
Abstract
The purpose of this research is to assess the neuropsychomotor development (NPMD) of 6- to 18-month-old infants and identify factors that may pose a risk to their development. They underwent NPMD assessments, while the parents/guardians were interviewed through the other instruments. Altogether, 64 infants participated in this research. The results revealed infants with questionable NPMD: 29.7% verified with AIMS and 32.8%, with Denver II. There were significant associations between NPMD and maternal low educational attainment (P = .032); family low socioeconomic status and NPMD (P = .026), verified with AIMS and Denver II (P = .037); stimulation opportunities at home and maternal low educational attainment (P = .00026), socioeconomic status (P = .035), and NPMD, verified with AIMS (P = .02) and Denver II (P = .009). The following were identified as risk factors for NPMD: maternal low educational attainment (the lower her attainment, the more likely for the NPMD to be questionable) and family socioeconomic status (infants from disadvantaged homes tend to have questionable NPMD). Stimulation opportunities at home were also significantly associated with NPMD—that is, insufficient stimulations at home may lead to questionable NPMD.
Background
Brazil is a developing country, whose infants up to 2 years old may be exposed to internal and external risk factors. These circumstances can affect their neuropsychomotor development (NPMD), with consequences to their quality of life. 1
Given the great advances in child development, early childhood, which extends from 0 to 6 years old, has a fundamental role in NPMD. 2 In this phase of life, neuroplasticity—the neuronal adaptation capacity according to individual needs due to various stimuli 3 —is more intense. It is characterized by integrated body growth, neuronal maturity, and motor behaviors and skills acquisition. 2 Thus, the earlier the stimulations begin (with movements and/or positioning, as motor strategies following the infant’s age group), the greater the benefit from this neural adaptation capacity as a means to protect them, and the less likely their NPMD will be at risk and/or delayed. 4
According to the context in which the child lives, acquired skills change and improve with time by interacting with their environment and everyday tasks.5,6 Hence, the environment where a child lives—for example, their home, school, and community—has a fundamental role in their development. 6
The family environment can provide stimulation to shape infant development. 7 Not only quantity, but also quality opportunities for stimulation, including a variety of toys, spaces inside and outside the home, different soil textures and levels, and interaction with parents.
Environmental risks, directly related to the child’s family environment, can reveal the parents’/guardians’ neglectful care for the child, precarious health care possibilities, lack of social and educational resources or uninterest in providing them, and so forth. These are oftentimes related to socioeconomic frailty and other conditions and can affect the child’s development. Hence, various studies have addressed the impact of educational, psychosocial, socioeconomic, and environmental factors on NPMD in different contexts. 8
In this regard, nursery schools and day care centers are relevant places to develop studies. Infants and children spend a long time in these institutions, due to the inclusion and expansion of women’s share in the job market.9,10 This has evidently brought about both negative and positive influences on child development scores.11-13
Infants at risk of NPMD delay due to environmental aspects and potential family, educational, and/or socioeconomic disadvantage should be identified as early as possible to avoid impairments in their quality of life—as long as early intervention programs are carried out after the risk has been identified. Early stimulation with child-and-family-centered therapeutic intervention aims to improve their functional health condition as part of the NPMD. It approaches the child’s functions, structures, activities, and participation, considering the environmental and personal contexts from the biopsychosocial perspective of health. As a result, children and their families are adequately inserted in the community.14,15
Hence, this study aimed to assess the NPMD of 6- to 18-month-old infants attending nursery schools/day care centers and identify factors that might pose a risk to their NPMD, due to personal, socioeconomic, and environmental issues.
Methods
This observational, cross-sectional research 16 with a convenience sample was conducted in partnership with the Municipal Department of Child Education of Curitiba, Paraná, Brazil, and was approved by the Research Ethics Committee of the Federal University of Paraná, under CAAE no. 57193516.6.0000.0102 and evaluation report no. 1.714.810.
Altogether, 9 nursery schools/day care centers participated in this research. The participants were recruited through announcements in these educational institutions, with leaflets that explained the research objectives and procedures. The children whose parents/guardians permitted by signing an informed consent form (ICF) participated in the research.
The criteria for inclusion in the study were infants 6 to 18 months old, enrolled in a nursery school/day care center, and whose parents/guardians authorized through an ICF and were available to answer the questionnaires. Infants with any type of syndrome that interfered with the NPMD, congenital malformations, a fever and/or infectious disease during the time of assessment, previously diagnosed hearing or visual impairments, or physical disability were excluded from the research, as well as those whose parents/guardians did not attend the interview after 2 attempts to schedule it.
