
Abstract
Background:
Breast magnetic resonance imaging (MRI) is an important imaging tool for the management of breast cancer patients and for screening women at high risk for breast cancer.
Objectives:
To examine long-term trends in the distribution of histologic diagnoses obtained from MRI-guided breast biopsies.
Design:
Retrospective analysis.
Methods:
We retrospectively reviewed the distribution of histologic diagnoses of MRI-guided breast biopsies from 2004 to 2019. All cases underwent central pathology review and lesions were classified based on the most prominent histologic finding present. Magnetic resonance imaging features were extracted from radiology reports when available and correlated with pathology diagnoses.
Results:
Four hundred ninety-four MRI-guided biopsies were performed on 440 patients; overall, 73% of biopsies were benign and 27% were malignant. The annual percentages of benign and malignant diagnoses remained similar throughout the 16-year period. Of the benign entities commonly identified, the percentage of benign papillary and sclerosing lesions detected in the benign biopsies increased significantly (13% in 2004-2011 vs 31% in 2012-2019, P = .03). The mean size of malignant lesions was larger than benign lesions (30.1 mm compared with 14.2 mm, P = .045); otherwise, there were no distinguishing radiologic features between benign and malignant lesions.
Conclusion:
The specificity of breast MRI remained constant over a 16-year period; however, there was a shift in the distribution of benign diagnoses with increased detection and biopsy of benign papillary and sclerosing lesions. Monitoring the distribution of breast MRI biopsy diagnoses over time with radiology-pathology correlation might improve the suboptimal specificity of breast MRI.
Introduction
Breast magnetic resonance imaging (MRI) is an important imaging tool for the management of breast cancer patients and for screening women at high risk for breast cancer. Current indications for the utilization of breast MRI include preoperative staging in women with known breast cancer, screening patients who are at high risk for the development of breast cancer, and assessing response to neoadjuvant chemotherapy. 1 Breast MRI can also be used to evaluate nipple discharge, complications of breast implants, and further characterize lesions that are indeterminate by other imaging modalities. While breast MRI is highly sensitive for the detection of breast cancer, the specificity of breast MRI remains suboptimal; the majority (60%-80%) of all MRI-guided breast biopsies continue to yield benign findings.2-9
Due to the inherent complexity of reporting breast MRI, combined with heterogeneous breast pathology diagnoses, breast MRI radiology-pathology correlation remains challenging. While prior studies have described the pathologic findings of MRI breast biopsies, often with radiologic correlation,2-9 there has been variable progress in reducing the number of unnecessary breast MRI-guided biopsies. Furthermore, no studies have focused on potential variation in the distribution of histologic diagnoses over an extended time period. Therefore, the main objective of this study was to evaluate changes in histologic diagnoses over time to focus MRI techniques and interpretation on potentially decreasing the false-positive rate of breast MRI.
Patients and Methods
The institutional radiology database was retrospectively reviewed to identify all MRI-guided breast biopsies performed at Dartmouth Hitchcock Medical Center between September 2004 and October 2019. Lesions detected by MRI but biopsied with different imaging modalities were excluded. Second-look ultrasounds were performed for discrete masses or nonmass enhancement greater than 3 cm in size. Second-look mammograms were performed to asses for targetable calcifications. If the second-look ultrasound and/or mammogram were negative, a MRI-guided biopsy was performed. The pathology slides were reviewed by a fellowship-trained breast pathologist (JDM), and diagnoses were classified based on the most prominent histologic finding present in the core biopsy. Benign categories included normal breast tissue, fibrocystic changes (combination of usual ductal hyperplasia, adenosis, and cysts), papillary and sclerosing lesions (papilloma, radial scar, and complex sclerosing lesion), fibroadenoma, fat necrosis, cystic apocrine metaplasia (CAM), and high-risk lesions (atypical ductal hyperplasia [ADH], atypical lobular hyperplasia [ALH], or lobular carcinoma in situ [LCIS]). Malignant lesions included invasive carcinomas and ductal carcinoma in situ (DCIS). At our institution, malignant lesions and ADH are excised; papillary and sclerosing lesions and lobular neoplasia are reviewed on an individual basis.
