
Abstract
Background:
The community-based health insurance (CBHI) program was established in Ethiopia to enhance access to healthcare and protect vulnerable populations, including women, from financial risk.
Aim:
This study analyzed healthcare utilization and its determinants between community-based health insurance members and nonmembers of women in Sidama’s Central Zone, southern Ethiopia.
Methods:
From January 19 to February 20, 2024, a community-based comparative cross-sectional study was conducted among 1280 women (640 insured and 640 uninsured). The study participants were selected using a multistage sampling technique, and data were collected through structured face-to-face interviews using the KoBo Toolbox.
Findings:
The analysis revealed that CBHI membership was associated with a 77% higher frequency of health facility visits than non-members (APR = 1.77, 95% CI: 1.52-2.06; P < .001). For insured women, some individual and community-level factors were associated with the frequency of health facility visits. Age was positively associated with health facility visits, with each additional year leading to a 1.0% increase (APR = 1.01, 95% CI: 1.01-1.02; P < .001). Healthcare satisfaction also played a role, with a one-unit increase associated with a 4.0% increase in the frequency of healthcare visits (APR = 1.04, 95% CI: 1.03-1.05; P < .001). Geographical accessibility was a barrier, as women living farther from facilities experienced a 41.0% reduction in health facility visits (APR = 0.59, 95% CI: 0.48-0.73; P < .001). Community literacy and poverty levels were also significant determinants, with women from high-literacy communities having more than twice the visits (APR = 2.11, 95% CI: 1.60-2.80; P < .001) and those from low-poverty areas having higher visit rates (APR = 1.58, 95% CI: 1.24-2.01; P < .001). Family size was a determinant among uninsured women, with each additional household member associated with a 9.6% increase in health facility visits (APR = 1.10, 95% CI: 1.02-1.18; P = .015). Healthcare satisfaction had a positive association with the frequency of health facility visits (APR = 1.05, 95% CI: 1.04-1.05; P < .001). Geographical accessibility remained a barrier, with a 42% reduction in visits for those living farther from facilities (APR = 0.58, 95% CI: 0.44-0.77; P < .001). Community literacy was also a significant factor, with women from high-literacy areas having more than twice the frequency of health facility visits (APR = 2.12, 95% CI: 1.60-2.81; P < .001).
Conclusions:
This analysis demonstrated that membership in CBHI substantially increased the frequency of health facility visits, resulting in a 77% rise relative to non-members. Among insured women, significant determinants included age, healthcare satisfaction, geographical accessibility, community literacy, and poverty levels. Conversely, for uninsured women, associated factors comprised family size, healthcare satisfaction, geographical accessibility, and community literacy, highlighting the necessity of addressing systemic barriers and community-level influences to enhance healthcare access and utilization in the region.
Keywords
Introduction
Healthcare access is a fundamental human right, essential for well-being, and is codified in international laws such as the Universal Declaration of Human Rights and the International Covenant on Economic, Social, and Cultural Rights. 1 This right encompasses availability, accessibility, acceptability, and quality, all critical for achieving universal health coverage. High-quality healthcare necessitates adherence to safety, effectiveness, patient-centeredness, timeliness, equity, integration, and efficient provision. 2
Indeed, several factors influence healthcare service utilization, including socio-demographic factors such as residence, gender, education, marital status, occupation, and family size. 3 Economic factors, such as household income, also play a significant role, and access-related factors like proximity to health institutions, transportation, and ambulance services are crucial predictors of healthcare utilization. 4
Healthcare need-related factors, such as chronic illnesses and attitudes toward community-based health insurance (CBHI) schemes, also affect healthcare utilization. 5 Financial constraints in low-income countries often result in out-of-pocket payments, underscoring the need for sustainable financing mechanisms. For example, high costs for consultations, diagnostics, and drugs can deter timely healthcare, leading to delays in diagnosis and treatment. 6
To this end, the Sustainable Development Goals (SDGs), particularly Goal 3, emphasize healthy lives and well-being for all, with a target of achieving universal health coverage by 2030. 7 Accordingly, many developing countries strive to expand universal health coverage using existing health systems, which encounter structural challenges.
Ethiopia’s health system is structured into a three-tier framework: primary, secondary, and tertiary. The primary level includes health posts, health centers, and primary hospitals, which are integral to community-based healthcare. Health posts, the first point of contact at the kebele level, serve 3000 to 5000 people and are staffed by two female Health Extension Workers (HEWs) per health post. 8
HEWs deliver essential health packages, focusing on family health, hygiene, sanitation, disease prevention, and health education. Health centers support health posts by providing more comprehensive services to 15 000 to 25 000 people. Primary hospitals offer inpatient and ambulatory services to a population of 60 000 to 100 000. 9
The Health Extension Program (HEP), launched in 2003, has enhanced access to preventive and promotive services by training and deploying over 30 000 HEWs. 8 The Federal Ministry of Health (FMOH) oversees the health system, collaborating with regional states to develop policies and strategies aligned with international initiatives to achieve universal health coverage. 10
Ethiopia operates community-based health insurance (CBHI) schemes targeting the informal sector to protect households from catastrophic health expenditures and enhance healthcare utilization. CBHI is a government-run program that involves community participation in its design, management, and supervision. The benefit package includes outpatient and inpatient services at public facilities, funded by member premiums and a 25% government subsidy.11,12
CBHI membership is voluntary, targeting rural communities and the informal sector, and offers services in public facilities but excludes treatments abroad or cosmetic procedures. The scheme aims to reduce financial barriers, increase service utilization, and improve the quality of care through community involvement. 12
Ethiopia plans to implement a Social Health Insurance (SHI) program for formal sector employees, aiming to improve healthcare access through contracted facilities. Premium costs will be shared between employees and employers. However, despite thorough planning and legislative groundwork, the program’s realization is hindered by public sector employee resistance and concerns about coverage limitations. Empirical evidence suggests that CBHI membership enhances healthcare service utilization, with studies in Ethiopia demonstrating increased utilization among insured households. 11
In Ethiopia, further research has identified the influence of socio-demographic and economic factors on CBHI enrollment and healthcare utilization, emphasizing the need to address the scheme to better serve the health needs of women in regions like Sidama, who face unique barriers such as limited decision-making power and cultural norms.13,14
Despite all this, a significant knowledge gap exists in healthcare utilization among CBHI members and nonmembers in southern Ethiopia. This gap is pronounced in methodologies, with most studies relying on conventional regression models that fail to capture variations across different hierarchical levels.11,12,15 This limitation hinders our understanding of how factors at various levels interact to influence healthcare utilization between CBHI members and nonmembers. Furthermore, in the southern part of Ethiopia, studies that compare healthcare utilization between insured & uninsured women were nonexistent. 16
In addition, research on health service utilization in southern Ethiopia has largely overlooked the patterns of health facility visits among community members, with notable exceptions. Most existing studies employ binary metrics, assessing only whether individuals access healthcare services or not. 17
While these measures provide basic insights, they neglect the complexities of healthcare engagement, particularly for women. A drawback of binary metrics is their failure to capture the frequency of health facility visits, which is essential for understanding individual healthcare behaviors. Analyzing visit frequency yields a better understanding of health service utilization patterns than simplistic yes/no classifications.18,19
There is also a critical knowledge gap concerning the perspectives of women within households. Existing studies primarily focus on the household level, marginalizing women’s experiences and views related to gender dynamics. 20 This oversight results in a lack of information about how gender-specific factors affect healthcare utilization patterns between women of CBHI members and nonmembers. These gaps underscore the need for future research incorporating analytical methodologies and perspectives, especially those related to gender differences and their impact on healthcare access and utilization behaviors.
