
Abstract
Background:
The incidence of breast cancer had increased around the world. More premenopausal women suffer from this condition with great economic and social impact. The objective of this study is to establish possible associations between lifestyle and the presence of breast cancer in premenopausal women.
Methods:
The study population was composed of 330 premenopausal patients younger than 55 years with breast disease, cared between 2013 and 2017 at the University Hospital Mayor Méderi. Two comparison groups were formed. Patients with a tumor diagnosed as malignant considering cases and control group of patients with a tumor diagnosed as benign. With factors associated significantly in the bivariate analysis (P < .10), the hierarchically organized multiple regression model controlled by the confounding variables was constructed. The logistic regression model was adjusted by the age variable, to avoid residual confounder.
Results:
The population included 330 premenopausal women with benign and malignant breast disease: 134 cases and 196 controls. From the multivariate analysis, it was identified that the whole-grain consumption was inversely associated with presence of breast cancer (odds ratio [OR] = 0.579; 95% confidence interval [CI]: 0.339, 0.991; P = .046). On the other hand, consumption of fish was associated with the presence of breast malignancy (OR = 2.560; 95% CI: 1.200, 5.460; P = .015).
Conclusions:
Considering the epigenetic and multiomics individual profiles in the development of premenopausal breast cancer and its social and economic impact can be useful in development of modern clinical strategies with crucial interventions at the primary, secondary, and tertiary prevention levels for this disease.
Keywords
Introduction
Currently, breast malignancy is considered a public health problem worldwide. 1 The data provided by the World Health Organization, International Agency for Research on Cancer, show a tendency to increase the incidence of breast cancer globally. It reports a growing number of cases and a difficult control of its mortality, showing an overall increase in the incidence, but a decrease in mortality, specifically in developed countries. This contrasts with the increase in mortality for third-world countries. Breast cancer is considered the second most common cancer in the world, the most frequent in women with 2.08 million new cases reported for 2018. It is the fifth cause of death worldwide in general, the leading cause of female death in developing countries, and the second for first-world countries. 2
In Colombia, it is the most frequent cancer in the female population and its mortality tends to increase. Approximately 8686 new cases are detected annually. About 2.649 women die from this cause, and in the last 20 years, it jumped from the fifth to the second in frequency. It is the cancer with the greatest impact on women’s health in the country 3 ; its incidence in 2018 was 44.1 per 100 000 inhabitants (rate adjusted by age) and is only exceeded in incidence by prostate cancer.
For the population of premenopausal women, the natural history of the disease has had a substantial change, reflected in the evident increase in the incidence of the disease in this age group in recent decades. 4
There are several factors related to the presence of breast cancer. Variables such as family history of cancer, anthropometric variables, body mass index (BMI), hormonal factors (age of menarche, use of oral contraceptives), reproductive factors (parity, age of first birth, breastfeeding), as well as genetic factors have shown association. In recent years, the importance of the social environment in the development of this type of cancer was documented, which could be involved in the variation of the incidence in different geographical settings.5,6 Finally, several studies show that factors related to lifestyle such as diet, exercise, cigarette consumption, alcohol, and night work have been associated with the presence of the disease.7,8 In this context, this study seeks to establish the possible associations between the factors related to lifestyle and the presence of breast cancer in premenopausal women attended in a university hospital of high level of complexity in Bogotá, Colombia, between 2013 and 2017.
Materials and Methods
Study design
A case and control study was performed, in which 2 groups of women were compared according to the histopathologic diagnosis. One group with benign tumor and the other group with malignant tumor. Taking as reference the patients who consulted the institution for breast pathology, between July 2013 and December 2017, the population was composed.
Participants
Inclusion criteria
Women with a tumor lesion in 1 of the 2 mammary glands, younger than 55 years at the time of the histopathologic diagnosis and/or periodic mammographic follow-up, any patient who had reached menopause, defined as the absence of menstrual cycles for more than 1 year, and women with metastases from breast confirmed; all patients were treated at the Hospital Universitario Mayor Méderi, during the period between July 2013 and December 2017.
