
Abstract
Improvements in survival of patients with breast cancer have been attributed to the development of agents that target key components of dysregulated pathways involved in oncogenesis and progression of breast cancer. Aberrant mammalian target of rapamycin (mTOR) activation has been implicated in oncogenesis, angiogenesis, and the development of estrogen independence and resistance to chemotherapy in breast tumors. Several mTOR inhibitors (sirolimus, everolimus, temsirolimus, and ridaforolimus) have demonstrated antitumor activity in breast cancer cells. Combining mTOR inhibitors with endocrine therapies has demonstrated clinical antitumor activity in patients with metastatic breast cancer. In addition, mTOR inhibitor combinations with various targeted biologic agents or cytotoxic chemotherapeutic agents are being examined in more than 40 clinical trials with some early promising results. Combination therapies targeting multiple components of these central signaling pathways may be an optimal treatment strategy for patients with advanced breast cancer.
Introduction
Improvements in overall or disease-free survival of patients with breast cancer have been attributed in part to the identification of dysregulated cell signaling pathways and the recent development of therapies that target key components of these pathways. 1 Some of these targets include vascular endothelial growth factor (VEGF) and its receptors (VEGFRs), epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2), and insulin growth factor receptors (IGFRs). 2 Monotherapy drug strategies aimed at these targets have yielded modest results in breast cancer trials, and many patients subsequently develop resistance to these agents. Despite these limitations, the role of cell signaling among these various pathways is clearly evident. Therapeutic agents in combination that target the aforementioned growth factors and/or their receptors represent an area of active investigation that has produced promising results, with some notable exceptions. 2
Mammalian target of rapamycin (mTOR) is a serine/threonine kinase that integrates multiple signals from growth factors and hormones3,4 and plays a central role in the control of cell growth, proliferation, and angiogenesis.4,5 Aberrant mTOR activation has been implicated in oncogenesis, angiogenesis, and the development of drug resistance in tumor cells.6–9 A high proportion of breast tumors exhibit constitutive activation of the mTOR pathway. 10 Convergence of multiple signaling pathways toward a central mediator, such as mTOR, lends itself to the hypothesis that targeting multiple pathways, including mTOR, with different classes of agents may be a more effective treatment strategy than monotherapy approaches. 11 Several mTOR inhibitors have been developed and evaluated in combination with chemotherapy, hormonal therapies, and other targeted biologic agents to investigate the utility of combination therapy for patients with advanced breast cancer.
Overview of the mTOR Pathway
Endocrine and growth factor receptors involved in the pathogenesis of breast cancer have been shown to activate mTOR through phosphoinositide 3-kinase (PI3K)/Akt signaling (Fig. 1).12,13 Multiple upstream signaling components of this pathway, such as the estrogen receptor (ER), 14 the receptor tyrosine kinase HER2, 15 VEGFR, IGF-1R, phosphatase and tensin homolog (PTEN), Akt (also known as protein kinase B), 16 PI3K, and the PI3K catalytic subunit (PI3KCA), 17 become deregulated in breast cancer and are thought to play a role in its development and progression.18,19 Therefore, inhibiting mTOR potentially interferes with breast cancer progression at multiple levels. Preclinical evidence demonstrates that the PI3K/Akt/mTOR pathway is involved in the response of breast cancer cells to hormonal therapies, 13 chemotherapy, 20 and targeted agents.21,22 Members of the EGFR family, including HER2, use the PI3K/Akt/mTOR pathway to promote cell growth and survival. 22 Overexpressed in approximately 20% of invasive breast cancers and associated with a poor prognosis,23,24 HER2-mediated activation of the PI3K/Akt/mTOR pathway is predictive of tumor progression in breast cancer 22 and has been implicated in angiogenesis and metastasis of breast cancer cells. 15 Trastuzumab, a monoclonal antibody that binds to the extracellular domain of HER2, has been shown to diminish HER2-mediated signaling, including activation of the PI3K/Akt/mTOR pathway in vitro. 25 In HER2-positive breast cancer cell lines, trastuzumab inhibited the feedback loop activation of Akt. 26 In addition, lapatinib, a specific dual inhibitor of HER2 and EGFR tyrosine kinase activity, has been shown to induce cell cycle arrest and apoptosis by inhibiting HER2-activated signaling pathways including PI3K/Akt/mTOR. 27