Further, policymakers and program managers can use the findings to design interventions that address the unique needs and barriers faced by women in accessing healthcare services, thereby contributing to the overall well-being of the population in the Sidama region, Ethiopia. Therefore, this study aimed to compare healthcare utilization and determinants between insured and uninsured women in the Sidama region, Ethiopia.
Methods
Study Area
The study was conducted in the Central Zone of the Sidama region in Ethiopia. This zone comprises six districts and one town administration, with an overall population of 956 967 as reported in 2016 EFY. 21 The specific sites for this study, namely Dale Woreda and Yirgalem City Administration, are geographically positioned approximately 45 km south of Hawassa, the regional capital, and 320 km from Addis Ababa, the capital of Ethiopia. 22
The selection of these areas was determined by their historical and strategic importance within the context of Ethiopia’s community-based health insurance (CBHI) program. Yirgalem City was among the first 13 sites to pilot the community-based health intervention (CBHI) program in 2011. 23 Moreover, Yirgalem Hospital, alongside Arba Minch Hospital, is recognized for its pioneering role in initiating innovative healthcare financing programs and for being among the earliest modern health institutions established in the region. 24
Focusing on women within these particular areas, the study sought to identify the determinants associated with healthcare utilization among female CBHI members and nonmembers, thereby contributing valuable perspectives and insights for future program development and refinement.
Study Design and Period
The study adopted a community-based, comparative cross-sectional design, with data collection held from January 19th to February 20th, 2024. This approach allowed for the simultaneous assessment of exposure and outcome variables at a specific point, providing a snapshot of 25 healthcare utilization patterns and associated factors between insured and uninsured women.
The cross-sectional design facilitated comparisons between these two groups within a study setting. Adherence to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist ensured comprehensive and transparent reporting, 26 with the checklist included as Supplementary File 1.
Source and Study Population
The study population consisted of women aged 18 years and older residing in Dale Woreda and Yirgalem City Administration in the Sidama region of Ethiopia, including both insured and uninsured in the CBHI program.
The exposed group comprised women aged 18 and older enrolled in CBHI, who were recruited from kebeles within Dale Woreda and Yirgalem City Administration of the central Sidama zone. Whereas, the unexposed group included women aged 18 and older who were not enrolled in CBHI, selected from different households within the same kebeles of Dale Woreda and Yirgalem City Administration.
Inclusion and Exclusion Criteria
The eligibility criteria for study participants encompassed women aged 18 years and older, irrespective of their membership status within the CBHI program. In households with polygamous marriages or where the mother was deceased and the father resided with a daughter aged 18+, the interview respondent was decided by the husband (household head). Households that have begun contributing premiums to CBHI but are not yet able to utilize health services were also considered non-members.
Sample Size Determination
The sample size was determined using OpenEpi, Version 3.1, based on a study conducted on community-based health insurance service utilization and associated factors in Addis Ababa, Ethiopia. 27 The sample size was calculated using a double population proportion, assuming a 95% confidence interval, 80% power, and a 1:1 ratio of controls to cases.
The percentage of controls exposed was 67.35%, and the percentage of cases with exposure was 55.58%; a design effect of 2 and an anticipated non-response rate of 10% were considered. Based on these assumptions, the required sample size for this study was 1280 participants (women), consisting of 640 CBHI members and 640 non-members.
Sampling Procedure
A multi-stage sampling technique was used to obtain the desired sample size. A total of 14 kebeles were randomly selected from Dale Woreda (one urban and eight rural kebeles) and Yirgalem City Administration (two urban and three rural kebeles).
The lists of uninsured households in each kebele were either obtained from the respective kebele or recorded separately as non-members of the community-based health insurance (CBHI) program in cases where a list was unavailable. At the time of data collection, there were 16 118 households (8646 uninsured households and 7472 insured households) across the 14 kebeles.
In the second stage, 640 CBHI members were proportionally allocated to each of the 14 kebeles based on the population sizes of insured households. Each kebele maintained its own CBHI registry, which contained lists of all CBHI members. In the third stage, insured households were randomly selected from the CBHI registry of each kebele. Similarly, 640 uninsured households were allocated to each kebele based on the population size of uninsured households. Study participants were then randomly selected from the list in each kebele until the required number was achieved.
Data collectors contacted the selected women for the final interview. If a woman was absent during data collection, up to three visits were made before excluding her to maintain a high response rate. When no eligible woman lived in the selected household, women from the next household were included. If an eligible woman was present, the interview proceeded as planned. In households with multiple eligible women, one was randomly selected. Each woman was assigned a unique number. These numbers were placed in a container, and the husband drew one number to select the participant. This method ensured an unbiased and fair selection.
Study Variables
The outcome variable was the frequency of health facility visits between insured and uninsured women. Health services utilization was measured as the number of outpatient and inpatient healthcare visits made in the previous 12 months to a health facility. This was reported by the women at the time of the interview. Outpatient visits include trips to a health post, health center, clinics, or hospital for health care, while inpatient visits refer to overnight health center or hospital for healthcare and medical treatment. 28
The independent individuals and community-level variables were age, marital status, family size, religion, area of residence, household head, level of education, membership status, wealth index, distance to healthcare facility, decision-making at household, waiting times at healthcare facility, satisfaction level, community-level women’s autonomy, literacy, and poverty. The details of the study variables’ measurement are provided in Supplementary File 2.
Data Source
The data sources for this study were women aged 18+ years, households of CBHI members, and non-members from the study areas.
Data Collection Tool and Procedure
The data collection tool was adapted from previous studies conducted elsewhere15,29 -39 and the questionnaire was provided as Supplementary File 3. In addition, before the data collection, the study team conducted a pilot test. From the pilot test, we identified and rectified some coding errors, labeling errors, and enhanced certain questions and responses.