The infants’ NPMD assessments took place in their classrooms after they got acquainted with the physical therapist/researchers to ensure the ecological validity of the study. 17 The parents/guardians were likewise interviewed at the nursery school/day care center where the infant was enrolled, in previously scheduled 40-minute sessions, on average.
The reliability of the 2 researchers was analyzed. Both were physical therapists trained and experienced in the use of infant assessment scales. The inter-assessor reliability for the Alberta Infant Motor Scale (AIMS) was analyzed with the intraclass correlation coefficient (ICC), whose score was higher than .90—that is, excellent reliability. 18 For the Denver II screening test, the kappa coefficient was used, whose score was 0.792—a sufficiently good inter-assessor reliability. 19 These results were enough to allow 2 researchers to perform the tests with the infants.
Instruments were used to assess the infants’ NPMD, as well as other tools to collect information about the environment where they lived. These instruments and their respective purpose are described in detail in Table 1. Two classifications were used for AIMS and Denver II: Typical (for infants whose NPMD was expected for their age) and questionable (for infants whose NPMD was at risk or delayed).
Instruments used in the research and their respective purpose.

Abbreviations: NPMD, neuropsychomotor development.
All instruments used in this research have been validated for the Brazilian population and/or translated into Portuguese.
Analysis strategy
In the statistical analysis, the Shapiro-Wilk test was used for the normality of data. To assess the association between the NPMD scales and the other qualitative variables, the chi-square test was used, or the Fisher’s test, when the sample was too small. The Mann-Whitney test assessed associations involving dichotomous categorical variables (AIMS or Denver II) and quantitative variables. The Kruskal-Wallis test was used to assess associations involving AHEMD-IS categorical variables and the quantitative variables. 24
Results
The final sample comprised 64 infants, of whom 51.56% (33) were males. Their age ranged from 6 to 18 months, with a mean age of 13 months, and a standard deviation of 3.41; most of them (21.9%) were 15 to 16 months old. At the time of the research, the day care centers admitted infants from 6 months old, who remained there for the whole day (about 40 hours a week, 8 hours a day).
NPMD classification
The typical and questionable NPMD classifications, according to the development assessment scales, are given in Table 2.
NPMD classification of the infants that participated in this research.
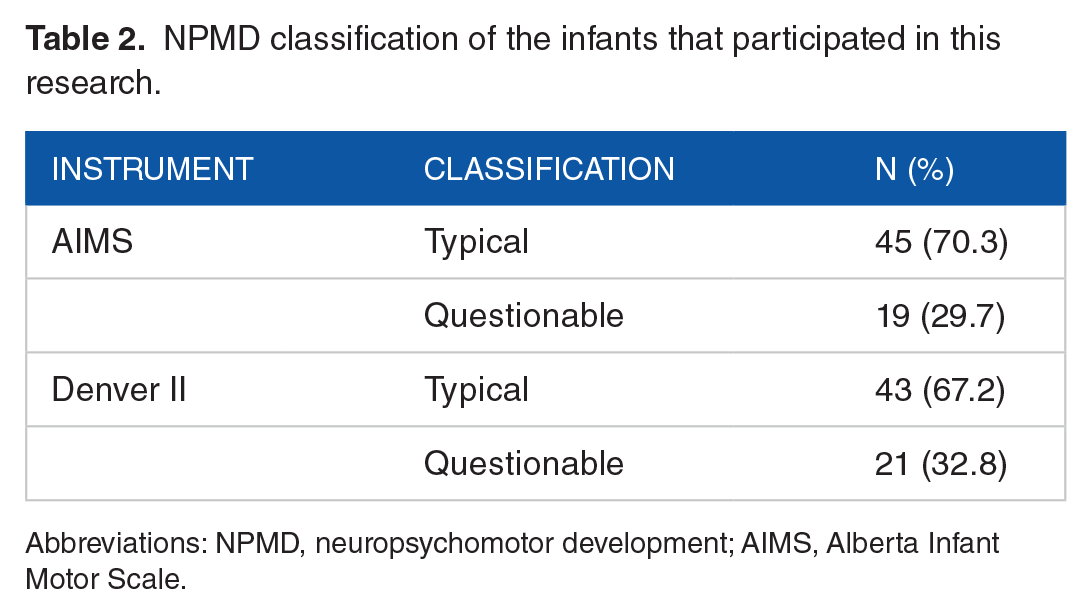
Abbreviations: NPMD, neuropsychomotor development; AIMS, Alberta Infant Motor Scale.
Family socioeconomic classification
Concerning the family socioeconomic classification, assessed with the ABEP questionnaire (Brazilian Association of Research Companies), 32.8% of the families were classified as B2, whereas 9.3% were classified as D-E, whose income is up to R$ 639.78. The general classification of the families is shown in Table 3.
