
Abstract
Introduction
Breast cancer is the most common cancer among Egyptian women. The disease is often advanced at diagnosis. Since molecular profiling is not feasible in routine practice, we sought to examine the association of age distribution with hormone receptor profile, disease stage and outcome among Egyptian women.
Patients and Methods
We conducted a retrospective review of breast cancer patients treated at Mansoura University Cancer Center in the Nile Delta from 2006 through 2011. Age groups were examined in relation to hormone receptors status and tumor clinicopathological criteria. Additionally, the effect of receptor status on disease relapse and disease-free survival was examined with logistic regression and Kaplan–Meier analysis.
Results
A total of 263 patients were included in the current analysis. About 66.9% (n = 176) of patients were hormone receptor positive, 14.1% (n = 37) were Her2/neu positive, and 19.0% (n = 50) were triple negative. Median age of the patients was 52 years and was equal across all receptor status types. Triple negative status correlated with increased risk of disease relapse (odds ratio = 1.8, P = 0.03) and with shortened disease-free survival (hazards ratio = 2.6, P < 0.01).
Conclusion
The age distribution and receptor status pattern in the Nile Delta region does not explain the aggressive behavior of the disease. The age of the patients at diagnosis is older than patients in earlier studies from Egypt emphasizing the importance of implementing mammographic screening programs.
Introduction
Breast cancer is the most common cancer of women worldwide. 1 In Egypt, the disease accounts for 37% of women's cancer with an incidence rate of 49.6/100,000. 2 The disease is often advanced at diagnosis, and the mortality is still high.3,4 Since the behavior of the disease is generally governed by its molecular subtype,5,6 there have been speculations that Egyptian women suffer aggressive subtypes more frequently. The molecular pattern of breast cancer in the Egyptian population was recently published. Salhia et al 7 examined around 200 tumor samples from Egyptian patients with immunohistochemistry (IHC) and classified them into luminal A, luminal B, Her+, and basal-like subtypes based on estrogen receptor, progesterone receptor, Her2/neu, ki67, EGFR, and CK 5/6 markers. Contrary to popular belief, basal-type carcinomas accounted for only 11% of the Egyptian samples. 7 These authors concluded that the advanced disease stage encountered in Egyptian practice cannot be explained by an increased incidence of the aggressive molecular subtypes. We sought to examine the association of age distribution with hormone receptor profile, disease stage, and outcome among Egyptian women. Additionally, to better understand the relation between tumor characteristics and the disease outcome, we sought to examine the association of receptor status on disease relapse and disease-free survival. We relied entirely on routinely performed laboratory tests as markers for tumor subtypes, and we considered the triple negative breast cancer as a rough surrogate for basal-type carcinoma.8–11
Patients and Methods
We retrospectively reviewed the data for all breast cancer patients treated at Mansoura University Oncology Center from 2006 through 2011. Data abstracted from patients’ charts included clinicopathological criteria, diagnostic and therapeutic procedures, and follow-up visits. Specifically, patient age, American Joint Cancer Committee (AJCC) stage, tumor grading, receptor status, date of diagnosis, date of last follow-up, and the occurrence of tumor-related events were extracted. Tumor staging was recorded according to the 2010 AJCC cancer staging. For the purpose of this study, we recorded the pathological staging on file.
Receptor status was determined by IHC on paraffin sections according to manufacturer's instructions (all from Thermo Scientific, Lab Vision Corp., Fremont, CA) using antiestrogen-α rabbit monoclonal (clone SP1, catalog # RM-9101-S1), progesterone receptor mouse monoclonal Ab-2 (catalog # MS-192-P) and Her2/neu Ab-17 (clone e2-4001+3B5, catalog # MS-730-P0). Weak staining or infrequent staining (<1%) was considered as negative for hormone receptors. 30% cut off threshold was used for Her2/neu. FISH was not routinely utilized due to low availability. For the sake of the current study, ER and/or PR positivity qualified the case as receptor positive regardless of Her/neu status.
For stage I and II, surgical treatment consisted of modified radical mastectomy (MRM) or breast conservative (BCT) therapy according to patient preference and coexisting contraindication for BCT. Stage III cases were offered MRM. A few of these patients opted for immediate autologous tissue breast reconstruction.
Adjuvant treatment protocols followed at the hospital were in accordance with the current recommendations at the time of therapy 12 In particular, adjuvant chemotherapy regimen used was CAF × 6 (cyclophosphamide 500 mg/m2 intravenous [IV] day one, doxorubicin 50 mg/m2 IV day one, 5-FU 500mg/m2 IV day one, every three weeks × 6 cycles). For triple negative cases, CAF × 3 followed by TAC × 3 (docetaxel 75 mg/m2 IV day one, doxorubicin 50 mg/m2 IV day one, cyclophosphamide 500 mg/m2 IV day one, every three weeks × 3 cycles). For Her2/neu cases, trastuzumab was added. Similar chemotherapeutic protocols were used as neoadjuvant in cases that were not technically resectable at presentation, for example, due to extensive skin involvement. These cases were not substratified for sake of simplification.
