
Abstract
Background
The aging population in Korea has driven a surge in demand for elderly care services, leading to significant growth in elderly welfare facilities, particularly Adult Daycare Centers (ADCs). However, despite advancements in care facilities, caregivers continue to face challenges in providing suitable elderly care due to difficulties arising from gaps in the latest information on the elderly and their coping abilities.
Objective
The objective of this study is to develop and evaluate the effectiveness of the elderly care assistant system, which facilitates the sharing of information and knowledge necessary for elderly care among caregivers.
Methods
The ECA system was designed to support knowledge sharing through a knowledge management system based on an ontological knowledge model, with a web-based user interface for improved accessibility. A field trial was conducted at ADC in Seoul from August 17 to September 21, with eight caregivers participating. A mixed-methods approach, involving both surveys and interviews, was employed to gauge the ECA system's effectiveness.
Results
The study found that the use of the ECA was beneficial in promoting knowledge sharing among caregivers. Additionally, caregivers noted the potential benefits of using the ECA in conjunction with family caregivers, who can offer additional information and perspectives on elderly care.
Conclusions
This study presents preliminary evidence of the potential benefits of a care knowledge sharing system among various caregivers in elderly care. Although the elderly care assistant effectively promotes knowledge sharing, more research is needed to fully understand its impact on elderly care outcomes.
Introduction
The aging population has led to an increased demand for elderly care services, including care facilities and caregiver support. In recent years, Korea has experienced significant growth in the care facilities industry, driven by the need to accommodate the aging population and provide adequate support to caregivers. Over the past 5 years (2017–2021), adult daycare centers (ADCs), a type of elderly welfare facility, and their users have exhibited remarkable growth, with an average annual increase exceeding 40% 1 . However, despite the expansion of care facilities, the number of elderly individuals assigned to each caregiver has increased 1 , adding to their care burden. Additionally, even if the elderly use welfare facilities, family caregivers still have a care burden in elderly care2,3. One of the major factors contributing to these difficulties is determining the most appropriate method to meet the care needs of each elderly individual and aligning their behavioral characteristics4,5.
To alleviate the care burden on caregivers, several studies have developed computer-based support systems to improve elderly care for both the elderly and their caregivers6–17. These systems generally address various aspects of care, including the elderly’s information, family communication, memory aids, caregiver support, behavioral solutions, personal health record tracking, and educational interventions. For example, MapHabit, a tablet-based app, offers a customizable visual map that provides step-by-step guidance and connections to family members for individuals with memory loss due to Alzheimer-related disorders 13 . Another system, Tele-STAR, provides customized, real-time educational interventions through video conferences to reduce the emotional burden on family caregivers 14 . Fuller-Tyszkiewicz et al. validated the effectiveness of a self-directed mobile health (mHealth) intervention delivered through a mobile app for reducing stress in informal caregivers 15 .
Studies in the field of elderly care have focused on improving care through the development of intelligent systems that enhance the physical and cognitive abilities of the elderly and reduce the care burden of caregivers. Despite these efforts, the implementation of these systems has been limited to supporting specific user groups, such as family members, volunteers, and community organizations. For example, the mSCS tablet application was designed to streamline the care process for the elderly by affording caregiving staff access to coping plans and daily routines 16 . However, the app was primarily intended for use by caregivers working in long-term care facilities, despite the elderly receiving care from various types of caregiver groups. In real life, the elderly receiving care are often attended to by multiple caregivers from different locations, including family members, volunteers, and community organizations. This can result in information gaps among caregivers, as it is crucial for them to continuously assess and monitor the elderly’s health status to observe any behavioral changes in order to provide personalized care9,18. As a result, there is a need for a plan to effectively share care knowledge, including personal information and coping skills, in order to provide customized care for the elderly19,20. Furthermore, sharing care knowledge has been known to improve care outcomes and decrease care burden and burnout for both family and professional caregivers, as reported in the study by Leng et al. 5 .
In this pilot study, we developed and evaluated the elderly care assistant (ECA) system, which is designed to facilitate the sharing of care knowledge among various types of caregivers for elderly care. We improved our previous ontology-based care knowledge management system, which can generate and share personalized care guides for both family members and care facility staff 21 . Knowledge on daily life care and care schedules was added so that the proposed ECA system can help caregivers in adult daycare centers (ADCs) share information about the elderly and summarize their observations during care. With the ECA, professional caregivers can share their coping methods based on updated information about the elderly with informal caregivers, and each caregiver can update the latest information for others as well, reducing gaps in coping ability and promoting collaboration among all caregivers. Additionally, a web-based application was developed to provide more convenient access to the care knowledge management system through any devices connected to the web. To evaluate the effectiveness of the ECA in supporting elderly care, we conducted a month-long field trial at an ADC in Korea. Caregivers who worked in ADCs used the ECA in field trials for a four-week period, and their experiences were evaluated through a mixed-methods approach, including a survey and interviews. The results of the study were analyzed to determine the impact of facilitated care knowledge sharing on elderly care.