Exclusion criteria
Women without a clear typification of the benign or malignant pathology of the gland; women with history or presence of other cancer type, patients with oophorectomy, and patients with some degree of mental disability that would not allow them to voluntarily consent to respond to the data collection instrument.
Case group
Conformed by women younger than 55 years with malignant neoplastic cell changes confirmed by histopathologic study of the mammary glandular lesion.
Control group
Conformed by women younger than 55 years with a diagnosis confirmed by histopathologic studies and/or periodic mammographic follow-up of abscess-type lesion, breast hypertrophy, adenoma, fibromatosis, fibroadenoma, or fibrocystic disease of the breast, in the absence of cellular atypia.
Variables
Sociodemographic variables for characterization and description of the population include age, marital status, socioeconomic stratum, level of education (low: no education or primary level, high: secondary or higher studies), and occupation at the time of diagnosis.
Factors classically described as associated with the presence of the disease correspond to the BMI; hormonal factors: age of menarche, use of hormonal medications; and reproductive factors: parity, breastfeeding (yes/no and breastfeeding time > 6 months).
Factors related to lifestyle include diet, physical activity, cigarette consumption, alcohol consumption, night work, and leisure activities (any activity conducted during the free time as artistic expressions, religious activities, among others).
In the presence of breast cancer, variable of interest is defined as evidence of malignant neoplastic cell changes confirmed by histopathologic study of the mammary glandular lesion.
Data source
A retrospective review of the patient medical records and patients cared at the institution during the period considered was conducted through institutional software, Servinte Clinical Suite Enterprise. A reference population of 553 women was formed, for whom later, via telephone, the collection instrument was applied to obtain the variables related to sociodemographic, hormonal, and reproductive factors and those considered among lifestyles. The design of the instrument was taking as a parameter the National Survey of the Nutritional Situation in Colombia 2010 considering only week consumption frequency for the nutritional variables grouped by nutritional groups without quantity because the recall time was 1 year before the benign or malignant breast lesion diagnosis. Trained nurses in data collection, blinded to the diagnosis, who made the calls and the completion of the questionnaire, performed the application of the instrument. The study population was composed of women who answered the interview completely, and variables known to be associated with disease were considered as confusing a priori exposure questions were asked in the same way in both the group of cases and the controls, without prior knowledge of diagnosis; women had tumor lesions in both groups.
Statistical analysis
For the quantitative variables that presented normal distribution (Kolmogorov-Smirnov and Shapiro-Wilk normality test, at a level of significance of 5%), the mean and maximum and minimum values were used. For variables that did not present a normal distribution, the median was used as a measure of central tendency and interquartile ranges as measures of dispersion. The qualitative variables were described in absolute and relative frequency tables.
The bivariate analysis was performed defining the presence of breast cancer as the outcome variable, using maximum likelihood estimates and the test for asymptotic chi-square assessment, the McNemar test for the qualitative variables that met the criterion of normality, and, for those that did not, the Mann-Whitney U test.
The multivariate model was constructed from the associated factors in the bivariate analysis with a level of significance of .10. A multiple regression model, hierarchically organized, controlled by the probable confounding variables, was performed. Age is taken as a confounding variable and analyzed as a ratio variable, at a higher hierarchical level, to have a better confounding control. Confusion adjustment was performed at the statistical analysis stage, and the resulting model allowed the effect of the confounding variable to be controlled. The consumption of fish, integral foods, and grains; the educational level; and lactation and parity formed the final logistic regression model that was adjusted by age. The odds ratio (OR) was estimated, and a level of significance of .05 was defined.
All the analyses were performed using IBM SPSS Statistics version 21 software, licensed by the Universidad del Rosario.
Results
The study population included 330 women younger than 55 years, premenopausal women with breast disease, 134 with malignant cellular alterations that corresponded to the group of cases and 196 were controls. The minimum age was 18 years and the maximum age was 54 years, median 45.5 years. In relation to the histopathologic and clinical diagnosis, the case group presented in their majority breast carcinoma not specified and, in the control group, the majority evidenced fibrocystic breast condition (Table 1).