Twenty-eight data collectors, who held bachelor’s degrees, were trained and conducted face-to-face interviews using the KoBo Toolbox mobile application. 40 Furthermore, the data collection process was supervised by five supervisors, who had master’s degrees in public health. The collected data were then exported to Stata version 17 for analysis. 41
To ensure data integrity, the study team, encompassing the principal investigator, supervisors, and data collectors, instituted a multi-faceted quality control protocol. This protocol comprised training and pre-testing of data collectors, the implementation of re-interviews, and the execution of daily data audits to identify and rectify errors, including inconsistencies in labeling, instances of incomplete responses, and formatting irregularities within the questionnaire. The adoption of these measures served to maintain and enhance the overall quality of the study. 42
Statistical Methods
Before proceeding with data analysis, variable recoding and categorizations were conducted. For the details, see Supplementary File 4. Consequently, categorical variables were summarized using absolute frequencies and percentages, while continuous variables were characterized by means and standard deviations (SD). 43
The wealth index was derived through principal component analysis (PCA), which served as a composite indicator of living standards, based on 42 items related to the ownership of selected household assets, including house ownership, construction materials, number of rooms, agricultural land area, presence of livestock, types of cooking fuel, and access to improved sanitation and water facilities. 44
To determine the associations between independent variables and the outcome of interest, a multilevel negative binomial model was utilized to estimate adjusted prevalence ratios with 95% confidence intervals (CIs)with significance set at P < .005. This model was preferred over multilevel Poisson regression due to observed overdispersion in the data, where variance exceeded the mean. 45 Subsequently, the necessity for a multilevel analysis was assessed using a random intercept model of the multilevel negative binomial model, which also allowed for the computation of the intraclass correlation coefficient (ICC) to affirm the necessity for a multilevel approach. 46
Given that the ICC exceeded 5%, the implementation of a multilevel analysis model became essential. 47 In light of the hierarchical nature of the data and to mitigate the potential underestimation of standard errors associated with ordinary models, a multilevel model was subsequently recommended based on preliminary analyses. 48
In the multivariate analysis, variables with P-values <.25 from the bivariate analysis were included alongside those supported by existing literature, thus accounting for potential confounding factors. 49 Furthermore, effect modification was assessed by systematically introducing interaction terms. Multicollinearity among independent variables was checked using multiple linear regression, with a variance inflation factor threshold set at <5. 50 In addition to this, to address the influence of a few outlying data points, we employed multilevel robust negative binomial regression models in this study. 51
Finally, the fitness of the model was evaluated through the assessment of four distinct models: Model 0 (empty model), Model 1 (incorporating only individual-level variables), Model 2 (incorporating only community-level variables), and Model 3 (including both individual- and community-level variables). The summary of these fitted models is detailed below (Tables 8 and 9).
Results
The study compared the socio-demographic characteristics of 1280 women from the Central Sidama Zone in Southern Ethiopia, with equal representation of insured (n = 640) and uninsured (n = 640) participants. All sampled women completed interviews, and several individual and community-level variables showed significant differences between the two groups.
Notably, ethnic affiliation varied between insured and uninsured women. Among uninsured women, 624 (51.11%) identified as Sidama, whereas 597 (48.89%) of insured women belonged to this ethnic group (P < .001). Consequently, the residential area also showed marked differences, with 222 (43.96%) of uninsured women living in urban areas compared to 283 (56.04%) of insured women (P < .001), suggesting that urban residence was significantly associated with being uninsured (Table 1).
Selected Socio-Demographic and Health-Related Characteristics of Insured and Uninsured Women in the Central Sidama Zone, Southern Ethiopia, 2024 (n = 1280).
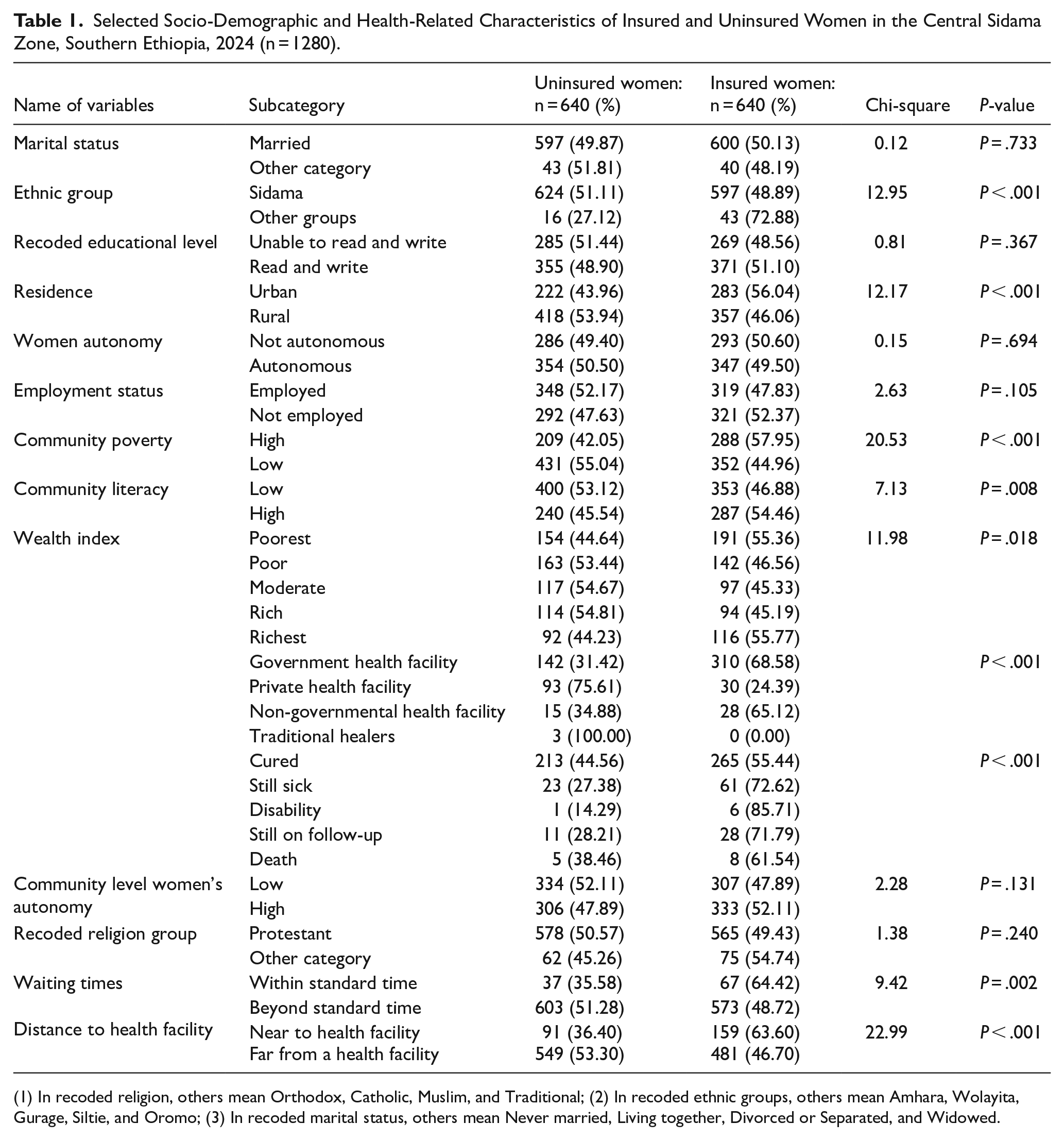
(1) In recoded religion, others mean Orthodox, Catholic, Muslim, and Traditional; (2) In recoded ethnic groups, others mean Amhara, Wolayita, Gurage, Siltie, and Oromo; (3) In recoded marital status, others mean Never married, Living together, Divorced or Separated, and Widowed.
