
Abstract
The bone-targeted agents (BTAs), bisphosphonates and denosumab, have an established role in the treatment of metastatic breast cancer bone disease and the prevention of cancer-treatment-induced bone loss. Evidence in support of their ability to improve survival in early breast cancer now indicates that the bisphosphonates are effective in postmenopausal women (naturally or chemically induced), but denosumab does not have similar benefits when added to standard adjuvant therapy. In postmenopausal women with early breast cancer, the choice of BTA may differ depending on the indication for treatment; for fracture prevention in low disease recurrence risk patients, denosumab may be favoured (in comparison with placebo) to maintain bone health, and when disease recurrence prevention is a priority in higher risk patients, bisphosphonates may be favoured. The reason for the lack of efficacy of BTAs in premenopausal/perimenopausal patients still remains unanswered and will need preclinical research to evaluate novel treatment combinations with BTAs in this patient group. This review covers the past, present, and future indications for BTAs in both metastatic and early breast cancer.
Introduction
The bone-targeted agents (BTAs), bisphosphonates (BPs) and denosumab, have several roles in breast cancer management in both the advanced metastatic setting and the early curative setting. In the advanced setting, both BPs and denosumab reduce the skeletal complications associated with bone metastases. In the early setting, BPs and denosumab prevent the bone loss associated with curative systemic cancer therapies, with oral BPs and denosumab reducing bone loss and fracture rates in postmenopausal women, and zoledronic acid (ZA) being the most effective BP at reducing the high level of treatment-induced bone loss in premenopausal women. More recently, the efficacy of BTAs to prevent breast cancer recurrence and improve survival, when given in early breast cancer, has been evaluated in large adjuvant breast cancer trials with evidence that BPs are effective at preventing recurrence in postmenopausal women only, but denosumab does not appear to have a role in metastases prevention in either menopausal group. Despite decades of research with BTAs in breast cancer, several questions remain unanswered, including why there is a lack of benefit in disease recurrence prevention in premenopausal women with early breast cancer and how to optimally schedule BTAs in the metastatic setting. Some of these questions will be answered by ongoing clinical trials, but others will require a return to the preclinical setting.
Treatment of Breast Cancer Bone Metastases
Bisphosphonates have been in clinical use for breast cancer bone metastases for several decades. Bone, as the most common site of metastases from breast cancer, is adversely affected by tumour cells through initiation of the recognized ‘vicious cycle’ of bone metastases, 1 leading to overactivity of bone forming osteoclasts, increased bone resorption, and the subsequent adverse clinical events in bone (termed skeletal-related events [SREs]; fracture, need for radiotherapy/surgery to bone and pain).
The concept that the osteoclast is the key bone cell to target to break this vicious cycle was taken forward in the clinical trials of BPs in breast cancer. The intravenous (IV) BPs such as pamidronate and ZA demonstrated the highest efficacy in prevention of SREs over the oral agents, and a phase III study comparing both drugs showed a significant reduction in SRE rates with ZA reducing SREs by 20%. 2 Four BPs are currently approved for use in malignancy-associated metastatic bone disease in Europe and America, and include oral clodronate, oral or IV ibandronic acid, IV pamidronate, and ZA. 3 While these drugs were effective at prevention of SREs, there was no convincing evidence that they affected survival. A retrospective analysis of phase III trials of ZA showed that normalization of bone turnover at 3 months on ZA (as measured by N-telopeptide of type I collagen (NTX)), in patients with elevated bone resorption at baseline, correlated with improved overall survival 4 with a reduction in risk of death in the breast cohort of patients of 48%. Whether this was due to prevention of fracture and its associated morbidity and mortality, or an anti-cancer effect of ZA was not known.