Diagnosis per groups.

The analyzed patients were mostly employed at the time of diagnosis and had a high educational level. Socioeconomic stratum II was the most frequent, followed by III. The entire population belonged to the contributory regimen in Colombia’s health system. Regarding the marital status, in the case group, there was a higher frequency of married patients, whereas in the control group, they were mostly single (Table 2).
Description of the sociodemographic characteristics by comparison groups and bivariate analysis between sociodemographic factors and the presence of breast cancer.

Inclusion criterion of variables to the logistic model, values (P ⩽ .10).
In the bivariate analysis, the educational level showed a statistically significant association with the outcome (P = .013; Table 2). Of hormonal and reproductive factors, breastfeeding was shown as a factor associated with the presence of cancer (P = .040), whereas parity was shown to be a protective factor for the presence of cancer (P = .050; Table 3). Regarding food factors, there was no association between the presence of premenopausal breast cancer and dairy products, carbohydrates, vegetables, fruits, fried food, sugary beverages, red meat, sausages, and fast foods. There were differences between cases and controls for the consumption of integral food, grains, and fish (Table 4).
Bivariate analysis between hormonal, reproductive, and lifestyle factors and presence of breast cancer.

Abbreviations: CI, confidence interval; OR, odds ratio.
Inclusion criteria of variables to the logistic model, values (P ⩽ .10)
Missing data corresponding to women with no exposure to breastfeeding.
Bivariate analysis between dietary factors and the presence of breast cancer.
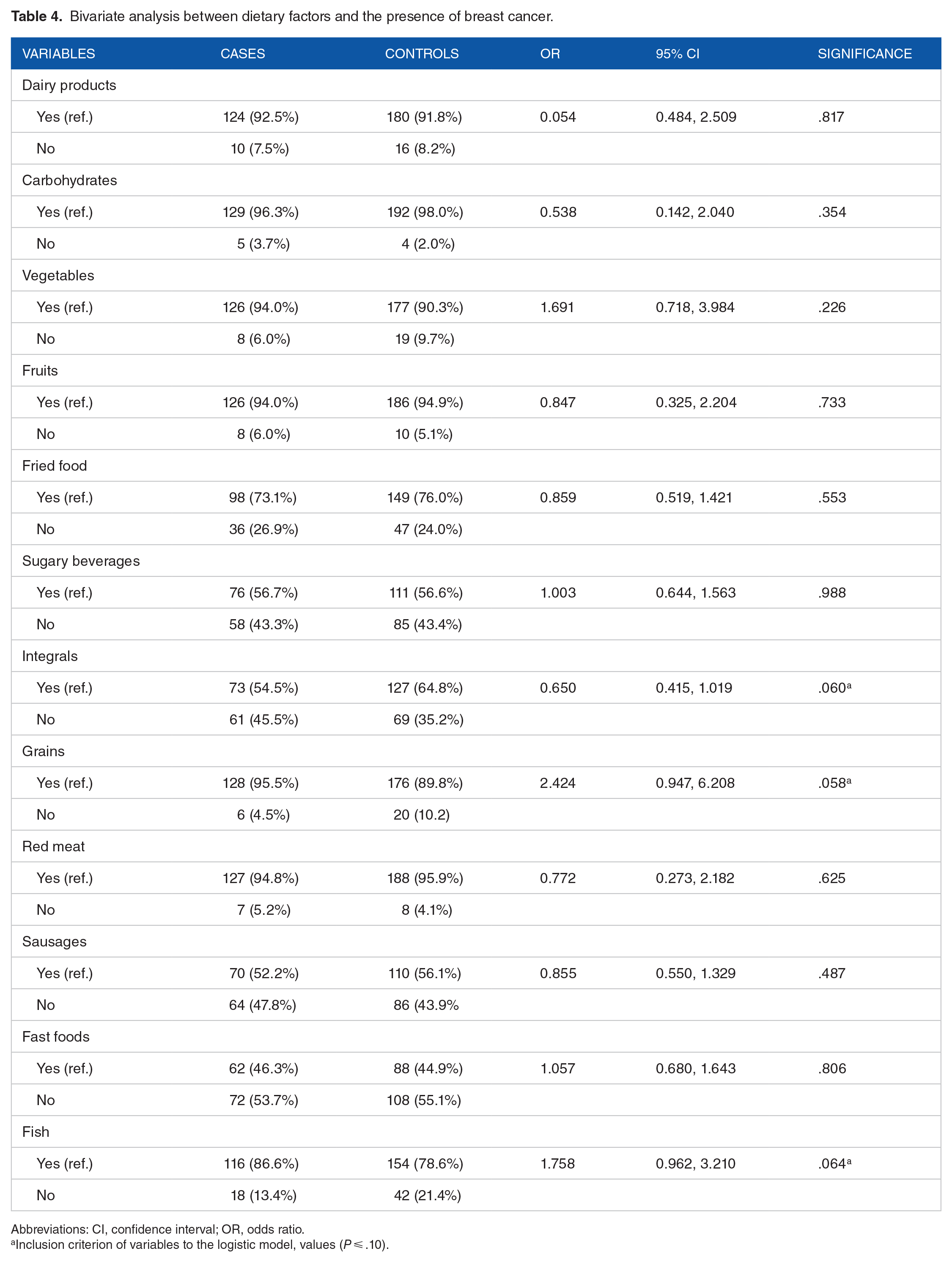
Abbreviations: CI, confidence interval; OR, odds ratio.
Inclusion criterion of variables to the logistic model, values (P ⩽ .10).
Multivariate analysis
