
Abstract
The incidence of cirrhosis is rising, and identification of these patients prior to undergoing any surgical procedure is crucial. The preoperative risk stratification using validated scores, such as Child-Turcotte-Pugh (CTP) and Model for End-Stage Liver Disease, perioperative optimization of hemodynamics and metabolic derangements, and postoperative monitoring to minimize the risk of hepatic decompensation and complications are essential components of medical management. The advanced stage of cirrhosis, emergency surgery, open surgeries, old age, and coexistence of medical comorbidities are main factors influencing the clinical outcome of these patients. Perioperative management of patients with cirrhosis warrants special attention to nutritional status, fluid and electrolyte balance, control of ascites, excluding preexisting infections, correction of coagulopathy and thrombocytopenia, and avoidance of nephrotoxic and hepatotoxic medications. Transjugular intrahepatic portosystemic shunt may improve the CTP class, and semielective surgeries may be feasible. Emergency surgery, whenever possible, should be avoided.
Introduction
Liver cirrhosis is the 8th most common cause of death in United States and the 13th most common cause of mortality worldwide. 1 In 2010, liver cirrhosis was estimated to contribute 31 million or 1.2% of global disability-adjusted life years (DALYs). Globally, liver cirrhosis was ranked 23rd leading cause of disease burden. Global liver cirrhosis deaths increased from 1.54% of global deaths in 1980 to 1.95% in 2010.2,3 Epidemic of obesity and growing incidence of chronic viral hepatitis have led to increasing worldwide prevalence of cirrhosis. In a recent population-based study, prevalence of cirrhosis in United States was found to be 0.27%. This prevalence rate when applied to 2010 US census data estimated about 633 323 adults with cirrhosis in the United States. In this study, 70% of patients reported not being aware of their cirrhosis diagnosis, highlighting a huge number of underdiagnosed patients. 4 Such patients may require surgery and any surgical intervention in undiagnosed cirrhotic patients may have catastrophic consequences.
This review article summarizes the current literature about the perioperative management of patients with cirrhosis who are undergoing surgery. After a brief introduction of cirrhosis and its natural history, utility of different scoring systems to assess the perioperative risk is discussed. The pathophysiology of cirrhosis is reviewed, and the use of different anesthetic medications with their pharmacokinetics is discussed. Particular attention has been given to various perioperative key components in patients with cirrhosis, such as nutritional status, thrombocytopenia, coagulopathy, fluid and electrolyte balance, ascites, hepatic encephalopathy (HE), and renal, cardiac, and pulmonary functions. Specific precautions pertaining to different types of surgical procedures are also highlighted with recommendations from recent studies. This knowledge could help in better selection of patients and type of surgery they should be recommended to minimize the morbidity and mortality.
Patients with history of risk factors for liver disease, such as chronic alcohol use, blood transfusion, substance use, tattooing, or family history of liver disease, should be evaluated for chronic liver disease prior to surgery. Suspicion for chronic liver disease should rise in any patient who is obese or has clinical features of cirrhosis, such as palmer erythema, spider nevi, ascites, splenomegaly, leg edema, gynecomastia, testicular atrophy, temporal wasting, parotid gland enlargement, or jaundice. Routine evaluation of liver function tests prior to surgery, in patients without known liver disease, is not recommended. When abnormal liver function tests are noted, detailed review of patient’s medications, including prescribed as well as over-the-counter and herbal medications, should also be done to exclude possible drug-induced liver disease.
Advanced liver disease affects every organ system and is associated with potential life-threatening complications. Preoperative risk stratification of patients with liver cirrhosis, requiring abdominal and nonabdominal surgery, is challenging. It is well known that patients with cirrhosis have increased risk of morbidity and mortality when they require emergent surgery. Careful selection of patients with liver cirrhosis requiring surgery depends on many factors, including stage of cirrhosis, type of surgery, timing of surgery (emergent or elective), and associated comorbid clinical conditions. 5
Cirrhosis can occur as a result of various causes and has 2 distinct phases: compensated and decompensated. The presence of complications of cirrhosis, namely, ascites, spontaneous bacterial peritonitis (SBP), variceal bleeding, HE, hepatocellular cancer, hepatopulmonary syndrome (HPS), and hepatorenal syndrome, characterizes the decompensated state of the cirrhosis. Patients with decompensated cirrhosis have a median survival of less than 2 years. Their 1-year mortality rate is 20% in the presence of ascites, and it rises to 57% if the clinical course is complicated with variceal bleeding. Lack of any of these features represents the compensated phase, which has a median survival of more than 12 years. 6 The other severe complications, including acute liver decompensation and clinical course, may also be complicated by severe coagulopathy, portal vein thrombosis, fluid and electrolyte imbalance, acute renal failure, and sepsis. Other determinants of adverse outcome include emergency surgery, advanced age, and concomitant cardiovascular disease.
Optimal preparation with attention toward cirrhosis complications during perioperative period may decrease the risk of complications or death following surgery. Preparation should include correction of coagulopathy, treating preexisting encephalopathy, controlling ascites, preventing sepsis, and optimizing renal function. 7 Although traditionally discouraged, with the advancements in perioperative care, increasing number of patients with cirrhosis are undergoing surgery. We aim to provide an updated review of comprehensive perioperative care for patients with cirrhosis who are undergoing surgery.
