
Abstract
Background:
Community-based health insurance (CBHI) plays a crucial role in achieving universal health coverage. This study investigates the determinants, challenges, and opportunities related to CBHI in Tigray, Ethiopia.
Design and methods:
A mixed-methods approach was employed. In 2020, a cross-sectional survey was conducted involving 800 rural households in Tigray, combined with semi-structured key informant and in-depth interviews. Multistage random sampling and logistic regression analyses were also applied.
Results:
Enrollment was strongly associated with having a chronic illness (AOR = 64.5, p ≤ 0.01), primarily due to a policy that permits indigents with chronic conditions to enroll without payment. Other factors included membership in a political party (AOR = 3.76, p ≤ 0.01), holding formal positions (AOR = 1.55, p = 0.03), receiving aid (AOR = 1.62, p ≤ 0.01), and membership in Edir (AOR = 1.66, p ≤ 0.01). Conversely, enrollment was negatively impacted by low trust (AOR = 0.66, p = 0.04), limited awareness (AOR = 0.4, p ≤ 0.01), poor healthcare quality (AOR = 0.51, p ≤ 0.01), bureaucracy (AOR = 0.02, p ≤ 0.01), being widowed (AOR = 0.34, p ≤ 0.01), and working as a daily laborer (AOR = 0.23, p ≤ 0.01). Key barriers included structural inefficiencies, substandard healthcare service quality, and inadequate awareness.
Conclusion:
To facilitate equitable expansion of CBHI, it is essential to address administrative obstacles, enhance trust and awareness, and provide support to vulnerable groups, in addition to leveraging traditional risk-pooling mechanisms.
Introduction
Community-based health insurance (CBHI) is a promising health financing strategy aimed at protecting low-income, vulnerable, and informal sector populations from high healthcare costs while improving access to essential services.1–3 International development agencies increasingly recognize CBHI as a critical pathway to achieving universal health coverage (UHC), particularly in rural areas where health disparities and weak financial infrastructure pose significant challenges.4,5
By reducing out-of-pocket expenses and increasing service utilization, CBHI can substantially enhance equity in healthcare access. However, implementation in low-income countries faces persistent challenges. High dropout rates and limited impact are common when enrollment remains voluntary, and risk pooling is insufficient. Without robust government support and subsidies targeting the poorest populations, CBHI schemes often struggle to make sustained progress toward UHC.6–8
Since the 1990s, CBHI initiatives across Sub-Saharan Africa have yielded mixed results, 9 frequently hindered by operational inefficiencies and weak management. 10 In Ethiopia, CBHI was introduced in 2011 as part of a national strategy to promote domestic resource mobilization and provide financial protection to the informal sector, which accounts for approximately 85% of the population.2,11 Pilot schemes launched in 2013 across 13 woredas in the Tigray, Amhara, Oromia, and SNNP regions achieved a 48 percent enrollment rate within 2 years. 12 Buoyed by this success, the program expanded nationwide in 2016 to include 198 districts and more than 800 kebeles.13,14 However, by 2020, enrollment among informal workers remained at only 37%, concentrated primarily in major regions and Addis Ababa, highlighting significant gaps in reaching the national target of 80%.2,15
Although numerous studies have examined CBHI implementation, findings regarding the sociodemographic determinants of enrollment remain inconsistent.16,17 Furthermore, few have specifically focused on the Tigray Regional State. This research addresses this gap by providing a comprehensive assessment of the determinants, challenges, and opportunities related to CBHI in Tigray, with the goal of supporting improved performance and advancing progress toward UHC in Ethiopia.
Methods
Study design and setting
This study used a mixed methods design to investigate the determinants, challenges, and opportunities of CBHI implementation in Tigray, northern Ethiopia. Quantitative and qualitative approaches were applied concurrently to provide a comprehensive understanding. Quantitative data identified household-level factors influencing enrollment, while qualitative data explored implementation challenges and local conditions affecting performance. This combination allowed triangulation, enhancing the depth and validity of the analysis. Data collection occurred between May and September 2020, after a survey pretest from December 2019 to January 2020.
The study area, Tigray, located in northern Ethiopia and bordered by Eritrea, Sudan, Amhara, and Afar, has diverse geographic and socioeconomic factors influencing health access and insurance participation. According to the Ethiopian Health Insurance Agency Northern Branch in Mekelle, 818,865 households were targeted for CBHI enrollment, but only 44,438 had registered by data collection, underscoring the need to examine both statistical patterns and contextual barriers.
In addition to surveys, interviews with health officials, insurance coordinators, and community representatives were conducted using protocols developed through literature review and team consultation to ensure rigor and local relevance. This mixed-method approach balanced numerical data with lived experiences, providing practical insights to improve scheme implementation.
Sampling and sample size
This study utilized a two-stage sampling method for the quantitative part. In the initial stage, three districts were purposively selected based on their role as the first to pilot the CBHI scheme in 2013. Ahferom, located in Central Tigray, is the most populous district with dense settlement patterns and relatively better infrastructure. Kilte-Awlaelo, situated in Eastern Tigray, reflects mid-altitude agroecological characteristics and moderate population density. Tahtay-Adiyabo, positioned in Northwestern Tigray, is characterized by lowland terrain and sparse settlements, presenting unique logistical challenges that affect service delivery and insurance uptake.
