
Abstract
Introduction:
Triple-negative breast cancer (TNBC) is a group of breast carcinoma characterized by the lack of expression of estrogen and progesterone hormone receptors (ER, PgR) and HER2. This form is also characterized by its aggressiveness, a low survival rate, and the absence of targeted therapies. This study was planned to evaluate the clinical features, treatment, and prognosis characteristics of TNBC in a population of Moroccan patients.
Methods:
In this retrospective study, a total of 905 patients diagnosed with breast cancer at the National Institute of Oncology in Rabat, Morocco, have been included. Based on molecular subtype, patients were divided into 2 categories: TNBC and non-TNBC patients. Data were recorded from patients’ medical files and analyzed using SPSS 13.0 software (IBM).
Results:
Overall, 17% of the patients had TNBC. At diagnosis, the median age of TNBC cases was 47 years, with extreme ages of 40 and 55 years. The median follow-up time was 30 months (10-53 months) and the 3-year survival rate was 76%. No significant difference was observed among the patients in terms of age at diagnosis, age at menarche, age at the time of first birth, nulliparity, oral contraception, and family history of breast cancer. Menopausal status and the number of pregnancy were significantly higher in the non-TNBC group. The percentage of grade 3 (G3) tumors was higher in the TNBC group (P < .001). Using neoadjuvant, adjuvant chemotherapy and radiotherapy, a net benefit in the event-free survival was registered for the 2 groups.
Conclusions:
This retrospective study was very informative and showed that women with TNBC had a less favorable prognosis than non-TNBC cases. Clinical data demonstrated that risk factors including age, premenopausal status, parity, hormonal contraceptive use, advanced disease, and a high histologic grade were independently associated with TNBC. However, large tumors and high Scarff-Bloom and Richardson grade prevail in TNBC cases with a higher incidence of lymph node metastases.
Keywords
Introduction
Worldwide, breast cancer (BC) is the most prevalent and the first leading cause of cancer death among females. Breast cancer represents 24.2% of all cancers in women and about 11.6% of all new cancer cases. 1 In 2018, the World Health Organization (WHO) has estimated that more than 630 000 women died due to BC. 1
Triple-negative breast cancer (TNBC) is an aggressive tumor form accounting for approximately 15% to 20% of all BC cases. 2 This subtype is defined pathologically by the absence of expression of the estrogen receptor (ER) and progesterone receptor (PgR) and does not exhibit amplification of the human epidermal growth factor receptor 2 gene (HER2). 3
Triple-negative breast cancer is a highly heterogeneous form of BC. This subtype is characterized by diagnosis at a younger age, larger tumor size, high-tumor grade, high mitotic index, and higher rate of mortality.4,5 Moreover, it is widely reported that TNBC constitutes an aggressive BC subtype because it is usually associated with a high frequency of metastasis with distinct metastatic patterns and a relatively high recurrence rate and it is usually accompanied by a significant decrease in overall survival (OAS). 6 Patients with TNBC are more likely to experience relapse within the first 3 years and are at high risk of death in the first 5 years following diagnosis. 7
In Morocco, data from different oncology centers converge toward its characterization as an aggressive form that occurs at a young age and poses a real health problem.7-10 This retrospective study was planned to investigate epidemiological and clinicopathological characteristics, treatment outcome, and survival rate in a Moroccan population with TNBC and to compare them with non-TNBC cases.
Methods
Study design and population
This retrospective study was conducted in the National Institute of Oncology in Rabat, Morocco. A total of 905 BC cases diagnosed in 2009 and followed up until 2014 were included in the study. For each patient, the medical record was carefully reviewed to obtain information regarding clinical, pathological, and therapeutic characteristics. A total of 405 cases with missed data, foreign people, and men patients were excluded and the remaining 500 BC cases were divided according to their molecular subtype into 2 groups: 85 patients with TNBC in group 1 (G1) and 415 non-TNBC patients in group 2 (G2).
The study was conducted concerning legal aspects and was approved by the Ethical Committee of Biological Research, Faculty of Medicine and Pharmacy—Rabat.