Following incorporation of BPs into routine clinical practice for breast cancer bone metastases, questions arose regarding the optimal scheduling of these drugs. The half-life of ZA in bone is measurable in years with ongoing evidence of biological activity for >3 years after a single infusion, 5 suggesting the frequency of administration of ZA could be reduced. Studies evaluated the role of de-escalating scheduling frequency and showed that after a year of ZA administered every 4 weeks (Q4W), de-escalation to every 12 weeks (Q12W) could be done with no significant differences in SRE rate reported between the 2 schedules. 6 , 7 The CALGB (Cancer and Leukemia Group B) protocol 70604 evaluated Q4W vs Q12W ZA for 2 years in patients with breast or prostate cancer or multiple myeloma (N = 1822) who had not received prior BTAs, with a primary endpoint of SRE rate at 2 years. This study showed non-inferiority between the 2 schedules (SRE rates: 29.5% Q4W vs 28.6% Q12W) after a median follow-up of 1.2 years. 8 These studies suggest that de-escalation of BPs is possible, probably because of their long half-life in bone.
Denosumab In 2010, a phase III study of the new pan-osteoclast inhibitor, denosumab, was undertaken comparing SRE rates with the current gold standard treatment, ZA. Denosumab, while still targeting the osteoclast, has a different mechanism of action, acting as a monoclonal antibody, targeting RANKL and preventing RANK-mediated osteoclast activation. Its half-life in serum is 28 days, but it is not incorporated into bone. A large phase III study compared Q4W denosumab (120 mg subcutaneous) with Q4W ZA (4 mg IV), and showed that denosumab was superior to ZA in the prevention of first and subsequent on-study SREs (relative risk = 0.77; 95% confidence interval [CI]: 0.66-0.89; P = .001 superiority) and had beneficial effects on pain. No survival differences were seen. 9
Denosumab became the standard of care in many centres following this head-to-head study, but the optimal scheduling of denosumab still remains to be defined. Its lack of incorporation into bone makes the ability to de-escalate unknown at present. In the osteoporosis setting, several case studies have reported that the resulting microarchitectural changes in trabecular bone on denosumab cessation have led to a rebound increase in vertebral fractures occurring within 2 to 10 months of stopping treatment. 10 Prior vertebral fractures, before or during denosumab treatment, were the strongest predictors of off-treatment new fractures. This osteoporotic population will clearly have differences when compared with a breast cancer population; however, the prevalence of vertebral fractures in breast cancer patients with soft-tissue metastases and no skeletal metastases has been shown to be 20-fold higher than the normal population. 11 Denosumab de-escalation studies are currently recruiting and results are awaited from the Swiss Group for Clinical Cancer Research (ClinicalTrials.gov identifier: NCT02051218) who are evaluating initiation of denosumab 120 mg Q4W for 3 doses followed by continuation at Q4W vs Q12W, with a primary endpoint of time to first on-trial symptomatic skeletal event (SSE). In addition, the Ottawa Hospital Research Institute in Canada is evaluating BTAs (pamidronate, denosumab, or ZA) delivered Q4W vs Q12W in patients with breast or prostate cancer, with primary endpoints of Quality of Life, pain, and SREs, in patients due to commence or already receiving BTAs (REaCT-BTA trial, ClinicalTrials.gov Identifier: NCT02721433). It is hoped these trials will provide evidence to guide clinical de-escalation decisions with denosumab.