Methods
Elderly care assistant
The ECA system comprises three main components: a web-based user interface, a knowledge management module, and an ontological knowledge model (referred to as the knowledge manager). Figure 1 shows an overview of the ECA and illustrates the flow of care knowledge.

Overview of the flow of care knowledge in the web-based elderly care assistant.
The web-based user interface allows users to input the latest information related to elderly care, including observations of regular activities and incidents such as falls or conflicts. The collected information is stored in the knowledge model and can be accessed by caregivers as needed. Depending on the type of information, the input may be directly stored by the knowledge manager or inferred and stored by the context reasoner and reasoning engine that are included in the knowledge manager (as indicated by the blue arrow in Figure 1). The ECA also provides users with care knowledge through two methods: directly delivering knowledge stored in the knowledge model or inferring the necessary knowledge and providing it to the knowledge manager and the knowledge presentation module (as indicated by the red arrow in Figure 1).
Web-based user interface
The design of the web-based user interface was aimed at improving accessibility for elderly caregivers. The interface was created considering the difficulties posed by small screen sizes and text sizes22,23 and was developed in compliance with the Web Content Accessibility Guidelines 2.0 (WCAG 2.0) 24 to enhance usability for seniors. Figure 2 shows the information architecture and an illustration of the web-based user interface in the ECA. The interface includes several features, such as the “Home” page for easily recording simple daily activities and checking statuses of the elderly, including the care schedule alarm, “Register New Elderly” for registering new patients and inputting personal information for care, “Register Additional Information” for adding care information of existing patients, “Care Knowledge View” for viewing care information of elderly, and “Chatbot Assistant” for asking and receiving information through a chatbot interface.
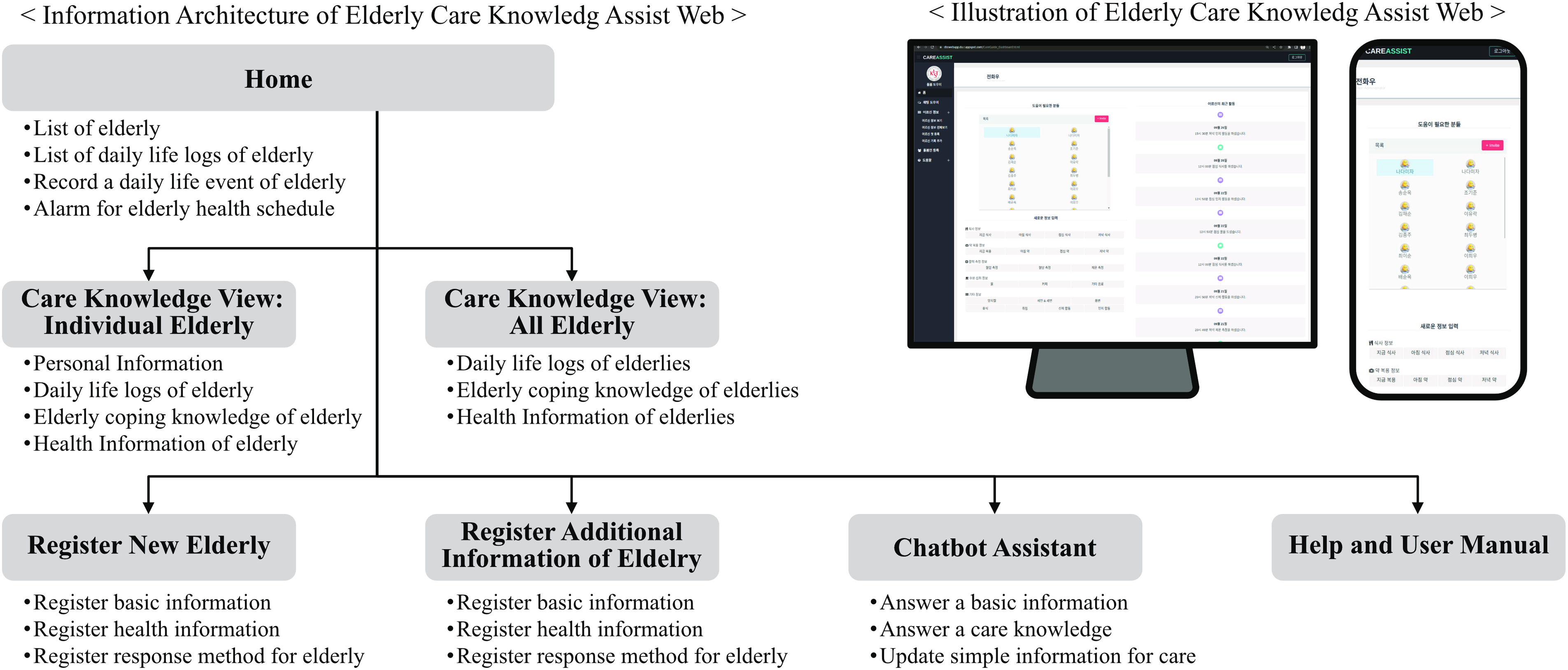
Information architecture and illustration of the web-based user interface in the elderly care assistant.
