
Abstract
In Ethiopia, there is low enrollment and a wide discrepancy in willingness to pay for community-based health insurance schemes, and there is a lack of nationally representative data on willingness to pay for community-based health insurance. Thus, this systematic review and meta-analysis aimed to estimate the pooled prevalence of willingness to pay for community-based health insurance and associated factors in Ethiopia. This was developed using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Databases such as PubMed/Medline, CINAHL, African Journals Online, and Google Scholar searches were performed to retrieve available published and unpublished studies from December 15 to May 17, 2022. Two independent reviewers screened the retrieved articles. Critical quality appraisal was performed using the Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument. To investigate the sources of heterogeneity, subgroup analysis and meta-regression were performed based on region, study setting (rural/urban), and sample size. RevMan software and STATA 14 software were used for the statistical analysis. A random-effect model was used to estimate the effect size at a 95% confidence interval. A total of 190 studies were retrieved, and six studies were included in the final meta-analysis. The pooled prevalence of willingness to pay for community-based health insurance was 78 (95% confidence interval: 74, 81). A subgroup analysis by region indicated the lowest proportion of willingness to pay community-based health insurance in the Oromia region, 76% (95% confidence interval: 68, 84), and the highest in the Amhara region, 79% (95% confidence interval: 77, 81). Nearly three in four households were willing to pay for community-based health insurance in Ethiopia. Thus, awareness of willingness to pay community-based health insurance is mandatory to improve the implementation of community-based health insurance.
Keywords
Introduction
Health insurance is a means to improve access to health care services by avoiding direct payments of fees by patients and helping spread the financial risk among all insured members.1,2 It is a means of pooling risks across different population groups so that it significantly reduces the financial burden of catastrophic illnesses for individuals. 3 There are two types of health insurance systems; these are social health insurance and community-based health insurance. Social health insurance (SHI) mainly focuses on individuals working in formal sectors. However, the community-based health insurance (CBHI) system is the most appropriate insurance model for employees of informal sectors and households in rural areas in low-income countries since their income is unpredictable. These two health insurance systems improve access to health services and guarantee the success of universal health coverage.4,5
Worldwide, families suffer excessive financial hardship while receiving health care services because of direct payments. 5 The World Health Organization (WHO) recommends that direct payments should be less than 15%–20% of total health expenditure, as this helps to reduce the incidence of financial catastrophe shock to negligible levels.5,6 Low-income countries face a catastrophic financial burden due to out-of-pocket payments (OPP), which account for 30%–85% of the total health care expenditure.7,8 In African countries, more than 40% of their total health expenditure was constituted by OPP,5,9,10 and in Ethiopia, 34% of health expenditure is generated from households. 11
In developing countries, including Ethiopia, where public health care suffers from poor management, service quality, and weak finances, the development of health insurance improves access to quality health care services and public health care, protects households from health-related financial risks, and ultimately, improves the health status of the poor.12–14 The lack of health insurance leads to delays in seeking care and noncompliance with the treatment regime. The WHO recommends compulsory health insurance as the best form of health care financing even though many factors affect clients’ participation.5,11,15,16
Health care financing in Ethiopia is mainly characterized by low government spending, strong reliance on OPP expenditure, inefficient and inequitable utilization of resources, and poorly harmonized and unpredictable donor funding.4,17 Although different health care financing reforms, such as revising user fees, revenue retention, outsourcing of nonclinical services, exemptions, and fee waivers, have been performed, health care financing is still a major problem in health care delivery systems. 18 Studies have shown that factors that affect willingness to pay for CBHI include but are not limited to sociodemographic, health care, perception, and knowledge of CBHI.19–22
Since the beginning of the CBH scheme in Ethiopia, although the scheme provides package benefits of all available services in the health centers and hospitals on basic health services, there has been low enrollment and a wide discrepancy in willingness to pay for the CBHI scheme.4,12,20,22–27 Moreover, there are inconsistent findings and a lack of nationally representative data on willingness to pay CBHI. Hence, this systematic review and meta-analysis aimed to estimate the pooled prevalence and identify associated factors of willingness to pay CBHI in Ethiopia.
Objectives
To estimate the pooled prevalence of willingness to pay CBHI in Ethiopia.
To identify associated factors affecting willingness to pay CBHI in Ethiopia.
Methods
Study protocol and registration
The Preferred Reporting Items for Systematic Review and Meta-analyses guidelines 28 were used to prepare the systematic review and the meta-analysis. The PRISMA-P 2015 checklist was used for the review report. 29 The protocol of this systematic review and meta-analysis was registered on PROSPERO registration number CRD42022325192.