The PI3K/Akt/mTOR pathway. 13
In cells demonstrating trastuzumab resistance, amplified signaling through both the PI3K/Akt/mTOR and MAPK pathways is evident in the presence of elevated levels of activated receptor tyrosine kinase Eph receptor A2 (EphA2). 28 Involvement of the mTOR pathway in HER2-positive trastuzumab-resistant patients is further supported by preliminary biomarker analyses from the neoadjuvant phase 3 GeparQuattro study (NCT00288002), 29 evaluating the addition of capecitabine and/or trastuzumab (in HER2-positive patients only) to epirubicin/cyclophosphamide followed by docetaxel combination chemotherapy. Increased levels of phosphorylated eIF4E-binding protein (4E-BP1), a substrate of mTOR, have been detected in the HER2-positive cohort of patients resistant to trastuzumab-cytotoxic therapy. 30 This contribution of mTOR to resistance will be further validated in the ongoing phase 3 GeparQuinto study (NCT00567554) 29 investigating the integration of bevacizumab, everolimus, and lapatinib into neoadjuvant chemotherapy regimens.
Approved and investigational mTOR and mTOR combination inhibitors.

The effectiveness of everolimus is based on an analysis of change in SEGA volume. Clinical benefit, such as improvement in disease-related symptoms or increase in overall survival, has not been demonstrated.
A key component of the mTOR pathway is the lipid kinase PI3K, which affects survival, proliferation, growth, shape, migration, and intracellular sorting in tumor development. 40 Three classes of PI3K enzymes, designated I to III, have been identified; members of PI3K class I have been implicated in the mTOR pathway and are a focus of potential therapy for solid tumors. 40 Agents such as BEZ235, PI-103, and XL765 are dual PI3K/mTOR inhibitors, which may bypass feedback loops, potentially increasing their efficacies. 41 These agents are currently being evaluated in clinical trials and may provide targeted therapeutic combinations that are effective against solid tumors.18,41
Approved and Investigational mTOR Inhibitors
Several mTOR inhibitors have been developed and evaluated as antitumor therapies, with some distinctive differences in metabolism, formulation, and schedule of administration (Table 1).32,38,42 Three agents have received United States Food and Drug Administration (FDA) approval (sirolimus, everolimus, and temsirolimus), and two of these (sirolimus and everolimus) are oral agents. Sirolimus (rapamycin), an agent that partially inhibits mTOR,
43
is approved for the prevention of kidney transplant rejection and has been investigated in combination with various agents to determine its clinical activity in breast cancer (Fig. 2A).29,44,45 Analogs of sirolimus demonstrating more favorable pharmacokinetics include temsirolimus, everolimus, and ridaforolimus (formerly deforolimus) (Fig. 2B–D).42,46,47 Temsirolimus, approved for the treatment of advanced renal cell carcinoma (RCC),
46
is a prodrug, and its primary active metabolite is rapamycin (half-life approximately 17 to 55 hours).
46
In breast cancer trials, as for RCC, temsirolimus is administered by a weekly intravenous infusion. Everolimus (half-life approximately 30 hours), another analog of sirolimus, is approved for the treatment of advanced RCC and progressive neuroendocrine tumors of pancreatic origin (PNET) at a dosage of 10 mg/day, adults with renal angiomyolipoma and tuberous sclerosis complex (TSC) not requiring immediate surgery at a dosage of 10 mg/day, and subependymal giant cell astrocytomas (SEGAs) associated with tuberous sclerosis at a dosage of 5 mg/day.
47
Everolimus recently (July 2012) received FDA approval for the treatment of postmenopausal women with advanced hormone receptor-positive, HER2-negative breast cancer in combination with exemestane after failure of treatment with letrozole or anastrozole at a dosage of 10 mg/day.