Scoring System and the Preoperative Risk Evaluation
The 2 most widely used scoring systems to help predict the morbidity and mortality of patients with cirrhosis undergoing various types of surgeries are Child-Turcotte-Pugh (CTP) and Model for End-Stage Liver Disease (MELD) score.
Child-Turcotte-Pugh was originally developed by Child and Turcotte in 1964 to predict the mortality during surgery. It was later modified by Pugh in 1973 and is currently used to assess the severity of cirrhosis, prognosis, and management plan. The CTP score has 5 measures, and each measure is given a score from 1 to 3, with 3 reflecting the most severe derangement of the respective clinical or laboratory parameter8,9 (Table 1). Child-Turcotte-Pugh score, though widely used in clinical practice, has not been validated.
CTP score calculation.
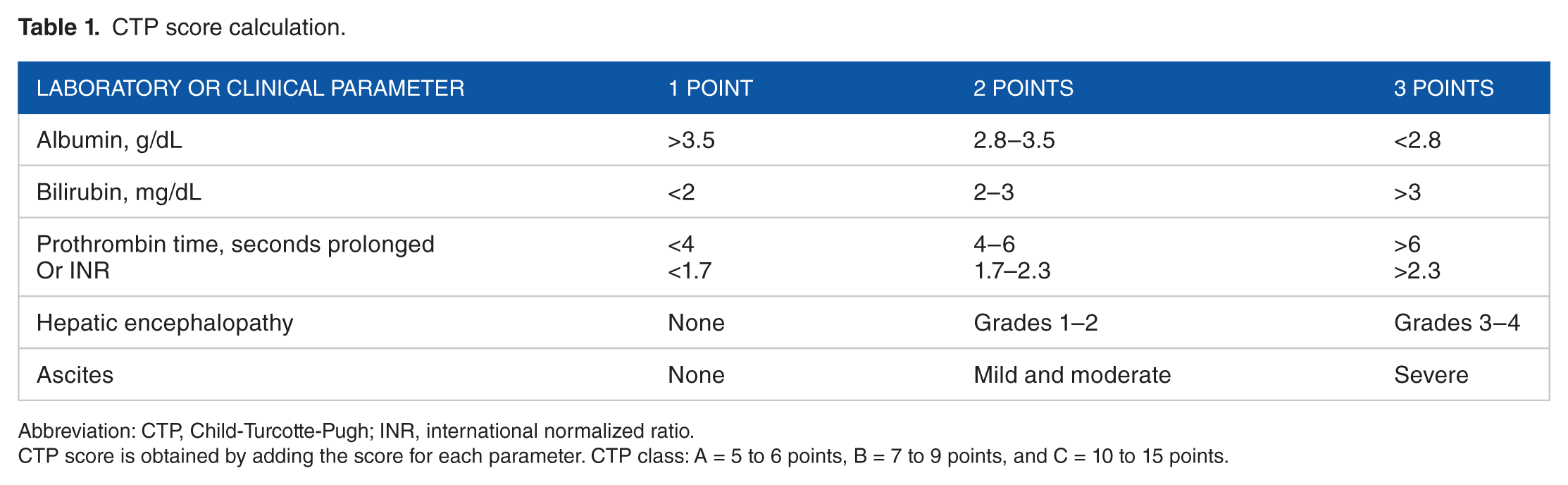
Abbreviation: CTP, Child-Turcotte-Pugh; INR, international normalized ratio.
CTP score is obtained by adding the score for each parameter. CTP class: A = 5 to 6 points, B = 7 to 9 points, and C = 10 to 15 points.
The CTP scoring system has its inherent problem with its reproducibility as it relies on observer’s assessment in evaluating the presence and severity of HE and ascites. The other major problem with CTP scoring system is its arbitrary selection of cutoff values for its parameters, such as albumin, bilirubin, and prothrombin time (PT). Hence, any elevation in bilirubin level above 3.5 mg/dL contributes to the same score in the calculation of the CTP class (ceiling effect).
