
Abstract
Background:
The impact of certain tumor parameters on the sensitivity of imaging tools is unknown. The purpose was to study the impact of breast cancer histology, tumor grading, single receptor status, and molecular subtype on the sensitivity of contrast-enhanced breast magnetic resonance imaging (CE-BMRI) vs X-ray mammography (XRM) to detect breast cancer.
Materials and Methods:
We ran a supplemental analysis of 2 global Phase III studies which recruited patients with histologically proven breast cancers. The sensitivity of CE-BMRI vs XRM to detect cancer lesions with different histologies, tumor grading, single receptor status, and molecular subtype was compared. Six blinded readers for each study evaluated the images. Results were summarized as the “Mean Reader.” For each reader, sensitivity was defined as the proportion of detected lesions vs the total number of lesions identified by the standard of reference. Two-sided 95% confidence intervals were calculated for within-group proportions, and for the difference between CE-BMRI and XRM, using a normal approximation to the binomial distribution.
Results:
In 778 patients, 1273 cancer lesions were detected. A total of 435 patients had 1 lesion, 254 had 2 lesions, and 77 had 3 or more lesions. The sensitivity of CE-BMRI was significantly higher compared with XRM irrespective of the histology. The largest difference was seen for invasive lobular carcinoma (22.3%) and ductal carcinoma in situ (19%). Across all 3 tumor grades, the sensitivity advantage of CE-BMRI over XRM ranged from 15.7% to 18.5%. Contrast-enhanced breast magnetic resonance imaging showed higher sensitivity compared with XRM irrespective of single receptor expressions (15.3%-19.4%). The sensitivities for both imaging methods were numerically higher for the more aggressive ER– (estrogen receptor), PR– (progesterone receptor), and HER2+ (human epidermal growth factor receptor 2) tumors. Irrespective of molecular subtype, sensitivity of CE-BMRI was 14.8% to 18.9% higher compared with XRM.
Conclusions:
Contrast-enhanced breast magnetic resonance imaging showed significantly higher sensitivity compared with XRM independent of tumor histology, tumor grading, single receptor status, and molecular subtype.
Keywords
Introduction
The introduction of mammography screening was the most important preventive achievement to reduce breast cancer mortality. 1 Today, digital X-ray mammography (XRM) is the standard breast imaging method all over the world. 2 X-ray mammography is a fast and cost-effective imaging tool for breast cancer screening and for detection/characterization of suspicious clinical findings.3,4
There is strong evidence that contrast-enhanced breast magnetic resonance imaging (CE-BMRI) provided higher sensitivity for detection of breast cancer compared with conventional digital XRM.5-12 However, CE-BMRI is in ongoing scientific debate for potentially higher costs per examination, 13 for featuring higher rates of false positive results, 14 over-detection,13,15 increased reoperation rates, 16 and increased mastectomy rates. 17 For these reasons, the European Society of Breast Cancer Specialists (EUSOMA) 18 and the American College of Radiology (ACR)19,20 currently recommend CE-BMRI selectively to address specific clinical questions, eg, screening of high-risk patients,18,20 determining the extent of disease,18,20 and additional evaluation of clinical or imaging findings. 20 Contrast-enhanced breast magnetic resonance imaging and XRM utilize completely different technical approaches to visualize breast tumors. While XRM is based on X-ray attenuation by fibroglandular and tumor tissue, CE-BMRI shows the relaxivity effect of gadolinium on water protons in vessels and the intercellular space. As the grade of malignancy and aggressiveness usually correlates with the ability of the tumor for angiogenesis, 21 we aimed to investigate whether the overall high sensitivity of CE-BMRI is further rising with increasing histopathological criteria for malignancy, ie, in situ/invasive, tumor grading 1 to 3, absence of hormone receptors (estrogen receptor [ER–] and/or progesterone receptor [PR–]), presence of human epidermal growth factor receptor 2 (HER2) receptor, or molecular tumor subtype.
The contrast agent gadobutrol is a macrocyclic, gadolinium-based contrast agent provided in a 1 molar formulation. 22 While approved for a number of indications, including breast imaging (“whole body”), its efficacy in lesion detection and characterization of breast tumors has been confirmed by a number of studies.23-25 As of January 31, 2022, >95.2 million gadobutrol administrations have been performed.