These districts stood out as the only areas in Tigray where CBHI was piloted in 2013, unlike other woredas that implemented CBHI after 2015. In the subsequent stage, proportional random sampling was applied to select households from these districts, ensuring fair representation.
Yamane’s formula, introduced in 1967, was employed to calculate the sample size, ensuring statistical reliability by applying a 5% significance level.

when n = sample size, N = population size, and e = significance level
Based on enrollment data, 400 households insured under CBHI were randomly selected using computer-generated numbers. To facilitate one-to-one matching and to support valid comparisons, an equal number of uninsured households were drawn from the same kebeles using woreda-level registration and administrative records. In total, 800 households were included, proportionally distributed across the districts according to number of enrolled and non-enrolled households, as presented in Table 1.
Sample distribution among the selected woredas.
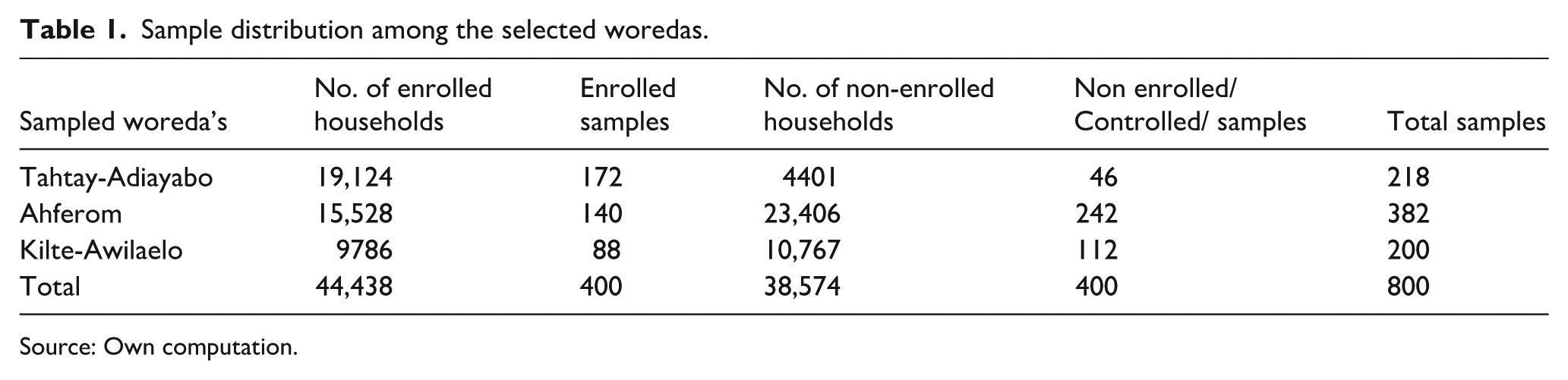
Source: Own computation.
Inclusion and exclusion criteria
For the quantitative component, participants were eligible if they had been enrolled in CBHI for at least 1 year or had been unenrolled for at least 1 year and had lived in the local area for at least 1 year. For the qualitative component, participants included those with three or more years of experience in CBHI leadership or committee roles. Individuals not meeting these criteria were excluded.
Data and data collection
Quantitative data were collected via a structured questionnaire (see appendix 3) examining sociodemographic, socioeconomic, and health-related factors affecting CBHI enrollment and outcomes. Originally in English, the questionnaire was translated into Tigrigna for data collection and retranslated into English for accuracy. A pilot test with 5% of the sample from neighboring kebeles identified ambiguous items, which were revised for clarity.
Acknowledging limitations of self-reported data, such as recall and social desirability biases, data collectors were trained to use neutral, consistent prompts. Surveys were conducted anonymously to encourage honest responses and reduce bias.
Data collection involved 10 experienced data collectors supervised by trained personnel. They received thorough training on study objectives, ethics, and privacy. Supervisors ensured daily quality control and interrater consistency. Secondary quantitative data from government records and literature helped validate findings.
Qualitative data were gathered through semi-structured, face-to-face interviews with 15 key informants (EHIA branch leaders, regional reps, sub-branch managers) and six in-depth interviews with community leaders (see appendix 4). In-depth interviews were preferred over focus groups to explore sensitive political issues and nuanced opinions. This combination strengthened validity and provided rich insights into CBHI challenges and opportunities.
Interview guides (see appendix 1) were developed through literature review and team discussions, then pretested for clarity. Written informed consent was obtained. Interviews, conducted in Tigrigna, lasted 40–60 min, were audio-recorded, and supplemented with detailed notes. Sessions took place in quiet, participant-chosen locations, mostly workplaces, to ensure comfort and openness.
Data analysis
Following data collection, primary quantitative data were entered into Excel and then exported to STATA version 17 for analysis. Descriptive statistics, including tabulations, two-sample t-tests, and chi-square tests, were performed.
