
Abstract
Background:
The challenge of breast-conserving surgery (BCS) is to remove the entire tumour with free margins and avoid secondary excision that may adversely affect the cosmetic outcome. Consequently, intraoperative evaluation of surgical margins is critical. The aims of this study were multiple. First, to analyse our methodology of intraoperative examination of the resection margins and to evaluate radiological and pathological methods in the assessment of the surgical margins. Second, to evaluate the factors associated with positive margins in our patient population.
M&m:
The data on the resection margin status of 290 patients who underwent BCS for invasive carcinoma or ductal carcinoma in situ (DCIS) between 2009 and 2016 were reviewed.
Results:
In the cohort of BCS with invasive carcinoma, the negative predictive value was 97.4% for intraoperative assessment by radiography and 81.8% for intraoperative assessment by pathology. The re-operation rate among cases without intraoperative assessment was 23.6% compared to 7.3% among cases with intraoperative assessment (P = .003). Margin status was significantly associated with tumour size, histological subtype (invasive lobular carcinoma), and multifocality. In the population of BCS with DCIS, margin status was significantly associated with preoperative localisation and intraoperative margin assessment (P = .03).
Conclusion:
There is no statistical difference between pathological and radiological intraoperative assessment. Tumour size, lobular subtype, and multifocality were found to be significantly associated with positive margins in cases with invasive carcinoma, whereas absence of intraoperative margin assessment was significantly associated with positive margins in cases with DCIS. Therefore, intraoperative margin assessment improves the likelihood of complete excision of the lesion.
Introduction
Breast cancer is the most common type of cancer in women worldwide. 1 The estimated number of new breast cancer cases for 2018 in Belgium was 11 851, with an incidence of 203.7/100 000. 2 Breast-conserving surgery (BCS) has generally been accepted as the treatment of choice for early invasive breast cancer.1,2 The challenge of BCS is to remove the entire tumour with negative margins, as the presence of positive or close margins increases the risk of local recurrence.2-4 Local recurrence is associated with an increased risk of systemic recurrence and poorer survival. 5 Consequently, intraoperative evaluation of surgical margins is crucial for improving oncological resection and avoiding a second surgery that may adversely affect the cosmetic outcome. The aims of this study were multiple. First, to analyse our methodology of intraoperative examination of resection margins and to compare the radiological and pathological assessment of the surgical margins of invasive and ductal carcinoma in situ (DCIS). Second, to evaluate the factors associated with positive margins in our patient population.
Materials and Methods
A total of 290 patients who underwent BCS for invasive carcinoma or DCIS between 2009 and 2016 were reviewed retrospectively. For each patient, the following parameters were assessed: imaging findings, multifocality, method used to localise the lesion (wire, carbon marking or clip; Tables 1 and 2), surgeon, intraoperative margin assessment, tumour size, histology (tumour type, tumour grade, luminal type, nodal status, and margin status), and tumour node metastasis (TNM) classification (8th edition of the UICC TNM classification of Malignant Tumours). 6 The margins were considered as positive in case of tumour cells touching ink in invasive carcinoma, and when tumour cells were identified within 2 mm of the margin in DCIS.4,7 Radiology (mammography or echography) or pathology (macroscopic examination) were used for intraoperative margin assessment. The method was selected at the surgeon’s discretion. In case of microcalcifications, the method used was mammography. In case of a mass or architectural disorganisation, the decision on the method of intraoperative assessment was made on a case-by-case basis by the surgeon or the multidisciplinary team. In case of a mass or architectural disorganisation, mammography or echography was used as radiological evaluation, and macroscopic inspection was used as pathological examination. Frozen sections were performed when there was doubt on the accuracy of the macroscopic evaluation.3,5,8-10 The specimen radiography method includes performing a mammography first. In case of doubt or if the lesion is not visible, ultrasound (US) examination is performed. If the lesion (microcalcification or mass) is <10 mm from the margin, immediate re-excision is performed. In case of pathological evaluation, the specimen is oriented, measured, and inked. Sections are made and the tumour is macroscopically evaluated by the pathologist. The tumour and its distance from the margins are measured. If the edges of the tumour are <10 mm from the margins, immediate re-excision is performed. Frozen-section biopsy (only one section) was performed only in cases of doubt following macroscopic evaluation.3,5,8-10 The study protocol was approved by the Institutional Ethics and Research Review Boards at Erasme Hospital (reference number study P2018/587). All continuous variables were categorised into groups. Fisher’s exact and χ2 tests were used to assess the association between the margin status on final histopathological evaluation and all analysed variables. P < .05 was considered to indicate statistically significant differences. All analyses were performed using Statistica© software.
Invasive carcinoma on BCS: patients characteristics and clinicopathological data.