Search strategies
Systematic reviews and meta-analyses, including registered protocols, were retrieved to avoid redundancy of studies. The PRISMA-P 2009 checklist was used to report the process of search strategies (PRISMA-P 2009 checklist) 30 . Published and unpublished articles were searched in the PubMed/Medline, CINAHL, African Journals Online, and Google Scholar databases from December 15 to May 17, 2022. The MeSH terms and entry terms were searched using the Boolean operator (OR, AND) string (Additional file 1). In addition, reference lists of included studies were retrieved.
Eligibility criteria
Studies performed in Ethiopia, all published studies, studies that reported the prevalence of willingness to pay CBHI and its associated factors, studies that only reported the prevalence of willingness to pay CBHI, only quantitative results for studies that reported both quantitative and qualitative results, all observational study designs (cross-sectional, case-control, and cohort study design), articles published in English, and studies conducted since 2010 were included, as this was the period the government of Ethiopia launched CBHI. 6 Articles published other than English, studies that did not report specific outcomes for willingness to pay CBHI, articles with no full text, studies with incomplete data and no response after email contact with the corresponding author, case reports, conference reports, reviews, and letters were excluded from the study.
CoCoPop/PEO
Co-Condition: willingness to pay for CBHI
Co-Context: Ethiopia
Pop Population: Households
E-Exposure of interest: exposure is an associated factor that increases or decreases the likelihood of willingness to pay CBHI in Ethiopia. The associated factors can be but are not limited to educational status, age, wealth quantile, knowledge, health status, history of illness, chronic disease, and perceived health status.
O-Outcome/condition: The primary outcome of the study was the pooled prevalence of willingness to pay for CBHI in Ethiopia. The willingness to pay for the CBHI scheme was defined as whether the participants were willing to pay the maximum (nonzero) amount that households were willing to pay for the insurance scheme in the primary study (yes, no). The secondary outcome of the study was to identify associated factors of willingness to pay for CBHI. The associated factors for willingness to pay for CBHI were defined based on whether the factor reported in more than one primary study was a significant factor and based on a similar classification in the primary studies.
Study selection
Two independent reviewers (E.W. and O.A.) screened the retrieved articles, and duplicate articles were removed. Assessment of articles using their title and abstract was performed, and irrelevant titles and abstracts were removed. A full-text review of relevant manuscripts was performed before the inclusion of articles in the final meta-analysis for eligibility based on inclusion and exclusion criteria. Endnote reference manager software 31 was used to collect and remove duplicate, irrelevant titles, and abstracts. The selection of article procedures was prepared using a PRISMA diagram.
Quality assessment
The Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument tool was used to critically appraise the quality of the studies 32 (Additional file 2). The components of quality assessment are whether the primary study has clear inclusion criteria, study participants and setting, standard measurement criteria, outcome and exposure measurements, and proper statistical analysis used. The two reviewers (E.W. and O.A.) independently assessed the quality of the studies, and studies with quality scores of 50% and above were included in the final systematic review and meta-analysis. During the critical appraisal of the studies, any disagreement among authors was resolved with the discussion.
Data extraction
Data were extracted independently by two authors (E.W. and O.A.) using a pilot test data extraction Excel sheet. The data extraction sheet components included the authors’ names, publication year, region, study design, study setting, sample size, response rate, and study subjects. Any disagreement was resolved by discussion. In the case of incomplete data, email contact was made with the corresponding author, and the study was excluded if there were no responses.
Statistical analysis
The final included studies were imported to STATA version 14 for analysis. Moreover, the event and control data for associated factors were extracted to RevMan software for analysis. A narrative description of the included studies was performed, and summary characteristics of the included studies were described in tables and graphs. Since heterogeneity in the meta-analysis was due to geographical and methodological differences between the studies and the assumption that a true effect varies from study to study, random-effects model meta-analysis was used to estimate the true effect at a 95% confidence interval (CI). 33 The results were presented using a forest plot with the respective prevalence, odds ratio (OR), and 95% CIs.