47
Ridaforolimus remains an investigational analog of sirolimus (half-life 49 hours) that is administered orally in breast cancer trials at 40 mg/day for 5 days/week (NCT01234857, NCT01220570, and NCT00736970).29,48 Overall, these different mTOR inhibitors share class-specific toxicities such as stomatitis, noninfectious pneumonitis, infection, hyperglycemia, and dyslipidemia.45–48
Sirolimus.
45
Everolimus.
47
Temsirolimus.
46
Ridaforolimus.
42




mTOR Inhibition in Combination with Chemotherapy
A variety of chemotherapeutic regimens are used in the treatment of patients with metastatic breast cancer (mBC); however, most tumors eventually develop resistance, necessitating a change in treatment. Because the mTOR pathway is upregulated in many chemoresistant cancers, mTOR inhibitors are a logical choice to resensitize tumor cells to chemotherapy or delay the development of treatment resistance by these upregulated or mutated key pathways.
Preclinical Evidence
Preclinical studies suggest that one mechanism of chemoresistance to paclitaxel and carboplatin is overexpression of HER2. 49 In breast cancer models with HER2 overexpression, the combination of an mTOR inhibitor with paclitaxel, carboplatin, or vinorelbine enhances apoptosis of the cells in vitro and antitumor efficacy in mouse xenograft models in vivo compared with either agent alone. 49 Moreover, the combination of mTOR inhibitors with cytotoxic agents demonstrates synergistic antiproliferative cellular activity irrespective of HER2 signaling, further suggesting the potential clinical utility of combination therapy for patients with breast cancer that has become resistant to chemotherapy. 49
Clinical Studies in HER2-Positive and HER2-Negative mBC
Registered combination clinical trials of everolimus in patients with HER2-positive breast cancer. 29
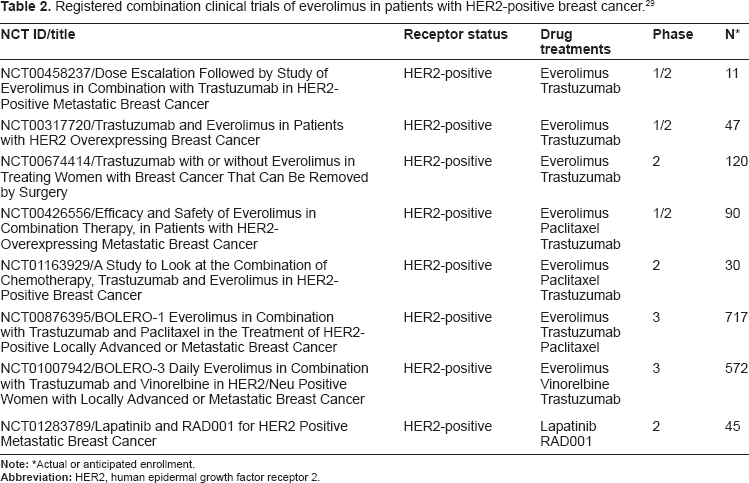
Actual or anticipated enrollment.
Registered combination clinical trials of everolimus in patients with HER2- and/or triple-negative breast cancer. 29

Actual or anticipated enrollment.
Registered combination clinical trials of everolimus in patients with HER2-negative hormone receptor-positive breast cancer. 29

Actual or anticipated enrollment.
Registered combination clinical trials of everolimus in patients with receptor status not specified. 29

Actual or anticipated enrollment.
Registered combination clinical trials of other mTOR inhibitors in patients with breast cancer. 29

Actual or anticipated enrollment.
Registered combination clinical trials of temsirolimus in patients with breast cancer. 29

Actual or anticipated enrollment.
mTOR Inhibition in Combination with HER2-Targeted Therapy
As discussed, trastuzumab with or without an Akt/mTOR pathway inhibitor25,26 and lapatinib
27
have been shown to exert antitumor effects by inhibiting HER2-activated signaling pathways, including PI3K/Akt/mTOR. A combination of HER2-targeted agents and mTOR inhibitors has demonstrated antitumor activity in resistant breast cancer cells, suggesting that mTOR inhibitors may have the potential to delay or prevent acquired resistance to HER2-targeted agents.