The objective of this supplemental analysis was to assess the impact of breast cancer histology, tumor grading, single receptor status, and molecular tumor type on the sensitivity of contrast-enhanced magnetic resonance imaging (CE-MRI) vs XRM to detect breast cancer.
Materials and Methods
Data sources
This is the second supplemental evaluation of 2 large Phase III studies (GEMMA Program—Gadobutrol-Enhanced MR Mammography) registered on ClinicalTrials.gov (GEMMA1: NCT01067976; GEMMA2: NCT01104584; here abbreviated as “G1” and “G2”). 6
Study population and interventions
Sardanelli et al 6 published the primary outcomes of both studies, including details on the study population and the interventions. Studies G1 and G2 included 390 and 397 patients, respectively. G1 recruited in 7 countries (Colombia, Finland, Germany, Italy, South Korea, Switzerland, and United States) (28 centers); G2 in 8 countries (Argentina, Canada, Germany, India, Poland, Spain, Taiwan, and United States) (39 centers.). The mean age was 55.7 years (G1) and 57.1 years (G2). About 3/4 were white patients, and 1/4 were Asian patients. 6
Patient inclusion criteria were a newly detected and histologically proven breast cancer (but not marked with a biopsy clip) and a most recent XRM. All patients eligible for the study underwent a supplemental CE-BMRI at 1.5 Tesla. Gadobutrol (Gadovist 1.0 mmol/mL, Bayer AG, Leverkusen, Germany) was applied intravenously at a dose of 0.1 mmol/kg body weight.
Standard of truth (SOT) consisted of a documented histopathological confirmation for regions harboring malignancy and a combination of a negative pathology report, mammography, and, if available, ultrasound for cancer-free regions.
Two SOT-committees (1 for each trial) and 6 blinded readers per study were working on the GEMMA trials. They evaluated the reports on XRM, BMRI, and histopathology and focused on lesion mapping. For this supplemental analysis, a post hoc readout of the available histopathology reports was performed, providing data on tumor histology, grading, and receptor status.
Blinded reading
The blinded reading consisted of 2 parts: Part 1 and Part 2. In Part 1, the unenhanced BMRI and the combined unenhanced and CE-BMRI images were evaluated in a randomized fashion.
After the evaluation of the unenhanced BMRI images and lock of the case report form (CRF) entries, the respective XRMs were added and evaluated together with the unenhanced BMRIs. After a break of at least 2 weeks, the same process was applied to the combined unenhanced and CE-BMRIs, ie, first evaluation of the combined unenhanced and CE-BMRIs and lock of the CRF entries. Then the respective XRMs were added, and the readers evaluated the combined unenhanced and CE-BMRI plus XRM image sets together. These evaluations were performed by 3 independent BMRI readers who were also experienced in XRM reading.
In Part 2, the XRM image sets were evaluated by 3 independent blinded readers, specialized in XRM evaluation.
Target variables
The primary target variable of this supplemental analysis was the sensitivity of CE-BMRI vs XRM for detection of breast cancers with different tumor histologies (ductal carcinoma in situ [DCIS], invasive lobular carcinoma [ILC], invasive ductal carcinoma [IDC], and mixed), tumor grading (grades 1-3), single receptor status (estrogen receptor [ER], progesterone receptor [PR], either ER and/or PR hormone receptor [HR], human epidermal growth factor receptor 2 [HER2]), and molecular subtypes (HER2-HR+, HER2+, triple negative [TN]). The molecular subtypes analyzed in this study are shown in Table 2.
Statistics
The primary statistical analysis of interest was sensitivity. Lesions identified by the SOT-committee were considered to be true cancers. Lesions identified as cancers by the SOT-committee and the readers were true positives (TPs). Lesions identified by the SOT-committee but not by the readers as cancers were false negatives (FNs). Sensitivity (TP/(TP + FN)) was defined as the proportion of lesions detected as cancers by the readers (TP) from the total number of lesions identified by the SOT-committee (TP + FN).