The MRI protocol during the study period consisted of prone examinations on a 1.5T GE Signa (Milwaukee, WI) or a 3.0T Siemens Skyra (Munich, Germany) using a Hologic 8-channel breast coil (Marlborough, MA) or an Invivo 7-channel breast coil (Orlando FL). The imaging protocol and biopsy procedures were as stated in a prior publication. 10
Background parenchymal enhancement, breast density, morphologic lesion characterization, and kinetic enhancement pattern were extracted from the radiology reports. Lesions were categorized as a focus (<5 mm), mass (⩾5 mm), or nonmass enhancement according to the Breast Imaging-Reporting and Data System (BI-RADS) criteria. 11 All lesions were BI-RADS 4 or 5. Diffusion-weighted imaging was not performed. Kinetic analysis was performed on contrast-enhanced images with enhancement curve analysis. The indication for breast MRI, if available, was obtained from the electronic medical record; indications were categorized as preoperative staging, high-risk screening, diagnostic evaluation of lesions indeterminate on mammography and ultrasound, and other. Detailed review of select MRI studies was performed by a breast radiologist (RDF).
Statistical analyses
Descriptive statistics were used to report patient age, clinical indication, histologic findings, and imaging features. To analyze trends over time, percentage of histologic diagnoses was compared between the first and second halves of the evaluation period (2004-2011 and 2012-2019) and 4 quarters (2004-2007, 2008-2011, 2012-2015, and 2016-2019). Microsoft Excel v16.44 (Redmond, VA) was used to create graphs demonstrating trends over time. IBM SPSS statistics v24 (Chicago, IL) was used to calculate P values by using 2-sample t tests when comparing continuous variables or chi-square testing when comparing categorical variables. A P value < .05 was considered significant.
Results
Clinical features and histologic findings
From September 2004 to October 2019, 6678 breast MRIs were performed, with 494 MRI-guided breast core needle biopsies performed on 440 patients (7% of all MRIs resulted in a MRI-guided biopsy). Clinical features and indication for breast MRI are summarized in Table 1. The most common indication for MRI-guided breast biopsy was pre-operative staging in a patient with a recent diagnosis of malignancy (n = 289, 59%). The percentage of MRI-guided biopsies for staging decreased from 71% (2004-2011) to 56% (2012-2019) (P = .06), and the percentage of biopsies for high-risk screening increased from 24% (2004-2011) to 34% (2012-2019) (P = .07).
Clinical features of MRI-guided core needle biopsies 2004 to 2019 (n = 494).

Abbreviation: MRI, magnetic resonance imaging.
Most MRI-guided breast biopsies were benign (73%, 363 of 494), while 27% (131 of 494) were malignant. Table 2 lists the distribution of diagnoses based on the predominant histologic finding. An atypical (high-risk) lesion (ADH, ALH, and LCIS) was the predominant finding in 26 cases. In addition, ADH, ALH, or LCIS was incidentally identified in 23 cases in which a benign, nonatypical lesion was the predominant finding; overall, 49 cases (10%) harbored such high-risk atypical lesions. In patients with recently diagnosed breast cancer undergoing preoperative staging MRIs, 63% of the MRI-detected and biopsied malignancies were ipsilateral to the known cancer and 37% were contralateral. In contrast, 59% of biopsies with papillary/sclerosing lesions or a high-risk lesion (either the predominant finding or an incidental finding) were contralateral to the known cancer and 41% were ipsilateral. The MRI-biopsied invasive carcinomas had the following receptor and tumor grade distributions: estrogen receptor (ER)/progesterone receptor (PR) positive (77%); human epidermal growth factor receptor 2 (HER2) positive (10%); ER negative, PR negative, and HER2 negative (13%); low grade (34%), intermediate grade (36%), and high grade (30%).
Predominant histologic findings of MRI-guided breast biopsies 2004 to 2019 (n = 494).