General classification of the socioeconomic status of the participating families, according to the ABEP.

Abbreviations: A1, family income of up to R$ 20 272.65; B1, family income of up to R$ 8695.88; B2, family income of up to R$ 4427.36; C1, family income of up to R$ 2409.01; C2, family income of up to R$ 1446.24; D-E, family income of up to R$ 639.78.
Affordances in the home environment for motor development
The participating infants’ general classification according to AHEMD-IS is shown in Table 4. The stimulation opportunities at home, assessed with AHEMD-IS, were considered moderately adequate for 20.3% and less than adequate for 4.6% of them.
General classification of infant stimulation opportunities at home.
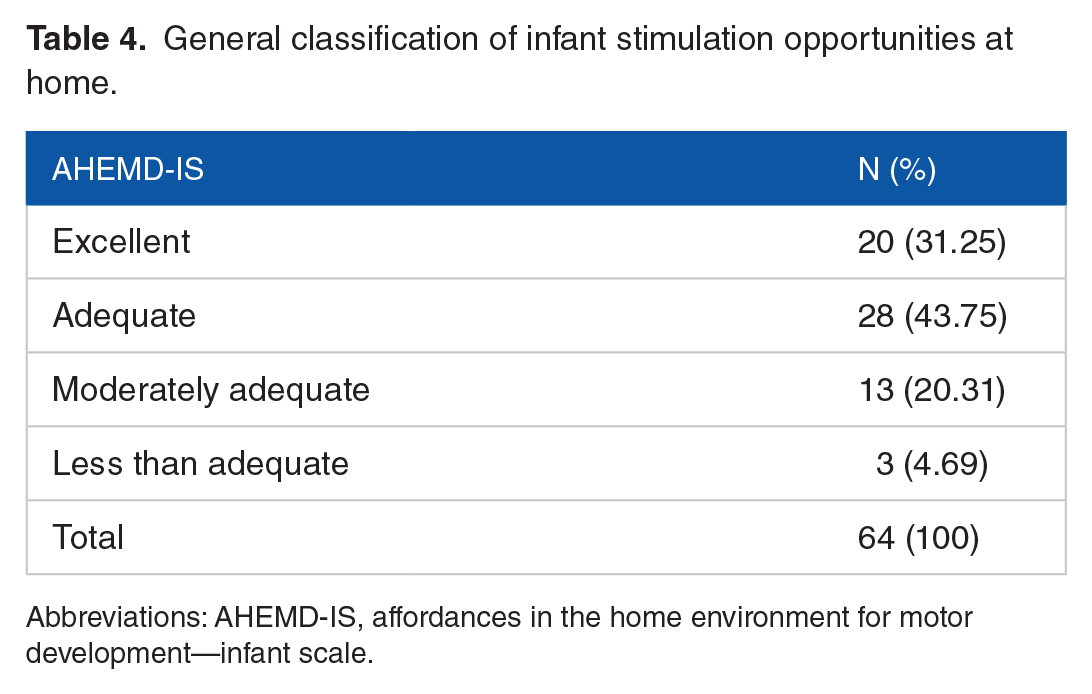
Abbreviations: AHEMD-IS, affordances in the home environment for motor development—infant scale.
Associations between NPMD and personal, family, and environmental factors
The results of the infants’ NPMD assessments were associated with personal, family, and environmental factors, namely: the parents’/guardians’ educational attainment, family socioeconomic status, and stimulation opportunities at home. Significant associations verified with the assessment instruments are briefly described in Table 5.
Significant association results between the instruments.

Abbreviations: NPMD, neuropsychomotor development; AIMS, Alberta Infant Motor Scale; AHEMD-IS, affordances in the home environment for motor development—infant scale.
Maternal educational attainment may be significantly associated with NPMD (P = .032)—that is, the lower her attainment, the less adequate the infant’s NPMD route might be, according to AIMS. The family socioeconomic status is also significantly associated with the NPMD, as verified with AIMS (P = .026) and Denver II (P = .037). Infants classified with questionable NPMD are more recurrent in low-income families.
Regarding environmental factors, AHEMD-IS analysis suggests that maternal educational attainment can also be significantly associated (P = .00026) with stimulation opportunities at home. Infant stimulation seems to be significantly related to the family socioeconomic status as well, as infants with fewer stimulation opportunities come from families in poorer conditions (P = .035).
Lastly, NPMD was associated with stimulation opportunities at home, with significant results between AHEMD-IS and the development assessment scales, AIMS (P = .02), and Denver II (P = .009).