For empirical analysis, logistic regression was selected as the most appropriate econometric model due to the binary nature of the dependent variable, indicating CBHI enrollment (yes/no). This approach estimates the probability of participation based on multiple explanatory variables while controlling for potential confounders. Unlike linear regression, which assumes a continuous outcome and can yield biased estimates in such cases, logistic regression is specifically designed for categorical dependent variables. Moreover, compared to the probit model, logistic regression coefficients—expressed as odds ratios—are more interpretable, providing meaningful information for public health decision-making and policy development. The model uses the logit link function to transform the expected value of the dependent variable into a logit, enabling robust estimation of the factors influencing enrollment decisions. 18
The logit link function is:

Where: p represents probability of Y = 1
Yi = the choice dependent variable (membership of CBHI: member HHs and Nonmember HHs)
n = total number of observations
The logit function is the natural log of the odds that Y equals one of the groups, Y has only two categories (0 for non-members and 1 for members). The logit regression function for the determinants of enrollment in the CBHI was mathematically expressed as follows:

Where:
●
● B0 = intercept term (average when all the observed variables are zero)
● Bi = coefficient parameters for each independent variable Xi
● Xi = independent variables:
X1 = Marital status of Household Head
X2 = education level of household head
X3 = Family Size
X4 = Age of Household Head
X5 = Gender of Household Head
X6 = Highest Education Level in the Household
X7 = Being a Member in PSNP
X8 = Formal Position Status of the Household Head
X9 = Wealth
X10 = Chronic Illness
X11 = Position
X12 = Distance to the Nearest Health Center
X13 = Perception of Quality Care
X14 = perception of Trust
X15 = Awareness level
X16 = the perception of bureaucracy
● εi = error term
The variables included in the determinants model (equation (2)) were selected based on statistically significant mean differences identified through independent-sample t-tests and chi-square tests. These preliminary analyses ensured that the predictors included in the logistic regression model were both statistically relevant and substantively meaningful. To address potential heteroskedasticity, robust standard errors were applied, enhancing the reliability of the inference. Multicollinearity was assessed using the Variance Inflation Factor (VIF), which provided a diagnostic measure of the linear correlation among independent variables. All VIF values fell within acceptable limits, indicating that multicollinearity was not a significant concern in the model.
For qualitative data analysis, the conventional content analysis method was used, allowing codes to be derived directly from the text without relying on pre-established categories. Themes emerged inductively, reflecting participants lived experiences. A coding tree was developed to organize codes into categories and overarching themes, enhancing transparency and structure in the analytical process. Data saturation was achieved when no new codes or categories emerged from additional interviews, confirming that the dataset was sufficiently rich for comprehensive analysis. To strengthen reliability, member checking was conducted as participants reviewed and validated the developed codes, themes, and categories. Two independent coders analyzed the data to ensure consistency and minimize bias. Integration occurred throughout the process, with findings from qualitative and quantitative components continuously compared and interpreted together. All coauthors participated in reviewing both datasets and engaged in collaborative reflection to ensure interpretations were grounded in both statistical trends and participant narratives.
Operational definition of main variables
The study investigates membership status in the CBHI scheme as the primary dependent variable, alongside demographic, socio-economic, and health-related predictors measured via the structured questionnaire.
Membership Status: Defined as a dummy variable, where “0” indicates members and “1” indicates non-members, denoting participation in CBHI.
Awareness Level: Measured through six questions covering CBHI concepts, roles, and beneficiaries. Correct answers were scored as one, and incorrect answers as zero. Total scores ranged from 0 to 6, categorizing participants into low (≤2), medium (3-4), or high awareness (5–6, ≥83.3%). This classification was adapted from previous study (19).
Productive Safety Net Program (PSNP): A seasonal social safety net initiative launched in Ethiopia in 2005, designed to prevent famine and protect household assets through labor-based transfers for public works. The program addresses food shortages, builds community assets, and mitigates shocks such as droughts.
Edir: A traditional Ethiopian risk-pooling association that provides mutual support during hardships, especially bereavement, through financial and emotional assistance.
Results
Descriptive findings
This study surveyed 800 households to analyze their socioeconomic, demographic, and health-related characteristics (Table 2). Of these, 70.5% were male-headed and 29.5% female-headed. Among household heads, 74.5% were married, 16% widowed, 4.1% single, and 5.6% divorced or separated. Religiously, 91.3% identified as Orthodox Christians, 8.3% Muslims, and 0.5% other religions (Protestantism, Catholicism).
Chi-square result for nominal and ordinal variables.