Sensitivity as described here was calculated for each reader individually. To reduce the variability associated with multiple readers, mean reader sensitivity was reported. Mean reader sensitivity was calculated as the mean of the sensitivity values for the 6 readers across the 2 studies. Patients were included in the analyses if they had at least 1 lesion identified by the standard of reference and had data available for the subgroup of interest. The 2-sided 95% confidence intervals (CIs) were calculated for within-group proportions using a normal approximation to the binomial distribution. The 2-sided 95% CIs for the difference between CE-BMRI and XRM were also calculated using the normal approximation to the binomial distribution. 26 No statistical adjustments were made for multiple comparisons, and no formal threshold for statistical significance was declared.
Results
Study population
This supplemental analysis included 778 patients with a total of 1273 cancer lesions. All patients had at least 1 index cancer. For 766 patients, histologies are available. A total of 435/766 patients (56.8%) had 1 lesion, 254 (33,2%) had 2 lesions, and 77 (10.1%) had 3 or more lesions. Thirty (4%) patients had bilateral lesions.
Of the 331 (43.2%) patients with multiple lesions, 307 patients had lesions with identical histology and 24 patients with more than 1 histology. The histologies of patients with 1 and 2 or more lesions are shown in Table 1.
Number of patients ⩾1 lesion and tumor histologies (n = 766, 1273 lesions, 30 patients with bilateral tumors).
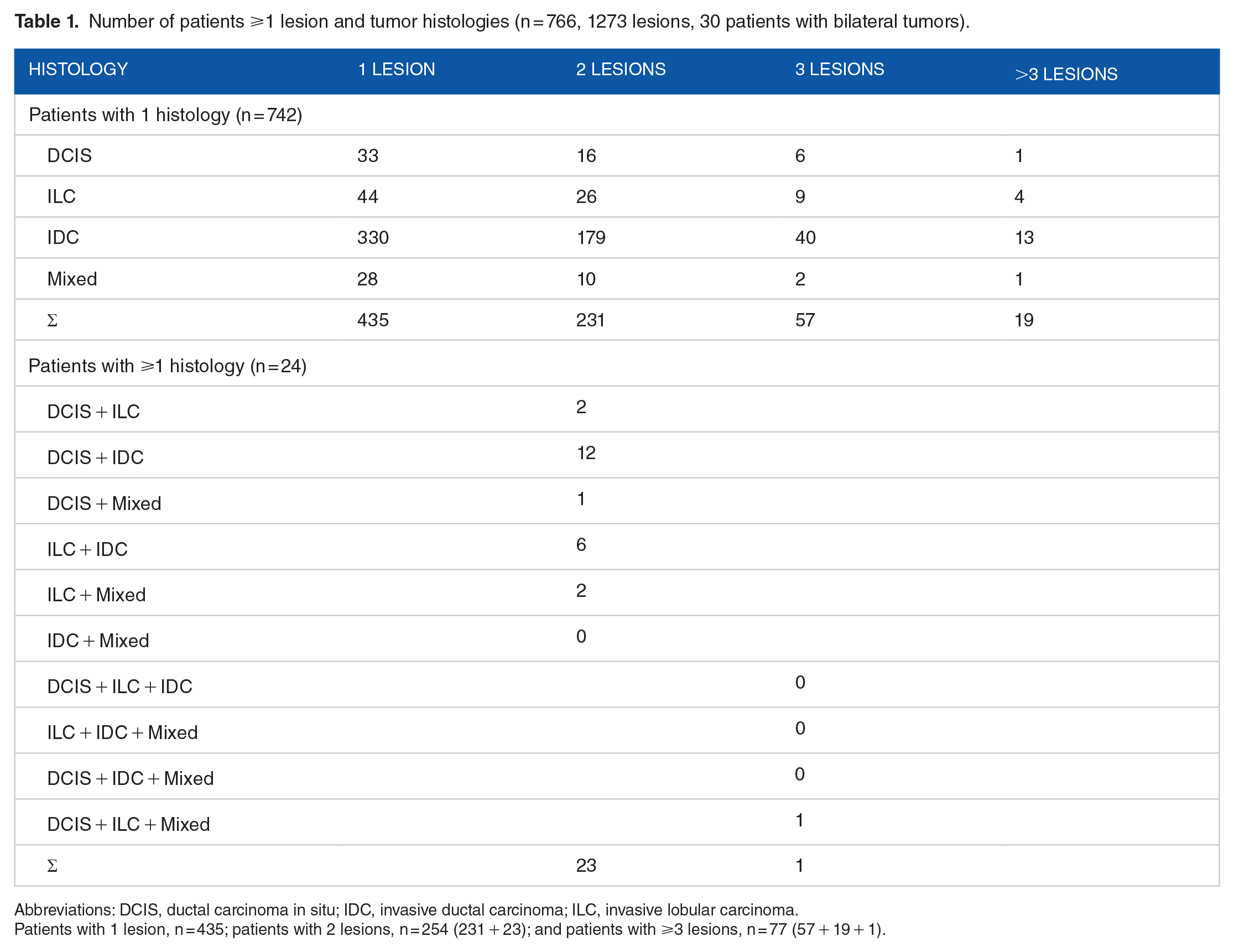
Abbreviations: DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma.