The MELD was initially developed to predict mortality within 3 months of transjugular intrahepatic portosystemic shunt (TIPS) procedure, 10 and later it was found to be useful in assessing the prognosis of liver cirrhosis and prioritization of candidates for liver transplantation. 11 The MELD score uses the patient’s bilirubin, serum creatinine, and international normalized ratio (INR). Any value less than 1 is given a value of 1, and if the dialysis occurred twice in the last 1 week, the factor for serum creatinine value is 4.0: MELD = 3.78 × ln[serum bilirubin (mg/dL)] + 11.2 × ln[INR] + 9.57 × ln[serum creatinine (mg/dL)] + 6.43. 11
In comparison with CTP, MELD score calculation is based on objective parameters and hence is reproducible. The MELD score has been validated in many studies and is used extensively. Model for End-Stage Liver Disease scores of <10, 10 to 14, and >14 are comparable to CTP classes A, B, and C, respectively. The advanced cirrhosis, defined by CTP class C, and higher MELD score of 14 and above have been consistently noted to presage the higher morbidity and mortality. Previous studies by Garrison et al 12 and Mansour et al, 13 conducted more than a decade apart, have shown comparable mortality rates among patients with liver disease undergoing abdominal surgery.12,13 Garrison et al identified the mortality rates of 10%, 31%, and 76%, whereas Mansour et al showed rates of 10%, 30%, and 82% in patients with CTP classes A, B, and C, respectively. A more recent study in 2010 by Telem et al, 14 however, has shown significantly lower mortality rates of 2%, 12%, and 12% in CTP classes A, B, and C, respectively, in patients with cirrhosis undergoing abdominal surgery.11,14
In the past decade, a number of studies have evaluated the utility of MELD score to predict mortality in patients with cirrhosis undergoing surgery (hepatic and nonhepatic). Study by Perkins et al 15 demonstrated higher postoperative morbidity in patients with MELD score >8; similar study by Befeler et al 16 showed higher postoperative morbidity and mortality in patients with MELD score >14. Northup and colleagues found a 1% increase in mortality for each MELD point until 20 and a 2% increase in mortality with each MELD point after 20. A MELD score of 5 to 15 had mortality of 5% to 11%, as compared with mortality of 26%, 50%, and 67% when the MELD reaches the value of 25, 35, and 45, respectively. 17
The MELD score was found to be superior to CTP class in predicting the outcomes of intra-abdominal surgery. D’Amico et al, 6 in a systemic review of 118 studies, suggested that CTP classification may be better in quantifying the risk in compensated cirrhosis, whereas MELD is better predictor in decompensated cirrhotic state. The prognostic variables in the compensated cirrhosis are different from the variables in the decompensated cirrhosis. Serum creatinine can be used as a surrogate marker of decline in circulatory status which is often seen in patients with decompensated cirrhosis. The MELD score, which uses serum creatinine, hence, may serve as a better predictor of mortality in patients with decompensated cirrhosis. 6
Nevertheless, both scoring systems are comparable in predicting the short-term outcomes. 18
Pathophysiology
Several studies have confirmed that the degree of decompensated liver disease, assessed by CTP classification and MELD score, is the most important factor that determines the perioperative outcomes.12 -14,16,18,19 Due to impaired liver functions, these patients have increased cardiac output, systemic vasodilatation with decreased systemic vascular resistance, diastolic dysfunction, and inappropriate response to surgical stress.
Several hemodynamic changes occur during surgery, which include the reflex systemic hypotension resulting from traction of abdominal viscera during abdominal surgery, hemorrhage, vasodilatation, and reduced blood supply to the liver and resultant ischemic injury to remaining functioning hepatocytes which increases the chance of acute decompensation. General anesthesia itself causes reduced hepatic arterial blood flow.
Preoperative Optimization of Liver Disease
Preoperative management should focus on patients with known cirrhosis and the ones with undiagnosed liver disease. It is important to identify the risk factors for liver disease.
A detailed history with focus on the risk factors for liver disease, such as personal history of blood transfusion, intravenous drug use, tattoos, high-risk sexual behavior, alcoholism, family history of liver disease, travel history, review of prescribed and over-the-counter medication use, and symptoms suggestive of liver decompensation, should be obtained. Physical examination should be performed with focus on the clinical signs of chronic liver disease and features of portal hypertension. Laboratory tests should include complete blood count, liver function tests, PT, partial thromboplastin time, INR, renal function, and electrolytes.
Incidental finding of low platelets, elevated PT, elevated bilirubin, low albumin, or elevated liver enzymes may suggest the presence of chronic liver disease and would warrant a thorough assessment to evaluate the severity of liver disease prior to elective surgery. 20
In patients with known liver disease, preoperative management aims at identifying the cause, and optimizing the liver function by improving the nutritional status, correction of coagulopathy with blood products, and treating subtle or overt HE, portal hypertension, and ascites, is of paramount importance. 20
Abdominal ultrasonography should be obtained to determine the texture and size of liver, size of spleen, and the presence or absence of ascites. Assessment for presence of cirrhosis in patients with chronic liver disease is important due to its serious clinical implications in perioperative period. Liver biopsy, the best reference test available, is invasive. Noninvasive methods, such as FibroTest, which is a combination of serum biochemical markers, and elastography, have been increasingly used. Elastography techniques include transient elastography, ultrasound elastography, and magnetic resonance elastography. Elastography, an alternative to liver biopsy, measures liver stiffness but has its limitations, such as limited depth of penetration and unreliable results in individuals who are obese or have ascites. 21
Preoperative Care
Preoperative anesthesia care
General anesthesia reduces the arterial blood flow to liver and predisposes to ischemic injury. This reduction in hepatic blood is augmented by surgical traction on the liver, rising intra-abdominal pressure either from laparoscopic surgery or positive pressure ventilation, hypocapnia, and use of α-adrenoceptor agonists. Hence, extra caution and meticulous monitoring are required.
With use of isoflurane, slight elevation in live enzymes without clinical consequences was noted. 22 Isoflurane is considered safe as long as the systemic blood pressure is not reduced by 30%. 23 The use of inhalation agents (isoflurane, desflurane, or sevoflurane), alone or in combination with small doses of fentanyl, can be used with reasonable safety profile. 24 Desflurane, due to its ability to preserve the hepatic blood flow and cardiac output, is considered the safest anesthetic agent in patients with cirrhosis. It undergoes minimal hepatic metabolism and is rapidly excreted from the body. 25
Among the opiate analgesics, remifentanil is the safest agent as it is metabolized by the red cell esterase, rather than the hepatocytes. Elimination of other opiates such as morphine, fentanyl, and alfentanil is reduced. In cases of advanced liver cirrhosis, the dose of intravenous anesthetic agent thiopental should be decreased. Etomidate can be used safely. Cirrhosis does not significantly affect the elimination half-life of propofol, suggesting its safety in such patients. 26 Benzodiazepines should generally be avoided. Comparison of midazolam with propofol in patients with cirrhosis has consistently shown propofol to be safer due to its faster elimination. 27 Owing to lack of hepatic excretion, atracurium and cisatracurium are safe neuromuscular blocking agents. However, vecuronium has been shown to prolong the duration of action of the neuromuscular blockade and also the time to recovery in patients with cirrhosis undergoing surgery. 28
Spinal or epidural anesthesia may reduce the mean arterial pressure, which is of concern in patients with cirrhosis who already have hyperdynamic circulation due to peripheral vasodilatation. When coagulopathy or thrombocytopenia is present, these routes are not preferred due to increased risk of bleeding.