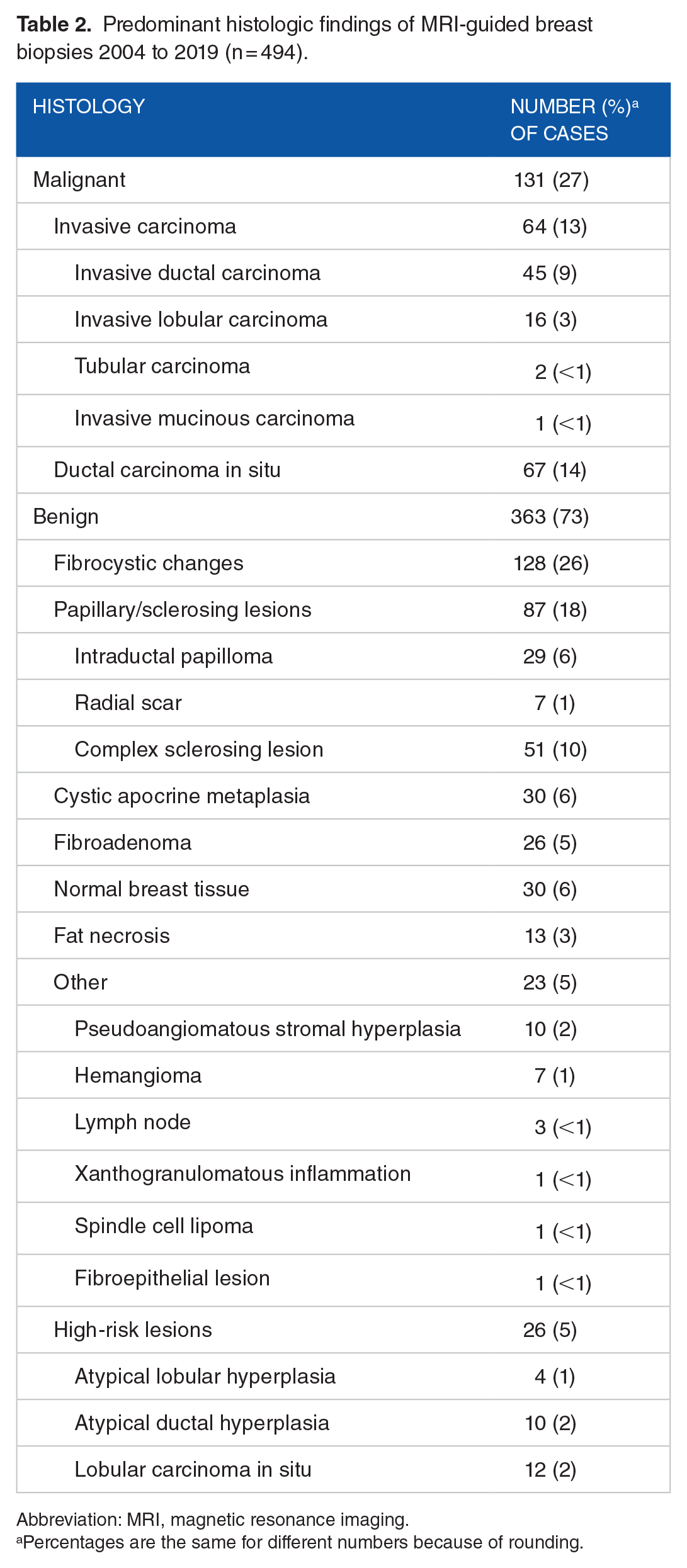
Abbreviation: MRI, magnetic resonance imaging.
Percentages are the same for different numbers because of rounding.
The yearly percentage of benign vs malignant diagnoses obtained from MRI-guided breast biopsies remained constant from 2004 to 2019 (Figure 1A). The overall 4 most commonly identified benign entities included fibrocystic changes (26%), papillary and sclerosing lesions (18%), CAM (6%), and fibroadenomas (5%). Of these, papillary and sclerosing lesions comprised an increasing percentage of the benign diagnoses between the first and second halves of the evaluation period (Figure 1B, mean 13% 2004-2011 vs 31% 2012-2019, P = .03).