Furthermore, community poverty levels demonstrated a strong association with community-based health insurance status. A substantial 209 (42.05%) of uninsured women lived in communities with high-poverty areas, whereas 288 (57.95%) of insured women came from low-poverty backgrounds (P < .001) (Table 1).
In addition, community literacy levels revealed significant differences, with uninsured women predominantly coming from communities with low literacy areas, comprising 400 (53.12%), while insured women were more likely to originate from high literacy areas, accounting for 287 (54.46%) (P = .008). This indicated that community-level literacy was associated with women’s access to community-based health insurance (Table 1).
Ultimately, the wealth index illustrated patterns associated with community-based health insurance coverage. Among uninsured women, 154 (44.64%) were categorized as the poorest wealth index, while 191 (55.36%) of insured women fell into the richest wealth index categories (P = .018). For detailed information, see Table 1.
An analysis of selected background characteristics among insured and uninsured women in the Central Zone of Sidama region, Ethiopia, was conducted, encompassing a sample of 1280 women (640 insured & 640 uninsured).
Notably, the uninsured women reported a mean age of 32.97 years (±9.14), while insured women reported a higher mean age of 36.42 years (±10.47). The mean age difference was approximately 3.45 years, with a statistically significant association (t = −6.27; P < .001) (Table 2).
Some Demographic and Health-Related Variables of Insured and Uninsured Women in the Central Sidama Zone, Southern Ethiopia, 2024 (n = 1280).

Concerning family size, uninsured women reported a mean family size of 4.68 (±1.43), whereas insured women reported a mean family size of 5.07 (±1.43). The difference in family size was approximately 0.38, and this difference was statistically significant (t = −4.80; P < .001) (Table 2).
Regarding healthcare satisfaction, uninsured women reported a mean score of 12.13 (±17.30), while insured women reported a higher mean score of 17.88 (±18.95). The difference in healthcare satisfaction scores was approximately 5.75, with a statistically significant association (t = −5.67; P < .001) (Table 2).
Analysis of Frequency of Health Facility Visits Between Insured and Uninsured Women in the Central Zone of the Sidama Region, Ethiopia, 2024 (n = 1280)
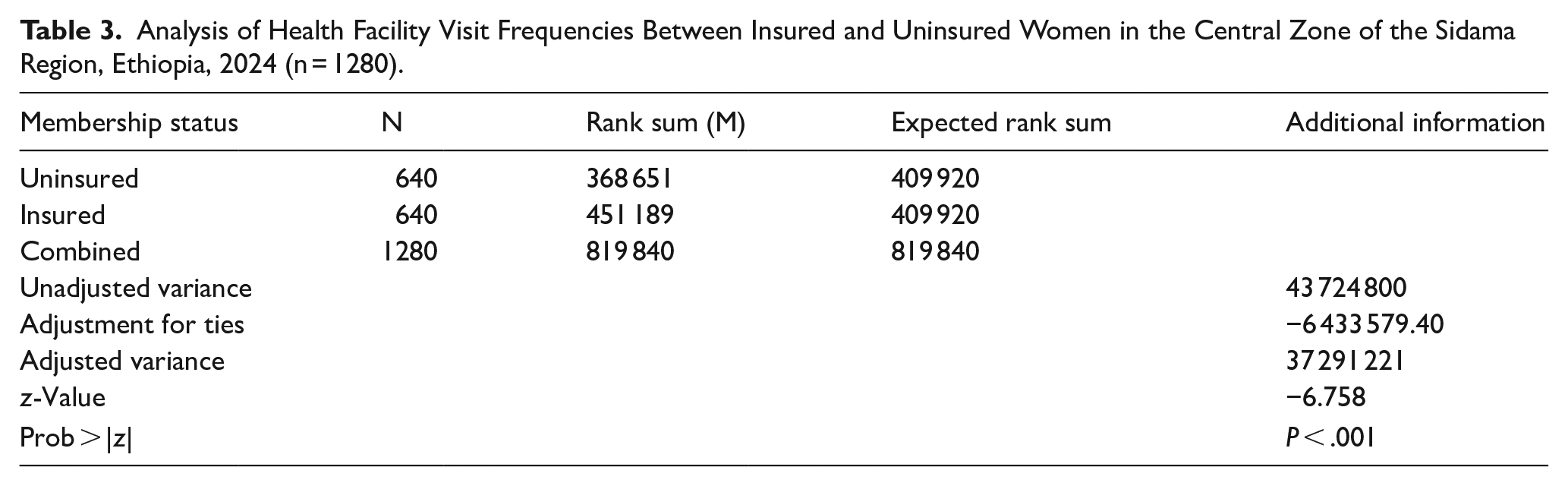
A comparative analysis was conducted to examine health facility visit frequencies among insured and uninsured women in the Central Zone of Sidama, Ethiopia. Using a sample of 1280 participants (640 insured and 640 uninsured), the study employed a two-sample Wilcoxon rank-sum test due to non-normal data distribution. 52
The results showed a significant difference in rank sums between these two groups, with a z-statistic of −6.758 and a P-value of <.001 (Table 3). This led to the rejection of the null hypothesis, indicating a statistically significant disparity in health facility visit frequencies between insured and uninsured women. The findings suggested that insured women had shown more frequent visits compared to uninsured women.
Analysis of Health Facility Visit Frequencies Between Insured and Uninsured Women in the Central Zone of the Sidama Region, Ethiopia, 2024 (n = 1280).
Null Hypothesis
Null hypothesis (Ho): There was no significant difference in the frequency of health facility visits between insured and uninsured women.
Alternative hypothesis (Ha): There was a significant difference in the frequency of health facility visits between insured and uninsured women.
Random Model Information
For women who were uninsured under the community-based health insurance (CBHI) scheme, the intraclass correlation coefficient (ICC) at the kebele level was estimated to be .26 (95% CI: 0.09, 0.46) (Table 4). This indicated that approximately 26% of the total variance in the frequency of health facility visits could be attributed to the clustering effect at the kebele level. In contrast, for women insured under CBHI, the ICC at the kebele level was significantly lower, at .15 (95% CI: 0.06, 0.30) (Table 4).