Perioperative Care
Following factors need specific attention in patients with cirrhosis.
Nutrition
Malnutrition among patients with cirrhosis is very common, and more than 80% of patients suffer from malnutrition.29,30 Accurate assessment of nutrition is challenging. Several factors contribute to malnutrition, such as reduced food intake due to anorexia and ascites, impaired absorption of nutrients, and increased catabolism. Malnutrition is an independent predictor of mortality in patients with liver cirrhosis. 31
The parameters suggested to assess malnutrition should include the assessment of lean body mass and muscle function, in addition to serum albumin and anthropometric parameters that are not affected by the excess fluid retention in patients with cirrhosis, such as triceps skin fold and mid-arm muscle circumference. 32
Hypoalbuminemia, a hallmark of liver disease and malnutrition, leads to reduced oncotic pressure and intravascular hypovolemia, impaired wound healing, sepsis, delay in recovery, impaired mobility, and respiratory muscle dysfunction resulting from muscle wasting. Hypoalbuminemia is a predictor of mortality in patients with cirrhosis undergoing surgery. A low serum albumin level of 2.1 g/dL when compared with serum albumin level of 4.6 g/dL was associated with higher mortality of 29% vs 1%, as well as higher morbidity of 65% vs 10%, respectively. 33 Postoperatively, serum albumin level can be low due to stress of surgery, injury, illness, and infection. Intravenous albumin infusion has no effect on mortality, and routine use is not justified.34,35
Perioperative nutritional supplementation may reduce the short-term complications. There is an association between nutritional state and postsurgical outcomes in these patients, and perioperative nutritional support leads to better outcomes.36,37 A preoperative nutritional consultation is of paramount importance to optimize the nutritional status of the patient, and nutritional supplementation should be continued in the postoperative period. In patients with a history of heavy alcohol use, a period of abstinence before undergoing any elective surgery is advised to prevent the development of withdrawal symptoms and delirium tremens. 38
If HE is present, diet to halt its progression should include high carbohydrate and high lipid. 7 Milk-based and vegetable-derived proteins are preferred. Branched-chain amino acid formula may also be used as a source of protein in patients with HE, but it is rarely used due to high cost and poor palatability. Nasogastric tube feeding should be considered in patients who are unable to take oral intake. Fat-soluble vitamin deficiency is often noted in patients with liver disease. Trace elements and vitamins, such as zinc, magnesium, copper, folate, and vitamin B12, also are noted to be low in patients with cirrhosis. These deficiencies should be corrected as they delay the wound healing and increase risk of infectious complications.
Coagulopathy and thrombocytopenia
Changes in hemostasis in patients with cirrhosis are complex. Cirrhosis affects levels of both procoagulants and anticoagulants. 39 Nonavailability of routine tests to measure the effect of cirrhosis on the levels of anticoagulants further complicates the matters. Thus, measuring the effect on procoagulants only and demonstrating elevated INR in a patient with cirrhosis are not equivalent to elevated bleeding risk in these patients. However, in the absence of an ideal test to measure the changes in hemostasis in patients with cirrhosis, use of INR continues to be a common practice.
Elevated INR is also included in the commonly used models, such as CTP and MELD score, for the severity of liver cirrhosis. With the understanding that coagulopathy due to liver synthetic impairment cannot be corrected with vitamin K supplements, in an elective surgery, vitamin K administration should still be tried in case malabsorption had contributed to coagulopathy.
Thromboelastography, a novel technique, assesses all the phases of clot formation and lysis. It measures the viscoelastic properties of blood clotting and should be used where available. It can precisely identify the deficiency of various components involved in the formation of blood clot and thus guide on what blood product to be used. 40 It has been shown to reduce the procedure-related unnecessary transfusions and its related complications without increasing bleeding complications. 41
When thromboelastography is not available, fresh frozen plasma (FFP) is often used to correct elevated INR. The effect of FFP transfusion is negligible in correction of coagulopathy if INR is less than 1.7. 42 Whenever FFP is being used, one should keep in mind the short half-life of certain clotting factors, such as von Willebrand (VWB) (2-5 hours), factor VII (5-7 hours), and factor VIII (8-12 hours). 43
It carries the potential risk of fluid overload and pulmonary congestion, and hence, central venous pressure monitoring is recommended.4,7 Coagulopathy and thrombocytopenia are not contraindications for placing a central venous line. Central line placement under ultrasonogram guidance is safe and further reduces the risk of complications. 44
If coagulopathy is not corrected with FFP, cryoprecipitate or desmopressin can be used to correct clotting abnormalities. Viscoelastic test–guided management would help reduce the use of FFP and guide the use of coagulation factors such prothrombin complex and fibrinogen concentrate. 45 In patients with fluid overload, cryoprecipitate is preferred over FFP as it contains a large amount of fibrinogen and VWB factor. The other useful pharmacologic agents with promising results include lysine analogs, such as epsilon aminocaproic acid or tranexamic acid, and serine protease inhibitor, such as aprotinin. 46 Use of these agents does carry the risk of thrombotic complications. None of these pharmacologic agents has shown any benefit in control of variceal bleeding. 47
Thrombocytopenia is common in a patient with cirrhosis, and, along with splenomegaly, it is considered a surrogate marker of portal hypertension. The proposed mechanisms include impaired synthesis of thrombopoietin, which is a stimulant of bone marrow for production of platelets, and increased destruction through hypersplenism. Prophylactic platelet transfusion is recommended before surgery if platelet count is <50 000/mm3. The required level of correction of coagulopathy and thrombocytopenia also depends on the type of surgery. Although peripheral vascular procedures including epidural anesthesia can be safely done with platelet count >50 000/mm3, any eye surgery or neurosurgical procedure 48 would require a minimum platelet count of 100 000/mm3.