Statistical analysis was performed using SPSS Gradpack 17.0 (IBM SPSS Inc., Chicago, IL). Descriptive statistics were presented as medians and 95% confidence intervals (Cis). Correlation of age with disease survival, stage, and grade was examined with the Spearman nonparametric test. Tumor relapse association with receptor status was examined with the chi-square test. Disease survival was modeled using the Kaplan–Meier method, and the effect of receptor status on survival was evaluated with the log-rank Mantel–Cox test. Multivariate analysis was performed with the logistic regression model for the event of relapse and with the Cox regression model for event-free survival.
Results
A total of 263 patients with completed receptor status and follow-up information were included in the current analysis. The mean age of the patients was 53 years (± 11.6 SD). The 25th, 50th (median), and 75th age percentiles were 45, 52, and 60 years, respectively. Pathological AJCC stage classification showed that 21 (9.5%) patients were in stage I, 92 (41.6%) were stage II, 104 (47.1%) were in stage III, and 46 (1.8%) were in stage IV. Tumor grading showed that grades I, II, and III represented 14 (5.5%), 195 (77.1%), and 44 (17.4%) of the tumors, respectively. In addition, 10 cases were ungradable special type tumors. A total of 176 (66.9%) patients’ tumors were hormone receptor positive (HRP), 37 (14.1%) were Her2/neu positive (HER), and 50 (19.0%) were triple negative (TN) (Fig. 1). At a median follow-up of 31 months, 151 (69.6%) patients were disease free and 66 (30.4%) patients had relapses.
The distribution of receptor status tumor type across the study population.
The age distribution was similar across the 3 types of patients as defined by the hormone receptor status (Fig. 2). Free and relapsed patients had the same median age of 52 years. Patient age was significantly correlated with tumor grade (Fig. 3), with younger age being correlated with high grade tumors (Spearman rho = −0.27, P < 0.01). Patient age was also correlated to a modest degree with tumor stage (Spearman rho = −0.14, P = 0.04). However, patient age was not correlated with patient survival (Fig. 4) (Spearman rho = −0.16, P = 0.80).
Patients’ age distribution according to the receptor status pattern. Median age of the whole population is depicted by a transverse line. Patients’ age distribution according to tumor grade. Median age of the whole population is depicted by a transverse line. Patients age according to the incidence of tumor relapse during the study period. Median age of the whole population is depicted by a transverse line.


The risk of relapse (number and percentage) by receptor patterns (hormone receptor positive, Her2/neu positive and triple negative) was compared using the chi-square test.

On multivariate analysis, tumor AJCC stage and receptor status predicted disease relapse. Triple negative status had almost double the risk of relapse compared with receptor positive status (odds ratio = 1.8, 95% CI = 1.1–3.0). (P = 0.03, logistic regression). On the other hand, tumor grade and patient age did not predict tumor relapse in the logistic regression model.
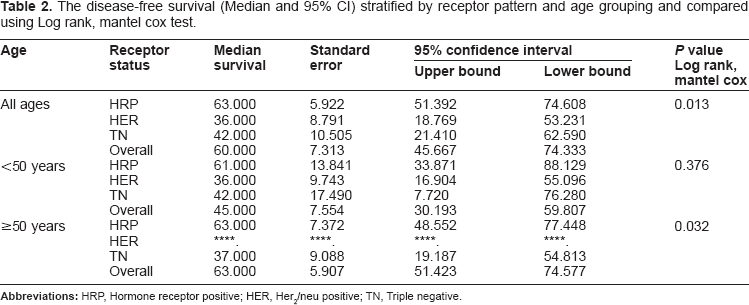
Median disease-free survival for the whole cohort was 60 months (95% CI = 45.7–74.3). Hormone receptor positive patients had a median survival of 63 months (95% CI = 51.4–74.6), Her2/neu cases had a median survival of 36 months (95% CI = 18.8–53.2), and triple negative patients had a median survival of 42 months (95% CI = 21.4–62.6), (Fig. 5). Receptor status had significant associations with disease-free survival for all patients and at every disease stage (P < 0.01, log-rank, Mantle Cox).