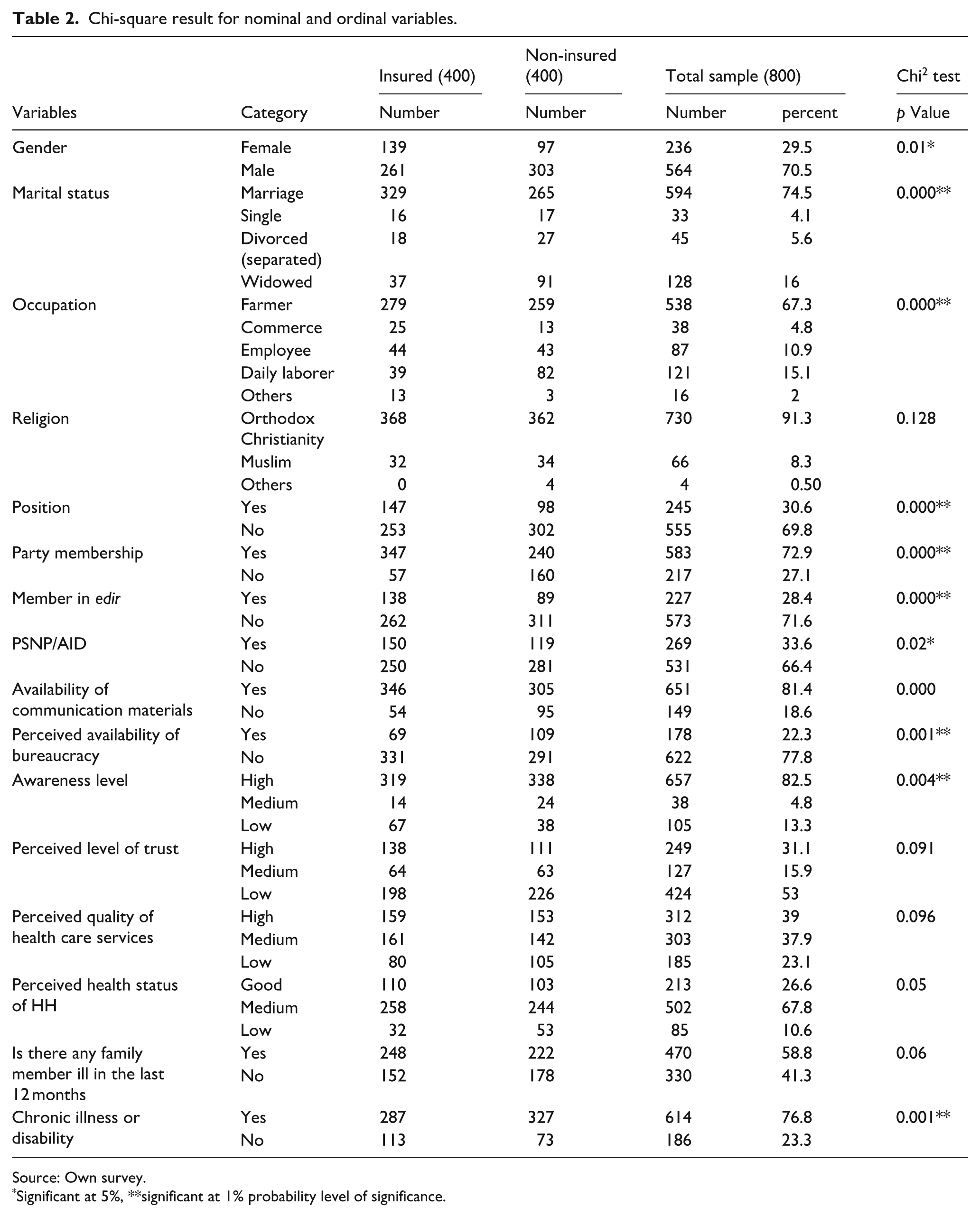
Source: Own survey.
Significant at 5%, **significant at 1% probability level of significance.
Farming was the main occupation for 67.3%, followed by daily laborers (15.1%), employees (10.9%), merchants (4.8%), and others (2%). Average household size was 4.6, with a working-age average of 2.2 members (18–60 years). Education levels were modest: household heads averaged 4.4 years of schooling, while the highest family attainment averaged 8.2 years.
Chi-square tests showed significant associations (p < 0.01) between CBHI enrollment and marital status, occupation, Edir membership, political party membership, perceived bureaucracy, chronic illness or disability, and communication device access. Additionally, gender and aid availability were significant at p < 0.05, offering detailed insights into factors influencing these households.
Households faced significant challenges accessing healthcare (Table 3). Families traveled an average of 10.3 km to the nearest health center, with distances ranging from 0.2 to 40 km, highlighting difficulties for those living farther away. Financial disparities were evident, with an average annual expenditure of 24,516.5 birr and average wealth of 73,847.2 birr, ranging widely from 1000 to 3,000,000 birr, indicating substantial economic inequality.
t-test result for continuous variables.

Source: Own survey, 2020.
Significant at 5%, **significant at 1% probability level of significance.
T-test analyses showed significant differences (p ≤ 0.01) in highest family education, number of males, number of individuals aged 18–60, and household wealth. The number of females was significant at p ≤ 0.05, providing insights into factors affecting healthcare access.
Determinants of enrollment decision into CBHI
Binary logistic regression (Table 4) identified key factors affecting CBHI enrollment. Low trust in CBHI and healthcare providers reduced enrollment likelihood (AOR = 0.66; 95% CI = 0.44–0.98, p = 0.04), while households with chronic illness or disability had much higher odds of enrolling (AOR = 64.5; 95% CI = 13.55–307.49, p ≤ 0.01).