Fluid and electrolytes
Fluid and electrolytes should be monitored closely and corrected as needed. Hyponatremia in liver cirrhosis is considered an ominous sign as it represents the fluid overload resulting from reduced solute-free water clearance. It can lead to severe ascites, HE, renal impairment, and increased hospital stay. Oral fluid restriction is required when the serum Na is less than 125 mmol/L. Postoperative ascites can be prevented from accumulating by restricting sodium and minimizing intravenous fluid administration. 49
Correction of hypokalemia also helps to restore the sodium level.
Vasopressin receptor antagonists increase the risk of variceal bleeding and mortality, hence are contraindicated. Demeclocycline, because of nephrotoxic potential, is best avoided.
Hypovolemic hyponatremia, in the context of decreased oral intake and excess diuretics, is a separate entity, requiring prompt identification and appropriate management. 50
Hypokalemia, through increased synthesis of ammonia in the proximal tubules, can precipitate and worsen the HE and should be corrected promptly. 51
Hepatic encephalopathy
Careful assessment of the mental status should be performed to identify subtle signs of low-grade (covert) HE. It may require psychometric or neuropsychological tests to diagnose low-grade HE. 52
Failure to identify low-grade HE may result in worsening of the condition to overt HE. It may lead to aggressive and uncooperative patient behavior interfering with delivery of important treatment measures and nursing care, immobility with its complications, aspiration pneumonia, and myriads of unnecessary investigations for the evaluation of acute delirium. 20 Malnutrition worsens the HE and needs special attention. 32
Diet should include protein intake of 1.0 to 1.5 g/kg daily with sodium restriction to 2 g in those with ascites. Certain medications, such as benzodiazepines, opiates, antidepressants, and antipsychotics, may specifically worsen or precipitate the HE and should be avoided. Other common precipitants include renal failure, gastrointestinal bleeding, infection, constipation, and diuretics-induced hypokalemia and alkalosis that help in the conversion of ammonium ion (NH4+) to ammonia (NH3). Hyponatremia increases the permeability of blood-brain barrier, which can potentiate the effects of hyperammonemia, and fluid restriction may be needed. Lactulose, when used to treat HE, should be administered with the target of 2 to 3 soft bowel movements each day.
Zinc deficiency, resulting from decreased protein intake, increased binding with albumin, and increased excretion, is common in patients with cirrhosis. Being an important cofactor, its deficiency deregulates the urea cycle and generates ammonia that ultimately worsens the HE. The replacement of zinc cannot be overemphasized. 53
Ascites
Diet low in sodium should be continued to prevent reaccumulation of ascites. Diuretics at appropriate doses should be started, with close monitoring of electrolytes and renal functions. Medical management of ascites may improve the CTP class, and surgery may become feasible in some patients if it was contraindicated due to ascites. Refractory ascites may need TIPS as a rescue measure prior to surgery if absolutely necessary. Optimal management of ascites may reduce certain postoperative complications such as recurrence of umbilical hernia.
Renal function
Decrease in lean body mass in liver cirrhosis can overestimate the renal function measured by serum creatinine despite the low glomerular filtration rate. Fluid and electrolyte balance need to be meticulously monitored. Nephrotoxic medications should be avoided. If therapeutic ascitic tap is performed, then albumin infusion at a rate of 6 to 8 g for every liter in excess of 4 L of ascitic fluid should be given. If there is evidence of SBP with a serum creatinine >1 mg/dL, blood urea nitrogen >30 mg/dL, or total bilirubin >4 mg/dL, patient should receive albumin infusion at a rate of 1.5 g/kg of body weight within 6 hours of detection and 1.0 g/kg of body weight on 3rd day. 49
Pulmonary functions
Pleural effusion associated with ascites is common and can rarely result in respiratory distress and hypoxia. Hypoxia is usually not severe and does not necessitate pleural drainage. The development of HPS or portopulmonary hypertension is portentous, and any surgical intervention becomes very challenging. 54
Hepatopulmonary syndrome, a triad of hypoxemia associated with intrapulmonary vascular abnormalities and liver cirrhosis, has no effective treatment other than liver transplant which has higher mortality when compared with patients without HPS.