The associated variables were considered significantly (P ⩽ .05) and close of evidencing association (P ⩽ .10) to be included in a hierarchical manner in the multivariate model. The logistic regression model included the age, the dietary factors: the consumption of fish, integral foods, and dry grains (legumes), the educational level, and the reproductive variables: breastfeeding and parity (Table 5).
Conditional logistic regression model for premenopausal breast cancer, adjusted estimates; bivariate analysis with raw estimates adjusted by age.

Abbreviations: CI, confidence interval; OR, odds ratio.
Significance level of .05.
Ranking by a higher educational level.
Measurement level, ratio scale, β value for the association.
Model adjusted by confounding factors; breastfeeding, parity, educational level, grains, integral food, fish.
Discussion
Breast cancer has evidenced an increase in its incidence globally and is the second after prostate cancer. In Colombia, the incidence for 2018 was 13.380 cases, 46.5% women younger than 55 years, and 24.7 age-standardized mortality rate (world) per 100 000 mortality, being the second cancer with the highest number of new cases for last years.9,10 The increase in the number of premenopausal patients suffering from such a condition has gone hand in hand with changes in old age at the first birth, limitations on breastfeeding, among other factors, that women assume in role society at the recent decades. 11 Women of reproductive age have had a demographic profile of current populations that suffered enough changes; there is a greater probability of this condition in the gestation stage, worsening individual results due to the limitation of accessing adequate treatment. This reality prompts us to consider new strategies applied in the management of premenopausal breast cancer. 12 Changes in screening may probably be associated with increased diagnosis at an early age; however, not all countries have imaging screening programs for breast cancer in premenopausal women.