Data collection
Data were recorded from patients’ medical files. The medical records were retrospectively reviewed and information regarding age, anthropometry measurement (weight and height), familial history of BC, hormonal status, clinical data, cancer stage, tumor size, histological type, tumor grade, lymph node involvement, metastases, hormonal receptors, treatment (surgery, chemotherapy, radiation therapy, hormonal therapy), and follow-up was collected using SPSS software.
The histological type was recorded and updated according to the latest WHO classification of breast tumors. 11 Pathological tumor-node-metastasis (pTNM) staging was done according to the TNM classification of the seventh edition of the American Joint Committee on Cancer (AJCC) classification. 12 Histological tumor grading was evaluated according to Scarff-Bloom and Richardson (SBR) grading system modified by Singletary et al, 13 and vascular invasion was quantified histologically.
Immunohistochemical analysis was used to determine ER and PgR status and was performed using standard procedures on 4-μm sections of paraffin-embedded tissue specimens stained with the monoclonal antibodies 6F11 and 1A6, respectively. Accordingly, ER and PgR were considered positive when the nuclear expression was observed in at least 10% of the tumor cells. 12
Immunohistochemical expression of Her2 was evaluated according to cytoplasmic membrane staining of the infiltrative component, concerning the intensity and the percentage of stained cells and taking into account the complete or incomplete membrane staining. Results are expressed in scores: 0/1+ for negative, 2+ for ambiguous, and 3+ for positive staining. Fluorescent in situ hybridization (FISH) was performed to assess Her2 amplification when the score was ambiguous. Accordingly, if the Her2 amplification is confirmed by FISH, the case was considered HER2 positive. 12
Follow-up
Patients were followed up until December 2014. Event-free survival (EFS) was calculated from the date of surgery or the date of starting the first course of chemotherapy to the date of loco-regional recurrence or distant metastasis.
Statistical analysis
Statistical analysis was performed using SPSS software version 13.0 (IBM, Armonk, NY, USA). Descriptive variables were expressed as mean ± SD or median (interquartile range). Differences between qualitative data were assessed using the chi-square test. Survival rate calculation was performed by the Kaplan-Meier method and compared using the log-rank test.