The Intraclass Correlation Coefficient Between Insured and Uninsured Women in the Central Zone of Sidama Region, Southern Ethiopia, 2024 (n = 1280).
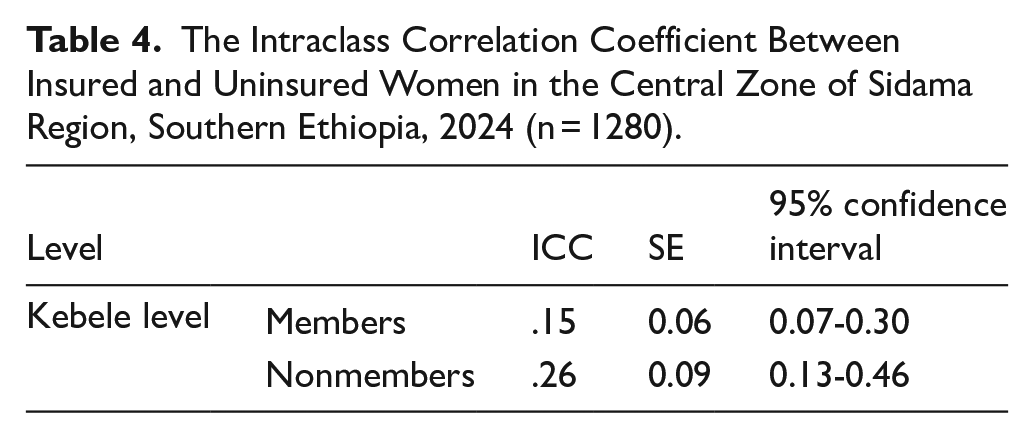
This suggested that about 15% of the total variance in health facility visits was due to the clustering effect at the kebele level. The substantial difference in ICC values between the two groups implies that CBHI membership is associated with a reduction in the unexplained variance in health facility visit frequencies at the kebele level.
The relatively narrow confidence intervals, coupled with the standard errors, demonstrate a reasonably precise estimation of the ICC, thereby supporting the rationale for employing a multilevel analysis. 53
A multilevel negative binomial regression analysis was performed on a sample of 640 insured women participating in community-based health insurance (CBHI) in the central zone of the Sidama region in 2024. The results revealed several significant individual and community-level determinants of health facility visit frequency.
Accordingly, age was found to be a statistically significant determinant, with each additional year associated with a 1.0% increase in the frequency of health facility visits (APR = 1.01, 95% CI: 1.01-1.02; P < .001). Healthcare satisfaction also emerged as an important factor, with each unit increase in healthcare satisfaction linked to a 4.0% rise in health facility visits (APR = 1.04, 95% CI: 1.03-1.04; P < .001) (Table 5).
Determinants of Healthcare Utilization Among Insured Women in the Central Sidama Zone, Southern Ethiopia, 2024 (n = 640).

Conversely, geographical accessibility presented a substantial barrier to accessing care, as women residing far from health facilities exhibited a 41% reduction in the frequency of health facility visits compared to those women who were living closer to such facilities (APR = 0.59, 95% CI: 0.48-0.73; P < .001) (Table 5).
Finally, women from communities with high literacy rates demonstrated significantly higher health facility visit compared to those from communities with low literacy areas (APR = 2.11, 95% CI: 1.60-2.80; P < .001) and women from communities with low poverty areas were associated with significantly higher health facility visit as compared to women from communities with high poverty areas (APR = 1.60, 95% CI: 1.24-2.01; P < .001) (Table 5).
In the examination of 640 uninsured women within the same study context in 2024, a distinct set of factors associated with healthcare utilization patterns was observed. Family size emerged as a critical determinant, with each additional household member significantly associated with a 10 % increase in health facility visits (APR = 1.10, 95% CI: 1.02-1.18; P = .015) (Table 6).
Determinants of Healthcare Utilization Among Uninsured Women in the Central Sidama Zone, Southern Ethiopia, 2024 (n = 640).

Among insured women, healthcare satisfaction demonstrated a positive association with health facility visits (APR = 1.05, 95% CI: 1.04-1.05; P < .001). However, geographical accessibility showed approximately a 42% reduction in health facility visits among women residing farther from health facilities (APR = 0.58, 95% CI: 0.44-0.77; P < .001). On the other hand, women from communities with high literacy areas exhibited significantly higher health facility visits compared to those from communities with low literacy areas (APR = 2.12, 95% CI: 1.60-2.81; P < .001) (Table 6).
Comparison of Significantly Associated Factors with Healthcare Utilization Between Insured and Uninsured Women
A comparative assessment of the determinants of frequency of health facility visits between insured and uninsured women in the Sidama region in 2024 (n = 1280) identified both shared and distinct patterns.
The comparison results depicted that age was a significant determinant of health facility visits solely for insured women, with each additional year associated with a modest increase (APR = 1.01, 95% CI: 1.01-1.02; P < .001). In contrast, family size was significantly associated with health facility visits only for uninsured women (APR = 1.10, 95% CI: 1.02-1.18; P = .015) (Table 7).
Comparison of Significantly Associated Factors with Healthcare Utilization Between Insured and Uninsured Women in the Central Zone of Sidama Region, Ethiopia, 2024 (n = 1280).