Causality
Multicausality continues to be accepted as an explanation in many types of cancers. Hormonal, reproductive, occupational exposure, environmental pollution, unreasonable diet, and genetic factors are closely related to breast cancer.7,13 These exposures translate at the molecular level with the genetic fact involved in carcinogenesis, the epigenetic as a process of regulation of gene expression without changes in the DNA nucleotide sequence, by DNA methylation essential for cellular and tissue homeostasis, it is particularly important for development of breast cancer, global hypomethylation of oncogenes and hypermethylation of tumor suppressor genes are characteristic of most types of cancer. 14 There is a strong relationship between tumor and inflammation, a hot spot in breast cancer research. Inflammation promotes the growth of blood vessels, the proliferation of cancer cells, and invasiveness, also negatively regulates the immune response changing the efficacy of certain antitumor drugs. 15 Some studies have shown that inflammation would help cancer to metastasize. Coffelt et al 16 found that γδ-T cells and neutrophils can facilitate lung and lymph node metastases in patients with breast cancer. Cancer is a complex disease that involves multiple abnormalities in the levels of DNA, RNA, proteins, metabolites, and medical imaging. 17
Epigenetics and metabolomics in breast cancer
Several studies show that diet products actively affect the development and progression of cancer. “Nutri-epigenetics” focuses on the influence of dietary agents on epigenetic mechanisms. These epigenetic alterations occur permanently linked to environmental factors and lifestyle risk factors (modifiable) that are particularly important for the development of breast cancer. 18 Likewise, metabolism is 1 of the key components of life. Studies have shown that the physiological state of cells and tissues is determined by the regulatory systems of the cell and its intermediate metabolism state. Metabolites provide functional information that cannot be obtained directly from the genome and proteome of cell and tissue states, associated with fully biochemical processes as initial, intermediate, or final products, and provide information on complex interactions between genes and environment of a given condition; metabolites can feed back into other physiological and pathological processes. Metabolome contains all endogenous metabolites and is divided into primary metabolome (governed by the host genome) and cometabolome (dependent on the microbiome). Association of the entire metabolome is able to discover the cause decided by the intricate interaction of genes, environment, and lifestyles in the general population. 19
Diet
Breast cancer rates vary widely among populations. In populations of migrants to developed countries, it was observed a higher incidence of this pathology. The trend toward a greater number of new cases in countries, not only in the first world, has led to hypothesize that dietary factors could explain the great variation in the incidence of breast cancer worldwide.20,21
Antioxidant properties of whole grains
The denomination integral grains are attributed specifically to cereals, that correspond to the seeds of grains such as wheat, maize, rye or oats, rice, or barley that conserve the 3 parts that compose them: bran, endosperm, and germ. These have phytoestrogens, phytochemicals, and antioxidants, rich in fiber, complex B vitamins, vitamin E, tocol minerals, phytonutrients, and anti-nutrients. Among the antioxidant compounds, we may find phenolic acids, tocopherol, tocotrienols, selenium, zinc, soluble fiber, and phytic acid. 22 Its consumption has been associated with a lower risk of developing long-term diseases, among them, cardiovascular diseases, type 2 diabetes mellitus, and some cancers. 23 The benefits associated with its consumption are due to the existence of the unique phytochemicals of whole grains. Recent research has shown that the total phytochemical content and the antioxidant activity of integral grains have been underestimated. In addition, they contain unique phytochemicals that complement those of fruits and vegetables when consumed together.22,24
Many of the products produced with whole grains have greater antioxidant capacity in relation to vegetables and fruits. In addition, they supply vitamin E, an intracellular antioxidant that they allow to maintain selenium in its reduced state avoiding carcinogens precursors; reduced selenium prevents malignancy of cells exposed to carcinogens. 24 The protective effect of whole grains does by combined and synergistic action of the different compounds they contain. 25
In Framingham cohort, the associations between whole and refined grains and their food sources in relation to the cancer risk related to adiposity were evaluated in a group of participants. Participants were adults, belonging to the Framingham Offspring cohort (N = 3184; ⩾18 years old) between 1991 and 2013, identifying 565 cancers confirmed by pathology, concluding that a greater consumption of integral grains per day, and sources of integral foods per portion per day, was associated with 39% and 47% less risk of breast cancer, (OR 0.61; 95% CI: 0.38, 0.98 and hazard ratio 0.53; 95% CI: 0.33, 0.86, respectively). 26
There is growing evidence supporting the regular benefit of whole grains on the decrease in risk of different types of cancer. In a review of case and control studies in hospitals in Italy, Chatenoud et al 27 found a pattern of protection of whole grains for different types of cancer, including, among them, breast cancer. Calle et al 28 also reported a reduction in the risk of all cancers studied in the Women’s Health Study participants in Iowa. 29 It is interesting to note that the decrease in the risk of the disease cannot be attributed to the action of a particular nutrient because the effects of the substances contained in whole grains overlap, suggesting that the effect of the nutrient mixture (vegetables and fruits) is more effective than the protection that a nutrient would provide in isolation. 30
Our study clearly confirms the importance of this nutrient in relation to a lower probability of breast cancer in premenopausal women (OR = 0.579; 95% CI: 0.339, 0.991; P = .046).