Univariate and multivariate Cox regression model was performed to compare variables and outcomes. The difference is considered significant if the P value is <.05. In the multivariate model, all parameters reported in previous studies to influence survival rates were included even if these parameters were not significant in the univariate model of this study.
Results
Clinicopathological characteristics
Concerning inclusion/exclusion criteria, 17% of BC cases registered at the National Institute of Oncology in Rabat have a TNBC (85/500). Clinical and pathological data are reported, respectively, in Tables 1 and 2.
Comparative clinical data.
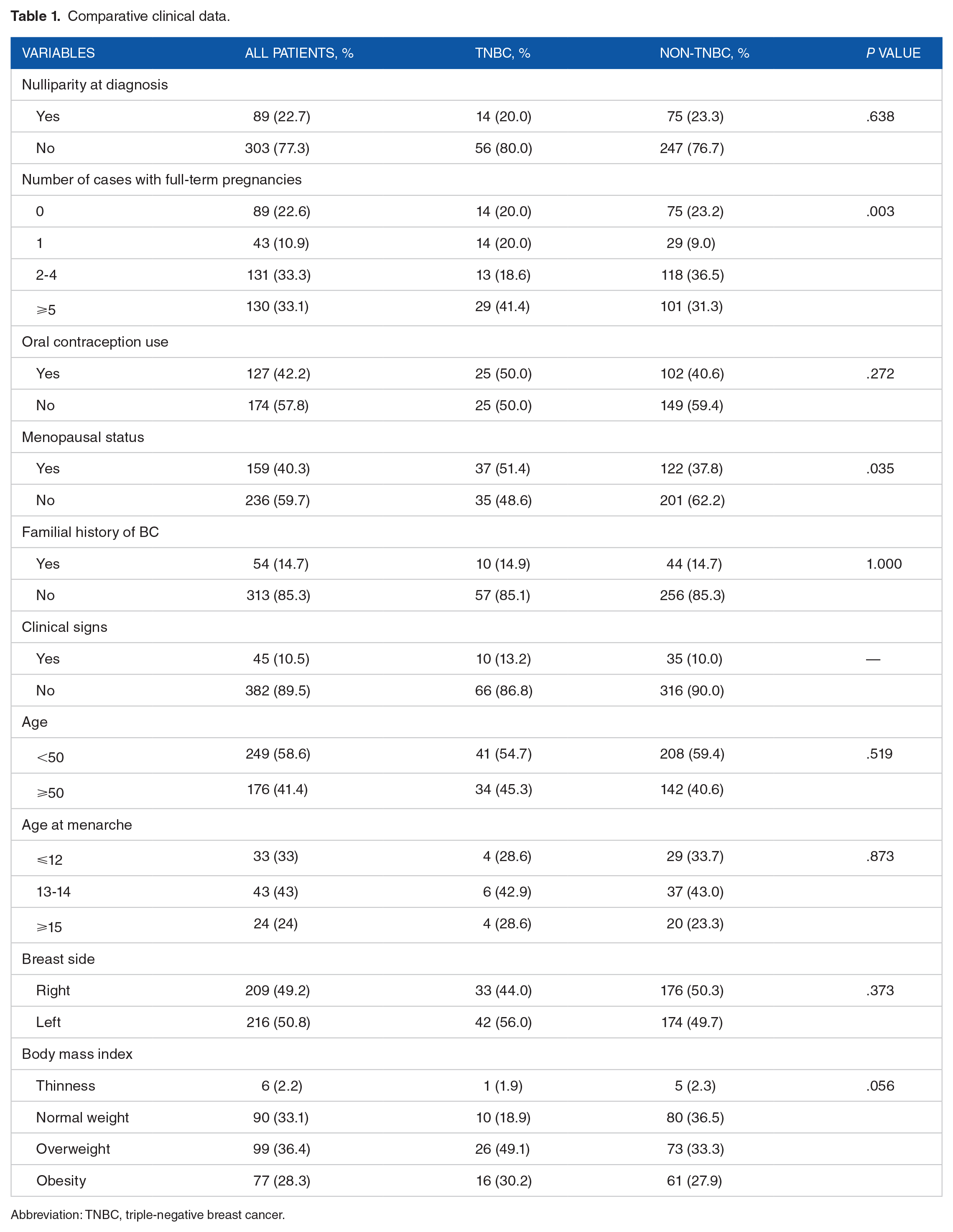
Abbreviation: TNBC, triple-negative breast cancer.
Comparative pathological data by TNBC groups.

Abbreviations: N, nodes; SBR, Scarff-Bloom and Richardson classification; TNBC, triple-negative breast cancer.
A complete database is given as an online suppelmantary file. Overall, the median age at diagnosis of TNBC cases was 47 ± 11.75, with extreme ages at 40 and 55 years. Only 14.9% of the cases have a familial history of BC. In this study, TNBC and non-TNBC cases shared the same distribution regarding clinical data.
A comparison between TNBC and non-TNBC cases showed a statistically significant difference for the number of full-term pregnancies (P = .003) and menopausal status (P = .035). A total of 41.4% of TNBC cases have more than 4 children as compared with non-TNBC cases. Moreover, 51.4% of TNBC cases (37/72) and only 37.8% of non-TNBC cases (122/323) are menopausal. The other parameters, including age, age at menarche, nulliparity at diagnosis, oral contraception use, and anthropometric data, did not show statistically significant differences between TNBC and non-TNBC cases.
The pathological characteristics of TNBC cases clearly show the predominance of N0 lymph node status and SBR grade III.
Comparison between TNBC and non-TNBC cases showed significant differences regarding intraductal components (P = .001), SBR grade (P = .001), and vascular invasion (P = .033).
Treatment
Patients with TNBC and non-TNBC received the same treatments as no specific treatment is recommended for TNBC cases; hormonal and Herceptin treatments are exclusively given to patients with positive hormone and Her2 receptors. Comparative treatment data between TNBC and non-TNBC cases are summarized in Table 3. Statistical analysis did not show any significant difference for the 4 treatment modalities.
Comparative treatment data by TNBC groups.

Abbreviation: TNBC, triple-negative breast cancer.