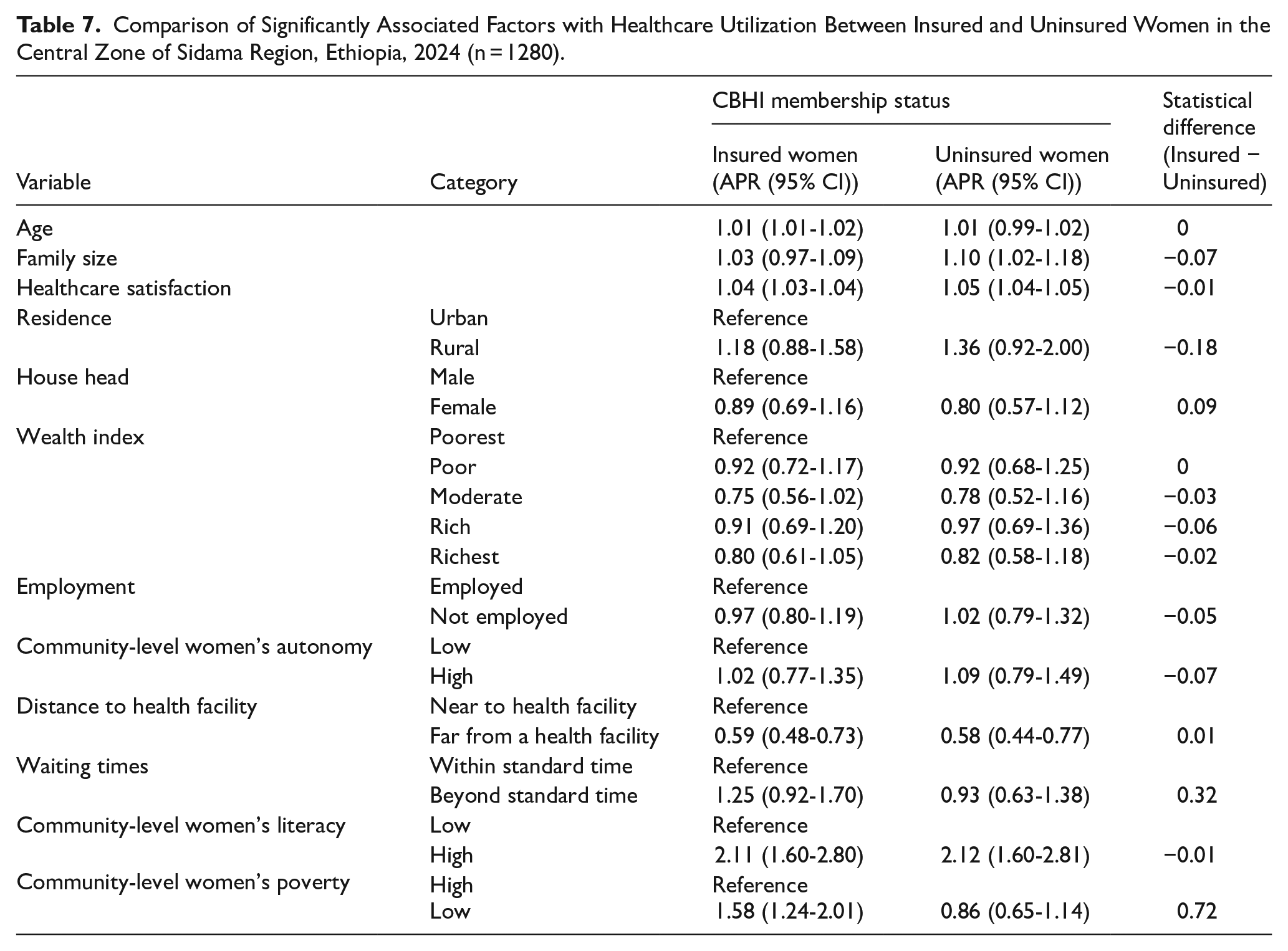
Community-level poverty exhibited differential effects across both groups: insured women in low-poverty areas had a significantly higher health facility visits, almost 60% higher (APR = 1.58, 95% CI: 1.24-2.01; P < .001), whereas this relationship was not significant for uninsured women (APR = 0.86, 95% CI: 0.65-1.14; P = .285) (Table 7).
Both insured and uninsured women showed similar results concerning healthcare satisfaction, where those with higher satisfaction had higher health facility visits (insured APR = 1.04 vs. uninsured APR = 1.05; both P < .001), and distance to health facilities, where those living farther from facilities were less likely to have health facility visits (insured APR = 0.59 vs. uninsured APR = 0.58; both P < .001) (Table 7).
High community-level literacy revealed a strong association for both groups, with more than double the health facility visits compared to communities with low literacy areas (insured APR = 2.11 vs. uninsured APR = 2.12; both P < .001) (Table 7).
Model Fitness Selection Procedure
Notably, four models were fitted and evaluated using log-likelihood, AIC, and BIC for comparison. a null model, a model with individual factors, a model with community factors, and a model containing both individual and community-level factors. These criteria were used to select the best-fit model. 54
Four statistical models were fitted and assessed using the Log-Likelihood (LL), Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC) to facilitate comparative analysis. The models included a null model (Model 0), a model incorporating individual-level factors (Model 1), a model incorporating community-level factors (Model 2), and a model integrating both individual and community-level factors (Model 8).
The assessment relied on LL, AIC, and BIC metrics to gauge model adequacy while accounting for penalization to mitigate overfitting. Among the models, Model 0 exhibited the highest LL value (−409.3513), indicating optimal data fit. Nevertheless, LL alone did not consider the complexity of the models. AIC and BIC offered additional insight by balancing model fit against complexity, with lower values signaling better fit (Table 8).
Model Comparison and Selection Criteria Among Insured Women in the Central Sidama Zone, Southern Ethiopia, 2024 (n = 640).

Abbreviations: AIC, Akaki information criteria; BIC, Bayesian information criteria; LL, loglikelihood.
Model 3, encompassing both individual and community-level variables, emerged as the preferred model due to its superior AIC (1615.776) and BIC (1696.082) scores, both being the lowest among all evaluated models. This highlighted its effectiveness in achieving a balance between parsimony and explanatory power. Conversely, while Model 0 achieved the highest LL value, its lack of inclusion of relevant variables rendered it overly simplistic, as reflected by its relatively increased AIC and BIC scores (Table 8).
Therefore, Model 3 was identified as the most appropriate model for analyzing CBHI-insured women in the Central Zone of Sidama region, southern Ethiopia, due to its integration of individual and community-level factors, alongside its robust model fit and complexity.
Table 9 provides a comparative analysis of various models employed to investigate factors associated with uninsured women in the central Sidama zone, southern Ethiopia. This evaluation was grounded in three primary criteria: log-likelihood (LL), Akaike information criterion (AIC), and Bayesian information criterion (BIC). These metrics enabled investigators to assess the fit and complexity of each model, facilitating informed decisions regarding model selection.
Model Comparison and Selection Criteria Among Insured and Uninsured Women in the Central Sidama Zone, Southern Ethiopia, 2024 (n = 640).

The log-likelihood (LL) serves as a measure of how well a model fits the data, with higher values indicating a superior fit. However, it does not account for model complexity. In contrast, the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) balance model fit with complexity, with lower values signifying a better balance. The BIC penalizes complexity more severely than the AIC, making it a more stringent criterion for model selection. 55
The results from the table reveal that the Null model (Model 0) possessed the highest log-likelihood value (−383.6563), suggesting it fits the data better than other models when considering fit alone. However, when balancing fit with complexity, Model 3, which incorporated both individual and community variables, was distinguished by its lowest AIC value (1111.813) (Table 9).
This indicated that Model 3 provides a favorable balance between explaining the data and avoiding overfitting by incorporating fewer unnecessary parameters compared to other complex models. Conversely, the BIC favors the Null model (Model 0) with the lowest value (780.2355), suggesting its preference if simplicity and avoiding overfitting are prioritized (Table 9).
The selection of the best-fit model is logically based on the study objectives. As the aim was to maximize explanatory power while maintaining a reasonable level of complexity, Model 3 was deemed the most appropriate choice due to its favorable AIC. This model offers an understanding of the factors influencing the outcome by including both individual and community variables.
Discussion
This study compared the association between community-based health insurance (CBHI) and health facility visits among 1280 women in the Sidama region, Ethiopia. The analysis revealed a significant association between CBHI membership and increased health facility visits, where insured women had 77% higher frequency of health facility visits compared to uninsured women (APR = 1.77, 95% CI: 1.52-2.06; P < .001).