Knowledge manager
The knowledge manager operates based on the knowledge model and performs three management tasks: inserting and updating care information to the knowledge model, summarizing and inferring care knowledge, and responding to requests from the web-based user interface. The knowledge manager is composed of three primary components: the context reasoner, the reasoning engine, and the chatbot engine. The context reasoner is responsible for handling user requests that are passed to the knowledge manager. The second component is a reasoning engine developed using Prolog, which is a logic language capable of executing reasoning functions assigned by the context reasoner. The chatbot engine manages the knowledge and dialog for chatbots.
Ontological knowledge model
The ontological knowledge model stores and represents care knowledge and information for the care of the elderly, such as personal information, characteristics, and coping methods, in a semantic form. The knowledge model is stored according to the resource description framework for representing directed graphs in the form of semantic triples. Additionally, the knowledge model was extended by incorporating feedback from caregivers regarding their needs for daily life care and care schedule knowledge, such as knowledge of regular meals, sleep, and dressing, based on the previous knowledge model 21 .
Evaluation of the elderly care assistant
In this study, we aimed to evaluate the usability and effectiveness of the ECA system in supporting elderly care among various types of caregivers. To achieve the goal of evaluation, we conducted an pilot field trial in an ADC where older adults are cared for by two distinct caregiver groups: family and institutional caregivers. Additionally, we conducted a survey to understand the effectiveness of the ECA system in an ADC and the expected benefits of using the system with family caregivers from the perspective of the caregiving staff. We adopted a mixed-methods approach, combining both surveys and interviews, to gather data and analyze the actual experiences of ADC caregivers in Korea.
Recruitment and eligibility criteria of participants
The participants were recruited from an ADC in Seoul, Korea (
Study design and procedure
The user study was carried out over a period of five weeks, as shown in Figure 3, with the participation of caregivers who worked in the ADC. The field trial occurred from 17 August 2022 to 21 September 2022, commencing with an orientation session during which researchers introduced the participants to the system, provided instructions for its use, and explained the study purpose. After one week of adaptation to become familiar with the ECA, face-to-face interviews were conducted with all participants to assess their adaptation to the system and to assist them in using the system. The four-week period following adaptation period was the actual experimentation phase, during which the participants actually used the system to care for elderly people in the care facility. Regular communication between participants and the research team was maintained through weekly midterm interviews, with the social worker who gathered user experiences from other participants over a week, and an open chat room led by the researcher. This provided system maintenance support and aided participants in their system utilization. Upon completion of the fifth week of the field trial, all participants were requested to complete an online survey with the goal of evaluating the usability, effectiveness, and anticipated effectiveness of using the system with a family caregiver. Additionally, the participants were requested to participate in a face-to-face interview with the researcher within one week of the end of the field trial.
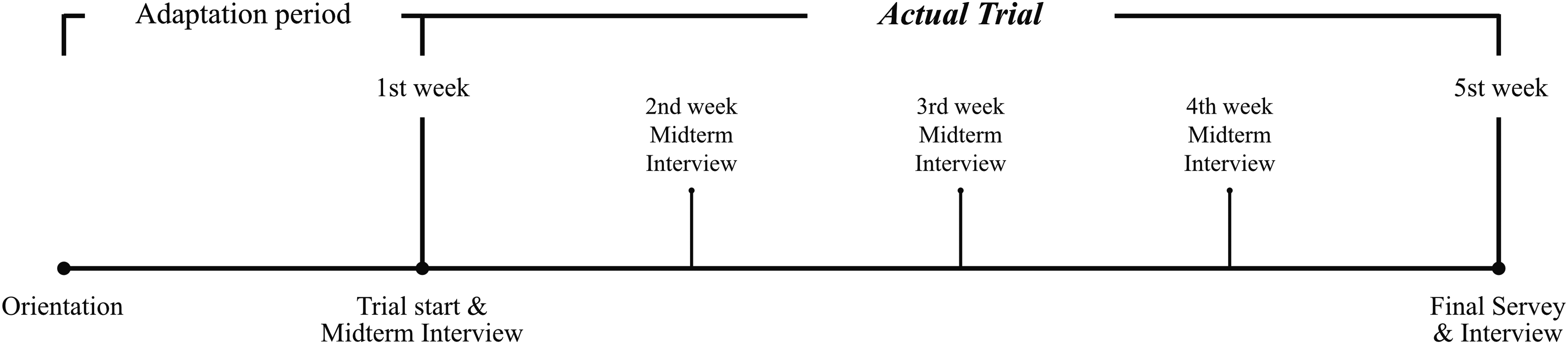
Timeline of the study.
User survey
The survey consisted of multiple questionnaires designed to evaluate the usability and effectiveness of the ECA system in facilitating knowledge sharing among various types of caregivers. The survey was divided into four main areas: usability section, a general assessment section and two knowledge management function sections on partnership and care stress. Examples of survey questions can be found at Supplemental Material.
