
Abstract
Mitigation measures the pandemic caused by the coronavirus disease 2019 (COVID-19) can change neuropsychomotor development (NPMD), diminishing adaptation, learning, and physical and cognitive development skills. Biopsychosocial screening in this scenario requires specific physical therapy assessment for each intervention setting, with validated scales. Hence, the objective of this study was to analyze the consequences of the COVID-19 pandemic on NPMD based on a case series in 4-to-24-month-old children assessed on land and in water. Case series descriptive study, based on physical therapy assessments with the Alberta Infant Motor Scale (AIMS), Developmental Screening Test (Denver II), and Adaptation of the Aquatic Functional Assessment Scale for Babies (AFAS-BABY©). AIMS classified 8 children as typical NPMD and 5 as suspect NPMD, while Denver II classified 10 children as typical NPMD, 3 as questionable NPMD, and 2 as delayed NPMD. AFAS-BABY© created a qualitative profile, relating it to the land assessments. Thus, the consequences of the COVID-19 pandemic on NPMD were analyzed based on a case series in 4-to-24-month-old children assessed on land and in water.
Introduction
The COVID-19 pandemic broke out in 2019, due to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and was declared a public health emergency by the World Health Organization (WHO). 1 It has broad symptomatology that commonly includes fever, fatigue, cough, expectoration, phlegm production, and breathlessness, possibly leading to death. 1 In children, symptoms are usually milder, involving cough, fever, and vomit—although children younger than 1 year require greater attention and prevention because of possible complications and more severe consequences, such as breathing discomfort, decreased oxygen saturation, and persistent high fever, possibly leading to death. 2
Thus, social distancing measures were taken to prevent COVID-19 and reduce virus transmission. Families and especially children suffered a high level of stress caused by such measures. 3 Moreover, the excessive, early, and prolonged use of technologies, along with the fear of contagion, school closure, lack of support networks, and financial difficulties, may negatively interfere with children’s neuropsychomotor development (NPMD).3,4
Consequently, children have been showing behavioral changes—as described by Costa et al, 5 who particularly found consequences such as attachment to caregivers, misbehavior, increased screentime, restlessness, difficulties sleeping, aggressiveness, and sadness. These may have negative consequences on NPMD, such as extrinsic factors that may directly interfere with intrinsic factors of small children’s development. 6 Furthermore, long-term losses probably include reduced adaptation skills, learning, and physical and cognitive development. 7
Lifelong NPMD is a complex process involving intrinsic (genetic and biological) and extrinsic aspects (eating, healthcare, level of stimulation, socialization, and diversified activities), considering settings and tasks.8,9 Typical NPMD is related to the maturation of the central nervous system, encompassing various functional domains, such as broad motor, adaptive fine motor, social, and linguistic ones, 10 besides the family, school, and social activities and settings with which babies interact, which may or may not have levels/diversity of stimulation. 11
The first years in children’s lives are essential to structure a solid basis for their development, as acquiring simple movements may help acquire various more complex skills.8,10 This demonstrates the need for following up on 0-to-2-year-old children to early assess and identify possible NPMD losses, which may lastingly interfere with their health and pose physical/functional risks and/or delays, considering neuropsychomotor domains.8,12
The International Classification of Functioning, Disability, and Health (ICF) is a tool that follows up and classifies human development and currently counts with an extended version for children and youth—thus helping analyze children’s health status and NPMD. 13 The ICF biopsychosocial (BPS) model addresses the domains of body functions (b) and structures (s) and activities and participation (d) (under the functioning indicator) and environmental (e) and personal factors (under NPMD contextual factors).12,14 To use the ICF, physical therapists must make specific assessments aimed at 0-to-24-month-old children, based on which their typical NPMD is adequately screened in aspects of functioning and contexts.
To recognize this new scenario and detect its impacts on NPMD in the assessment process, physical therapists must use good instruments that comprehensively assess and screen individuals according to their singularities, 15 considering the BPS concept of health. Mélo et al 14 point out that the main scales used in Brazil are from other countries; they are validated for the Brazilian population and used in NPMD follow-up of children up to 6 years old.