57
Furthermore, PI3K pathway activation due to low expression/loss of function of PTEN and/or mutations in the
Preclinical Evidence
Preclinical studies in HER2-overexpressing mouse tumors and cell lines suggest that PI3K/Akt/mTOR pathway inhibition is required for optimal antitumor effects of HER2 antagonists 57 and may be a clinically applicable strategy for overcoming trastuzumab resistance caused by hyperactivation of the PI3K pathway due to PTEN deficiency.20,26 In vitro, low doses of everolimus significantly increased growth inhibition by trastuzumab; everolimus also enhanced the antitumor efficacy of trastuzumab in vivo in mouse xenograft models. 26
Clinical Studies
Results of phase 1 studies in patients with HER2-overexpressing mBC resistant to trastuzumab showed that everolimus is well tolerated in combination with trastuzumab and paclitaxel or vinorelbine and that the combination had antitumor activity and formed the basis of the now closed,50,51 previously mentioned phase 3 trials of everolimus with chemotherapy and trastuzumab in patients with HER2-positive mBC (BOLERO-1 [NCT00876395], BOLERO-3 [NCT01007942]). 29 As noted above, several clinical studies are exploring the potential of everolimus as well as other mTOR inhibitors for improving the efficacy of, or overcoming resistance to, HER2-targeted therapy as outlined above with sirolimus and temsirolimus. These combinations of an mTOR inhibitor with select antimicrotubule agents demonstrate antitumor activity in patients refractory to both trastuzumab and taxanes. 50
mTOR Inhibition in Combination with Endocrine Therapy
The ER is expressed in approximately 30% of premenopausal patients with breast cancer and 60% to 70% of postmenopausal patients with breast cancer and has a significant role in cancer cell proliferation and metastasis.59–62 Approximately 30% of patients with ER-positive breast cancer are intrinsically resistant to hormonal therapies, and the remainder of patients eventually acquire resistance to hormonal therapy.
63
In 25% of primary breast cancers, mutations in
Preclinical Evidence
In preclinical breast cancer models using MCF-7 cells with constitutively active Akt/mTOR that exhibit hormone and chemotherapy resistance, mTOR inhibitors enhanced the efficacy of selective ER modulators tamoxifen, raloxifene, and ERA-923 67 ; the ER downregulator fulvestrant 66 ; and the aromatase inhibitor letrozole. 68 In addition, dual inhibition of mTOR and ER signaling in cellular models of breast cancer was shown to have a synergistic effect on cell cycle arrest and induction of apoptosis. 69 The strategy of combination therapy of a selective ER modulator with rapamycin or temsirolimus has also been shown to restore sensitivity to endocrine therapy in breast cancer cells and may be attributed to the return of normal apoptotic response to endocrine therapy. 70 In fact, the BOLERO-2 trial was based on the preclinical combination therapy data with letrozole plus everolimus shown to restore sensitivity to letrozole in breast cancer cells by inhibiting cell cycle progression and triggering apoptotic cell death. 68 Additionally, a phase 1 dose-escalating study that evaluated everolimus plus letrozole in postmenopausal women or men with stable mBC or progression after ≥ 4 months of first- or second-line therapy with letrozole alone found that an everolimus dose of 10 mg/day provided antitumor activity with no pharmacokinetic interactions. 71
Clinical Studies
Several clinical studies have explored and reported results for the potential of mTOR inhibitors to improve efficacy or overcome resistance to endocrine therapy. Recently reported robust results from the international randomized, placebo-controlled, phase 3 study (BOLERO-2, NCT00863655) have generated the most enthusiasm and excitement for the further advancement of mTOR inhibitors in breast cancer. The first of the BOLERO trials evaluating everolimus in mBC, BOLERO-2, evaluated the combination of everolimus and exemestane in patients with ER-positive mBC refractory to letrozole or anastrozole, demonstrating that the addition of everolimus to exemestane significantly improved PFS (Table 4).