Concern about fish
In relation to fish consumption, there is evidence of its benefits as a source of essential nutrients. In addition to containing proteins, essential vitamins, such as vitamin D, and minerals, fish and shellfish possess lipids as the main source of energy for their growth. Polyunsaturated fatty acids, eicosapentaenoic acid, and docosahexaenoic acid are required to provide energy and produce phospholipids and lipids essential for the formation of the cell membranes. The n-3 fatty acids, which are found especially in fatty fish, such as salmon, sardines, and herring, have been considered factors that improve cardiovascular risk. 31
Nevertheless, the increase in industrialization, urbanization, and mining causes air, soil, and water pollution which threatens the quality of food, being a health risk. Heavy metals, including methylmercury (MeHg) derived from mercury used in the gold industry in some areas of the world, have regained great interest due to their carcinogenic and mutagenic effect. 32 Methylmercury is 1 of the most toxic mercury-derived compounds present in the environment, due to its lipophilic nature, its ability to accumulate in the tissues of fish, and its ability to biomagnify throughout the food chain.33,34 Methylmercury content of large and long-lived fish such as tuna, among others, is higher. This compound binds to proteins; therefore, it is not removed when cleaning or cooking fish. 35 It has been studied the influence of this compound, and their role in the cytotoxicity and viability of triple-negative breast cancer cells for receptors. In cells that were exposed to varying concentrations, mercury induced cellular cytotoxicity of 35%, while flow cytometry revealed a detection of G1 stage of the cell cycle. 36 In vitro studies in breast cancer cells have shown that when metalloestrogens bind to the receptor, there is an increase in the transcription and expression of genes regulated by estrogens, which induces the proliferation of cells in breast cancer dependent on them, and MeHg is a metalloestrogen. 36 The activity this type of compound provides estrogen receptor and influences the hormonal response by altering the endocrine system generating greater cell proliferation.37,38
Taking into account the study by Trujillo et al, 39 who evaluated commercial fish mercury concentration interest in aquatic ecosystems of Orinoquia, between Colombia and Venezuela, high concentrations of Hg were found in several species of consumption associated with contamination of waters by gold mining. 40 Among results of the study found, fish consumption showed a higher probability related to breast cancer (OR 2.560; 95% CI: 1.200, 5.460; P = .015). This women population life in the center of the country, mostly in Bogotá city, the fish consumed often comes from continental masses of fresh water, its quality, and a possible exposure to the toxic metabolites described should be considered in the production chain. 41
Personalized oncology
Breast cancer is highly heterogeneous in the patient cohort; it is necessary to change the diagnostic and therapeutic approach in premenopausal women. The impact of nutrients on association with disease warrants a paradigm shift. The introduction of individualized molecular biological profiles as part of primary and secondary prevention is required. Without diet, the metabolism does not exist, that warrants studies that ensure greater accuracy because its characteristics require a specific categorization for an adequate measurement, which is not possible to obtain with retrospective studies. 42 The great economic effort and high failure rates in generalized management suggest that an individualized approach provides better cost-effective and beneficial results for patients with premenopausal breast cancer. Global activity in life science research on molecular biology has been growing almost exponentially since the early 1990s. 43 Omics technologies have a wide range of applications both in cancer research and clinical treatment, and based on sequencing, genomics and transcriptomics provide a better understanding of the structure of cancer. Multiomics strategies are aimed mainly at the comprehensive detection of genes (genomics), RNA (transcriptomics), proteins (proteomics), metabolites (metabolomics), and quantitative characteristics of medical images (radiomics) to systematically understand carcinogenesis at different biological levels; it is increasingly used in clinical treatment and basic cancer research. 17 This profile has the potential role in the establishment of different molecular subtypes and stratification of different patients. The integration of multiomics data plays a fundamental role in elucidating the molecular mechanism of tumorigenesis and the discovery of new biomarkers and pharmacologic targets; therefore, a radical change in cancer treatment is taking place in prediction, prevention, and personalized medicine with individualized profiles and predictive diagnostics. 42