Abbreviation: NST, no special type.
Pure DCIS on BCS: patients characteristics and clinicopathological data.

Abbreviations: BCS, breast-conserving surgery; DCIS, ductal carcinoma in situ.
Results
Intraoperative margin assessment
The results of margin assessment are summarised in Figure 1. A total of 187 patients with a mass were evaluated, 122 by radiography, and 65 by macroscopic examination. In the group evaluated by radiology, 67% (82/122) had intraoperative positive margins. One patient with peroperatory negative margins had positive margins in the final diagnosis. Therefore, the negative predictive value (NPV) was 97.4% (38/39). For the group evaluated by macroscopic examination, 83.1% (54/65) had peroperatory positive margins. Two cases with peroperatory negative margins had positive margins in the final diagnosis. Of note, all patients with intraoperative positive margins underwent re-excision until the margins were negative. Therefore, the NPV was 81.8% (9/11). This difference in the results between radiology and pathology were not found to be statistically significant. Thus, intraoperative examination reduces the risk of positive margins in the final diagnosis in cases of pure DCIS (P = .03), but not in cases of invasive carcinoma (P = .42; Tables 3 and 4).
Relation between margins status and clinicopathological features in invasive carcinoma.

Bold values are statistically significant (P < .05).
Relation of margins status and clinicopathological in pure DCIS

Abbreviation: DCIS, ductal carcinoma in situ.
Bold values are statistically significant (P < .05).

Results of intraoperative margin assessment with the two techniques.
Clinicopathological characteristics and association with margin status
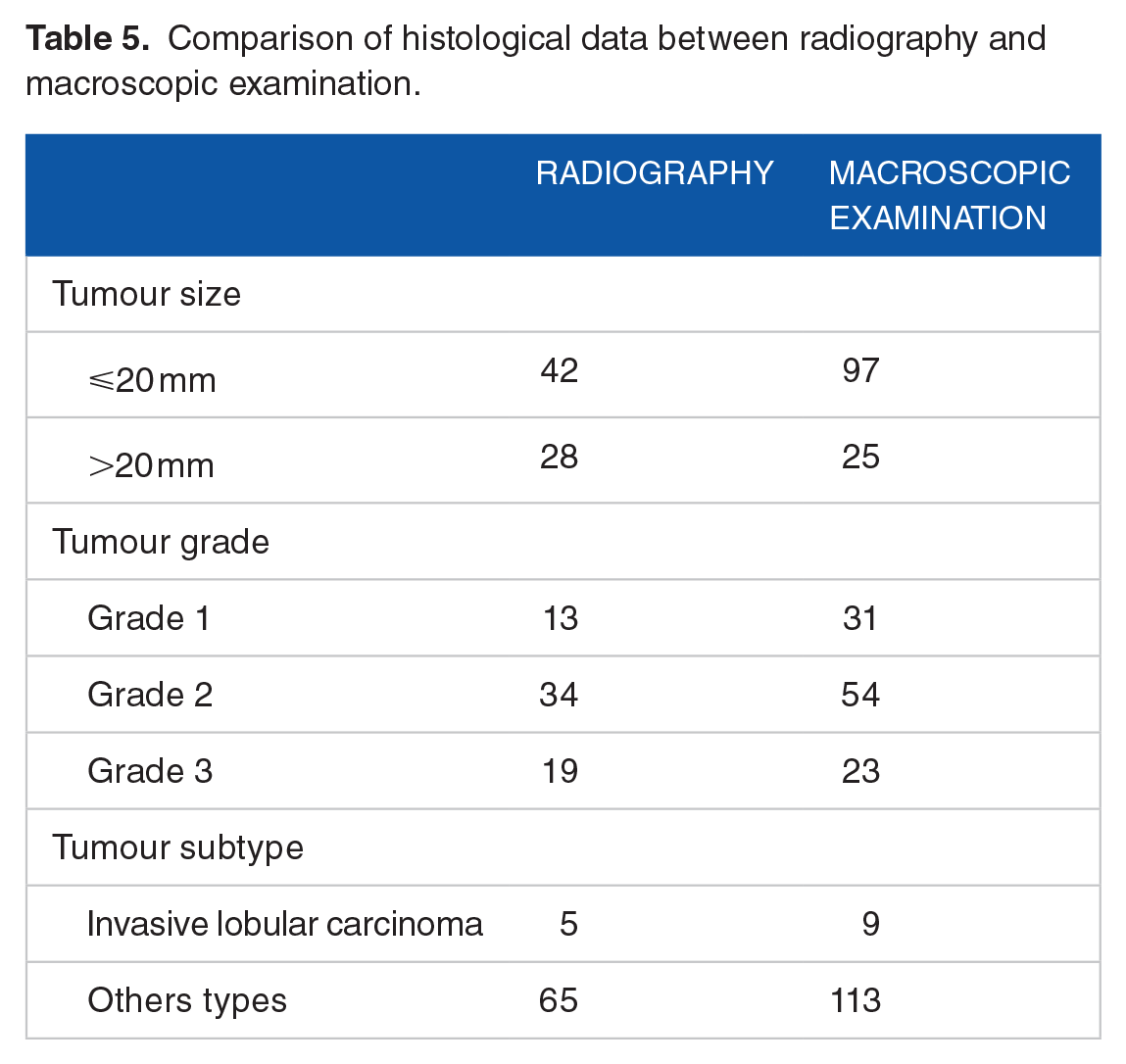
The study was performed on 290 patients who underwent BCS for invasive carcinoma or DCIS between 2009 and 2016. A total of 254 patients had invasive carcinoma on BCS and 36 patients had DCIS without invasion in the final excision (pure DCIS). In the population with invasive carcinoma, the age range of the patients was 28 to 91 years, with a mean age of 60.5 years. The histological subtypes of the surgical specimens were invasive carcinoma of no special type (NST) for 182 patients (72%) and invasive lobular carcinoma for 28 patients (10%). Tables 1 and 2 summarise the clinical and histological characteristics of these 2 study populations. Table 5 shows the tumour characteristics of the subgroups (radiological vs pathological intraoperative margin assessment). In the population with invasive carcinoma, margin status was significantly associated with tumour size (P = .010), histological subtype (presence of invasive lobular carcinoma; P = .005) and multifocality (P = .022; Table 3). The status of the resection margins in cases with invasive carcinoma was not affected by the intraoperative examination (P = .42). The mean tumour size did not seem to be a confounding factor (Table 6). In the population of pure DCIS, the patient age ranged from 40 to 81 years, with a mean age of 58.8 years. Margin status was significantly associated with image-guided preoperative localisation (P = .007) and intraoperative margin assessment (P = .03). No significant association was observed between margin status and clinicopathological data (Table 4). The margins were positive in surgical specimens in the final pathology in 12.6% of the cases (32/254) in the population with invasive carcinoma vs 22.2% of the cases (8/36) in the population with pure DCIS. There was no statistical difference between invasive and in situ carcinoma as regards the risk of positive margins in the final diagnosis.
Comparison of histological data between radiography and macroscopic examination.
Relation between tumour size, margin status and intraoperative assessment.