This finding was consistent with previous studies in Ethiopia, which reported healthcare utilization rates of 50.5% among CBHI members versus 29.3% for non-members in the South Gondar zone. 56 Additionally, a study in northwest Ethiopia showed a healthcare utilization rate of 1.3 visits per individual per year of health service among CBHI members compared to nonmembers. 57
Globally, similar trends were observed; in Burkina Faso, insured individuals exhibited a 40% higher healthcare utilization rate, although this did not result in a significant increase in inpatient care. 31 In Senegal, insured individuals accessed healthcare more frequently than their uninsured counterparts. 58 In Bangladesh, the utilization was 50.7% for insurance enrollees compared to 39.4% for non-members. 59
Evidence from India further stresses disparities in healthcare visits by insurance status, highlighting the vital role of health insurance in increased health services utilization patterns. 60 In Rwanda, nearly universal health coverage resulted in insured households utilizing healthcare services at twice the rate of uninsured households. 61 Additionally, a study in Kenya indicated higher hospitalization rates among insured individuals. 62
This substantial effect size extends beyond simple association, emphasizing how CBHI is likely linked with the financial barriers that commonly deter individuals, especially women, from seeking timely healthcare services in low-income settings. 63 Financial inaccessibility has long been recognized as a major impediment to healthcare use, often causing delays in healthcare or outright avoidance, which worsens health outcomes and increases long-term costs. CBHI’s capacity to prepay healthcare costs and pool risks mitigates this problem, enabling insured women to use health services more frequently and proactively. 12
Nevertheless, it is essential to critically examine whether increased health facility visits necessarily translate into improved health outcomes. Ethiopia’s healthcare system, particularly in rural areas like Sidama, continues to face supply-side challenges including shortages of skilled health personnel, frequent stock-outs of essential medicines, inadequate infrastructure, and poor service quality. 64
If the rising demand associated with CBHI membership is not met with better service readiness and quality, there is a risk of overcrowding. This can lead to longer waiting times and lower quality of provider-patient interactions. Consequently, these issues may harm health outcomes. 11 In such cases, more healthcare visits may reflect repeated visits for unresolved health problems or poor-quality healthcare, rather than proper and effective use of services. Thus, the increase in visit frequency should be viewed cautiously. It shows only one aspect of access and does not necessarily indicate the effectiveness of the whole system with better health outcomes. 65
Therefore, increased health facility visits do not necessarily result in better health outcomes. For example, though there was a positive association with CBHI membership, healthcare utilization in Ethiopia falls short of international standards across several key metrics. The Healthcare Access and Quality (HAQ) Index, for instance, shows Ethiopia’s score increased from 10.6 in 1990 to 28.1 in 2016, below the global average of 54.4. 66 In addition, the outpatient visits in Ethiopia average only 0.48 per person annually, far below the WHO’s recommended three to four visits per year.67,68
This could be partly due to Ethiopia’s healthcare system, particularly in rural areas may encounter several challenges. There are shortages of skilled staff, frequent shortages of essential medicines, poor infrastructure, and low service quality. 64 If demand rises due to CBHI but service quality and readiness do not improve, problems like overcrowding and long waiting times may happen. This can reduce the quality of healthcare and services’ effectiveness. 38
The cross-sectional design of this study also limits inferences about causality between frequency of health facility visits and CBHI. Women with CBHI may differ from uninsured women in ways this study did not measure. For example, insured women might be better aware and health-conscious, have higher health needs, or suffer from chronic illnesses that lead them to more frequent visits. 69
Additionally, recall bias may also affect the accuracy of self-reported visit data. Long-term studies or quasi-experiments would better show if CBHI directly increases health facility visits or if other factors better explain this link. 70 This study highlights the association between community-based health insurance (CBHI) enrollment and reduced financial barriers as well as increased healthcare utilization among Ethiopian women. It also points to the need for improved service quality to ensure that increased access is associated with better health outcomes. 71
The study conducted in the central zone of the Sidama region further identified some individual and community-level determinants of the frequency of health facility visits. Accordingly, age was positively associated with the frequency of health facility visits. This highlights the need for age-specific healthcare services unique to health challenges faced by the older population, including women, which was complemented in studies from Sri Lanka, 72 Nigeria, 73 India, 74 and Kenya. 75
The positive association between age and healthcare visits can be critically examined through the lens of health needs and awareness. As individuals age, they are more likely to experience chronic conditions that require ongoing checkups, leading to increased healthcare utilization. 76 Furthermore, older adults may also be more aware of their health needs and understand the importance of subsequent care, which can lead to increased utilization rates. This highlights the need for age-specific healthcare strategies that address the unique health challenges faced by older populations. 77
Geographical accessibility was another critical factor associated with healthcare utilization in Ethiopia, as evidenced by the finding that insured women residing farther from health facilities experienced a (41%) reduction in health facility visits compared to those living closer to health facilities. This aligns with existing studies highlighting the role of distance and inaccessibility in healthcare access in Ethiopia.78 -80
Globally, distance consistently emerges as a significant impediment to healthcare access, resulting in reduced utilization and adverse health outcomes. A scoping review underscores the importance of proximity to healthcare facilities in minimizing delays and enhancing health metrics. 81
Countries have adopted diverse strategies to address these challenges. For example, India has successfully leveraged telemedicine and mobile clinics to bridge the urban-rural healthcare divide, utilizing technology to provide specialized care to underserved rural populations through innovations like teleconsultations and mobile health units. 82
This is because telemedicine programs have been proposed as solutions and an alternative to traditional approaches for improving outreach to underserved rural communities, highlighting the need for innovative strategies to bridge geographic gaps in healthcare access. 83 These solutions should be thoroughly examined to ensure they address the complex interplay between physical accessibility and social determinants of health, such as transportation expenses and limited digital literacy, which may further exacerbate disparities in healthcare access. 84
Although Ethiopia continues to rely on traditional healthcare delivery models, it lacks adequate technological integration. India’s approach offers promising alternatives for improving access in remote areas, highlighting the potential of technology-driven solutions to mitigate the issue of geographic barriers. 85
The study also revealed that health services satisfaction was associated with increased health facility visits, consistent with other findings from a systematic review and meta-analysis, 86 Australia, 87 China, 28 South Africa, 88 Ethiopia, 89 and Northwest Ethiopia. 90
However, a study in the UK indicated that patient satisfaction varied significantly across different healthcare services, impacting overall healthcare utilization. The challenges faced in the UK highlight that, while satisfaction is crucial, systemic issues can affect overall healthcare utilization. 91
This relationship underscores the importance of quality care and positive patient experiences in driving higher utilization rates. Critically, patient satisfaction can be influenced by a range of factors, including perceived quality of care, communication with healthcare providers, and cultural sensitivity of services. Therefore, improving patient satisfaction requires a holistic approach that addresses these multifaceted aspects of healthcare delivery. 92
Moreover, women in communities with higher literacy levels exhibited a two times higher frequency of healthcare visits compared to women who resided in communities with lower literacy levels. This result was consistent with studies from India, 93 the United States of America, 94 Ethiopia,95 -97 and a systematic review and meta-analysis. 98 This is because higher literacy rates likely empower women with knowledge about available services and the importance of seeking timely healthcare. 99
However, this relationship can be critically detailed by recognizing that literacy is not solely an individual attribute but is also influenced by broader community factors, such as access to education and cultural norms around health-seeking behavior. 100 Therefore, interventions aimed at improving healthcare utilization through literacy must consider these contextual factors and address systemic barriers to education and health information. 101
Finally, women who lived in low-poverty community areas had a 1.58 times higher frequency of health facility visits compared to those who resided in higher-poverty community areas. This highlights the influence of socioeconomic status on healthcare utilization. Women in low-poverty areas generally hold more positive views of healthcare services, encouraging greater utilization. 102
The finding is consistent with the studies conducted in Taiwan, 103 Nepal, 104 India, 105 Viet Nam. 106 Insights from 21 developing and emerging economies. 107 Study from European Union member states, 108 Netherlands, 109 and an analysis of the most recent Demographic and Health Surveys conducted in 31 countries. 110
This could be explained partly as high poverty areas often lack adequately equipped healthcare facilities, resulting in longer wait times and suboptimal healthcare, which can inhibit women from seeking necessary medical attention. This situation often leads to delays in receiving care, resulting in worsened health outcomes over time. 111 Economic constraints further exacerbate these challenges. Limited financial resources in high-poverty communities frequently lead to inadequate investment in healthcare services, compromising their quality and accessibility. 112
Limitations of the Study
This study has several notable limitations. Firstly, its cross-sectional design restricts causal inferences69,113 about the relationship between healthcare utilization determinants and CBHI membership.