User version of the mobile application rating scale
We utilized the Korean version of the user version of the mobile application rating scale (uMARS) 25 , which was a translated adaptation to Korean 26 . The uMARS is a tool developed to evaluate the quality of mobile health application in a simpler and more user-friendly way than the original mobile application rating scale (MARS) 27 . MARS was designed for use by trained researchers to determine whether mobile applications meet certain criteria rather than relying on subjective rating systems. The uMARS consists of a 20-item measure that includes four objective quality subscales (engagement, functionality, aesthetics, and information quality) and one subjective quality subscale, as well as a six-item perceived impact subscale. Applications are considered to possess acceptable quality at a score of 3 or above on the uMARS evaluation and to be of high quality if the score was 4 or higher 28 . All questions were answered on a five-point Likert scale ranging from 1 (inadequate) to 5 (excellent). The uMARS 25 has been shown to have good reliability and excellent internal consistency, with high individual alphas for all of its subscales.
General assessment of the ECA
The general assessment section of the survey included two questions that aimed to evaluate the effectiveness of the overall system in promoting elderly care. The first question asked the participants to indicate whether the system had helped care for the elderly, while the second question asked whether the participants believed that using the system with family caregivers could help care for the elderly. Both questions were rated on a five-point scale (1 = very invalid, 2 = invalid, 3 = moderate, 4 = valid, and 5 = very valid).
Knowledge management function: Partnership
The knowledge management function focused on partnership consisted of a questionnaire to evaluate the effectiveness of the knowledge management function in promoting collaboration between staff and family caregivers in elderly care. The questionnaire asked the participants (1) what attributes of partnerships were facilitated when they experienced knowledge management features and (2) what attributes they expected the system to support when used with family caregivers.
Both questions offered the participants an identical set of options, allowing them to select multiple options, or none, for each option. The options were based on constituent attributes of partnership identified in the study by Jang 20 , which investigated the concept of partnerships in elderly care by identifying the constituent attributes of partnership and highlighting the cooperation between caregiving staff and family caregivers. The options included “Shared Responsibility” (the extent to which staff and family caregivers shared the responsibility of caring for the elderly), “Involvement in Care” (the level of involvement of family caregivers in the care process), “Negotiation” (the ability of caregivers to negotiate and resolve conflicts), “Professional Competence” (the level of competence and professionalism of the staff), “Shared Decision-Making” (the extent to which staff and family caregivers made decisions together), “Information Sharing” (the level of information shared between staff and family caregivers), and “Relationship” (the quality of the relationship between staff and family caregivers).
Knowledge management function: Care stress
The knowledge management function focused on care stress consisted of a questionnaire to evaluate the effectiveness of the knowledge management function in reducing care stressors in elderly care. The questionnaire asked the participants (1) what attributes of care stressors were reduced when they experienced the knowledge management function and (2) what attributes they expected the system to support when used with family caregivers.
Both questions offered participants an identical set of options, allowing them to select multiple options, or none, for each option. The options were based on attributes of care stressors identified in the study by Kim 29 , which defined the attributes that comprise such care stressors in elderly care. The attributes of partnership included “Coping Ability” (the ability of caregivers to cope with caring for the elderly), “Communication with Staff” (the quality of communication between staff), “Physical Fatigue” (the level of physical fatigue experienced by caregivers), “Work Confidence” (the level of confidence caregivers had in their caregiving skills), “Relationship between Staff” (the quality of the relationship between staff), and “Caregiving Stress” (the level of stress experienced by caregivers).
Interview
Midterm interview
To concurrently maintain the study and mitigate COVID-19 transmission risk, we established a strategy to collect participant feedback while minimizing direct contact with caregivers. This was particularly necessary for resolving issues encountered during the field trial and promptly incorporating feedback into user experience enhancements. Throughout the field trial, we implemented a protocol of weekly midterm interviews and maintained an open chat room. Midterm interviews were conducted face-to-face with a social worker. During the field trial, the social worker systematically gathered data on participants’ user experiences, including challenges encountered, suggestions for improvements, and desired additional features, through continuous interactions with participants in their care process. The researcher subsequently received these user experiences through midterm interviews with the social worker. The open chat room also served as an online platform for participants to communicate with the researcher whenever needed. Using the data collected from the interviews and chat room, the researcher conducted necessary ECA maintenance and provided additional manuals as required by the participants.
Final interview
The interviews were conducted in a face-to-face setting with the researcher within one week of completing the final survey. The purpose of the interview was to gather specific explanations and examples of participant survey responses, as well as to gather detailed information on areas where the system could be improved (see Supplemental Material for the interview guideline). The questions were divided into two main topics.
The first topic of the interview focused on exploring the overall experiences of the participants with the ECA system. The participants were asked whether they found the system helpful and whether they had any specific examples of how it assisted them. They were also asked about supplementary points for system improvement and specific examples. Additionally, they were asked about the format and language used in the system for adding elderly information and whether it was similar to existing care record documents. Lastly, the participants were asked about supplementary points of the system that could be improved to enhance its efficacy in assisting elderly care when utilizing the system in conjunction with family caregivers.