Patients with 1 lesion, n = 435; patients with 2 lesions, n = 254 (231 + 23); and patients with ⩾3 lesions, n = 77 (57 + 19 + 1).
The study population has been described in detail by Sardanelli et al. 6
Histology
The sensitivity of CE-BMRI was significantly higher compared with XRM across the 3 histological types. Sensitivity of CE-BMRI ranged from 72.8% to 85.1%, and sensitivity of XRM ranged from 53.8% to 69.7%. The largest difference between both imaging modalities was seen for ILC (22.3%) and DCIS (19%) (Figure 1).

Sensitivities of CE-BMRI vs XRM by tumor histology (n = 1231 cancer lesions) (% [±95% CI]). *95% CIs do not overlap. CE-BMRI indicates contrast-enhanced breast magnetic resonance imaging; CI, confidence interval; DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; XRM, X-ray mammography.
Tumor grading
A similar trend was seen for tumor grading. CE-BMRI sensitivity ranged from 77.0% to 85.4%, and XRM sensitivity ranged from 61.3% to 68.4%. The difference between both modalities ranged from 15.7% to 18.5% in favor of CE-BMRI. For all grades, the CI did not overlap (Figure 2).

Sensitivities of CE-BMRI vs XRM by tumor grading (% [±95% CI]). *95% CIs do not overlap. CE-BMRI indicates contrast-enhanced breast magnetic resonance imaging; CI, confidence interval; XRM, X-ray mammography.
Single receptor status
Contrast-enhanced breast magnetic resonance imaging showed significantly higher sensitivity compared with XRM irrespective of single receptor expressions. The difference ranged from 15.3% to 19.4%. The sensitivities for both imaging methods were numerically higher for ER–, PR–, and HER2+ tumors compared with ER+, PR+, and HER–, respectively (Table 3).
Molecular types of breast cancer
For 777/1273 (61%) lesions, the complete receptor status (HER2, ER, PR) was available. The majority of lesions (n = 546/777; 70.3%) were HER2-HR+, followed by HER2+ (150; 19.3%) and TN (81; 10.4%) (Table 2).
Molecular subtypes.

Abbreviations: ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor.
Irrespective of molecular subtype, the sensitivity of CE-BMRI was higher compared with XRM. The sensitivity range was 81.5% to 86.8% for CE-BMRI, the one for XRM was 62.6% to 70.0%. The highest difference between both imaging modalities was seen for HER2-HR+ tumors (18.9%) (Figure 3).

Sensitivities of CE-BMRI vs XRM by molecular subtype (% [±95% CI]). *95% CIs do not overlap. CE-BMRI indicates contrast-enhanced breast magnetic resonance imaging; CI, confidence interval; HER2, human epidermal growth factor receptor 2; TN, triple negative; XRM, X-ray mammography.
Discussion
In this supplemental analysis, we compared sensitivities of CE-BMRI vs XRM for detecting breast cancer lesions with different histologies, tumor grades, single receptor status, and molecular tumor subtypes. The main results 6 and analyses by breast density were published elsewhere. 27 The evaluation was done on a pooled database of 2 large Phase III studies.