The reliance on self-reported data may introduce response bias, thereby compromising the accuracy of reported healthcare utilization and associated factors. Furthermore, as the data was collected, the previous 1-year information from the respondents may be subject to recall bias.
One notable limitation of this study is the potential for selection bias arising from adverse selection. Specifically, individuals with pre-existing health conditions may be more likely to participate in community-based health insurance schemes.74,114 -116
This could result in an overestimation of the association between community-based health insurance membership and health service utilization, as increased utilization may reflect underlying health needs rather than the direct effect of community-based health insurance coverage.30,31,36
Additionally, the study’s focus is limited to the Sidama National Regional State, which may affect the generalizability of the findings to other contexts. Moreover, concentrating exclusively on women may overlook the influence of male decision-makers and broader family dynamics on healthcare utilization.
While various individual and community-level factors were examined, potential unmeasured socio-cultural influences may also play a role 117 in healthcare utilization, the data collection was confined to a specific timeframe (1 month), possibly missing seasonal variations in health-seeking behaviors may also influence the utilization patterns. 118
Finally, the study’s quantitative approach may have overlooked qualitative insights 119 that could provide a more detailed understanding of participants’ experiences with healthcare utilization. Acknowledging these limitations is essential for refining future research methodologies and deepening the understanding of factors contributing to healthcare utilization.
Conclusion
This study found a significant association between community-based health insurance (CBHI) membership and the frequency of health facility visits among women in the Central Zone of Sidama region, with insured participants attending health facilities 77% more frequently than their uninsured counterparts. Key determinants associated with this relationship included age, satisfaction with healthcare services, geographical accessibility, community literacy levels, poverty status, and family size.
To promote more equitable access to healthcare, it is recommended to expand CBHI coverage, enhance the accessibility of health facilities, improve community literacy, and address barriers related to poverty, taking into account both individual and contextual factors. Furthermore, future research should use longitudinal designs. It should also include baseline health data. This will help clarify how effective CBHI is and support evidence-based policy decisions.
Supplemental Material
sj-docx-1-his-10.1177_11786329251368662 – Supplemental material for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study
Supplemental material, sj-docx-1-his-10.1177_11786329251368662 for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study by Kare Chawicha Debessa, Keneni Gutema Negeri and Mesay Hailu Dangiso in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329251368662 – Supplemental material for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study
Supplemental material, sj-docx-2-his-10.1177_11786329251368662 for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study by Kare Chawicha Debessa, Keneni Gutema Negeri and Mesay Hailu Dangiso in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329251368662 – Supplemental material for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study
Supplemental material, sj-docx-3-his-10.1177_11786329251368662 for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study by Kare Chawicha Debessa, Keneni Gutema Negeri and Mesay Hailu Dangiso in Health Services Insights
Supplemental Material
sj-dta-4-his-10.1177_11786329251368662 – Supplemental material for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study
Supplemental material, sj-dta-4-his-10.1177_11786329251368662 for Health Service Utilization by Women Members and Non-Members of Community-Based Health Insurance Schemes in Sidama, Southern Ethiopia, 2024: A Comparative Cross-Sectional Study by Kare Chawicha Debessa, Keneni Gutema Negeri and Mesay Hailu Dangiso in Health Services Insights
Footnotes
Acknowledgements
The authors wish to express their heartfelt gratitude to the study participants, data collectors, supervisors, Hawassa University College of Medicine and Health Sciences, Sidama National Regional Health Bureau, and the health offices of Dale Woreda and Yirgalem City for their contributions to this study. Their support and collaboration were instrumental in achieving the successful completion of the study.
Ethical Considerations
This study complied with the Declaration of Helsinki and its amendments, ensuring ethical standards for human research. Ethical approval was granted by the Hawassa University College of Medicine and Health Sciences IRB (Ref: IRB/021/16, November 22, 2023). Informed written consent was obtained from all study participants.
Consent to Participate
Confidentiality and privacy were strictly maintained. Study participants were fully informed about the study’s purpose, procedures, and confidentiality assurances, with these details included in the consent form. The consent process was thoroughly documented. Additionally, a support letter was secured to reinforce participant protections. Together, these measures ensured rigorous ethical oversight, prioritizing participant privacy and anonymity throughout the study.
Authors’ Contributions
Kare Chawicha Debessa: Led conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resource management, software development, supervision, validation, and drafting of the manuscript. Keneni Gutema Negeri: Contributed to formal analysis, investigation, methodology, project administration, supervision, validation, and the drafting of the manuscript. Mesay Hailu Dangiso: Engaged in formal analysis, investigation, methodology, supervision, software development, validation, and the drafting of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Sidama National Regional Health Bureau. The funding agency did not participate in the conceptualization, design, data analysis, manuscript preparation, or publication processes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets employed in this study can be found within the manuscript as Supplemental File 3.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.