The second topic was constructed based on survey responses regarding uMARS and knowledge management functions. The participants were asked to provide reasons for their scores on the items with the lowest and highest scores from each of the five uMARS subscales. Additionally, they were asked to explain how the knowledge management function assisted in providing care for the elderly and their expectations of its usefulness when used by family caregivers. This helped to gain a deeper understanding of their perceptions and experiences with the system.
Data analysis
Quantitative analysis
We computed descriptive statistics for items on the uMARS and the user survey (general assessment and knowledge management function). For the uMARS, we calculated the average rating of items within each domain as well as the average rating across domains, and interpreted the results based on the work of Stec et al. 28 . In the general assessment of the ECA, we computed the average score for each question. For the ’knowledge management function’ domain in the effectiveness questionnaire, we counted the total number of participants who selected each item within each domain.
Qualitative analysis
The data collected from interviews, which were guided from interview guidelines (see Supplemental Material for the interview guideline), to gain understanding of the usability and effectiveness of the ECA, were repeatedly analyzed by the researchers. The guideline focused on the participants’ overall experiences with the system and their responses to the user survey. Participants’ responses were documented via voice recordings and handwritten notes. Following this, a process of ’thematic analysis’ was employed, in which the data were initially disassembled into keywords. Patterns or ’themes’ were subsequently identified from these coded data, and then reassembled to enable interpretation and analysis.
Results
Participants’ characteristics
Although recruiting facilities and participants for the field trial was challenging due to COVID-19 prevention measures, eight caregivers employed at a single ADC participated in the study after providing written informed consent. Despite experiencing two postponements in the commencement of the field trial due to facility closures caused by COVID-19, all participants successfully completed the five-week field trial. However, the survey results of one participant were excluded from the survey results due to the lower reliability of their survey responses. As shown in Table 1, the participants’ occupations were as follows: two elderly welfare social workers (25%), four elderly caregivers (50%), and two nurse assistants (25%). The work experience for each job group was as follows: elderly welfare social worker: 6.5 years (standard deviation [SD] = 5.24, range 1–12), elderly caregiver: 6.5 years (SD = 7.77, range 5–13), and nursing assistant: 1.62 years (SD = 1.94, range 0.25–3). A total of eight participants provided written informed consent and was enrolled in the study.
Characteristic of the participants.

Measurement of system usage
During the experimental period, caregivers logged in an average of 9.0 times per day (SD = 6.92) and updated elderly information an average of 57.0 times per day (SD = 37.27). The most frequently used times were 13:00 (30.4%), 15:00 (14.2%), and 20:00 (8.8%). A total of 20 (19 + 1) elderly were included in the study, with 19 registered during the first week of the experiment, and one individual added during the third week. Among the elderly whose information was recorded, two had a diagnosis of dementia, three had diabetes, and one had hypertension.
User survey
uMARS ratings
The mean total uMARS score, with a maximum score of 5, was 3.24 (SD = 0.4), ranging from 2.9 to 4.8 (Table 2). Among the objective quality subscales, information was rated highly, with an average score of 3.61 (SD = 0.20). However, engagement received the lowest score, with a mean of 2.74 (SD = 0.32). Additionally, the scores of all subscales except for engagement were 3 or higher, which is the predefined score for “acceptable quality.” 28
uMARS ratings for the elderly care assistant.

The engagement scores were compiled from five questions on entertainment, interest, customization, interactivity, and the target group. The scores for engagement ranged from 2.4 to 3.2 (mean = 2.74, SD = 0.32). The target group was rated highly within the engagement category (mean = 3.43, SD = 0.49). However, interactivity received the lowest score (mean = 2.0, SD = 0.53). Functionality scores, compiled from four questions on performance, ease of use, navigation, and gestural design, ranged from 2.75 to 4 (mean = 3.39, SD = 0.48). Gestural interactivity scored highly within the functionality category (mean = 3.57, SD = 0.49), while navigation was the lowest-rated category, with a mean score of 3.14 (SD = 0.63). Aesthetics scores, compiled from questions on the app’s layout, graphics, and visual appeal, ranged from 3 to 4 (mean = 3.38, SD = 0.4). The layout (mean = 3.43, SD = 0.49) and visual appeal (mean = 3.43, SD = 0.49) of the app had higher scores compared to the visual appeal score (mean = 3.29, SD = 0.45). Information scores, compiled from four questions on quality of information, quantity of information, visual information, and credibility of source, ranged from 3.5 to 4 (mean = 3.61, SD = 0.2). Credibility of source scored highly within the information category (mean = 4.14, SD = 0.63), while quality of information (mean = 3.14, SD = 34) and quantity of information (mean = 3.14, SD = 63) were the lowest-rated categories. The subjective quality or satisfaction score, which was compiled from questions on recommendation to others, use in the next 12 months, overall star rating, and app cost, ranged from 2.24 to 3.5 (mean = 2.89, SD = 0.22). Overall, star rating to others received the highest score (mean = 3.14, SD = 0.34), while recommendation received the lowest score, with a mean of 2.29 (SD = 0.7).