The factors affecting enrollment in CBHI, result of binary logistic regression.

Source: Own survey.
AOR: adjusted odds ratio.
Significant at 5%, **significant at 1% probability level of significance.
Widowed heads were less likely to enroll than married ones (AOR = 0.34; 95% CI = 0.16–0.7, p ≤ 0.01). Daily laborers were also less likely than farmers to join (AOR = 0.23; 95% CI = 0.14–0.04, p ≤ 0.01), whereas pensioners and unemployed were more likely (AOR = 20.8; 95% CI = 3.32–130.3, p ≤ 0.01). Low awareness and negative perceptions of healthcare quality decreased enrollment odds (AOR = 0.4 and 0.51, respectively; p ≤ 0.01).
Perceived bureaucracy and poor administration negatively influenced enrollment, as households with high perceptions of bureaucracy were 0.02 times less likely to join (AOR = 0.51; CI = 0.01–0.07, p ≤ 0.01). In contrast, political party membership, holding formal community positions, PSNP participation, and Edir membership increased enrollment likelihood by 3.8 times, 1.6 times, 1.6 times, and 1.7 times, respectively (all p ≤ 0.03).
Qualitative result
This part of study examined the benefits, challenges, and opportunities of CBHI implementation in Tigray Regional State, Ethiopia. Key findings were gathered through informant interviews, supplemented by in-depth interviews for a more comprehensive analysis.
The informant interview result
Benefits of CBHI
Key Informant (KI) findings reveal that the benefits of CBHI can be systematically categorized into distinct thematic areas. These include improving healthcare utilization, protecting households from catastrophic health expenditures, promoting social interactions within communities, addressing health and income inequalities, empowering women, and enhancing the quality and accessibility of healthcare services.
Boosts Healthcare Service Utilization
The CBHI scheme has significantly enhanced healthcare utilization among poor households. Key informants emphasized its role in creating awareness and reducing out-of-pocket health expenditures, encouraging rural families to take greater responsibility for their health.
CBHI serves as an alarm bell for rural households to take care of their health. After the implementation of the scheme, the utilization of healthcare is continuously increasing. – KI-3
Reduces Catastrophic Health Expenditures
CBHI protects households from catastrophic health expenditures, reducing the need to sell property, borrow money, or resort to begging to cover healthcare costs during health shocks.
CBHI protects against unexpected selling of property, borrowing, and begging. – KI-15
Increases in Social Interaction in the Community
The scheme promotes social interaction and engagement by fostering healthier individuals who participate in community meetings and training. It also improves household income by enhancing health, which contributes to productivity.
Healthy individuals are more productive than unhealthy ones. Therefore, CBHI can boost household income by improving health conditions. – KI-5
Reduces Inequality and Empowers Women
CBHI reduces health and income inequality, directly improving access to healthcare while empowering women. Female-headed households have especially benefited, as women can seek treatment independently without relying on male partners for financial support.
Female members of CBHI now go to health institutions without needing to ask for money from their male spouses, which is a significant benefit for rural females. – KI-6
Improves Quality and Accessibility of Healthcare Services
CBHI has led to improvements in healthcare service quality, as health bureaus conduct assessments of institutions to ensure compliance with contractual obligations.
Under the contract between CBHI schemes and healthcare provider institutions, many institutions have improved their service quality. – KI-10
Challenges of CBHI
Key Informants (KIs) provide crucial insights into the challenges confronting the CBHI scheme in Tigray National State. These findings are systematically categorized into thematic areas and their respective sub-themes, which include structural and administrative issues, awareness-related barriers, fluctuating enrollment and renewal rates, affordability and financial sustainability challenges, and limitations in healthcare capacity and quality.
Structural and administrative problems
Key informants highlighted significant issues in the structure and administration of CBHI, including:
Lack of Clear Structure and Communication Among Actors: The CBHI scheme lacks clear accountability and effective coordination between the EHIA, health bureaus, district schemes, and regional coordinating committees. The unclear administrative structure creates confusion, particularly at the woreda level, where limited staff struggle to manage responsibilities effectively.
There is no clear administrative accountability regarding who is more responsible for the development of the CBHI scheme – KI-12 . . .As CBHI staff, we report to multiple authorities, but unfortunately, the administrative hierarchy and lines of responsibility are unclear. A well-defined structure is essential for the effective development and implementation of the scheme – KI-8
Poor administration and Bureaucracy: Bureaucratic delays, such as lengthy reimbursement processes and the scheduling inconsistencies of CBHI board meetings, lead to transportation costs, reduced community trust, and inefficiencies in service delivery. These issues are exacerbated by political crises, affecting enrollment rates and satisfaction levels.
Bureaucracy and bias remain a source of complaints for several households. Addressing poor administration is halfway to solving the issue, – KI-9
Lack of Professional Human Resources: CBHI staff are often transferred from the health bureau without sufficient training in health insurance management. The shortage of trained professionals and an inadequate workforce affects the efficiency of CBHI operations.