Analysis of EFS
The estimated median follow-up period was 30 ± 21.28 (10-53) months with extreme ranges of 3 to 67 months. Event-free survival was calculated using univariate analysis by Kaplan-Meier method and results are reported in Figure 1. The 3-year EFS of patients with the local disease was 76% and 83% of women with TNBC and non-TNBC, respectively. After 5 years, the EFS was higher in patients with TNBC (73%) than in patients with non-TNBC (65%). The difference between EFS in TNBC and non-TNBC patients is not statistically significant (P = .42). Results of EFS correlation to some relevant parameters are represented in Figures 2 and 3. Event-free survival is poorer in TNBC women with N3 lymph nodes (P = .00). In non-TNBC women, EFS is better in patients with N3 lymph nodes (P = .00).

Event-free survival (EFS) in TNBC/non-TNBC patients with local disease. TNBC indicates triple-negative breast cancer.
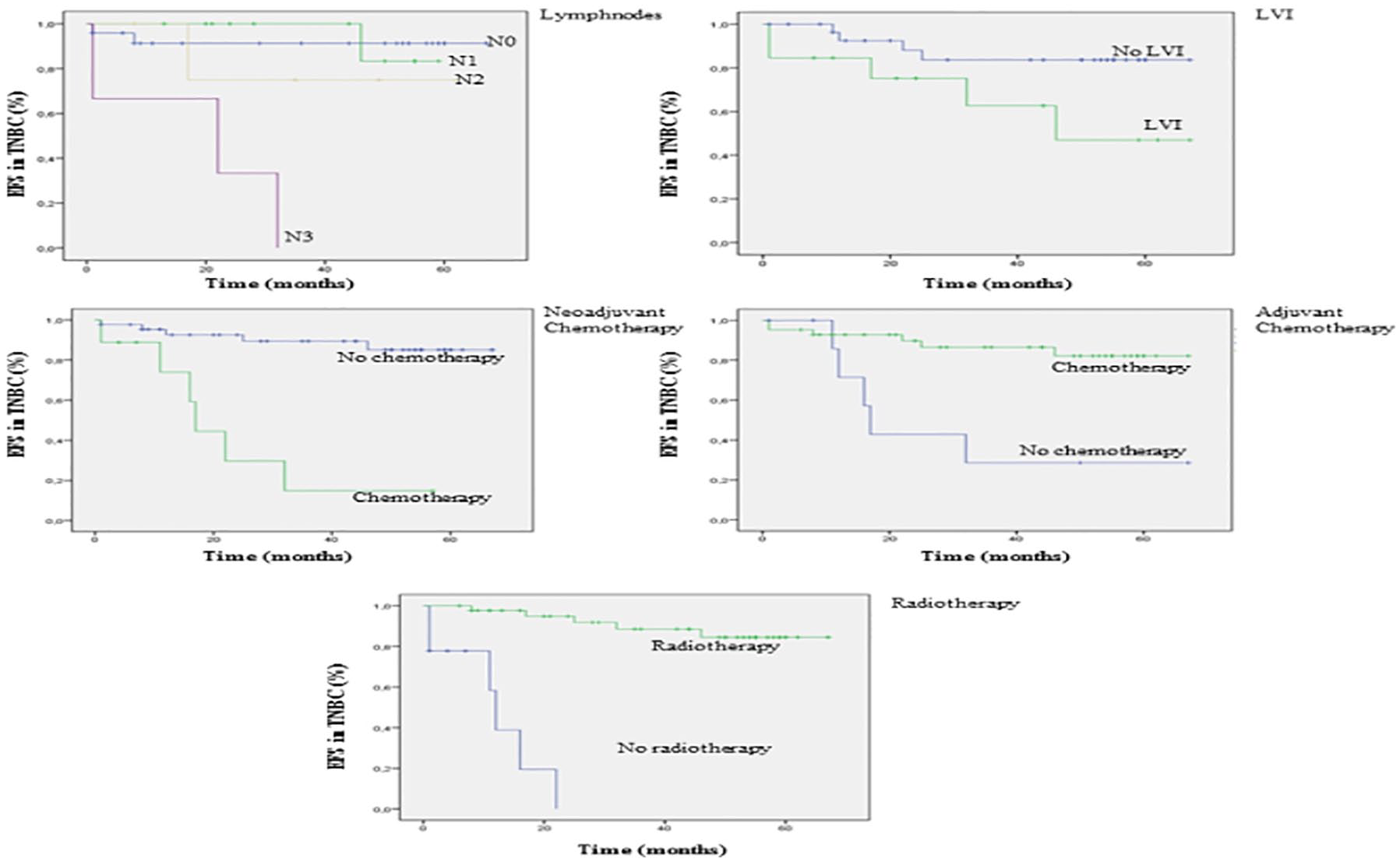
Event-free survival correlated to lymph nodes, lymphovascular invasion, neoadjuvant chemotherapy, adjuvant chemotherapy, and radiotherapy in TNBC group. TNBC indicates triple-negative breast cancer.