The present study has some limitations. On one hand, the selection of the sample from a specific population that showed up at the hospital institution of socioeconomic stratum and social security regimen, and the sample size obtained was not enough to achieve inferences for the overall population. On the other hand, the retrospective data collection does not allow a detailed analysis of variables, such as dietary variables about characteristics of food, quantities, and consumption frequency, necessary for analysis on entire context. To preserve the principles of comparability, and thus limit the problems of validity in the analytical design, both cases and controls were obtained from a homogeneous group of patients treated for breast pathology, ensuring similarity between groups. Obtaining a control group that will have a breast lesion was taken as a strength because it facilitated the control of biases, such as memory.
The multifactorial human body is controlled by various endogenous and exogenous factors such as age, sex, environmental stressors, lifestyle, diet, and eventually stage of cancer. Several studies have shown that plants and natural products (both whole products and their compounds) control the development and progression of breast cancer. Phytochemicals, as widely available bioactive, have demonstrated apparent anticancer potential specifically targeting aberrant epigenetic changes. 44 On the other hand, toxic metabolic compounds can also be part of foods, promoting cellular disruption, increasing carcinogenesis, that way nutritional risk profiles are very useful in prevention. 42
Conclusions
Premenopausal breast cancer as a major health challenge, the social and economic impact that this means, requires the creation of new strategies that are better adapted to the needs of society in general by advancing care based on predictive diagnostic approaches, specifically innovative screening programs focused on the individualization of premenopausal women, prevention focused on high-risk groups such as young potentially reproductive women considering devastating results in gestational breast cancer.
Several studies show that diet products actively affect the development and progression of cancer. “Nutri-epigenetics” focuses on the influence of dietary agents on epigenetic mechanisms. This approach has gained considerable attention; because, unlike genetic alterations, epigenetic modifications are reversible and affect early carcinogenesis, these epigenetic alterations occur permanently linked to environmental factors and lifestyle risk factors (modifiable) that are particularly important for the development of cancer of the breast that comprises the majority of all cases in the world. In this way, clinical research can define epigenetic modulations related to the identification of high-risk individuals; consequently, the epigenetic profile of individuals can be useful in the development of modern clinical strategies with crucial interventions at the primary, secondary, and tertiary prevention levels for this disease
Footnotes
Acknowledgements
The authors thank Milcíades Ibáñez Pinilla, MSc, who participated in the statistical analysis and interpretation of the findings; Sandra Mayerli Prieto, Ingrid Lorena Pulido, and Ana Julieth Palacios for their participation as interviewers in the process of data collection; Hospital Universitario Mayor Méderi and Centro de Investigaciones Méderi (CIMED) for the support, help, and accompaniment in performing this research.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
LS-I helped in study design, fieldwork, data analysis and interpretation, development, and writing of the manuscript. JDLP helped in thematic design, analysis of the results, and revision of the manuscript. WR helped in thematic design, analysis of the results, and manuscript revision. AMR-S helped in methodological design, interpretation of the results, and development of the discussion. All authors read and approved the final manuscript.
Ethical Approval
This study was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and was approved by the Research Ethics Committee of the Universidad del Rosario, under Act DV0005-1-142-CE1849.
Consent to Participate
Verbal informed consent was obtained before the interview.
Data Availability
The set of data used and/or analyzed during the current study are available from the corresponding author at reasonable request.