This scheme needs professional workers trained in health insurance management. The government has’,t given enough attention compared to the scheme’s benefits. – KI-13
Weak Data Management: CBHI currently relies on manual systems for enrollment, claims processing, and audits. The absence of digital technology solutions hampers transparency, timely service delivery, and efficient problem resolution.
Data management in the CBHI scheme is weaker than in other sectors, even if there has been some improvement recently, – KI-1
Awareness-related issues
Low awareness among the community and other actors was identified as a major challenge affecting CBHI.
Lack of Knowledge: The community, government administrators, and healthcare providers often lack understanding of CBHI’s short-term and long-term benefits, as well as its packages.
Many people argue about the level of benefits due to a lack of knowledge, – KI-9
Wrong Perceptions: Negative perceptions, such as perceived bias by healthcare providers and false rumors, hinder enrollment, renewal, and utilization of CBHI services.
The big problem is the awareness and perception of the community. Several members perceive healthcare providers as biased against them, – KI-7 Some patients tried to hide their CBHI card at health facilities to avoid perceived bias, only presenting it after receiving treatment. This behavior led to procedural disruptions and strained interactions between providers and patients. – KI-4
Low Trust: Low trust in CBHI, stemming from poor management, awareness gaps, and unmet expectations, has grown over time. Negative rumors further weaken public confidence in the scheme.
Negative false rumors offset the positive referrals to the scheme. The government has not done enough to combat these rumors, – KI-11
Fluctuating Enrollment and Renewal Rates
CBHI has experienced fluctuating enrollment trends and low retention rates, posing sustainability challenges. For example, in Woreda Ahferom, the average renewal rate from 2012 to 2020 was 0.61, indicating that 40% of members did not renew their membership. This inconsistency reflects systemic and operational hurdles.
Despite an initially promising start, enrollment trend showed irregular patterns, reflecting operational and systemic hurdles. – KI-15
Affordability and Financial Sustainability Problems
Many woredas face budget deficiencies and insolvency issues. Some low-income households struggle to afford premiums, while adverse selection in government subsidies worsens financial instability.
The premium amount is small, but budget deficiency and adverse selection for subsidies make it worse, – KI-5
Limitations in Healthcare Capacity and Quality
Healthcare institutions lack the capacity to deliver quality services. Common challenges include shortages of drugs, medical equipment, and professionals, as well as misconduct by private drugstores issuing fake receipts to members.
Households complain about drug availability. After diagnosis, health providers send them to private drugstores, where reimbursement delays occur, – KI-7
Opportunities of CBHI scheme
Traditional Risk-Pooling Experiences in Society
The CBHI scheme benefits from the community’s experience with traditional risk-pooling programs, particularly Edir, widely practiced in Tigray. Edir serves as a foundation for understanding and adopting CBHI principles. The government is encouraged to study and apply the successful practices of Edir to further strengthen CBHI.
The community has good experience with pooling risks through different traditional associations like Ekub, Mahber, and mainly Edir. We can consider this an opportunity to improve the CBHI scheme. – KI-7
Strong Political, Cultural, Religious, and International Support
CBHI benefits from support provided by political, cultural, and religious institutions, as well as contributions from international organizations like the WHO. Additionally, wealthy individuals assist by covering premiums for disadvantaged households, broadening the scheme’s reach and impact.
Religious leaders are supportive and have expressed their support for the scheme in various meetings and media. They have said that the CBHI goals align with their religious teachings, such as pooling financial risk from the healthy to the sick or from the rich to the poor. – KI-5
Availability of Civil, Political, and Religious Associations
Numerous associations, including youth groups, women’s associations, veterans’ groups, farmers’ associations, and the “1 to 5” structure, provide valuable resources for mobilization and targeted subsidization of the poorest households.
. . .we can use associations for mobilization purposes and for recruiting the poorest for targeted subsidization. – KI-1
In-depth interview results
The findings from the in-depth interviews closely echoed those of the key informant interviews, reinforcing shared themes and challenges in the implementation of the CBHI scheme in Tigray. Participants emphasized administrative issues such as biased practices, corruption, and poor governance, which were further exacerbated by political unrest. Gaps in follow-up and evaluation processes, along with disputes over the allocation of medical supplies and drugs, were also reported.
Referral delays emerged as a critical concern, particularly in emergencies like snake bites. Procedural hurdles and requirements for upfront payments often had severe consequences, including fatalities. One tragic case in Ahferom Woreda involved a delay in issuing a referral certificate, which led to a woman’s death—an event that profoundly affected community trust and demoralized CBHI staff.
Misperceptions regarding CBHI premiums were another significant issue. Some community members believed their premiums were wasted if healthcare services were not utilized and suggested that unused premiums should be carried forward or credited toward future renewals. These misunderstandings undermined participation in the scheme.
Overall, the interviews provided valuable insights into the challenges impacting CBHI implementation and highlighted important areas for improvement, including enhancing administration, resolving referral issues, and fostering greater understanding and trust within the community.
Discussions
The Ethiopian Community-Based Health Insurance (CBHI) scheme has made significant progress, largely due to strong government involvement. This support, including subsidies and effective administration, distinguishes it from many voluntary, community-managed schemes that often lack such backing, and has been vital to the scheme’s success (2017 WHO report). Although challenges remain, the scheme has achieved notable milestones in expanding coverage.