(A) Percentage of benign and malignant diagnoses obtained from MRI-guided biopsies from 2004 to 2019. (B) Percentage of select benign diagnoses from 2004 to 2019 (percentage of all benign biopsies). Data are displayed as percentage for each quartile; data labels in 1B are for benign papillary and sclerosing lesions. MRI indicates magnetic resonance imaging.
MRI findings
Table 3 summarizes the available MRI features and compares benign vs malignant lesions. Malignant lesions were more likely to be larger than benign lesions (30.1 mm compared with 14.2 mm, P = .045); there were no additional distinguishing imaging features between benign and malignant lesions. Most MRI-detected and biopsied lesions (benign and malignant) displayed nonmass enhancement (59%) and washout kinetics (45%) among women with minimal background parenchymal enhancement (BPE) (51%) and heterogeneous density (45%) (Figure 2).
Imaging features of MRI lesions.

Chi-square testing was used to compare multiple categorical variables, and a 2-sample t test was used to compare continuous variables. Imaging features were not available for all cases.
Abbreviations: BPE, background parenchymal enhancement; FGT, fibroglandular tissue; MRI, magnetic resonance imaging.
P value was calculated between benign and malignant lesions.

MRI-detected lesions with nonmass enhancement and washout kinetics. (A, B) Fibrocystic changes. (A) T1 Gd-enhanced axial image demonstrates clumped focal nonmass enhancement. (B) Core biopsy showed a mixture of cysts, columnar cell changes, and florid usual ductal hyperplasia. (C, D) DCIS. (C) T1 Gd-enhanced axial image demonstrates clumped segmental nonmass enhancement. (D) Core biopsy showed intermediate nuclear grade DCIS, cribriform pattern, with central necrosis. DCIS indicates ductal carcinoma in situ; MRI, magnetic resonance imaging.
Given the increased biopsy of papillary and sclerosing lesions later in the study period, we further evaluated patient and MRI characteristics of these lesions. Compared with other benign lesions, papillary and sclerosing lesions were more likely to be detected in older patients (mean age: 59 vs 52 years, P < .001) and to display washout kinetics (58% vs 38%) (P = .014). However, there were no significant trends when evaluating imaging features over time.
There was an association between MRI indication (staging vs high-risk screening) and a benign or malignant biopsy diagnosis. From 2004 to 2019, 30% of biopsies performed because of staging MRI yielded a malignant diagnosis compared with 19% of biopsies performed as a result of high-risk screening (P = .001). Within this same time frame, patients with malignant diagnoses were older (mean age: 59 years) compared with patients with benign diagnoses (mean age: 54 years, P < .01).
Discussion
We evaluated trends in histologic diagnoses of breast lesions that were detected and biopsied by MRI over an extended period of time (16 years). The most notable result of the study was that the percentage of benign vs malignant diagnoses remained essentially unchanged throughout the evaluation period, during which the proportion of preoperative breast MRIs decreased relative to the proportion of screening breast MRIs. Our study highlights the continued low specificity of breast MRI and emphasizes the diverse spectrum of benign entities that have overlapping imaging features with malignant lesions.
Regarding specific histologic diagnoses, we found an increasing percentage of papillary and sclerosing lesions detected in benign biopsies; however, the cause of this increase at our institution is unknown. Papillary and sclerosing lesions accounted for 24% of benign biopsies in our review, which is higher than that reported by other institutions (range of 5%-14%).4-6,8 Perhaps, the concurrent decrease in other benign entities such as fibrocystic changes and fibroadenomas suggests that certain imaging features such as T2 hyperintensity might be increasingly used to differentiate benign from malignant enhancing lesions. The trend lines in Figure 1B support this notion, but there was a lack of statistical significance.