For instance, the purpose of the Alberta Infant Motor Scale (AIMS), developed by Piper and Darrah in Canada in 1994, 16 is to assess the gross motor function in 0-to-18-month-old full-term and preterm babies. 16 It is observational, low-cost, quick, and easy to apply, which makes it usable by all professionals. 14 Denver II, developed by Frankenburg et al, 17 is another much-used instrument encompassing further areas and ages. It addresses the main areas of development (personal social, adaptive fine motor, gross motor, and language) to assess babies and children up to 6 years old and screen their development.14,18
Hence, both scales have specific items for each age and are divided into domains that assess functioning with functions/structures, activities, and participation, which are present in ICF and pertain to child NPMD as health status and environmental and personal contexts.14,19 Thus, there are validated NPMD assessment and screening instruments approaching land settings. If used in combination, they provide a comprehensive approach from the BPS perspective of health, as indicated by WHO in the ICF. 14
However, NPMD must be assessed not only on land—it must specifically address the medium in which interventions take place. Aquatic physical therapy must include assessments in water—particularly in the case of this study, heated swimming pools. 15 Despite the few specific aquatic assessment scales, 15 using such instruments aimed at children helps explore their motor behaviors and potentialities in liquid environments, complementing BPS land assessments, and helping plan interventions aimed at individual competencies and needs, respecting the peculiarities of the aquatic setting.20,21 Hence, this study used the Adaptation of the Aquatic Functional Assessment Scale for Babies (AFAS-BABY©), 20 which assesses the babies’ various motor behaviors in a heated pool.
Physical therapists can use both land and aquatic assessment data to establish the children’s health status, functioning and context characteristics, and physical therapy objectives, and thus develop and follow up an aquatic physical therapy intervention plan. Such a process in the aquatic setting aims to improve the children’s sensory perception and motor skills, 22 as it is an appropriate environment for the neuro-sensory-motor stimulation centered on children and their families. Thus, it helps motivate and increase child and family adherence to the intervention program with fun activities, counting on the physical and thermal properties of water and therapeutic, functional, creative, and pleasurable activities, preventing risks and delays with early stimulation and active participation of children and families.7,23
Hence, given the few validated aquatic assessment scales and the children’s isolation during the pandemic, the objective of this study was to analyze the consequences of the COVID-19 pandemic on NPMD based on a case series in 4-to-24-month-old children assessed in both land and aquatic settings.
Methodology
This is a case series descriptive study 24 in 4-to-24-month-old children recruited by convenience, aiming to approach at least one sample per trimester.
The research inclusion criteria were as follows: (1) 4-to-24-month-old children; (2) both sexes; (3) mother/father or guardian available to accompany the child; (4) medical certificates for both the parent/guardian and the children, allowing their participation in aquatic activities; (5) parents’/guardian’s signature of an informed consent form; and (6) wearing COVID-19 protection equipment.
The exclusion criteria were as follows: (1) children and/or parents/guardians with symptoms or suspicion of COVID-19; (2) children with infectious and contagious diseases or skin lesions; and (3) atypical children with any clinical NPMD-related diagnosis.
Based on these, the collection began at a private clinic in Curitiba, Brazil. The assessment period was divided into 3 moments: assessments began on land, along with parent/guardian interviews using the socioeconomic questionnaire adapted from Araujo (2013) and signature of an informed consent form and photo consent form. Lastly, the aquatic assessment was made with AFAS-BABY©.
The whole team was instructed to follow the WHO safety protocols, 25 including the use of personal protective equipment, masks, alcohol-based hand sanitizer, and only one companion per child.
The land assessment was made with AIMS, 16 which addresses gross motor skills in 0-to-18-month-old babies with 58 items divided into 4 subscales: prone (21 items), supine (9 items), sitting (12 items), and standing (16 items). 26 This assessment observes the babies’ spontaneous movements in 4 different positions and records the observed and non-observed behaviors. 26 Those observed during assessment make up the “motor window”; each observed item scores 1 point, and those not observed score 0. Each subscale score is the sum of the points obtained by items within the motor window and before the motor window (which also score 1 point, as these are items previously presented by the child). 20
Lastly, subscale results are added and converted into a percentage, classifying NPMD as typical (above 25%), suspect (between 25% and 6%), or delayed (5% or less). 9
Denver II is also used in land NPMD assessment 17 of 0-to-6-year-old children, based on the analysis of 4 main areas: personal social, language, adaptive fine motor, and gross motor. 18 The scale is applied by observing and classifying specific behaviors according to the age group, namely: pass (P), not observed (NO), refused (R), fail (F), caution (C).14,17 Behaviors presented by more than 90% of the other same-age children are classified as “F,” while those presented by 75% to 90% of same-age children are classified as “C.” 14
The final scale classification indicates typical NPMD (children with up to 1 caution), questionable NPMD (1 fail or 2 or more cautions), or suspect of delay (2 or more fails). 14
For the physiotherapeutic intervention to be effective and assertive, it is necessary to use instruments that consider the environment in which the intervention takes place, in this case, the aquatic environment. 15 In this sense, the evaluation instrument AFAS-BABY©, has the ability to consider the peculiarities of the aquatic environment, possibilities and motor behaviors of the body in immersion, relevant to each age. 20 The items observed in the scale obtained favorable validation from expert judges and high relevance. 20
Aquatic physical therapy assessment was made with AFAS-BABY©, which assesses aquatic motor skills in 4-to-24-month-old babies. 20 Altogether, 61 behaviors are scored from 1 to 5 points—1, when the child does not have the behavior; and 5, when they have maximum motor control over it. The maximum final score is 305 points. 20
After applying Denver II, AIMS, and AFAS-BABY©, a qualitative analysis approached the assessment process and each child’s reactions in social interaction with the evaluators and the environment.