The descriptive analysis showed 70.5% of participating households were male-headed and 29.5% female-headed, consistent with FAO (2006) findings. 20 Household heads had an average of 4.4 years of education, but the highest educational level within families, nearly twice as high, significantly influenced enrollment decisions according to t-tests. Educated family members, such as children and spouses, often played pivotal roles in enrolling households, often outweighing household heads’ influence given their limited schooling. This highlights the importance of considering the highest family education level, particularly in rural and developing contexts. Future research should explore this factor further for deeper insights into enrollment dynamics.
Logistic regression revealed widowed households were less likely to enroll than married ones, possibly due to lower incomes, reduced social capital, and stigma, which can act as barriers. This finding aligns with studies by Moyehodie et al. and Teshome Bekele (2022)21,22 Many widowed female-headed households in the region result from recurrent conflicts; thus, special attention to female-headed households is warranted. Similarly, divorced heads showed lower enrollment likelihoods than married heads, though this was not statistically significant.
Households with chronic illnesses or disabilities were much more likely to enroll, reflecting their greater healthcare needs and access to subsidies, which is consistent with several studies.19,23 However, this finding contrasts with some research 24 where these factors were insignificant, possibly due to differing study settings or methodologies.
Daily laborers were less likely to join CBHI compared to farmers, likely due to irregular and low incomes that limit financial planning and living expense coverage. Their minimal participation in community meetings may also reduce awareness of the scheme, an observation supported by a 2017 Ethiopian study. 25 In contrast, pensioners (veterans) and unemployed individuals had higher enrollment rates than farmers, attributable to targeted government subsidies. Indigent households constitute about 21% nationally. 26 However, this contrasts with a Malawi study (2022), where economic barriers prevented both pensioners and unemployed individuals from enrolling. 27
While wealth showed a positive influence on CBHI enrollment, it was statistically insignificant in this study. The low annual premium (240 birr, about $2.10) makes the scheme affordable even to poorer households. In Tigray, 26% of enrolled households received subsidies intended for indigent members. Although logistic regression found wealth insignificant, t-tests and qualitative data suggested a positive association, implying wealth may affect enrollment but less strongly than other factors. This aligns with findings from Eseta et al. and Chanie and Ewunetie (2020), who reported higher enrollment among wealthier households without statistical significance.6,28 Wealth was similarly insignificant as a predictor of dropout in Jimma, Ethiopia, while other studies did not include wealth due to contextual or methodological reasons.
Low awareness was strongly associated with reduced enrollment, consistent with existing studies.11,29 Negative perceptions about healthcare quality and bureaucratic obstacles also discouraged enrollment. 30 Trust emerged as a crucial factor: low trust in CBHI and healthcare providers significantly lowered enrollment likelihood.17,19 Without trust, voluntary schemes struggle to attract members, emphasizing the need to improve quality of service and member attitudes to sustain participation. 31
Household heads holding formal governmental or non-governmental positions were more likely to enroll. These roles provide direct exposure to CBHI through meetings and stakeholder interactions, increasing awareness. Such individuals often act as community role models, influencing decision-making and activities. This influence of formal positions has been largely overlooked, yet findings underscore their critical role in enhancing enrollment rates. Engaging community leaders thus represents a promising strategy for expanding CBHI participation.
Membership in Edir (traditional social insurance associations) and political parties correlated with higher enrollment. Edir membership imparts substantial knowledge and experience in risk-pooling, positively impacting enrollment decisions. According to the World Bank (2018), while modern insurance knowledge is generally low among Ethiopians, Edir sustains a strong informal insurance culture. This study uniquely includes political party membership as an influencing factor, a variable rarely considered in CBHI literature but suggested by pilot survey feedback. Political membership provides access to meetings and outreach that raise awareness and encourage insurance participation. This insight offers a fresh, context-specific perspective on social drivers of CBHI enrollment.
Qualitative findings emphasized CBHI’s benefits, primarily increased healthcare utilization, aligning with quantitative studies such as Atinafu, 32 which found insured families accessed services nearly twice as often (50.5% vs 29.3%). Another significant benefit is reduction of catastrophic health expenditures, supported by a Northeast Ethiopia study reporting only 4.4% of insured households faced catastrophic expenses compared to 15.6% of uninsured. 33
CBHI also plays an important role in empowering women, especially in rural areas where male heads traditionally control finances, often delaying medical funds. CBHI facilitates women’s direct access to healthcare, improving outcomes and timeliness of care. Key informants noted women experienced greater increases in healthcare use and out-of-pocket expenditure reductions than men, and are increasingly assuming leadership roles within CBHI schemes, enhancing their capacities. These findings point to the need for further research on gender- and age-disaggregated benefits of CBHI.