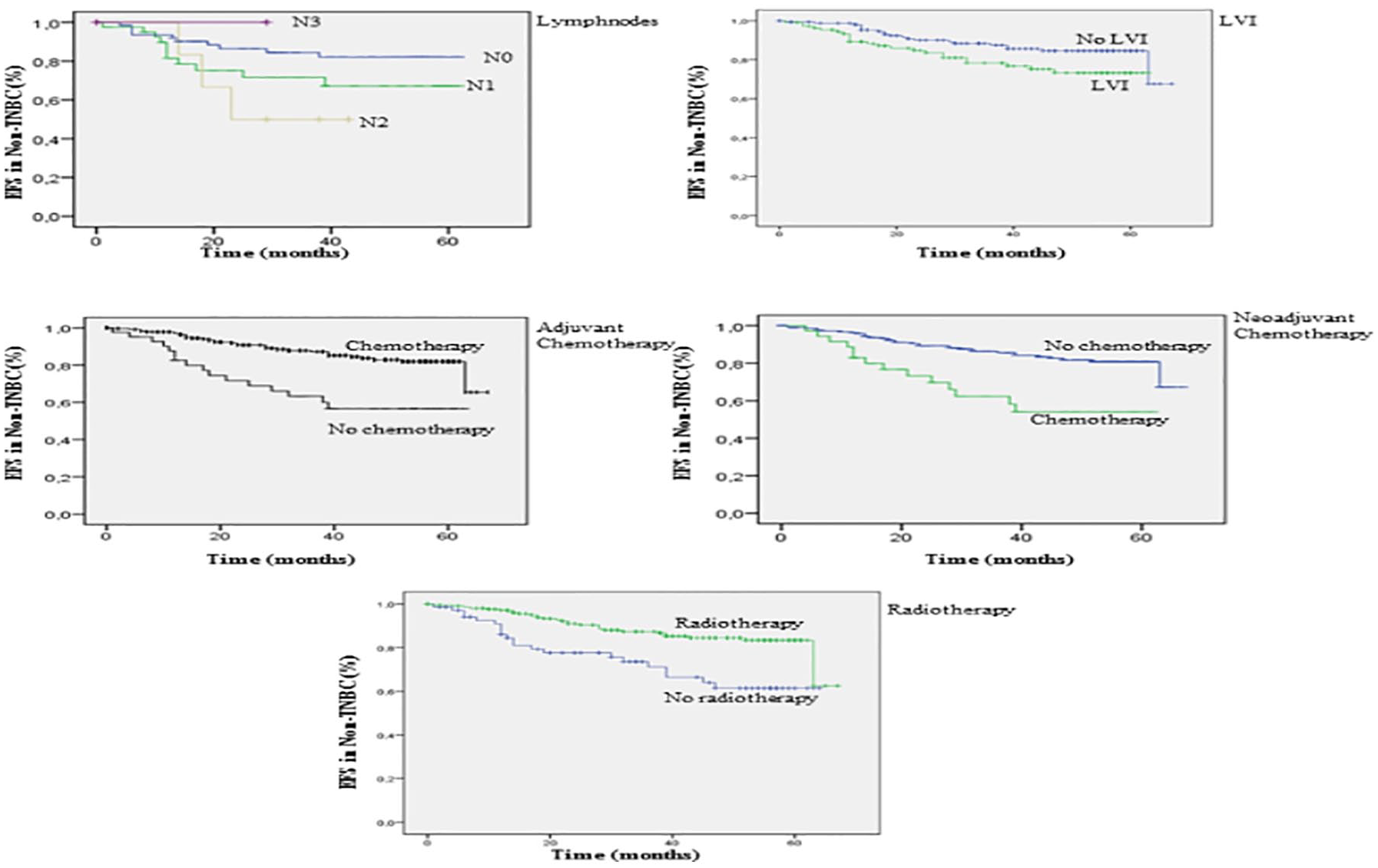
Event-free survival correlated to lymph nodes, lymphovascular invasion, neoadjuvant chemotherapy, adjuvant chemotherapy, and radiotherapy in non-TNBC group. TNBC indicates triple-negative breast cancer.