General assessment of the ECA
In the general assessment section, the effectiveness of the overall system, as experienced by participants during their use of the ECA and as expected by them for use with family caregivers, was evaluated through a survey of seven participants. The responses were analyzed to determine the average overall system effectiveness score, which was three points (SD = 0.57). The anticipated effectiveness score when used with family caregivers was also assessed, resulting in an average score of four points (SD = 0.82). These results are presented in Figure 4.

Evaluation of system effectiveness and expectations assumed when using the system with a family caregiver.
Knowledge management function: Partnership
In a survey assessing the effectiveness of the knowledge management function focused on partnerships, “Information Sharing” (five participants) was the most commonly selected attribute that helped the system to care for the elderly, followed by “Shared Responsibility” and “Professional Competence” (four participants each). A similar pattern was observed when considering use of the ECA with family members, with most participants expecting “Information Sharing” with family (six participants), followed by “Shared Responsibility” and “Professional Competence” (four participants each). These results are presented in Figure 5.
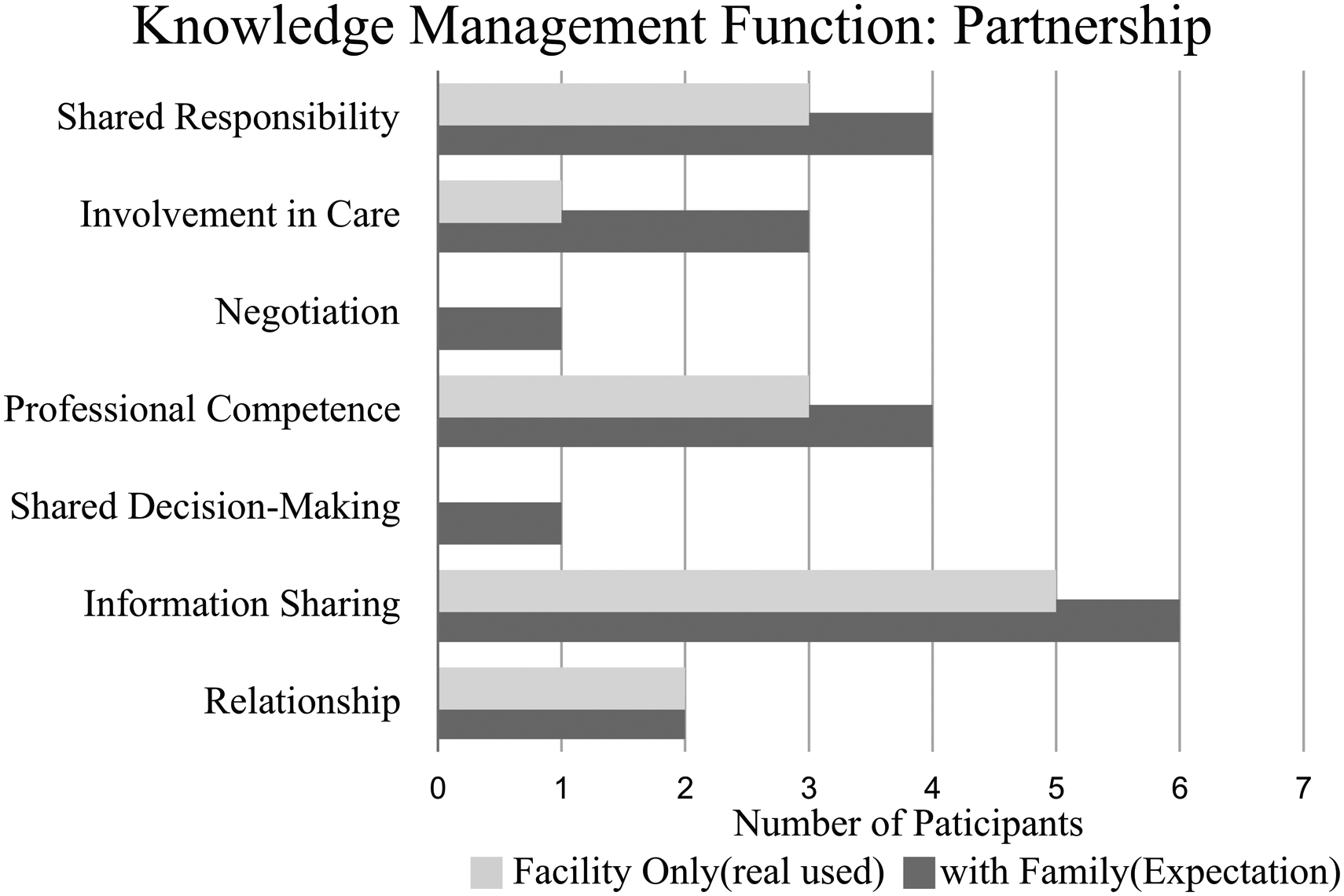
Evaluation of the knowledge sharing effectiveness and expected potential when used with family focused on partnership between staff and family caregiver.