Heterogeneity among the included studies was assessed by the I2 statistic. 34 I2 statistics of 25%, 50%, and 75% indicated low, moderate, and increased levels of heterogeneity, respectively, with p < 0.05. The I2 statistic estimates the percentage of total variations among studies that are due to actual differences between studies rather than chance. The possible differences in heterogeneity between the studies were addressed by subgroup analysis based on region, study area (rural/urban), and meta-regression based on region, study area (rural/urban), and sample size. 35
Results
Study selection
A total of 190 studies were retrieved through an electronic database search. Articles were screened using their titles, abstracts, and full-text review. Forty-six duplicated articles were removed. One hundred twenty-nine irrelevant titles and abstracts were excluded for not related to the topic, not conducted in Ethiopia, duplication, and abstract. Fifteen full-text articles were assessed for eligibility, and 10 articles were excluded for not being related to the outcome variable. Moreover, one article was identified from a cross-references search of the included studies. 36 Finally, six studies were included in the final meta-analysis (Figure 1).

Flow chart of study selection for meta-analysis of willingness to pay community-based health insurance in Ethiopia, 2022.
Quality appraisal
All included studies met four out of eight (50% and above) JBI critical appraisals. In four studies, the criteria for inclusion were clearly defined. Strategies to address confounding factors and appropriate statistics were made in all included studies. However, since all the included studies were cross-sectional studies, the identification of confounding factors was not applicable to this study (Table 1).
Quality appraisal of included studies based on Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI) critical appraisal tool.
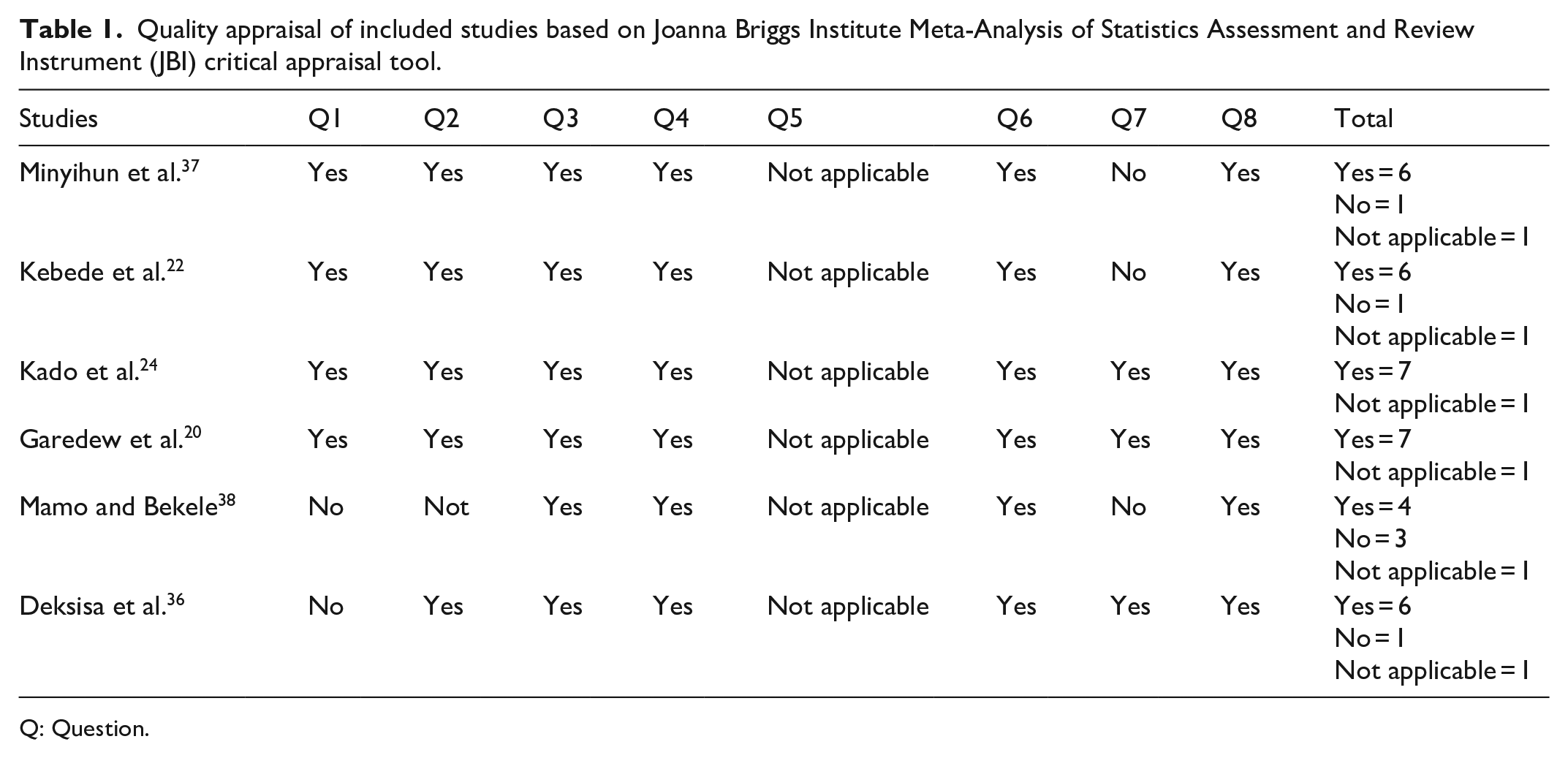
Q: Question.