Results
Data were described considering sample characterization and land and aquatic assessments, and then associating both assessments.
The results of the medical history questionnaire used to describe the sample are shown in Table 1.
Sample distribution and characterization.

Source: The authors (2022).
AIMS land assessment results are shown in Table 2. Two out of the 15 participating children were older than 18 months and therefore were not assessed with this instrument. Hence, considering 13 children (100%), 38.46% (n = 5) were classified as suspect NPMD and 61.53% (n = 8), as typical NPMD.
AIMS classification of participants up to 18 months old.
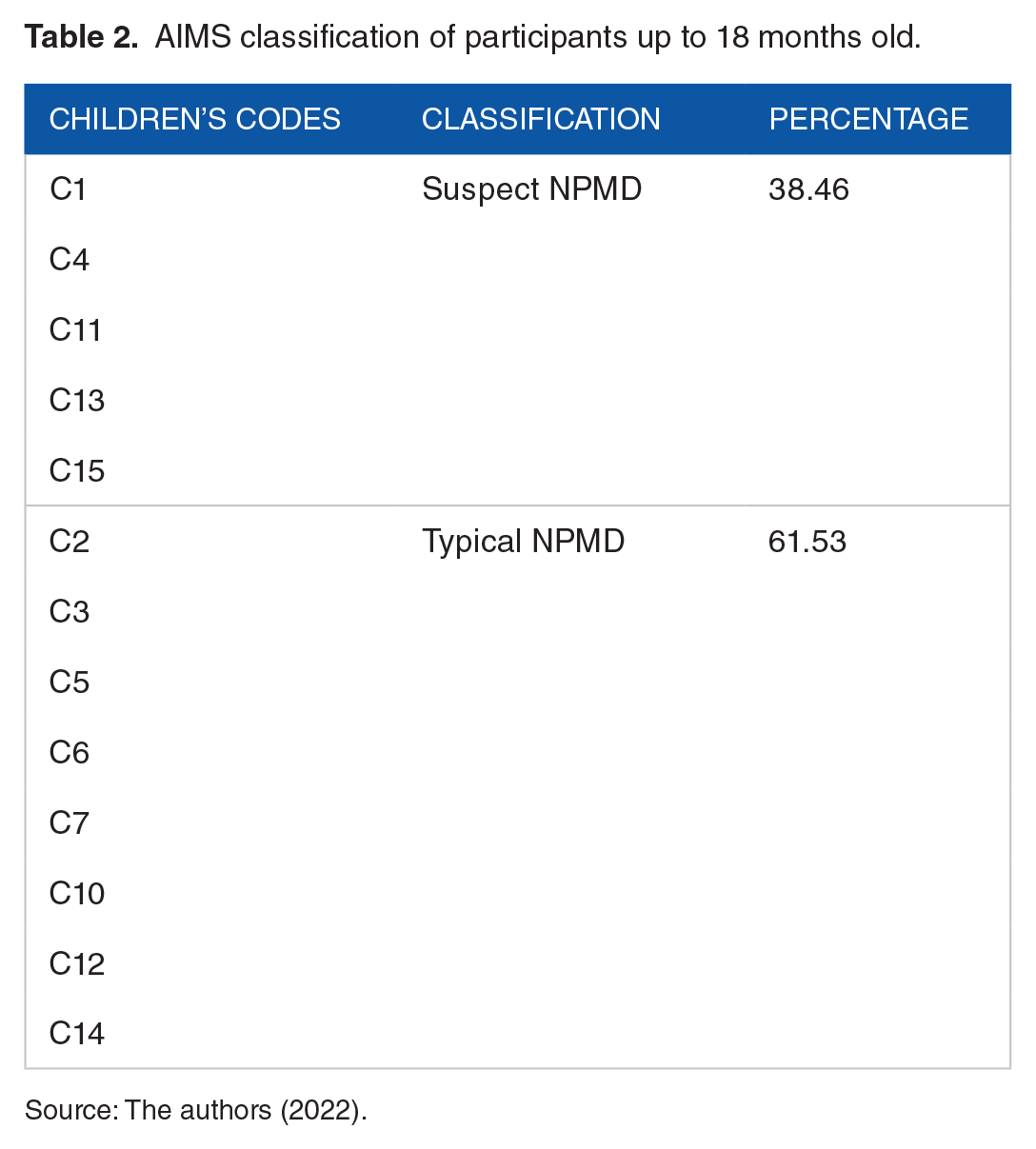
Source: The authors (2022).