Knowledge management function: Care stress
In a survey assessing the effectiveness of the knowledge management function focused on care stressors, “Coping Ability” (four participants) was the most commonly selected attribute that helped the system to care for the elderly, followed by “Communication among Staff,” “Relationship among Staff,” and “Caregiving Stress” (two participants each). A similar pattern was observed when considering use of the ECA with family members, with most participants expecting improvement of “Coping Ability” (six participants), followed by “Communication among Staff” and “Relationship among Staff” (four participants each). These results are presented in Figure 6.

Evaluation of the knowledge-sharing effectiveness and expected potential when used with family focused on care stress.
Interview and participant feedback
The responses from the final interviews, conducted to gather information on the user experience of ECA systems in actual elder care, included feedback on effectiveness, positive aspects of usability, and improvement points.
Effectiveness
In terms of effectiveness, all participants reported instances in which the system’s knowledge-sharing feature successfully helped provide care to the elderly.
“It was nice to check in advance how the elderly were doing before returning to work after a vacation, instead of having to contact the facility.” “A feature that reminds us of health checks for the elderly and notifies us of missed appointments would be helpful for our work, especially in facilities with a lot of elderly patients.” “Using the system to check the elders’ daily routine allowed me to observe their behavior more closely and to understand them better.” “Sharing details of abnormal behavior, relationship formation, and preferred activities within the center would help in coping with situations outside the facility, and would be significant to identify and refer to the activities of the elderly when not under observation (weekends, evenings, etc.).” “The system is mainly used to enter information on the elderly, but it could be helpful in many situations if used to obtain information as well.”
Additionally, all the participants expressed positive expectations that use of an ECA in collaboration with a family caregiver would provide more support in caring for the elderly compared to solely utilizing the ECA within a facility.
Usability: Positive aspects
In terms of usability, six participants noted that the app was intuitive and easy to follow, citing its layout, large icons, and large fonts as reasons for this. All the participants responded that the terminology used in the system and the terminology used by the center were consistent and that the input format of the elderly response knowledge input format used in the system well contained the contents of the elderly coping manual that was handwritten and used by the center.
“It was easy to spot the elderly care list because it was formatted and neatly arranged with only the necessary information, making it convenient to check the elderly information.” “It was easy to understand because the system used the same terminology and care manual as the center.”
Usability: Improvement point
In the final interview, various opinions, issues, and suggestions for future improvements were expressed. Users cited the difference from the existing method as the main reason for reporting low engagement and subjective quality scores in the evaluation of uMARS. Suggestions for future changes included customizing the list of patients to manage according to user preference and customizing the facility’s care schedule and information addition form. Additionally, it was suggested that the interactivity function for user input be augmented, and that it would be desirable to minimize the page movement for the elderly to enter information because it is cumbersome.
“In the past, only those with abnormal situations contacted the office, but (when we were using the system) it was a lot of work to record all of the elderly’s days that went well and those that did not.”
Last, complaints about the chatbot assistant were also reported. All users responded with low scores on the subjective quality of the system due to negative emotions about the chatbot, inconvenience in using functions, and inaccuracy and reported that the chatbot acted as a deduction factor for the information subscale in uMARS score.
“Chatbots are working, but the process of asking and answering questions via text was cumbersome. And I tried to use it a few times because I sometimes didn’t understand people’s names, but I ended up not using it. I think that the interface was awkward and inconvenient to use. Also, the chatbot responses were not satisfactory or, even if it was valuable, could be obtained more conveniently through other methods.”
Discussion
Principal findings
In this study, we developed the ECA system to facilitate the sharing of care knowledge on elderly care among various types of caregivers. A field trial of pilot use for elderly care at an ADC in Korea validated the usability and effectiveness of the proposed system, with positive feedback on the system’s ability to support caregivers. To our knowledge, this study is the first field trial into the application of an ontology-based care knowledge management system to support care knowledge sharing among various types of caregivers. We next discuss the specific evaluation findings of the ECA system’s effectiveness in elderly care and its anticipated effectiveness when used by family caregivers.
Effectiveness of care knowledge sharing in elderly care
The effectiveness score of the system evaluated in this study was 3.0. The participant evaluation of the ECA system’s knowledge management function reported that “Information Sharing” and “Elderly Coping Ability” were the most valuable attributes supported by the function. During the final interviews related to this function, the participants stated that the system had a positive impact on elderly care and provided specific examples. They reported that the ECA system summarized and shared care knowledge, including information generated from caring for the elderly and information collected through phone calls and family counseling, offering easy access to caregivers. In addition, they reported that the coping ability of the caregiver was improved through the ECA, and information sharing with the family caregivers became easier even though the family did not use the system together in this experiment.
These results indicate that the coping ability of the elderly can be improved through information sharing, which is consistent with previous research that found effective information sharing to be a crucial resource in individualized care for the elderly in care facilities16,19,30.