29
In an interim analysis, median PFS was 6.9 months for everolimus plus exemestane compared with 2.8 months for exemestane plus placebo, corresponding to a 57% reduction in the hazard ratio (HR = 0.43, 95% confidence interval [CI], 0.35–0.54,
Positive results for TAMRAD, a randomized phase 2 trial of 111 patients investigating the combination of tamoxifen and everolimus in patients with hormone receptor-positive or progesterone receptor-positive and HER2-negative mBC previously treated with an aromatase inhibitor and any numbers of previous chemotherapies, were recently reported.
77
In the intent-to-treat analysis, the clinical benefit rate in the tamoxifen and everolimus group was 61.1% (95% CI, 46.9–74.1) versus 42.1% (95% CI, 29.1–55.9) in the tamoxifen-only group, yielding a clinically significant difference (
mTOR inhibition, in combination with the selective ER downregulator fulvestrant, has also demonstrated promising activity in patients with metastatic ER-positive breast cancer in which aromatase inhibitors were not effective. Interim results from this ongoing, single-arm, phase 2 study demonstrated a median time to progression of 8.6 months (of 11 evaluable patients, 7 had stable disease and 1 had partial response). 78
In earlier-stage disease, letrozole plus everolimus or letrozole plus placebo was recently tested in a randomized, phase 2, neoadjuvant trial in 270 postmenopausal women with ER-positive breast cancer. The everolimus combination resulted in improved tumor response rate compared with letrozole/placebo (68% vs. 59%, respectively,
mTOR Inhibition in Combination with other Signal Transduction Inhibitors
Another potential strategy is to combine mTOR inhibitors with other inhibitors of signal transduction pathways. The IGF-1 pathway is a major contributor to breast cancer pathogenesis. IGF-1R and the insulin receptor substrate 1 frequently are expressed at increased levels in breast cancers and are associated with chemoresistance in breast cancer.21,80 mTOR integrates incoming signals from insulin or IGF via receptor-mediated activation of the PI3K/mTOR/Akt signaling pathway. 16 An explanation for the limited activity of mTOR inhibitor monotherapy in breast cancer is that mTOR inhibition blocks negative feedback on IGF-1R signaling, impinging on PI3K and resulting in an increase in PI3K and Akt activation, which counteracts the inhibition of mTOR. 81 Under normal conditions, IGF-1R–induced activation of the mTOR pathway elicits a negative feedback loop whereby mTOR/S6 kinase reduces insulin receptor substrate I levels, the main ligand for the IGF-1R. 82 mTOR inhibition interferes with feedback regulation of upstream signaling elements, thereby paradoxically activating IGF-I signaling and lessening the antitumor effectiveness of mTOR inhibition. Treatment with the mTOR inhibitor rapamycin results in increased Akt activity and Akt phosphorylation at S473, which is dependent on IGF-1R and is associated with increased levels of insulin receptor substrate-1 (IRS-1). 82 Along these lines, blockade of IGF-1 and its receptor, IGF-1R, enhanced the antiproliferative effect of rapamycin, and, therefore, blocking IGF-1R appears to prevent mTOR inhibitor–induced feedback activation of PI3K/Akt and sensitizes tumor cell lines (including breast cancer) to the antiproliferative effects of mTOR inhibitors. 82 As such, this preclinical evidence suggests that IGF-1R inhibitors restore sensitivity in breast cancer cells that are resistant to mTOR inhibition. Currently, the combination of mTOR inhibitors and IGF-1R inhibitors is under study in several clinical trials, such as in the phase 1 trial evaluating temsirolimus in combination with cixutumumab (IMC-A12) against IGF-1R mentioned previously (Table 7) (NCT00699491). 29 Similarly, treatment with weekly doses (50 to 70 mg) of RAD001 (everolimus) resulted in activation of the ERK/MAPK pathway in tumor biopsies from patients with metastatic cancer. 83 Inhibition of MAPK (via upstream inhibition of ERK with a MEK1/2 inhibitor) enhanced the antitumor action of rapamycin. 83 In both instances, sensitivity to mTOR inhibitors was enhanced by a combination of agents that target multiple aspects of the PI3K/Akt/mTOR pathway. The clinical utility of mTOR inhibitors may be limited by complex signaling feedback loops. Therefore, more clinical studies are needed with combined therapeutic approaches aimed at the mTOR pathway.