Histology
There are 4 major histological types of breast cancer: (1) DCIS, (2) ILC, (3) IDC (most frequent type), 28 and (4) mixed tumors. DCIS is a preinvasive cancer that has not so far crossed the basal membrane of the milk ducts. 29 However, this early nonmass lesion is hard to detect with imaging methods.
Irrespective of histology, sensitivity of CE-BMRI was consistently higher compared with XRM, in particular in DCIS, showing 19% more lesions (Figure 1).
Riedel et al studied 327 patients at high risk for breast cancer in a prospective study applying XRM, ultrasound, and CE-BMRI and relating sensitivities to histopathologic evaluation. They found sensitivities for these 3 imaging modalities of 50%, 42.9%, and 85.7%, respectively (P < .01). Interestingly, CE-BMRI detected not only significantly more invasive but also significantly more preinvasive cancers (DCIS), a trend we could confirm with our data here. Riedel et al 30 conclude that CE-BMRI not only improves the detection of invasive cancers but also improves the detection of preinvasive cancers and premalignant lesions, and therefore should become an integral part of breast cancer surveillance in high-risk patients.
Similarly, Preibsch et al 31 reported a diagnostic advantage of CE-BMRI in 123 patients with biopsy-proven, pure DCIS who got an additional CE-BMRI after suspicious XRM. DCIS was occult on XRM in 24.4% (30/123 patients) but only in 1.6% (2/123 patients) on CE-BMRI.
Also Kriege et al analyzed tumor histology in 50 lesions of 1909 women. Sensitivity of CE-BMRI was 100% for lobular and tubular cancers. Sensitivity of XRM was 25% and 0%, respectively. 32 In contrast, Sung et al 33 found that CE-BMRI detected more likely invasive cancers whereas XRM more DCIS, possibly because of their microcalcifications.
Tumor grading
Histological grading is based on morphological assessment of biological characteristics of the tumor and is one of the best established prognostic factors for breast cancer patients. 34 The Nottingham Grading System distinguishes between well-differentiated tumors (Grade 1), moderately differentiated tumors (Grade 2), and poorly differentiated tumors (Grade 3).28,34 Prognosis deteriorates with increasing tumor grading. 29
In the present study, sensitivity of CE-BMRI was significantly higher compared with XRM for all grades (Figure 2).
The literature search identified 2 studies on this topic. Kriege et al (see above) showed consistently higher sensitivities of CE-BMRI vs XRM for all tumor grades—Grade I: 69% vs 39%, Grade II: 100% vs 50%, and Grade III: 78% vs 44%. 32 Somewhat close to this topic, Riedel et al reported tumor details of 28 cancers in 327 patients. Twelve patients had G2 cancers, and 9 patients had G3 cancers. In 11 of these cases, CE-BMRI showed a higher Breast Imaging Reporting and Data System (BI-RADS) scores compared with mammography and ultrasound, 30 thus providing better characterization of tumor malignancy. We tentatively suggest that higher grading, ie, higher malignancy, is correlated with higher tumor vascularization, which is the basis for CE-BMRI lesion enhancement.
Receptor status
Estrogen receptor and/or PR expression is one of the most important prognostic and predictive immunohistochemical markers. Cancer lesions may express 4 profiles of hormone receptors: ER+/PR+, ER−/PR−, ER+/PR−, and ER−/PR+. 35 The gene that encodes HER2 is overexpressed in approximately 20% of newly diagnosed breast cancers. HER2+ tumors are more aggressive than HER2– ones, 36 but TN cancers are the most aggressive ones. 37 In the first step, single receptor expressions were analyzed with respect to the impact of sensitivity of the 2 imaging tools.
Contrast-enhanced breast magnetic resonance imaging showed a significant higher sensitivity compared with XRM irrespective of receptor status. Numerically, sensitivity of both tools was higher for the more aggressive tumors, ie, higher for ER– or PR– compared with ER+ and PR+ and for HER2+ vs HER2– (Table 3).
Sensitivities of CE-BMRI vs XRM by single receptor expression.

Abbreviations: CE-BMRI indicates contrast-enhanced breast magnetic resonance imaging; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; XRM, X-ray mammography.