Despite advantages, the study identified substantial challenges and opportunities. Structural and administrative issues—inefficient information flow, weak monitoring, and unclear leadership—threaten scheme sustainability. Ms. Frehiwot Abebe, Director General of the Ethiopian Health Insurance Agency (EHIA), noted difficulties in reimbursing facilities due to fragmented pooling, ineffective purchasing, and weak claims auditing. Public, coordinator, provider, and stakeholder awareness remains low, resulting in misconceptions, rumors, and apathy that reduce enrollment and renewal rates.
Healthcare providers face inadequate preparedness, limited capacity, and subpar care quality, with many facilities not prioritizing CBHI. 34 Financial instability is pronounced: low premiums fail to cover costs, and adverse selection excludes the poorest. Interviews revealed corruption, medicine shortages during political crises, referral delays, and mistrust amplified by false rumors, echoing observations that “bad news travels faster than good news,” 35 all of which negatively impact renewal rates.
Nevertheless, strong political, cultural, and religious support, combined with community experience in traditional mechanisms like Edir and widespread associations, create a favorable environment for CBHI expansion and progress toward universal health coverage. These supportive factors, often overlooked in prior research, distinguish this study and highlight important prospects to improve CBHI reach and effectiveness.
Limitations of this study include the study’s timing in the politically tense Tigray region during COVID-19 and the onset of northern Ethiopia’s armed conflict, which may have influenced responses. Furthermore, primary data relied on participant interviews, potentially affected by respondents’ willingness and recall accuracy.
Conclusions
Ethiopia’s CBHI scheme stands out for its strong government support in administration and financing, differentiating it from similar models in other developing countries. Enrollment is influenced by factors such as disability, chronic illness, political affiliation, formal leadership roles, participation in the Productive Safety Net Program (PSNP) and Edir associations, marital status, occupation, awareness, perceived service quality, and bureaucratic barriers.
Qualitative findings show that CBHI improves healthcare utilization, reduces out-of-pocket expenses, and protects families from catastrophic health costs. It particularly benefits women, who gain greater access to services and financial protection, helping reduce inequality and empowering women through subsidies and increased participation in health management.
Despite successes, challenges remain including structural and administrative issues, limited awareness among communities and administrators, suboptimal service quality, and financial sustainability concerns. Opportunities for growth include integrating traditional risk-pooling like Edir, mobilizing political, cultural, and religious networks, and strengthening community associations.
Sustaining the scheme requires strong political commitment and strategic measures such as expanding contracts with private providers, increasing financial support to avoid insolvency, providing enrollment and retention incentives, and improving essential medicine and equipment supply. Awareness campaigns need scaling via media and outreach through political, civil, and religious groups. Capacity building for administrators, transparent management to build trust, and targeted support for vulnerable groups like widows and daily laborers are also vital.
Moving from voluntary to mandatory enrollment and introducing social health insurance are key steps toward a sustainable national insurance system. Future research should investigate the long-term equity and financial impacts of this transition to guide inclusive health policies.
Supplemental Material
sj-doc-3-phj-10.1177_22799036251388587 – Supplemental material for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study
Supplemental material, sj-doc-3-phj-10.1177_22799036251388587 for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study by Abraham Gebrehiwot Yihdego, Ali Akbari Sari, Maryam Tajvar and Amirhossein Takian in Journal of Public Health Research
Supplemental Material
sj-docx-1-phj-10.1177_22799036251388587 – Supplemental material for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study
Supplemental material, sj-docx-1-phj-10.1177_22799036251388587 for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study by Abraham Gebrehiwot Yihdego, Ali Akbari Sari, Maryam Tajvar and Amirhossein Takian in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251388587 – Supplemental material for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study
Supplemental material, sj-docx-2-phj-10.1177_22799036251388587 for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study by Abraham Gebrehiwot Yihdego, Ali Akbari Sari, Maryam Tajvar and Amirhossein Takian in Journal of Public Health Research
Supplemental Material
sj-pdf-4-phj-10.1177_22799036251388587 – Supplemental material for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study
Supplemental material, sj-pdf-4-phj-10.1177_22799036251388587 for Determinants, challenges, and opportunities of the community-based health insurance scheme in Tigray Regional State, Ethiopia: A mixed method study by Abraham Gebrehiwot Yihdego, Ali Akbari Sari, Maryam Tajvar and Amirhossein Takian in Journal of Public Health Research
Footnotes
Acknowledgements
We extend our heartfelt thanks to all study participants and the CBHI coordinators from the study area for their valuable contributions. Our gratitude also goes to the respected editors for their insightful feedback, which greatly improved this manuscript. We express our appreciation to Tehran University of Medical Sciences for providing a partial scholarship that made this study possible. Finally, we would like to thank Aksum University for their unwavering support throughout the research process.
Ethical considerations
Ethical approval was granted by the Ethical Review Board of Tehran University of Medical Sciences (Approval ID: IR.TUMS.SPH.REC.1398.217).
Consent to participate
All participants provided written informed consent.
Author contributions
YAG led the conceptual development, study design, data collection, and drafted the manuscript. AAS, MT, and AT served as academic advisors, contributing to conceptual refinement, supervision of data collection, and providing editorial guidance throughout the manuscript preparation. All authors reviewed and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting this study is available upon reasonable request from the corresponding author, adhering to ethical guidelines.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.