Prevention of Cancer-Treatment-Induced Bone Loss
Bone loss as a result of curative breast cancer therapy is well recognized and is primarily a result of the effects of cancer therapies on oestrogen levels. Naturally occurring bone mineral density (BMD) loss in postmenopausal women is 1% per year 12 and increases to 2.6% with the use of aromatase inhibitors (AIs) 13 with maximum effects seen in premenopausal patients receiving gonadotropin-releasing hormone (GnRh) agonists plus AI at 7% per year 14 and those who experience primary ovarian failure as a result of chemotherapy at 7% per year. 15 The management of this accelerated bone loss requires lifestyle advice in addition to pharmacological intervention. 16
Bisphosphonates
Bisphosphonates are generically available established treatments used for the prevention of both benign and malignant bone loss. In premenopausal women with breast cancer only, the most potent BP, ZA, has been shown to reverse the significant bone loss associated with ovarian suppression, but in postmenopausal women, both IV infusion and oral BPs have shown efficacy in reversing AI-induced bone loss (reviewed in Hadji et al 16 ). The majority of these studies have used the endpoint of BMD loss, but the more recently reported AZURE trial (ISRCTN79831382) evaluated the impact of adjuvant ZA on fractures in both premenopausal and postmenopausal women. The Adjuvant Zoledronic redUce REcurrence in early breast cancer (AZURE) trial is an academic, multi-centre, randomized phase III study evaluating the addition of ZA 4 mg to standard therapy (neoadjuvant/adjuvant chemotherapy and/or endocrine therapy) for 5 years (administered IV every 3-4 weeks for 6 doses, then 3 monthly 8× and 6 monthly 5×) in patients with stage II/III early breast cancer. The 5-year fracture rate was reduced from 5.9% (95% CI: 4.8%-7.1%) (control) to 3.8% (95% CI: 2.9%-4.7%) with ZA. ZA significantly increased time to first fracture (hazard ratio [HR] = 0.69, 95% CI: 0.53-0.90, P = .0053), but the majority of fracture prevention benefit occurred after a disease-free survival (DFS) event (HR = 0.3, 95% CI: 0.17-0.53, P < .001) (see Figure 1). 17 Fracture benefits from ZA were similar across menopausal subgroups. These data suggest that while ZA does decrease fracture incidence prior to disease recurrence, its effects are not as great as would have been predicted by the BMD studies.
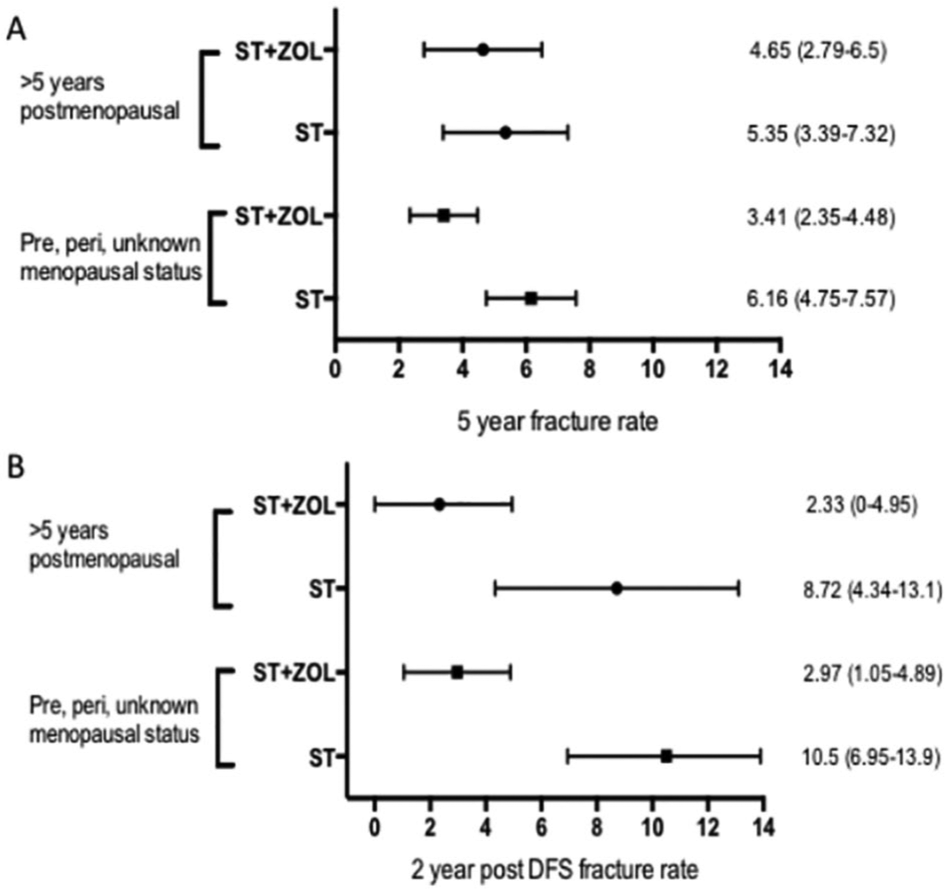
Interactions between menopausal status, treatment allocation, and frequency of clinical fractures. (A) Overall 5-year fracture rates in patients treated with ST (control) and ST plus ZOL according to menopausal status. Error bars are 95% CIs. Hazard ratios for time to first fracture according to menopausal status are 0.45-0.88 for premenopausal, perimenopausal, and unknown menopausal groups, and 0.52-1.33 for >5 years postmenopausal group. (B) Two-year fracture rates post-DFS event in patients treated with standard therapy alone (control) and ST plus ZOL according to menopausal status. Error bars are 95% CIs. Hazard ratios for time to first fracture post-DFS event according to menopausal status are 0.21-0.71 for premenopausal, perimenopausal, and unknown menopausal groups, and 0.06-0.75 for >5 years postmenopausal group. Reproduced with permission from Elsevier, Licence number 4381410096039.17 CIs indicate confidence intervals; DFS, disease-free survival; ST, standard therapy; ZA, zoledronic acid.
Denosumab