55
Intravenous infusion of epoprostenol, prostaglandin I2, may improve pulmonary hemodynamics and help facilitate the liver transplant, but postoperatively, pulmonary hypertension may continue to worsen.
56
Pulse oximetry with exercise can be used to assess the pulmonary function in the patients suspected to have HPS. Baseline arterial blood gas can be obtained in patients with cirrhosis as a part of preoperative assessment.
57
Patients with Pa
Infections
Preoperative evaluation should focus on preexisting infections and appropriate treatment as undiagnosed, and untreated infections in patients with cirrhosis have increased morbidity and mortality compared with their noncirrhotic counterparts undergoing the same surgery. The prophylactic antibiotic choice remains the same as for noncirrhotic patients. 58
Patients with cirrhosis have impaired immunity that makes them prone to infections, with higher incidence of multidrug-resistant organisms. Currently, prophylactic antibiotics are recommended in the setting of low-protein ascites (<1.5 g/dL) and advanced cirrhosis (primary prophylaxis), prior history of SBP (secondary prophylaxis), and gastrointestinal hemorrhage. 59 In patients with SBP, albumin infusion at recommended doses improves the risk of mortality.
Esophageal varices
Undergoing a surgery does not put a patient with cirrhosis and varices at risk of variceal bleeding, but fluid overload with consequent worsening of portal hypertension should be avoided. Patients with small esophageal varices, in conjunction with CTP class B or C cirrhosis or large varices irrespective of CTP class, require prophylaxis with nonselective β-blockers. If the bleeding from esophageal varices is not controlled with endoscopic variceal ligation, or bleeding recurs despite pharmacologic and endoscopic treatment, TIPS should be performed to reduce portal hypertension, an underlying pathologic mechanism. 60
Postoperative Care
Postoperative pain relief
Pain management in patients with cirrhosis is a unique challenge. Morphine has a prolonged duration of action and decreased clearance in this group of patients. 61 In patients with CTP class A, morphine and fentanyl are well tolerated. However, the dose and frequency of opiates should be reduced in patients with cirrhosis due to increased half-life and bioavailability. These patients should be carefully monitored for signs of sedation and encephalopathy, and opioid-induced constipation should be avoided with the use of laxatives. 61 Regional analgesia in the form of local infiltration or transverse abdominis plane block is an alternative in patients who are intolerant to opiates because of advanced disease and have high risk of HE.
Epidural analgesia should be considered only after the correction of coagulopathy with INR <1.5 and thrombocytopenia with target platelet count >100 000/mm3. 25
The use of acetaminophen is not contraindicated, but it should be used with caution, and recommended dose is 2 to 3 g/day. Nonsteroidal anti-inflammatory drugs should be avoided because of their potential nephrotoxicity, gastrointestinal bleeding, and platelet dysfunction. 61
Specific Precautions for Different Types of Surgery
In addition to the severity of cirrhosis, American Society of Anesthesiologists physical status classification, reflecting the presence and severity of comorbid conditions, is also expected to influence the survival after major surgeries in patients with cirrhosis. 62 Emergency surgical procedures had unacceptably high mortality of 57% compared with 10% in elective surgeries. 5
Certain surgical procedures, such as cardiac surgeries or open abdominal surgery, are associated with higher mortality and morbidity. Open abdominal surgical procedures were particularly noted to have higher mortality, such as 17% with open cholecystectomy, 24% with colectomy, and 54% with gastric resection, in addition to unacceptably high rates of morbidity, as high as 48% with colectomy and 78% with gastric resection. Laparoscopic approach has significantly reduced postoperative mortality in these patients who have poor functional hepatic reserve.
The study by Befeler et al 16 found anemia to be an independent factor that contributes to poor outcome and suggested preoperative blood transfusion to target hemoglobin of 10 g/dL.
Cholecystectomy
Gallstone disease, mostly secondary to pigment stones, is not uncommon. Compared with cholesterol gallstones in general population without cirrhosis, pigment stones in cirrhosis occur at an older age and involve men more commonly or in equal proportion to women. 63 Prior to advent of laparoscopic approach for cholecystectomy, mortality with open cholecystectomy was reported to be as high as 87%. 64 Subsequently, several meta-analysis and reviews have demonstrated the safety of laparoscopic approach. It has led to significant decline in postoperative mortality, other complications, and overall hospital stay.65-69 In patients with CTP class C, cholecystectomy should be avoided, and instead, conservative management with antibiotics and cholecystostomy tube placement or endoscopic retrograde cholangiopancreatography with sphincterotomy should be performed.