Out of the total 15 children (100%), Denver II classified 10 (66%) as typical NPMD, 3 (20%) as questionable development, and 2 (13.33%) as delayed NPMD.
The percentages of the dimensions at greater risk of developmental delay according to Denver II are shown in Figure 1. The adaptive fine motor (40%), personal social (20%), and gross motor dimensions (6.66%) summed up most failures.

Percentage of dimensions with the most fails.
Each child’s final AFAS-BABY© score is shown in Figure 2. C11 and C15 were the children in the sample with the lowest scores. This scale, however, does not have a final NPMD classification.

Each child’s final AFAS-BABY© score.
The sample’s qualitative profile is described in Chart 1. Out of the 5 (100%) children classified by AIMS as suspect NPMD, 4 (80%) presented social interaction difficulties, excessive attachment to parents, and insecureness during the assessment. And, out of the 5 (100%) children classified by Denver II as questionable or delayed NPMD, 4 (80%) had socialization difficulties and did not easily make friends with the evaluators during the assessment. AFAS-BABY© assessment does not have a final classification, but the qualitative profile of the children’s performance varies according to the level of familiarization with the assessment setting. Hence, C12 stood out with the second highest score, though being only 9 months old.
Qualitative land and water profile, considering the 3 assessment instruments.

Discussion
According to Newell et al, 27 NPMD can be understood based on the ecological model, which explains the interaction between individuals, environments, and tasks in different contexts directly involved in the developmental process. 6 Thus, family contexts are pointed out as the main external factor capable of potentializing NPMD because they are the first environment (and perhaps the only 1 during the pandemic) experienced by children. 28
The sample characterization showed that few children attended school full time, which agrees with findings in the literature. Due to the pandemic in Brazil, the Ministry of Education canceled in-person activities in public and private schools. 29 Feitosa et al 30 pointed out the negative consequences of distancing measures in childhood on cognitive, learning, and socialization dimensions, as children need social exchange and interaction.
AIMS results showed a considerable number of children classified as suspect NPMD. This may be due to the COVID-19 contagion prevention measures, such as social distancing, which impairs development, causes stress, increases exposure to technologies, decreases stimuli from parents or caregivers, and diminishes environmental exploration in children. These factors may cause or worsen functional and behavioral difficulties in babies. 31
Moreover, the perception of a threatening event like the COVID-19 pandemic causes stress, changing babies’ physical activity and sleep—which are essential elements to NPMD because they impact brain plasticity. 31 It was observed in the study that most children classified as suspect NPMD had social interaction difficulties, insecureness, and excessive attachment to their parents during the assessment. The study by Jiao et al 32 demonstrates that small children have difficulties reasoning the pandemic scenario, mainly reacting to their parents’ behavioral and daily routine changes. It is therefore natural that babies’ sleep, eating, and behavior be affected, showing distancing, which are ways children find to cope with adverse situations.4,32 However, these changes may impair the children’s learning processes and prevent them from reaching their full NPMD potential.4,32
Denver II findings point to a significant percentage of the sample with questionable or delayed development. The study by Feitosa et al 30 may explain these results, as they comment on the main consequences of the COVID-19 social distancing measures. According to the authors, the cognitive, learning, socialization, and development dimensions require social interaction, strengthened by contexts like schools to which children belong.