The Austrian Breast and Colorectal Cancer Study Group (ABSCG)-18 study randomized postmenopausal patients with early hormone receptor positive breast cancer receiving AIs to receive either denosumab 60 mg or placebo administered subcutaneously every 6 months. Denosumab halved fracture rates irrespective of baseline T-score, 18 suggesting that the existing guidelines that recommend selecting of patients for treatment with osteoclast inhibitors on the basis of baseline BMD or loss of BMD over time 19 may undertreat some patients at risk of fracture on adjuvant systemic therapy. The patient population in this study was low risk for recurrence with the majority having T1, node negative, grade 2, oestrogen receptor positive, and herceptin-negative tumours not requiring adjuvant chemotherapy.
Prevention of Formation of Metastases
Bisphosphonates
The emergence of data showing that BPs could improve survival and prevent recurrence, when used in the early breast cancer setting, came from the ABCSG-12 study which randomized premenopausal women rendered chemically postmenopausal with goserelin to tamoxifen or anastazole +/–ZA. There was a relative risk reduction of 29% for disease recurrence with ZA compared with endocrine only (HR = 0.71 95% CI: 0.55-0.92) with a significant overall survival benefit seen in women >40 years (HR = 0.57, 95% CI: 0.33-0.99, P = .042). 20 Following this, the AZURE study reported which used a more intensive schedule of ZA (detailed above) in premenopausal and postmenopausal women. Improvements in DFS with ZA were seen only in women who were >5 years postmenopausal at initiation of study with a relative risk reduction for recurrence of 25% (HR = 0.75, 95% CI: 0.59-0.96) and risk of death of 26% (HR = 0.74 95% CI: 0.55-0.98). 21 These 2 studies taken together suggested that in patients with low levels of ovarian hormones, ZA was preventing disease recurrence. This led to a meta-analysis of individual patient data from 18 766 patients treated with adjuvant BPs (predominantly ZA, clodronate, and ibandronate) and demonstrated a highly significant reduction in breast cancer mortality (death rate 0.82; 95% CI: 0.73-0.93) with BPs in postmenopausal women only. This was irrespective of tumour type, BP choice, and schedule. In the meta-analysis, the definition of menopausal status was a clinical definition of premenopausal, perimenopausal, and postmenopausal (natural or induced). If clinical menopausal status was unavailable, years of age was taken to define menopause (grouped as <45 [premenopausal], 45-54 [perimenopausal], ⩾55 [postmenopausal]). In clinical practice, however, it is well recognized that menopause cannot be reliably assumed by age. 22 If the clinical definition of menopause is not possible, the evaluation of a panel of female hormones at the start of BPs, including inhibin A, oestradiol, and follicle-stimulating hormone, may assist patient selection for the treatment with adjuvant BPs if these are in assay-specific postmenopausal range, as evidenced from the evaluation of these hormones in baseline serum samples of 865 patients randomized in the AZURE trial. 23 In addition, this study showed that baseline oestradiol and follicle stimulating hormone (FSH) levels appeared to influence the pattern of disease recurrence, with a propensity for recurrences outside bone in women with postmenopausal levels irrespective of treatment received. 23 This may indicate that the distribution of disseminated tumour cells (DTCs) at the time of initiation of BPs could influence the disease-modifying efficacy of BPs within the bone microenvironment.