Anticipated effectiveness using the ECA with family caregiver
The study evaluated the anticipated effectiveness of the ECA system when used with family caregivers. The results showed that the ECA system received a higher score of 4.0 when used with family caregivers compared to a score of 3.0 when used solely in a care facility. The participants in the knowledge management function evaluation reported receiving support for “Information Sharing,” “Shared Responsibility,” and “Professional Competence” regarding partnership for and “Elderly Coping Ability,” “Communication among Staff,” and “Relationship among Staff” regarding care stress. Furthermore, they indicated that these attributes were expected to yield greater benefits when ECA systems were utilized in collaboration with family caregivers compared to using ECA only in care facilities (Figure 5). Notably, they also expected the system to be more effective for “Negotiation” and “Shared Decision-Making” in the partnership questionnaire, which were not answered when used only within the facility.
Moreover, participants concurred that using the ECA with family caregivers would result in more efficient and effective care for the elderly. In the final interview, the frequent input when using the ECA system solely in the ADC was the reason for this perception of the system as an additional workload. The participants expected that involving family caregivers would mitigate this perception because it would provide a more up-to-date perspective on caregiving and increase the need for the ECA system. Additionally, they anticipated that nonexpert family caregivers would gain from the care knowledge provided by care facility personnel, allowing them to respond suitably to related situations.
These results suggest that employing the ECA system with family caregivers will improve elderly care. This finding is consistent with previous research, which highlights the significance of family involvement in elderly care20,31 and the value of family member information and perspectives in understanding the elderly’s life history, habits, preferences, and care needs32,33.
Limitations and future work
There are limitations to this study that should be acknowledged. First, the study found that participants rated their engagement and subjective quality scores as “Poor” 28 using uMARS. During the interviews, the participants identified increased workload as the main reason for their dissatisfaction with the proposed ECA system. To address these limitations, further research needs to update an interface to record simultaneously the elderly’s work and performance while leveraging advancements in action recognition research 34 or tracking devices 35 to automate the recording process. Such an approach will not only streamline the data collection process but also improve the accuracy and efficiency of the recording, which is essential for analyzing the elderly’s daily activities and making informed decisions about their health and well-being. Therefore, it is advisable to focus on incorporating these features into the design of any future interventions or tools that aim to support the elderly in their daily activities.
Second, the study had a limited scope of participants in the evaluation experiments, as it was conducted solely with caregivers who were employed in one certain ADC, which may limit the generalizability of the findings. The ECA was designed to facilitate knowledge sharing among various caregiver groups, including family caregivers. Further study is needed to validate its effectiveness with more sample size in this regard.
Furthermore, studies on technology-driven interventions for caregivers have shown potential benefits, including reduced caregiver burnout, improved quality of life for both the elderly and caregivers, and enhanced care quality6–8. Future studies should investigate the specific outcomes of the ECA system in care facilities, including its impact on caregiver stress, burnout, and job satisfaction, as well as the overall quality of care provided to the elderly.
Conclusions
In this study, we developed and evaluated the ECA, an ontology-based care knowledge management system designed to facilitate care knowledge sharing among various types of caregivers in elderly care. The system includes an ontological knowledge model of elderly care and a knowledge manager that operates it and provides reasoning based on the knowledge model. The system also features a web-based user interface to enhance the accessibility for caregivers. In the field trial, the proposed system demonstrated its potential to reduce gaps in coping ability and information access for the elderly while fostering collaboration among caregivers. Consequently, it is anticipated that the system could alleviate the care burden experienced by caregivers, although this must be validated in a future study.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231200976 - Supplemental material for A web-based care assistant for caregivers of the elderly: Development and pilot study
Supplemental material, sj-docx-1-dhj-10.1177_20552076231200976 for A web-based care assistant for caregivers of the elderly: Development and pilot study by Hwawoo Jeon, Yong Suk Choi and Yoonseob Lim in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231200976 - Supplemental material for A web-based care assistant for caregivers of the elderly: Development and pilot study
Supplemental material, sj-docx-2-dhj-10.1177_20552076231200976 for A web-based care assistant for caregivers of the elderly: Development and pilot study by Hwawoo Jeon, Yong Suk Choi and Yoonseob Lim in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank the caregivers working at the adult day care center of Seongbuk welfare center in Korea for providing valuable feedback on the proposed systems and helping us to improve it.
Contributorship
HJ, YC, and YL conceptualized the study design. HJ and YL developed the system and conducted field trials. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of Institutional Review Board (IRB) at Korea Institution of Science and Technology approved this study (IRB number: KIST-202209-HR-001).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the KIST Institutional Program (2E32282), by the National Research Council of Science & Technology (NST) grant by the Korea government (MSIT) (No. CAP21052-200), by a National Research Foundation of Korea (NRF) and IITP grants funded by the Korean government (Ministry of Science and ICT) (nos. 2018R1A5A7059549, 2020R1A2C1014037, and 2020-0-01373), and by the Government-wide R&D Fund for Infections Disease Research (GFID), funded by the Ministry of the Interior and Safety, Republic of Korea (no. 20014463).
Guarantor
YL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.