Thus, according to Araújo et al, 4 school closure—where child development is extensively encouraged—, increased use of technological devices, and caregivers’ stress may help reduce movement potentialities, environmental exploration, and stimuli. This agrees with the findings in this study, as 33.33% of the sample had delayed or at-risk NPMD.
Most failures were related to the adaptive fine motor (40%), personal social (20%), and gross motor domains (6.66%). Corroborating these findings, Bortagarai et al 33 found greater risk/delay indices in adaptive fine motor and gross motor domains. Moreover, the research by Fauls et al 34 verified that delayed gross motor skills interfere directly with activities and participation and have consequences on socialization and cognitive function.
Zago et al 6 and Muluk et al 35 sought to further the discussion on areas with greater NPMD delay and found a greater prevalence of risks/delays related to language—which disagrees with the findings in the present research, whose sample did not have fails in language. However, according to Basílio et al, 36 stimuli presented by mothers during their time spent together can contribute to language development—which can be explained by the findings of the present research, as most of the sample spent most of their time with their mother.
The 2 children with low AFAS-BABY© scores (C11, 8 months old, and C15, 7 months old) were not familiarized with aquatic environments and had social interaction difficulties. Moreover, their mothers were overprotective, which was reflected in these children’s insecureness. Corroborating with these findings, the study by Wizer et al 21 points out that the greater the aquatic experience and its quality, the greater the aquatic skill achievements in childhood. Hutchon et al 37 also stated that the greater the parents’ involvement and confidence during fun aquatic therapy, the better the children’s NPMD stimulation and social interaction.
The comparison of the 3 scale results—AIMS, Denver II, and AFAS-BABY©—shows 2 children (C11, 8 months old, and C15, 7 months old) with at-risk and/or delayed NPMD according to land assessments and low AFAS-BABY© scores. This demonstrates that AFAS-BABY© agrees with land assessments, complementing such screening. 20 Furthermore, according to Valla et al, 38 children who have developmental difficulties on land are expected to also have difficulties developing motor skills in aquatic settings.
On the other hand, C13 had a high AFAS-BABY© score but was at risk of delay in AIMS and Denver II. In this regard, the study by Araújo et al 20 explains why older children can perform some behaviors in AFAS-BABY© more easily, possibly indicating a different level of physical growth, maturation, and motor learning.
Recognizing NPMD peculiarities during the COVID-19 pandemic, the study by Irwin et al 39 shows that everyday changes may explain the consequences on NPMD. Social distancing, school closure, and economic deficits lead to these children’s decreased emotional well-being, NPMD stimulation, performance, and independence. 39 However, different realities even in similar age groups depend on the impact on the families’ socioeconomic condition, reflecting on the quality of the environment available for children to explore. Hence, corroborating with the present study, COVID-19 influences cases of at-risk and/or delayed NPMD, even though this cannot yet be measured in detail. 39
Conclusion
The main objective of this study was met, as it could analyze the consequences of the COVID-19 pandemic on NPMD, based on a case series in 4-to-24-month-old children assessed on land and in water.
This study helped learn the consequences of COVID-19 prevention measures on children’s NPMD. It will hopefully be useful to other physical therapists responsible for following up on child development, encouraging families to actively participate in the NPMD process, promoting babies’ health, and preventing possible developmental risks and delays.
Nevertheless, future studies should address the possible long-term consequences of COVID-19 on NPMD more in-depth and in further detail, always focusing on physical therapy healthcare centered on children and families, with specific scales and respecting peculiarities of each reality and intervention environment.
Hence, products for the community should be developed, to help instruct families on how to deal with such consequences. Through strategies that help parents and guardians to continue the process of stimulating the child during the pandemic period and, thus, prevent damage to the DNPM. As an example, health education programs that address this topic at home, such as booklets and guidance documents, are produced by professionals responsible for stimulating the child. In addition, providing reliable information to family members about the consequences of COVID-19 mitigation measures on the child’s development is essential, as it is a tool capable of empowering the family through knowledge and promoting family-centered practice.
Footnotes
Acknowledgements
Gratitude is extended to all research participants.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The authors DFL, SFS, BKC, JB and MB, contributed with the theoretical basis, scientific writing, administration and data analysis, production of graphic elements, debates and conclusions of the main ideas of the articles. TRM, LBA and VLI contributed in guiding the follow-up of the project, corrections and feedback throughout the entire process of writing the article.
Number of Identification/Approval From the Research Ethics Committee
Federal University of Paraná (UFPR), CAAE: 57193516.6.0000.0102, evaluation report no. 1.714.810.