Hernia
Owing to raised intra-abdominal pressure due to ascites and muscle weakness from decreased muscle mass and malnutrition, umbilical and inguinal hernia incidence is higher in patients with cirrhosis. Interestingly, umbilical hernias can also be present in a patient with cirrhosis without refractory ascites. 70 Hypothesis purported behind this finding is probable transmission of portal pressure from recanalized umbilical vein to umbilicus. 71
Acute rupture of umbilical hernia in patients with liver cirrhosis carries high mortality. 72 Elective surgery of umbilical hernia, through the laparoscopic approach, with use of intraperitoneal mesh insertion, should be performed in selected patients. The improved surgical techniques and improved perioperative care have resulted in reduced morbidity and mortality. 73 Emergency surgical repair of hernia was invariably related to higher complication rate, including recurrence of hernia (22%), surgical site edema (17%), HE (5%), and variceal hemorrhage (5%). The high recurrence rate can be ameliorated through optimization of medical care for ascites such as salt and fluid restriction, appropriate dose of diuretics, and even evaluation for TIPS. 74 If there is absolute contraindication for hernia repair, TIPS should be considered for control of ascites and to prevent the progression of hernia and its complications. Transjugular intrahepatic portosystemic shunt can also be considered, even in the absence of ascites, in the management of recurrent umbilical hernia in patients with cirrhosis, as TIPS helps to mitigate the portal hypertension that is a major contributing factor for the development of umbilical hernia. 70 Azoulay et al 75 studied the use of TIPS to reduce portal hypertension prior to elective major abdominal surgery, with favorable results. Optimization of medical care with adequate nutrition, antibiotics, and nonocclusive dressing, along with ascites management, should be continued, prior to surgical repair without mesh. 72
If the patient with cirrhosis has umbilical hernia with obstructive symptoms such as intermittent incarceration or trophic skin changes, surgical repair should be considered. 76 Medical optimization should be achieved before the elective operative intervention of the hernia. Emergency repair of the hernia should be avoided as the mortality in emergency surgery remains unacceptably high. 77 A recent retrospective study of liver disease patients with umbilical hernia found a mortality of 11.1% in patients with MELD score of 15 or higher compared with 1.3% in patients with MELD score <15. The study authors suggested to avoid elective repair of umbilical hernia in patients older than 65 years, with MELD score of 15 or more, preoperative sepsis, and serum albumin <3.0 g/dL. 78
Bariatric surgery
Because of the rising obesity epidemic, many obese patients are undergoing bariatric surgery. Obesity-related nonalcoholic fatty liver disease in these patients puts them at higher risk of complications from the surgical procedures. As indicated in studies by Weingarten et al 79 and Brolin et al, 80 about 1% to 2% of patients were found to have cirrhosis as an unexpected finding on the surgical table. Patients with compensated cirrhosis undergoing bariatric surgery had 2-fold increase in mortality compared with patients without cirrhosis and it climbed to 20-fold with decompensated cirrhosis. Mortality further climbed to 41% in decompensated liver cirrhosis exclusively treated at smaller centers performing fewer than 50 bariatric surgeries per year. 81
More recently, in compensated cirrhosis, bariatric surgery has been performed without any additional postoperative complications. Bariatric surgery in such patients, in addition to weight loss, results in improvement in metabolic profile and reversal of hepatic steatosis. 82 If possible, laparoscopic procedures such as laparoscopic Roux-en-Y gastric bypass, laparoscopic sleeve gastrectomy, or laparoscopic adjustable gastric banding should be performed as it is associated with fewer complications, lower mortality, and similar reduction in weight and its attendant benefits of improvement in metabolic profile. 83
Colorectal surgery
Colorectal surgery in a patient with cirrhosis is associated with 26% mortality. Postoperative complications such as stoma complications and anastomotic leaks are unique to this group. Not surprisingly, a higher MELD score of 15 or more is an independent predictor of mortality. 84 Colorectal surgeries in patients with CTP class A are safe; however, patients with CTP classes B and C had higher morbidity and mortality especially if emergency surgery was needed. 85
Gastric surgery
Peptic ulcer disease is common in patients with liver disease. Esophagogastroduodenoscopy to evaluate for peptic ulcer disease and treatment with proton pump inhibitor is the mainstay of treatment.
If surgical repair is needed, laparoscopic approach should be preferred. The mortality of 9% to 10% has been noted in patients with cirrhosis undergoing gastric surgery.86,87
Hepatic surgery
Patients undergoing liver surgery should be evaluated for the presence of portal hypertension. Definite measures such as measurement of hepatic venous pressure gradient or the presence of gastroesophageal varices should be used rather than the surrogate markers such as splenomegaly and thrombocytopenia, as the mere absence of splenomegaly and presence of normal platelet count do not rule out the possibility of portal hypertension. Clinically significant portal hypertension doubles the mortality and increases the complication rate 3 times compared with patients without it. 88
Certain clinical issues are very unique to liver cirrhosis. Elevated lactate level portends poor prognosis, and non-lactate–containing solutions should be used.
Hypophosphatemia is particularly dangerous, with its associated complications such as neuromuscular dysfunction, respiratory muscle weakness, impairment in energy production with resultant cellular dysfunction, and hemolytic anemia. 89 Supplementation of branched-chain amino acids after hepatic resection has been found to be associated with feeling of well-being and improved quality of life. Hyperglycemia is a common phenomenon, associated with higher morbidity and mortality and merits special attention. Postoperative coagulopathy typically worsens on days 2 to 5, with elevation in INR and decline in platelet count and fibrinogen level. Judicious use of analgesics is advised, including removal of epidural catheter before the coagulopathy is expected to get worse. Synbiotic treatment, a combination of prebiotics and probiotics, through enteral nutrition will help preserve the intestinal mucosal integrity and prevent infectious complications. 90 In the postoperative period after hepatic surgery, thromboembolism happens less frequently compared with other abdominal surgeries. But nevertheless, patients with cirrhosis are in hypercoagulable state, stemming from the deranged balance from the impaired synthesis of both anticoagulants and procoagulants. The rate of venous thromboembolism decreases with chemical prophylaxis, without any additional bleeding episode requiring blood transfusion. 91 Colloids are preferred intravenous solution in patients undergoing liver surgery.