Following the meta-analysis, BPs have been incorporated into clinical care in Europe and America with relevant guidelines published to aid clinicians on how to select patients for treatment and suggested drug dosing schedules. 16 , 24 The published guidelines have recommended oral clodronate or IV ZA as choice of agent; however, ibandronate may be an additional choice of agent following results from the SWOG S0307 study of 6097 patients with stage I-III breast cancer randomized to receive 3 years of clodronate (1600 mg daily), ibandronate (50 mg orally daily), or ZA (4 mg IV monthly for 6 months, then 3-monthly for 2.5 years), which showed no difference in 5-year DFS between the 3 arms. 25 Recently, the phase III SUCCESS A trial compared 2 years of adjuvant ZA with 5 years, post-chemotherapy in 3754 women with high-risk early breast cancer, and found no difference in DFS or overall survival between the 2 groups, suggesting that the recommended 3 to 5 years in published clinical guidelines could be reduced further. 26
Denosumab
In the ABSCG-18 study of postmenopausal women, Gnant and colleagues reported fewer DFS events in patients treated with denosumab (n = 167) compared with placebo (n = 203), equivalent to an 18% reduced risk of recurrence at a median follow-up of 4 years; 18 however, the study was unblinded and patients offered active treatment from 2016, so longer term survival data from this trial may not become available. The role of adjuvant denosumab was evaluated in the D-CARE study (NCT01077154) which recently reported at American Society of Clinical Oncology. 27 In total, 4509 premenopausal and postmenopausal patients with early breast cancer were randomized to receive standard (neo)adjuvant therapy +/–denosumab 120 mg subcutaneous placebo monthly 6× then 3 monthly for up to 5 years. The primary endpoint was bone metastasis free survival (BMFS), and no benefits for the addition of denosumab were seen in the overall population after a median follow-up of 67 months. Surprisingly, denosumab did not improve disease outcomes in the postmenopausal subset (n = 2149), which contradicts the results of the ABCSG-18 study. While denosumab does have a role in fracture prevention in postmenopausal low recurrence risk early breast cancer patients, it is now apparent that for those in whom risk of recurrence is greater, a BP would be the preferred choice of BTA.
Outstanding Questions – Can Preclinical Research Help?
In keeping with the clinical data, there have been a large number of preclinical studies describing anti-tumour effects of ZA alone or in combination with chemotherapy against breast cancer cells in the bone environment (see Table 1). Preclinical models have also shown increased efficacy of ZA against metastatic outgrowth of dormant tumour cells in the skeleton of ovariectomized mice compared with sham-operated animals. 36 It was originally hypothesized that these anti-tumour effects were largely the result of ZA-induced osteoclast inhibition leading to a disruption of the vicious cycle. This hypothesis appeared to be supported by mouse experiments using the mouse monoclonal antibody to RANKL (fcOPG) that also showed reduced tumourigenesis in the bone of ovariectomized mice compared with sham-operated animals. 45 In the clinic, however, administration of denosumab had no effect on metastasis in premenopausal or postmenopausal women. It therefore appears that osteoclast activity is not the dominant driver of bone metastasis, and further research is required to establish the key mechanisms that promote this condition.