Reoperation and local recurrence
The global reoperation rate was 7.6%. In the population of invasive carcinomas, 32 patients had positive margins in the final diagnosis, 10 of whom underwent a mastectomy and 9 a second surgery. These 19 patients did not develop local recurrence. A total of 11 patients did not undergo further surgery, 2 of whom presented with local recurrence during the follow-up period (at 52 and 33 months, respectively). Of the 222 patients with negative margins in the final diagnosis, 7 developed a local recurrence over a follow-up period of 8 to 87 months. For this population of invasive carcinomas, the reoperation rate was 7.5% (19/254) and the local recurrence rate was 3.5% (9/254; Figure 2). In the population of pure DCIS, 8 patients had positive margins in the final diagnosis, 2 of whom underwent a mastectomy and 1 re-excision. These 3 patients did not develop local recurrence. The 5 remaining patients did not undergo further surgery, but radiotherapy alone; 2 of them presented with local recurrences (1 invasive carcinoma and 1 carcinoma in situ). Of the 27 patients with negative margins, only 1 developed local recurrence (microinvasive carcinoma). For this population of pure DCIS, the reoperation rate was 8.3% (3/36) and the local recurrence rate was 8.3% (Figure 3). Intraoperative margin assessment was associated with a lower reoperation rate. The global re-intervention rate (invasive and pure DCIS) without intraoperative assessment was 23.6% (10/43) compared to 7.3% (18/247) with intraoperative assessment (P = .003). In the population of pure DCIS, the reoperation rate among cases without intraoperative assessment was 42.9% (3/7) compared to 3.4% (1/29) among those with intraoperative assessment (P = .018). In the population of invasive carcinomas, the reoperation rate without intraoperative assessment was 19.4% (7/36) compared to 7.8% (17/218) with intraoperative assessment, but this difference was not statistically significant (P = .057).

Results of intraoperative margin assessment in case of invasive carcinoma.

