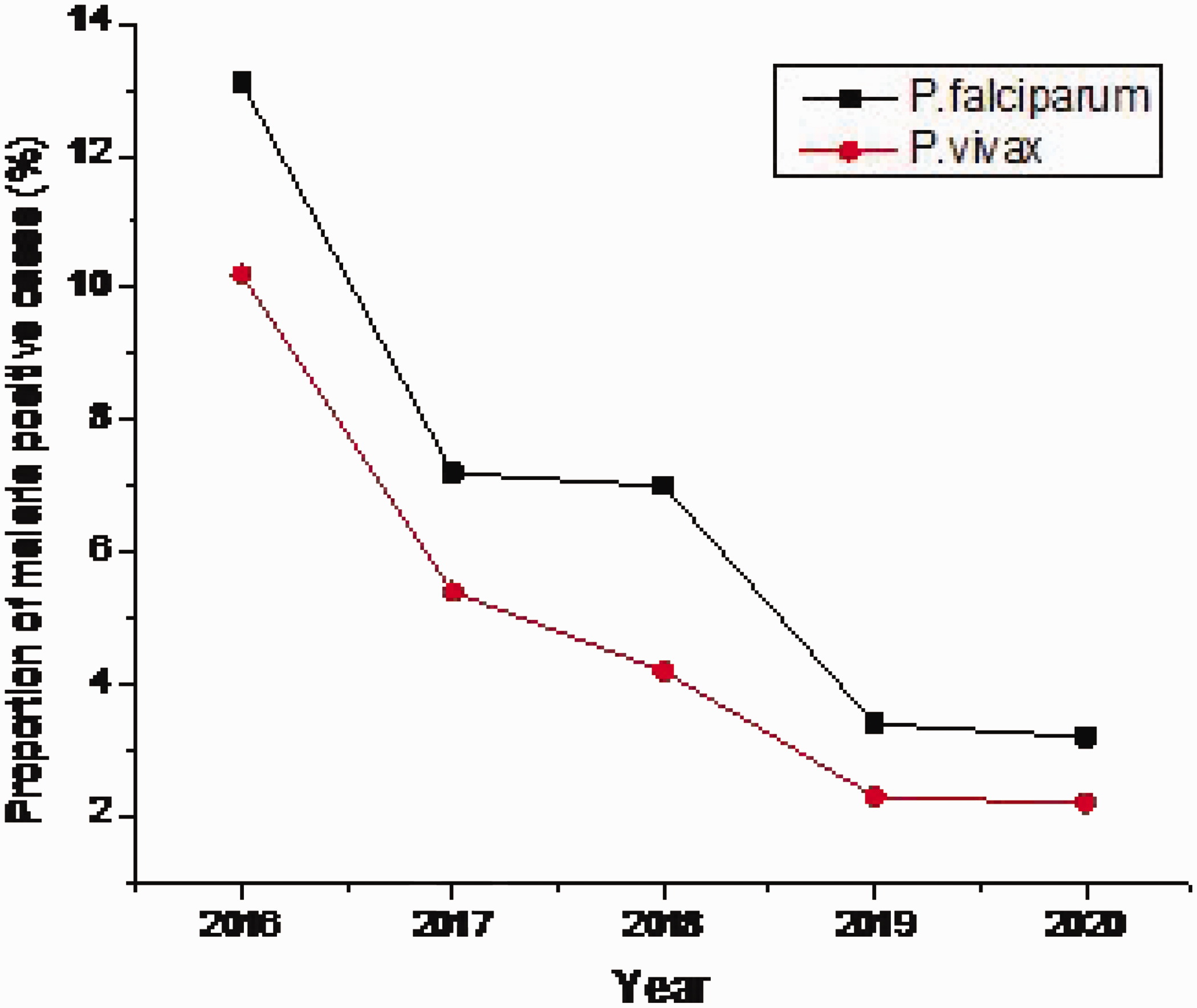
Five-year trend of malaria cases in Boset District, Central Ethiopia, 2016 to 2020.