Due to the often overlapping histology of intraductal papillomas, radial scars, and complex sclerosing lesions seen on core biopsies, we combined these entities into a single group. A prior detailed subanalysis of these lesions found that complex sclerosing lesions were more likely to have washout kinetics and intraductal papillomas to have a larger proportion of cases with T2 hyperintense features. 12 In this study, we were unable to identify discriminating imaging characteristics of papillary and sclerosing lesions that reliably allow for differentiation from malignant entities. The clinical significance of increased detection of such papillary and sclerosing lesions, which are often considered “high-risk,” remains uncertain with differing outcomes and recommendations.13,14
Cystic apocrine metaplasia is also a relatively common benign finding in MRI-guided breast biopsies, with institutions reporting CAM as representing 10% to 38% of biopsied lesions.2,6,7,15,16 We have previously shown that CAM should be considered when T2-hyperintense enhancing foci or subcentimeter circumscribed masses (with or without washout kinetics) are seen. 10 During the first quarter (2004-2007) of our study, CAM was the prominent histologic finding in 11% of all MRI biopsies, while in the last quarter (2016-2019), CAM only represented 4% of biopsies. Our breast pathologists and breast radiologists participate in monthly pathology-radiology biopsy correlation conference with review of benign and malignant MRI-guided breast biopsies. Such conferences might have increased awareness of benign imaging features of CAM and thereby contributed to the trend of decreased biopsy of CAM over time.
Prior studies have also highlighted the radiologic overlap between benign and malignant lesions. Jabbar et al reported that despite 84% of benign lesions displaying persistent kinetics, many (57%) of their lesions with washout kinetics were also benign. 4 Torous et al described that nearly 80% of malignant nonmass enhancing lesions demonstrated T2 dark signal, but 18% of benign lesions were also T2 dark. 8 Because of this considerable radiologic overlap, most MRI biopsies continue to yield benign findings.
We are entering an era in which the use of abbreviated breast MRI will increase the number of women undergoing annual breast cancer screening. Abbreviated MRI uses a limited number of sequences, thereby reducing costs and improving workflow for radiologists. 17 Relevant to this study, abbreviated MRI does not offer information of enhancement kinetics, which would potentially eliminate biopsy of those benign lesions characterized by suspicious washout kinetics (including many papillary and sclerosing lesions) and improve overall specificity. Increased annual breast MRI screening may also allow for follow-up of small lesions as an alternative to biopsy as our study highlights the smaller size of benign lesions. Kim et al recently reported decreased sensitivity of abbreviated MRI when compared with full diagnostic MRI, but there was improved specificity. 18 Understanding which lesions contribute to false-positive biopsies following abbreviated MRI will have increasing clinical relevance, and future radiology-pathology correlation studies will be needed.
The strengths of this single-institution study are the relatively large number of cases (494), the extended evaluation period (16 years), and central pathology slide review by a breast pathologist. However, there are a few limitations of the study. As noted by Torous et al, multiple histologic alterations are often present within the same case and it can be unclear as to which alteration is responsible for the MRI findings. 8 Central pathology review allows for classification based on the dominant finding present, but cannot fully account for co-existing lesions that have only been partially sampled by the biopsy (and in actuality might be the dominant finding). Finally, the clinical management of the papillary and sclerosing lesions and other high-risk lesions was not fully evaluated; the main objective of this study was to document the distribution of histologic diagnoses over time. Prior reports describe the clinical management (and upgrade rates) of these lesions from portions of this patient cohort.12,19
Conclusions
Most MRI breast biopsies continue to yield benign results. We demonstrated that benign papillary and sclerosing lesions were an increasing source of “false-positive” breast MRIs. Monitoring the distribution of breast MRI biopsy diagnoses over time with radiology-pathology correlation might allow for changes in MRI interpretation and the development of new techniques to improve the specificity of breast MRI.
Footnotes
Acknowledgements
The authors wish to thank Tracy Frazee for assistance with institutional review board submissions and database information retrieval, and Eugene Demidenko, PhD, for statistical consultation.