Results of intraoperative margin assessment win case of ductal carcinoma in situ.
Discussion
Evaluation of the resection margins in breast cancer is an important criterion for adjuvant treatment after surgery. A number of authors have investigated this subject, we herein aimed to present our experience in this field. Moreover, we use 2 different methods of intraoperative margin assessment. Another factor that is not often studied in the literature is the comparison between surgeons who perform the excision. No statistical difference was identified between surgeons in this study. The rates of positive margins following BCS for invasive or in situ carcinomas are reported to be between 6% and 60% in the literature.8,11,12 Cabioglu et al 5 reported a rate of positive margins of 28% for pure DCIS and 6% for invasive carcinoma. In our study, the global rate of positive margins was 13.8%: 12.6% (32/54) for invasive carcinoma and 22.2% (8/36) for pure DCIS. The distinction between invasive and in situ carcinoma was made because the definition of positive margin differs between the 2. Currently, the margin is considered positive when the tumour cells are touching ink in invasive carcinoma and when they are within 2 mm of the margin in pure DCIS. 3 ,5,7,12,13 This definition was used in this study to categorise the margin status of invasive and in situ carcinomas. Intraoperative assessment of margin status may be performed by pathological examination (macroscopic evaluation, imprint cytology, or frozen section) or by radiography (mammography or echography). Specimen radiography is the method of choice in cases of DCIS, as the majority of these lesions are associated with microcalcifications only visible on mammography, whereas macroscopic evaluation is feasible only for palpable tumours.3,5,8-10,14,15 However, the techniques used across centres are different, and variability in the sensitivity of the different methods has been reported.10,15-17 In our institution, DCIS intraoperative margin status is generally assessed by radiography. Of note, in our population of DCIS, 12 patients had a mass and 7 of them were clearly delineated and palpable. For these patients, the surgeon decided to excise the lesion without intraoperative assessment. Performing an intraoperative margin assessment was statistically associated with negative margins in cases with pure DCIS (P = .03). However, the selected method (radiology or macroscopy) for intraoperative margin assessment did not affect the final margin status in cases with pure DCIS, as only 1 case was assessed by pathological examination (positive margins on final pathology). However, the number of cases with pure DCIS in this study was limited (n = 36). Therefore, the results of this category must be interpreted with caution and comparison with larger-sample studies is recommended.
A total of 17% of the cases of positive margins were without intraoperative margin assessment compared to 11.9% with intraoperative margin assessment in cases of a mass corresponding to an invasive carcinoma. Surprisingly, the status of the resection margins in these cases was not affected by the intraoperative examination (P = .42). Of note, the tumour size (mean) was not a confounding factor in our series (Student’s t-test; P = .3057). These data are interesting, as they may indicate that there is no reason to make an intraoperative examination in case of invasive carcinoma presenting as a mass. However, these findings must be interpreted with caution due to the small number of cases in our study. It would be interesting to differentiate between subtypes of masses (well- or ill-defined, lobulated or spiculated, etc) in larger studies to confirm this hypothesis. This would be important, as all BCS for invasive carcinoma presenting as a mass currently include an intraoperative examination in our institution, which is very time-consuming and costly. Of note, when considering intraoperative margin assessment of tumours presenting as a mass, the NPV of intraoperative assessment by pathology was 81.8%, while it was 97.4% for assessment by radiography, but this difference was not statistically significant, possibly due to the small number of cases. Multiple predictive factors of positive margins have been described. Younger age, larger tumour size, presence of DCIS, high tumour grade, multifocal disease, lobular histology, and axillary node-positive disease are the most frequent factors found in the literature in case of BCS.2,3,5,18 In agreement with these studies, we found that larger tumour size, multifocality, and lobular histology were statistically significantly associated with positive margins for invasive carcinoma. In cases of pure DCIS, absence of preoperative localisation and absence of intraoperative margin assessment were statistically significantly associated with positive margins. DCIS associated with invasive carcinoma was not associated with positive margins in our study. In this study, the global reoperation rate was 9.6%: 9.4% for invasive carcinoma and 11.1% for pure DCIS. Intraoperative margin assessment was statistically significantly associated with a lower reoperation rate in cases of pure DCIS (3.4 vs 42.9%). This result is consistent with our previous results on the association between performing an intraoperative margin assessment and margin status. Our re-operation rate is also consistent with the literature, in which the global reoperation rate ranges between 2.6% and 50%,11,12,19 and the DCIS reoperation rate ranges between 14% and 46%.5,11,17 The goals of this study were to evaluate our own experience with evaluation of margin resection and our own identified risk factors. Our predictive factors of positive margins are consistent with those found in the literature. Therefore, intraoperative assessment of surgical margins by radiology improves the safety of complete excision of the lesions, particularly in cases with pure DCIS, and reduces the risk of reoperation. Larger studies are required to verify our findings, as this was a retrospective study with a small number of DCIS and lacking true comparison between radiological and pathological intraoperative margin assessment.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CK, J-CN, CM, PS, MS, XC made a contribution to the design of the work.
CK, J-CN, CM, PS, MS acquired the data.
CK, XC, J-CN analyzed the data.
CK, CM, MS, XC drafted the manuscript.
J-CN and PS approved the version to be published. All of the authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.