Characteristics of included studies
In this systematic review and meta-analysis, six studies were included. The studies were published from 2014 to 2020 in different regions of Ethiopia. All studies used a cross-sectional study design. Approximately 3111 participants were included in the study. The sample size of the included studies ranged from 389 to 830 in the Oromia region.20,36 Of the six articles, three studies were performed in the Oromia region,20, 24 ,36, and three studies were performed in the Amhara region.22,37,38 Moreover, five studies performed logistic regression analysis to identify factors associated with willingness to pay for CBHI (Table 2).
Characteristics of included studies in the meta-analysis of willingness to pay community-based health insurance in Ethiopia, 2022.

AOR: adjusted odds ratio; CBHI: community-based health insurance; CI: confidence interval.
The pooled prevalence of willingness to pay for CBHI in Ethiopia
The pooled prevalence of willingness to pay for CBHI was 78% (95% CI, 74, 81), with significant heterogeneity between studies (I2 = 81.74%, p ⩽ 0.001). The proportion ranged from 70% (95% CI: 66, 75) 20 to 83% (95% CI: 80, 85) 36 in the Oromia region. Studies with the largest weight ranged from 18.54 36 to 15.19 20 in the Oromia region (Figure 2).

Forest plot showing the pooled prevalence of willingness to pay community-based health insurance in Ethiopia.
Subgroup analysis
Subgroup analysis was performed based on the region and study setting (rural/urban) to identify the possible source of heterogeneity across the studies. Subgroup analysis based on the study setting showed that rural-based studies had moderate heterogeneity (I2 = 69.81%). A subgroup analysis by region indicated the lowest proportion of willingness to pay CBHI in the Oromia region, 76% (95%, CI: 68, 84), and the highest in the Amhara region, 79% (95%, CI: 77, 81) (Table 3).
Subgroup analysis for the prevalence of willingness to pay community-based health insurance in Ethiopia.
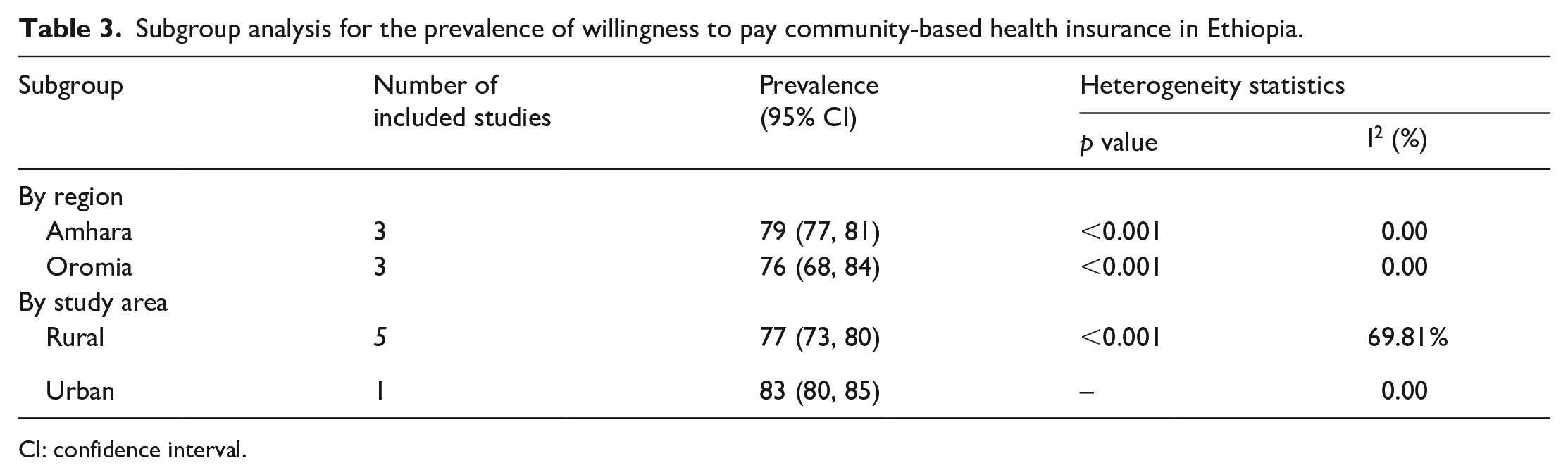
CI: confidence interval.