Cardiothoracic surgery
Cirrhosis of liver is a well-recognized predictor of mortality in patients undergoing cardiac surgery. This high mortality is related to inherent problems related to hemodynamic changes associated with liver disease rather than cardiac surgery itself.
Diastolic dysfunction, a common finding in patients with cirrhosis, is not related to increased mortality or postoperative complications. 92
A review by Hayashida suggested that in patients with CTP class A, cardiac surgery even with cardiopulmonary bypass may be performed safely, but with advanced cirrhosis, the risk of complications and mortality is too high. Mortality ranging between 50% and 80% with CTP class B and 100% with CTP class C were recorded with cardiopulmonary bypass. 93 However, others have reported significant mortality across all CTP classes of cirrhosis patients. Systemic review of 30-day mortality after cardiac surgery by Jacob et al showed 9%, 37%, and 52% mortality in class A, B, and C cirrhosis patients, respectively.
In open-heart surgery, higher morbidity was noted in patients with advanced CTP class, use of cardiopulmonary bypass, and higher crossclamp times, whereas high MELD scores and low serum cholinesterase levels predicted higher mortality. 94
If cirrhosis is compensated, thoracic surgery has been performed for lung cancer without any added risk of mortality or postoperative complications, compared with patients with no cirrhosis. Surgical approaches ranged from explorative thoracotomy, wedge resections, segmentectomies, lobectomies, and pneumonectomies. 95
Gynecologic surgery
Literature on gynecological surgeries in patients with cirrhosis is scarce. In a study by Nielsen et al, 96 high 30-day postoperative mortality was noticed among patients with cirrhosis compared with controls (7.6% vs 0.6%) who underwent hysterectomy. In another retrospective analysis among patient with cirrhosis undergoing surgery for gynecological cancer, significantly higher complication rate was observed. 97
Orthopedic and spine surgery
Even though the knee or hip replacement surgeries are elective, the presence of cirrhosis causes unfavorable systemic reactions leading to more complications. 98
Patients with any stage of cirrhosis, undergoing elective knee or hip replacement for severe osteoarthritis, had similar intraoperative complications compared with noncirrhotic patients, but they were more likely to be transferred to intensive care unit or medical unit, had higher risk of deep prosthetic infection (2.5-fold higher), 30-day mortality, and need of revision surgery. Infection recurrence in reimplanted prosthesis is about 30%, with hepatic dysfunction being the most important risk factor for development of infection related to prosthesis. 99 There was also a high readmission rate mainly due to infection, liver, or renal failure. 100 Similarly, higher perioperative complication rate of up to 41% was noted in incremental fashion in advancing cirrhosis, especially in association with low albumin or ascites. 101
Neurosurgical procedures
Patients with cirrhosis may have spontaneous intracranial hemorrhage or traumatic brain injury for which they may require neurosurgical intervention. A retrospective review by Chen et al 102 showed a high complication rate of 54% and mortality rate of 24% in these patients. Liao et al 103 have reported higher rates of blood loss, hospitalization days, and complications in patients with cirrhosis undergoing lumbar spine surgery. Higher CTP class of cirrhosis has been shown consistently, like other surgeries, to predict higher morbidity and mortality.
Conclusions
Validated scores such as MELD and CTP class can assess the perioperative morbidity and mortality in patients with cirrhosis. The severity of liver decompensation, timing of surgery, and type of surgery are the most important determinants of the surgical outcome in patients with cirrhosis. Elective surgery should be planned whenever possible. Patients with CTP class A can undergo most of the surgical procedures with a reasonable safety profile. Patients with CTP class C and MELD score above 15 should not undergo any elective surgical procedure, rather nonsurgical approach such as endoscopic or interventional radiological procedures should be preferred, if absolutely necessary.
Emergency surgery confers 4 to 5 times higher mortality, and certain surgeries, such as cardiac surgeries with cardiopulmonary bypass, are to be avoided even in patients with CTP class B. Emergency surgeries should be deferred if possible, and with meticulous optimization of medical management (Table 2), the semielective surgery should be arranged. Advancing age, and the presence and severity of comorbidities, may provide additional clue in assessing the perioperative morbidity and mortality. Transjugular intrahepatic portosystemic shunt can be considered to reduce portal hypertension prior to the nonhepatic abdominal surgery. Laparoscopic surgery should be performed whenever possible, as it is associated with less tissue trauma, traction of the abdominal viscera, and risk of bleeding and infection. Cautious control of hemostasis is a critical component of surgical care. Nephrotoxic and hepatotoxic medications need to be avoided. Any patient with cirrhosis undergoing major surgery should be referred to a specialist with experience in managing liver disease, and such surgery should be performed in a center with adequate volume.
Summary of perioperative evaluation and management in patients with cirrhosis.

Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; DDAVP, desmopressin; ECHO, echocardiography; FFP, fresh frozen plasma; GFR, glomerular filtration rate; HPS, hepatopulmonary syndrome; HRS, hepatorenal syndrome; INR, international normalized ratio; SBP, spontaneous bacterial peritonitis; TIPS, transjugular intrahepatic portosystemic shunt.
Footnotes
Peer review:
Four peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1450 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NA, HA, and JM wrote the first draft of the manuscript. BB made critical revisions and approved final version. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) has provided to the publisher signed confirmation of compliance with legal and ethical obligations including, but not limited to, the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication. There are no disclosures.