Discussion
The results reveal that 29.7% and 32.8% of the infants in the sample had a questionable NPMD, according to the AIMS and Denver II scales, respectively. Similar results can be found in the studies by Zago et al 25 (33.33%); Araujo et al 26 (31.2%); Silva and Halpern 1 (35%); Araujo et al 15 (42%); and Mélo et al 9 (37%-59%). The numbers reported by these authors may be explained by neonatal complications, parental acceptance of infants, birth weight, inadequate feeding, and social disadvantages. Another issue that may interfere with these NPMD risk rates is the lack of screening and early stimulation, which can cause future learning difficulties for the infant, as suggested by Araujo et al. 15
This high frequency of infants with questionable NPMD endorses the need to screen and assess children that attend day care centers, with the potential for early actions as a means of optimizing the window of neuroplasticity opportunities. 9
Regarding the associations of NPMD with environmental and economic issues, the results suggest that maternal educational attainment can interfere with the course of the infants’ NPMD—that is, the lower her attainment, the greater the incidence of moderately adequate and less than adequate stimulation at home. Studies conducted over the years show results that agree with the findings in the present research, in that the lower the maternal educational attainment, the higher the risks for NPMD.25,27-31 This outcome can be justified by the possible lack of adequate stimuli to improve the infant’s NPMD, which can be observed in families whose mothers have low educational attainments, among other factors. 27 This fact connects directly with another finding of the research, that mothers with lower educational attainment have offered their infants less stimulation at home.
Another possibility for this association is that mothers with low educational attainment consequently have less access to information on how to care for the child—that is, probably, the higher the maternal educational attainment, the greater the access to information, and consequently the greater the offering of varied stimulation. This is reported in other studies, in which maternal educational attainment was also associated with a questionable NPMD.25,27-31
The family socioeconomic status was also significantly associated with the risk for NPMD and stimulation opportunities at home, just as in other studies.29,32-34 Such finding indicates that everyday activities for the acquisition of motor skills are not much offered due to difficulties in the environment, even some families’ disadvantagedness. In this sense, Guerreiro et al 35 point out indications that greater delays may be proportionately related to greater poverty. Less purchasing power leads to vulnerability in terms of basic health, nutrition, education, and cultural services.25,36 The concern with poverty as a component that gathers various intervening factors, favoring the delay, has already been mentioned by Grantham-McGregor et al 37 in The Lancet. Moreover, it can have an impact on stimulation possibilities (also called affordances) at home, with which significant associations have been identified. Poorer families tend to have more difficulties acquiring toys.7,38
Lastly, concerning the relationship between NPMD and affordances according to AHEMD-IS, a significant association was identified between this scale and Denver II and AIMS. Infants with moderately adequate or less than adequate affordances tend to present a questionable NPMD, as already mentioned in other studies.39-41
The present study makes evident the complex, multifactorial, and biopsychosocial nature of NPMD risk and delay situations in the participating infants’ health conditions. These dimensions are interrelated and interdependent regarding functional aspects involving biological function and structure factors, besides the activities and participation domains, and contextual, personal, and environmental factors. This ratifies the need to assess and follow up on the infant’s NPMD progress throughout their life.
As a limitation of this study, the infants underwent only one assessment. Hence, their motor repertoire may not be completely demonstrated, as suggested. 42 Another limitation was that this study did not assess the quality of the infants’ stimulations at the nursery schools. As they spend most of their time in these institutions, analyzing the stimulation types and quality educators use at school, as well as their training as educators, can indicate whether educational environments pose a risk to development. Another limitation was that no independent parent-child interaction measures were included.
Conclusions
Based on the association analysis, the conclusion is that maternal educational attainment is a risk factor for NPMD—that is, the lower her attainment, the greater the possibility of questionable NPMD. Likewise, the family socioeconomic status, as children from disadvantaged homes tend to have questionable NPMD. Moreover, the stimulation opportunities at home were also significantly associated with NPMD—that is, poor stimulation at home can lead to questionable NPMD. The maternal educational attainment and socioeconomic status in the infant’s family are factors associated with less stimulation at home.
Footnotes
Acknowledgements
Gratitude is extended to all research participants.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was conducted with support from CAPES – Finance Code 001.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Karize Rafaela Mesquita Novakoski, Luize Bueno de Araujo, Tainá Ribas Mélo and Vera Lúcia Israel have made a substancial contribution to the concept and design of the article, acquisition, analysis, interpretation of data for the article.
Research Ethics Committee Identification/Approval Number
Federal University of Paraná, CAAE: 32679520.4.0000.0102; evaluation report: 4.146.615.