Meta-regression
Meta-regression was performed by considering both continuous and categorical variables, such as region, study area (rural/urban), and sample size, to identify the possible source of heterogeneity among studies. Meta-regression indicated that the pooled prevalence of willingness to pay for CBHI was not associated with the region, study area (rural/urban), or sample size due to the presence of heterogeneity (p > 0.05) (Additional file 3, Supplemental Table S1).
Factors associated with willingness paying CBHI in Ethiopia
The pooled OR that affects willingness to pay for CBHI was reported in different studies. Although educational status (Figure 3) and wealth index (Figure 4) were repeatedly reported in two studies as significant factors for CBHI,36,24 the variables were not statistically significant in this study.

Forest plot showing the association between educational status and willingness to pay community-based health insurance in Ethiopia.

Forest plot showing the association between wealth index and willingness to pay community-based health insurance in Ethiopia.
Discussion
This systematic review and meta-analysis aimed to assess the pooled prevalence of willingness to pay for CBHI and its associated factors in Ethiopia. There are inconsistent findings on willingness to pay for CBHI in different regions of Ethiopia. Moreover, there are no systematic review and meta-analysis research findings on the pooled prevalence of willingness to pay for CBHI and associated factors in Ethiopia. Therefore, the findings from this systematic review and meta-analysis will help policy-makers design appropriate strategies to enhance willingness to pay for CBHI in Ethiopia.
In this study, the pooled prevalence of willingness to pay CBHI was 78% (95% CI: 74, 81). This finding was in line with studies conducted in East and West Africa, 78.8%, 39 and Nigeria, 81%. 40 This finding was higher than those of studies performed in Nigeria (13.1%), 40 St. Vincent and Grenadines, 72.3%, 41 and Sudan, 68%. 42 However, the finding was lower than that of Bangladesh (86.7%) 43 and Nigeria (86.3%).44,45 The difference might be due to differences in the study period, study setting, sociodemographic factors, health services accessibility, and quality.
In the meta-analysis, the pooled OR of factors affecting willingness to pay for CBHI was analyzed for two variables (educational status and wealth index), which were repeatedly reported as significant factors in more than one primary study. The pooled ORs of willingness to pay for CBHI among households who had education and a high wealth index were statistically insignificant, with ORs (OR = 1.94, 95% CI: 0.9, 4.04) and (OR = 1.08, 95% CI: 0.18, 6.34), respectively. However, a qualitative review of the primary studies showed that there were significant factors affecting willingness to pay CBHI, including attending formal education, history of illness, household size, awareness about the scheme, wealth status or higher income, merchant household, good knowledge about CBHI, access to public health facilities, older age groups, and participation in indigenous community insurance or social networks.20,22,24,36,37 This study might have limitations in terms of heterogeneity. Only articles published in the English language and only cross-sectional studies were included, and we cannot conclude the temporal relationship. Moreover, this meta-analysis represented only studies reported from two regions of the country, and it may lack national representativeness.
Conclusion
Nearly three in four households are willing to pay for CBHI in Ethiopia. Thus, awareness of willingness to pay community-based health insurance is mandatory to improve the implementation of community-based health insurance.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221135876 – Supplemental material for Willingness to pay for community-based health insurance and associated factors in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121221135876 for Willingness to pay for community-based health insurance and associated factors in Ethiopia: A systematic review and meta-analysis by Etsay Woldu Anbesu, Oumer Abdulkadir Ebrahim and Nigus Desalegn Takele in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221135876 – Supplemental material for Willingness to pay for community-based health insurance and associated factors in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121221135876 for Willingness to pay for community-based health insurance and associated factors in Ethiopia: A systematic review and meta-analysis by Etsay Woldu Anbesu, Oumer Abdulkadir Ebrahim and Nigus Desalegn Takele in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121221135876 – Supplemental material for Willingness to pay for community-based health insurance and associated factors in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-3-smo-10.1177_20503121221135876 for Willingness to pay for community-based health insurance and associated factors in Ethiopia: A systematic review and meta-analysis by Etsay Woldu Anbesu, Oumer Abdulkadir Ebrahim and Nigus Desalegn Takele in SAGE Open Medicine
Footnotes
Acknowledgements
The authors show their gratitude to Samara University for the HINARY database website and network access.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.