Other Investigational mTOR Inhibitors in Breast Cancer
Additional novel inhibitors of the PI3K/Akt/mTOR pathway are being assessed in early-phase clinical trials. BEZ235, an investigational dual PI3K/mTOR inhibitor, has shown additive effects with trastuzumab and lapatinib in a PTEN knockdown breast cancer cell line. 84 Additionally, BEZ235 has demonstrated antitumor activity in trastuzumab-resistant breast cancer cells with activating mutations in p110α, in trastuzumab-resistant breast cancer xenografts, 85 and in lapatinib-resistant breast cancer cells in vitro. 86 This drug currently is being tested in phase 1 clinical trials of patients with mBC and other solid tumors alone (NCT00620594) 29 and in combination with other agents (NCT01285466, NCT01248494). 29
Ridaforolimus, an investigational oral mTOR inhibitor, improved PFS compared with placebo in patients with metastatic soft tissue or bone sarcomas who previously had a favorable response to chemotherapy in the SUCCEED trial (NCT00538239).29,87 In October 2011, the FDA accepted the new drug application filing for ridaforolimus in the treatment of metastatic soft tissue or bone sarcoma in patients who had a favorable response to chemotherapy. The use of ridaforolimus in mBC in combination with the IGF-1R inhibitor is currently being explored in a phase 2 study in HER2-negative, ER-positive, high-proliferation breast cancer. 29
Conclusions
The PI3K/Akt/mTOR pathway contributes to estrogen independence, growth factor independence, and the development of resistance not only to chemotherapy but also to endocrine and biologic targeted HER2 agents in advanced breast cancer. Inhibitors to mTOR have demonstrated antitumor activity in a variety of cancer types, including hormone receptor–positive, HER2-negative advanced breast cancer, RCC, PNET, renal angiomyolipoma associated with TSC and SEGA associated with TSC, for which they have gained FDA approval. BOLERO-2 has demonstrated that the combination of mTOR inhibitors with endocrine therapies is a promising strategy, with the mTOR inhibitor everolimus, in combination with exemestane, improving PFS in patients with hormone receptor–positive advanced breast cancer refractory to nonsteroidal aromatase inhibitors. Furthermore, the strategy of combining mTOR inhibitors with other targeted agents or with cytotoxic chemotherapy has produced signals of antitumor activity or has delayed the development of resistance to these agents. Selective patient criteria and rational selection of combination therapies may enhance the success of mTOR therapies based on information emerging from the many ongoing clinical trials of mTOR combinations in mBC. Designing effective combination therapies using mTOR inhibitors together with different agents that target key molecular elements involved in breast cancer relies heavily on the identification of predictive markers that may provide a basis for individualized patient therapy. Biomarker-based evaluations in ongoing and future trials may identify the most beneficial therapeutic strategies for different patient subgroups. Future clinical studies may stratify patients based on previous responsiveness or resistance to endocrine or trastuzumab therapy. Although mTOR inhibitors already play a critically important role in delivering more effective cancer therapy, their role as partners to current treatment strategies for advanced breast cancer continues to be defined.
Author Contributions
Conceived and designed the experiments: DAY. Analyzed the data: DAY. Wrote the first draft of the manuscript: DAY. Contributed to the writing of the manuscript: DAY. Agree with manuscript results and conclusions: DAY. Jointly developed the structure and arguments for the paper: DAY. Made critical revisions and approved final version: DAY. The author DAY reviewed and approved of the final manuscript.
Funding
Editorial assistance was funded by Novartis Pharmaceuticals Corporation.
Competing Interests
DY is a consultant to Novartis.
Disclosures and Ethics
As a requirement of publication, the author has provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The author has read and confirmed her agreement with the ICMJE authorship and conflict of interest criteria. The author has also confirmed that this article is unique and not under consideration or published in any other publication, and that she has permission from rights holders to reproduce any copyrighted material. Dr. Yardley has no disclosure to report. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgements
The author thanks Matthew Grzywacz, PhD, of ApotheCom for editorial and technical support in the development of later drafts of this manuscript. The author also acknowledges Harleigh E. Willmott, PhD, of Scientific Connexions for support in the development of earlier drafts.