Univariate and multivariate Cox regression analysis
The results of univariate and multivariate Cox regression analyses are reported in Table 4. Univariate analysis indicated that N3 lymph node, chemotherapy, and radiotherapy are statistically significant parameters influencing EFS in women with TNBC.
Univariate and multivariate Cox regression analysis for event-free survival (EFS).
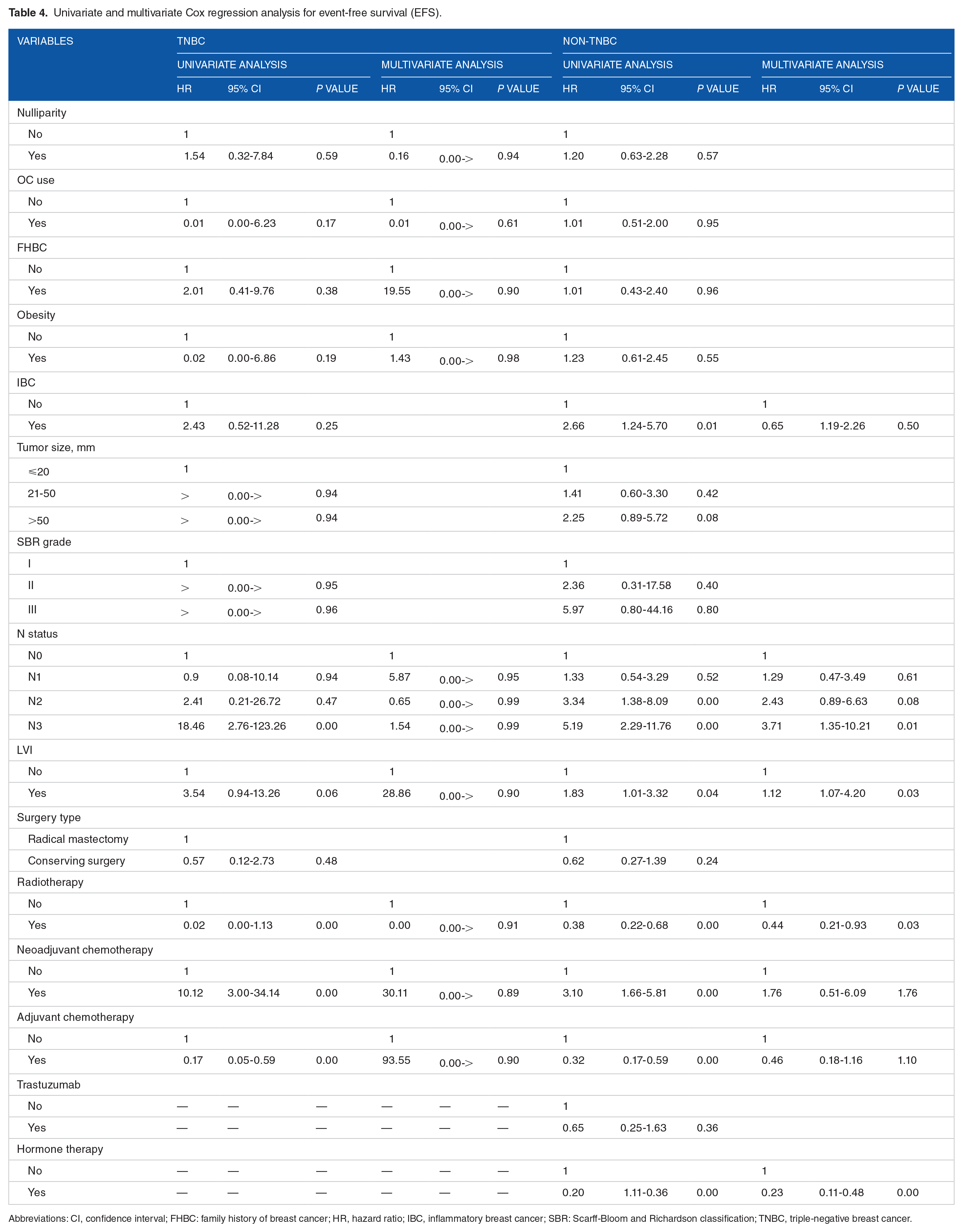
Abbreviations: CI, confidence interval; FHBC: family history of breast cancer; HR, hazard ratio; IBC, inflammatory breast cancer; SBR: Scarff-Bloom and Richardson classification; TNBC, triple-negative breast cancer.