Discussion
The current study revealed that the overall malaria SPR in Boset District was 12.4% (21,059/169,986), implying a relatively average malaria morbidity in this area. The positivity rate from public health facilities in the district was higher than the SPR in Olanchiti Hospital and in private health facilities (Table 1). This is perhaps owing to ease of accessibility of public health facilities for most treatment seekers. The present study showed a lower malaria SPR compared with previous studies in Hadiya Zone, Ethiopia among febrile cases with an overall SPR of 25.8%, 18 and in Batu Town with an SPR of 17.13%. 19 Despite the numerous studies conducted in Ethiopia at national and regional levels on expanding malaria interventions, malaria remains a leading communicable disease, causing considerable morbidity. There was a clear decline in the malaria incidence rate and malaria death rate in Ethiopia from 2001 to 2016; however, the malaria case number and incidence remained high, with 19.8 cases per 1000 people reported in 2016, exceeding the World Health Organization standard for pre-elimination.
Regarding the trend in malaria cases across the study period, a sharp decline from 23.3% to 5.3% during 2016 to 2020 was observed (Figure 2). Despite well-documented seasonal variation in the malaria prevalence and incidence in Ethiopia, 20–24 meteorological variables (mainly rainfall) are strongly associated with the incidence of both P. falciparum and P. vivax malaria, 25 according to data records used in the present study (Supplementary Figure 1).
Regarding the types of Plasmodium species associated with infection, P. falciparum showed a slight predominance (58%) over P. vivax (42%) among malaria-positive cases. This finding is in line with the previously reported Plasmodium composition in Ethiopia, where P. falciparum and P. vivax account for 60% and 40% of Plasmodium species in this country, respectively. 3 The present study findings are also in agreement with previous reports in Ethiopia in which P. falciparum and P. vivax account for 71.8% and 23.9% in Wolaita Zone and 75.2% and 24.5% in Benishangul-Gumuz Regional State, respectively.26,27 However, our findings are in contrast to reports that P. vivax is the predominant species in Jimma Town, Hadiya Zone, the highland fringes of Butajira, Adama Town, and Batu Town, Ethiopia, with proportions of 71.4%, 86.5%, 71.7%, 61%, and 50.5%, respectively.18,19,23,28,29 Despite differences in proportions, nearly all studies concur in reporting that P. vivax is co-endemic with P. falciparum in Ethiopia, one of the few African countries in which this situation exists. Despite earlier studies showing that P. falciparum and P. vivax account for 60% and 40% of all malaria cases, respectively, 3 recent studies report that these two species have equal case incidence rates, 30 although some studies report that P. vivax is the main causative agent of malaria in Oromia Regional State in Ethiopia.31,32
In the present retrospective data analysis, more malaria cases were recorded among male individuals than their female counterparts. This result is in line with previous local studies.33,34 This might be associated with the traditional work culture in Ethiopia where male individuals are more engaged in outdoor activities like agriculture than female Ethiopians. The age distributions showed that individuals aged 15 years and above accounted for a higher proportion of malaria cases. This finding is in agreement with previous studies elsewhere in the country;21,23,27,35 this age group also accounts for the most hospital admissions among all age groups.
There are several study limitations that should be noted. Data for mixed infections were excluded because of incomplete and inconsistent reports between public and private health facilities. Inclusion of these data could have enriched the study results. In addition, limitations associated with the recording and handling of data might affect the reliability of the findings.
Conclusion
In the present study, we found a malaria SPR of 12.4% among public and private health facilities in Boset District from 2016 to 2020, with a sharp decline from 23.3% in 2016 to 5.3% in 2020. Regarding the distribution of Plasmodium species among malaria-positive cases, P. falciparum (58%) was more prevalent than P. vivax (42%). The declining trend in malaria cases over the 5-year study period may reflect the results of expanded malaria interventions at national and regional levels in Ethiopia. To maintain this reduction in malaria cases across the area and for eventual elimination of the disease, scaling up the available malaria prevention strategies and control measures is necessary.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221121957 - Supplemental material for Assessment of malaria prevalence in Boset District, East Shawa Zone, Oromia Regional State, Ethiopia: a retrospective study
Supplemental material, sj-pdf-1-imr-10.1177_03000605221121957 for Assessment of malaria prevalence in Boset District, East Shawa Zone, Oromia Regional State, Ethiopia: a retrospective study by Bayissa Chala and Tigist Tilaye in Journal of International Medical Research
Footnotes
Acknowledgments
We are grateful to the East Shawa Zone Health Office for providing us the data needed for this study and to Mr. Hassen Shube for his kindness in developing the map of the study area.
Author contributions
BC designed the study, collected and analyzed the data, and wrote the paper. TT designed the study, collected the data, and reviewed the paper. Both authors read and approved the manuscript.
Data availability statement
The authors confirm that all data underlying the findings are fully available without restriction.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was fully funded by the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.