Kaplan–Meier curve for disease-free survival in the entire study population stratified by receptor pattern.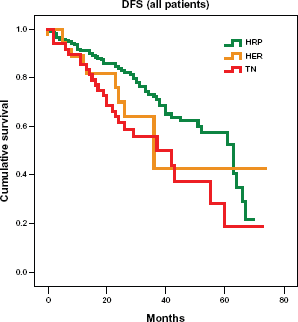
Median disease-free survival for patients younger than 50 years was 45 months (95% CI = 30.19–59.81) (Fig. 6). For patients ≥50 years, median disease-free survival was 63 months (95% CI = 51.42–74.58) (Table 2 and Fig. 7). On multivariate analysis, tumor stage and receptor status independently predicted shorter disease-free survival.
Kaplan–Meier curve for disease-free survival in patients younger than 50 years stratified by receptor pattern. Kaplan–Meier curve for disease-free survival in patients 50 years and older stratified by receptor pattern. The disease-free survival (Median and 95% CI) stratified by receptor pattern and age grouping and compared using Log rank, mantel cox test.

Discussion
In this cohort, we determined the age distribution and the receptor status profile of Egyptian breast cancer patients and their relation to the disease outcome. The disease was diagnosed at a median age of 52 years, almost two-thirds of cases (67%) were positive for hormone receptors and the disease outcome was worse in hormone receptor negative patients.
There is a widely held belief that breast cancer is a disease of younger Egyptian women. Median age at diagnosis is often quoted to be midforties.3,13,14 The Middle East cancer consortium report is a landmark source for population-based cancer incidence in Egypt and included cancer incidence information from the Gharbia governorate in the Nile Delta.2,15 This report indicated an exceptionally high incidence of breast cancer in the age group 25 to 34 years. Hospital-based reports from The National Cancer Institute in Cairo indicated a median age of 46 years. 3 Consequently, practitioners in our country adopted a concept of limited utility of mammography as a screening tool not only because of its cost but also because of the youth of the target population. We previously proposed a breast cancer screening program based on clinical breast examination with selective use of mammography, and we rationaled our proposal on the decreased accuracy of mammography at young ages. 16 The data in the current study and other recent reports from Egyptian databases indicate a trend towards an age distribution shift from the midfifties to the early sixties.7,17 This changing trend in age at diagnosis emphasizes the importance of implementing screening mammography in our community and advises against the reticence of many practitioners to recommend mammography for routine screening. In fact, a recent governmental outreach program for mammographic screening implementation in Egypt showed encouraging results. 18 However, the age at diagnosis described herein is still younger than the median age of 61 years in the United States as published by the Surveillance, Epidemiology and End Results (SEER). The age difference from US figures may be partially explained by the overall younger population in Egypt.
Interestingly, Stage I disease is twice as frequent in our series compared with the Gharbia Cancer Registry data (9.5% vs. 4.4% respectively). Metastatic cases decreased dramatically, while the percentage of locally advanced cases remained unchanged. This change is possibly associated with a time trend from the years 1999–2006 in Gharbia registry to 2006–2011 in our series.
The prevalence of hormone receptor positive cancer however seems comparable to Western data. Overall, 67% of cases were positive, and 23% were negative for hormone receptors as examined by IHC. These results are comparable to other published data from Egyptian databases. Dye and colleagues reported a 69% incidence of hormone receptor positivity in all cases with known receptor status in Gharbia Cancer Registry in Egypt. 19 Similar reports from Asia described 17.6% of triple negative cancer in 3 ethnic populations of Malaysia 20 and 20.6% in a Chinese population. 21
The current study is the first local study to examine the association of age distribution with hormone receptors. Nevertheless, we acknowledge some limitations. As we used databases from governmental health care institutions, the examined population probably represent a lower income group than typical Egyptian breast cancer patients. This limitation is basically universal to all published reports from the Nile Delta region that examines patients who seek mostly free governmental healthcare services. Due to the absence of a national medical insurance coverage, the private health care sector accommodates many of the higher income population. However, hospital based-data from the National Cancer Institute in Egypt 3 representing an income group similar to our patients still showed a younger median age than the present study. Using a retrospective design, we could not identify a primary source for mortality data. However, disease-free survival data clearly show the pattern of disease biological and outcome features.
In conclusion, the profile of breast cancer in this Egyptian cohort shows an age distribution that is different from those of Western countries. Stage at diagnosis is still relatively advanced and the treatment results are disappointing. This pattern is typical for developing communities where Western lifestyles import several risk factors for increased cancer, while the health care service is still lagging behind. The present data dispel the concept of the limited utility of mammographic screening and strongly advise more effort to implement screening programs and provide adjuvant therapy.
Author Contributions
Conceived the study: OH. Collected the data and discussed the results: AA, MM, OF, KF, MA. Analysed the data and reviewed the results: AE-S, OH. Reviewed the literature, interpreted the results and wrote the first draft of the manuscript: OH. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgment
We are thankful to the staff of the Mansoura University Cancer Center for their help and support.