Univariate analysis showed that, among non-TNBC cases, inflammatory BC, N2 and N3 status, presence of vascular invasion, radiotherapy, chemotherapy, and hormone therapy are associated with poorer EFS.
Concerning N3 lymph node status, the risk of relapse is higher in the TNBC group (18.46; P = .001) as compared with the non-TNBC group (5.19; P = .001). Of particular interest, the administration of neoadjuvant chemotherapy is a risk factor for both TNBC group (10.12, 3.00-34.14; P = .001) and non-TNBC group (3.10, 1.66-5.81; P = .001). However, adjuvant chemotherapy was beneficial for progression-free survival. In fact, the relapse risk was lower, corresponding to 0.17 (P = .005) for patients with TNBC and 0.32 (P = .001) for non-TNBC patients. For radiotherapy, the risk of relapse was lower for both TNBC and non-TNBC patients, with 0.024 (P = .001) and 0.38 (P = .001), respectively. For non-TNBC group, the risk of relapse after hormone therapy was 0.20 (P = .001).
Multivariate analysis showed no statistically significant results for TNBC cases. However, in non-TNBC cases, the multivariate analysis highlighted the same results than the univariate analysis regarding N3 status, presence of vascular invasion, radiotherapy, and hormone therapy.
Discussion
Worldwide, epidemiological and clinical data clearly showed that TNBC is an aggressive form of BC and is associated with a poor prognosis and a low EFS rising on a great challenge in the global management of BC. In Morocco, limited data on TNBC are available and studies were conducted on small size series.7,8,10 Therefore, this study was planned to be a large one to assess the epidemiology profile, tumor characteristics, and treatment patterns of TNBC cases compared with non-TNBC cases recruited in the National Institute of Oncology (INO) in Rabat. National Institute of Oncology is considered as the reference public health oncology center in Morocco and receives patients from the whole country.
In this study, TNBC was reported in 17% of BC cases, which is comparable to previously reported data in Morocco.7,8,10 Table 5 reports the prevalence of TNBC in Morocco as compared with other North African countries and some sub-Saharan, European, American, and Asian countries.
Comparison of TNBC frequencies.

Abbreviation: TNBC, triple-negative breast cancer.
Triple-negative breast cancer prevalence in Morocco is in agreement with obtained data in the other North African countries (Algeria and Tunisia) and much lower than almost sub-Saharan countries. These results highlight the high prevalence of TNBC in sub-Saharan countries that could be due to some genetic factors or attributed to some technical limitations leading to an overestimation of false-positive/negative results in performing and interoperating immunohistochemistry analysis related to ER, PR, and Her2 expression.
Triple-negative breast cancer is a complex and heterogeneous BC subtype associated with clinical, pathological, and biological factors highly variable according to the population. In our study, nulliparity at diagnosis is significantly less frequent in women with TNBC than in women with non-TNBC, and TNBC cases are more obese. These results are in agreement with recent studies reported by Plasilova et al, 19 showing that the risk for developing TNBC rises with increasing parity and increasing the waist-to-hip ratio circumference, suggesting a complex interaction of genetic biomarkers and societal factors.