Only 1 study related to this topic was identified in the literature search. Kriege et al reported higher sensitivities of CE-BMRI vs XRM for ER– and ER+ tumors: 79% vs 29% and 83% vs 35%.
Lack of ER and PR expression indicates that the tumor cells have lost resemblance to normal glandular cells and are therefore more malignant. In addition, tumors of higher malignancy are also known to be better vascularized due to more effective neo-angiogenesis. For example, in our study, sensitivity of CE-BMRI was 87.3% and 82.2% for ER– and ER+ tumors, respectively. This might be the reason for the higher sensitivity for CE-BMRI that visualizes vessels but not for XRM. With respect to HER2+ expression, also a sign of higher malignancy, CE-BMRI showed a sensitivity of 87.1% vs HER2– cancers with 81.5%. As these differences are small, larger studies are needed to elucidate whether there is an impact of receptor expression on sensitivity of CE-BMRI.
Molecular subtypes
Molecular subtype classifications vary in the literature; however, all are based on the receptor expression of HER2, ER, and PR and on the growth factor Ki67.38-40 As Ki67 was not determined in the framework of the GEMMA studies, the classification used by Harbeck et al 40 was applied: HER2–/HR+, HER2+, and TN. Malignancy increases and prognosis gets increasingly worse from HER2–/HR+ to TN.38,41
Irrespective of molecular subtype, sensitivity of CE-BMRI was higher compared with XRM.
Wu et al investigated potential association between CE-BMRI and XRM imaging characteristics and molecular subtypes of breast cancer in 300 Chinese patients. On XRMs of luminal cancers, they saw “clustered calcification distribution,” “nipple invasion,” or “skin invasion,” and in basal-like tumors more “rim enhancements.” On CE-BMRIs, they described an association between HER2+ cancers with persistent enhancement in the delayed phase. 42
Sung Eun Song et al published a retrospective comparative study on CE-BMRI and XRM imaging features of HER2+ breast cancers according to hormone receptor status. While survival, pattern of recurrence, and treatment (neo-adjuvant) response differ between HER2+/HR+ vs HER+/HR– remarkably (and are hard to predict43,44), they did not find any differences in mammographic imaging presentations and calcification features and magnetic resonance (MR) kinetic features by a computer-aided diagnosis (CAD). 45 However, no direct comparison of sensitivities of the 2 imaging tools was reported.
Finally, the fact that tumor histology, tumor grading, single receptor status, and molecular subtype did not affect the degree of sensitivity increase of CE-BMRI over XRM was not expected. Initially, we assumed that the benefit of CE-MRI would increase with malignancy, as malignancy is closely linked to vascularization. Highly vascularized tumors grow faster, and their vessels are clearly visualized by CE-MRI, while poorly vascularized tumors grow slower and sometimes necrotize in the tumor center, which is as seen microcalcifications in XRM.
Limitations
Some limitations of our study need to be acknowledged: (1) this was a supplemental analysis, not planned prospectively as part of the clinical trial analysis plan; (2) Ki67 was not collected; (3) total sensitivities were generally lower than in daily clinical practice, due to the somewhat artificial Phase III image reading setting. All readers based their diagnosis solely on the images. They were not provided with any further information on the patients’ medical history, clinical examination, or other diagnostic findings. (4) The number of patients in some subgroups was small. (5) Although increasingly popular, neither artificial intelligence applications nor radiomics have been used.46,47
Conclusions
Contrast-enhanced breast magnetic resonance imaging showed significantly higher sensitivity compared with XRM independent of tumor histology, tumor grading, single receptor status, and molecular subtype.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GS and JB declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. JE, DH, OW and ZJT are Bayer employees.
Author Contributions
JE: Study protocol, evaluation strategy, writing manuscript, final approval, full accountability
GH: Study protocol, evaluation criteria, drafting manuscript, final approval, full accountability
DH: Statistical strategy, data processing, drafting manuscript, final approval, full accountability
OW; Drafting manuscript, final approval, full accountability
ZJ: Initial study protocols, initial study conduct, manuscript review, final approval, full accountability
JB: Study protocol, evaluation, drafting manuscript, final approval, full accountability