Summary table of preclinical studies showing anti-tumour efficacy of zoledronic acid alone or in combination with other therapeutic compounds.

Evidence that adding ZA to chemotherapy inhibits growth of breast cancer cells outside of bone in mouse models (see Table 1) and reduces breast cancer recurrence in non-bone sites in postmenopausal women suggests that ZA is able to elicit anti-tumour effects outside of the bone environment. ZA is a potent inhibitor of the mevalonate pathway; 44 this pathway is ubiquitous to all cell types and despite only being present in the circulation for ~4 h, adding ZA 24 h after doxorubicin has been shown to activate the mevalonate pathway and increase apoptosis in breast cancer cells in mouse models. 33 It is possible that the differential anti-tumour effects of ZA in bone and in peripheral metastasis, according to menopausal status, are not due to reduced bone resorption but are driven by direct ZA-induced anti-tumour affects.
The differential effects of ZA in premenopausal and postmenopausal women indicate a role for oestradiol in driving resistance to anti-tumour effects of ZA in peripheral metastasis. Evidence from preclinical models has shown apposing roles for oestradiol; we and others have shown that low levels of oestradiol caused by ovariectomy promote outgrowth of tumour cells already disseminated in bone, 45 , 46 whereas supplementing mice with oestradiol enhances spontaneous metastasis of oestrogen receptor positive (ER+ve cells) to bone. 39 Bone metastases were inhibited in both of these models by ZA in the absence of chemotherapy. Taking the clinical and preclinical data together, data suggest that high oestradiol may attract tumour cells to bone and may influence their survival and dormancy in the bone microenvironment or cause them to disseminate to other organs.
The mechanisms of how oestradiol and ZA interact to affect tumour growth in bone and non-bone sites have not been identified. There is a suggestion from in vivo studies that low oestradiol levels may enhance ZA action through increasing interleukin (IL)-1 expression that ‘unmasks’ DTCs and makes them susceptible to death from high local concentrations of ZA in the bone microenvironment. 47 Both oestradiol and ZA have profound effects on the immune system: oestradiol has well-documented immunosuppressive effects via upregulation of programmed death ligand 1 (PD-L1). 48 Recent data support that oestradiol also increases PD-L1 in breast cancer cells, and high PD-L1 expression levels in breast cancer inhibit T-cell anti-tumour responses. 49 On the other hand, ZA acts as an immune modulator by significantly inhibiting expansion of regulatory T cells. 50 It is, therefore, likely that oestradiol-induced PD-L1 expression on tumour cells interferes with ZA activity in premenopausal women. Further research is underway in our laboratory that will establish whether targeting breast cancer cell PD-L1 with avelumab in combination with ZA has the potential to improve the anti-tumour efficacy of BPs in premenopausal women.
In contrast to ZA, denosumab specifically targets RANKL leading to osteoclast apoptosis and reduced bone resorption. In addition, RANKL is a key mediator of progesterone action and is expressed by a number of different breast cancer cell lines. Systemic inhibition of RANKL in preclinical models blocked proliferation of the mammary epithelium and inhibited progesterone-driven tumorigenesis.51–53 These findings gave hope that denosumab would elicit a 2-pronged attack directly killing tumour cells and generating an unfavourable environment for bone metastases to establish. Unlike ZA, the effects of denosumab on anti-tumour immune cells are not reported, and there is limited data on the effects of this drug on different breast cancer subtypes. The failure of denosumab to elicit anti-metastatic effects in women with breast cancer in the clinic highlights the need for further preclinical studies. Identifying why this denosumab appears to be a less effective anti-metastatic therapy than initially hypothesized will allow research into novel methods of increasing its therapeutic efficacy.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: Time for literature review/manuscript writing provided by Weston Park Cancer Charity (Grant no. CA140).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
PO and CW were equally responsible for writing and reviewing of final submission.