Triple-negative breast cancer and patients’ age are well studied and discussed. Some results showed that in all ethnic/racial groups, the incidence of TNBC increased among young patients.21,22 In the United States, Plasilova et al 19 have reported that in white patients, TNBC prevails in patients below age 40, whereas in black patients, the incidence of TNBC is still higher until age 60. Of particular interest, the age of BC onset is 10 years earlier than in Western countries. 2 This finding is in agreement with previous studies in patients with TNBC from Tunisia. 15 A recent study conducted in Morocco highlighted the high frequency of BC in young women as compared with Western countries. 23 In this study, both TNBC and non-TNBC cases prevail in younger women, with no statistical difference between the 2 groups.
Worldwide, published data show that TNBC cases are characterized by bigger tumor sizes and high-grade histology.24,25 Regarding tumor size, there is no statistical difference between TNBC and non-TNBC groups in this study. Of particular interest, Dent et al 26 have conducted a long-term follow-up of 1608 patients with BC and found that the recurrence of TNBC did not correlate with the tumor size.
The association between lymph node status and TNBC is controversial. Some authors report that lymph node negativity is more frequent in TNBC. 27 Others support a higher frequency of lymph node positivity 28 and this lymph node positivity is associated with a poor prognosis, 24 whereas some publications suggest the absence of any association between increased tumor diameter and lymph node metastasis.28,29 In this study, most of the TNBC cases exhibit an SBR grade III as compared with non-TNBC cases (55.4% vs 30.9%). Large tumors and high SBR grade are in favor of a high lymph node metastases incidence. However, after adjustment of these factors, the incidence of positive nodes with TNBC is considerably less than non-TNBC, which is in agreement with previously reported data.7,19,30 Conversely, some other studies show that there is no statistical correlation of lymph nodes status between TNBC and non-TNBC groups.5,14
Triple-negative breast cancer is unresponsive to endocrine therapy, and currently, chemotherapy is the main option for systemic treatment of women with TNBC. In our study, the most of the TNBC and non-TNBC patients received systemic chemotherapy. Moreover, the odds of receiving chemotherapy were much greater for TNBC than for non-TNBC cases, even when adjusted for stage and grade. Furthermore, TNBC cases were more likely to receive neoadjuvant chemotherapy treatment.
As already reported widely,31,32 TNBC was significantly associated with poorer EFS, mainly because of the inability to administer hormone therapy to this BC subtype.
This study is very informative highlighting the main characteristics of TNBC cases in our population. The main limitations of the study are as follows: (1) the absence of a date of death in the medical records, which limited the calculation of the OAS, and (2) the noncomplete data in some patients’ files records that could have influenced the analysis.
Conclusions
Understanding the pathogenesis of TNBC and molecular and immunological characteristics of the disease is the key for better management of this heterogeneous disease. Clinical data highlighted that TNBC have the worse outcome compared with the non-TNBC. Moreover, common risk factors including age, premenopausal status, increased parity, hormonal contraceptive use, high histologic grade, and advanced disease were independently associated with TNBC.
Nowadays, many promising therapeutic pathways are investigated, but without a comprehensive consideration of TNBC pathogenesis, predicting the effectiveness of these strategies will be compromised.
Supplemental Material
Database_of_TNBC_and_non-TNBC_women-_Mouh_Fatima_Zahra_xyz23299106ae2b6_1 – Supplemental material for Clinicopathological, Treatment and Event-Free Survival Characteristics in a Moroccan Population of Triple-Negative Breast Cancer
Supplemental material, Database_of_TNBC_and_non-TNBC_women-_Mouh_Fatima_Zahra_xyz23299106ae2b6_1 for Clinicopathological, Treatment and Event-Free Survival Characteristics in a Moroccan Population of Triple-Negative Breast Cancer by Fatima Zahra Mouh, Meriem Slaoui, Rachid Razine, Mohammed EL Mzibri and Mariam Amrani in Breast Cancer: Basic and Clinical Research
Footnotes
Acknowledgements
Special thanks to Dr. Mohammed Erraki and all the staff of the epidemiology unit at the National Institute of Oncology for providing medical records needed for the study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
FZM participated in the project design, data collection, and statistical analysis and drafted the manuscript. MS participated in data collection and statistical analysis. RR was in charge of the statistical analysis. MEM participated in the design of the study and review of the final manuscript. MA participated in the design and coordination of the project and review of the final manuscript. All authors read and approved the final manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.