
Abstract
The number of patients with breast cancer diagnosed with sleep disturbance has grown substantially within the United States over the past 20 years. Meanwhile, there have been significant improvements in the psychological treatment of sleep disturbance in patients with breast cancer. More specifically, cognitive behavioral therapy for insomnia (CBT-I), mindfulness, and yoga have shown to be 3 promising treatments with varying degrees of benefit, supporting data, and inherent limitations. In this article, we will outline the treatment approach for sleep disturbance in patients with breast cancer and conduct a comprehensive review of CBT-I, mindfulness, and yoga as they pertain to this patient population.
Introduction/Epidemiology
According to the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition), insomnia disorder is defined as the “dissatisfaction with sleep quantity or quality” associated with difficulty initiating and/or maintaining sleep that causes clinically significant distress or impairment, occurs despite an adequate opportunity for sleep and occurs at least 3 nights per week for at least 3 months, is not attributable to the physiological effects of a drug/medication, another sleep-wake disorder, or comorbid mental health and/or medical conditions 1 (see Table 1).
Definitions of key terms commonly encountered in sleep medicine research.
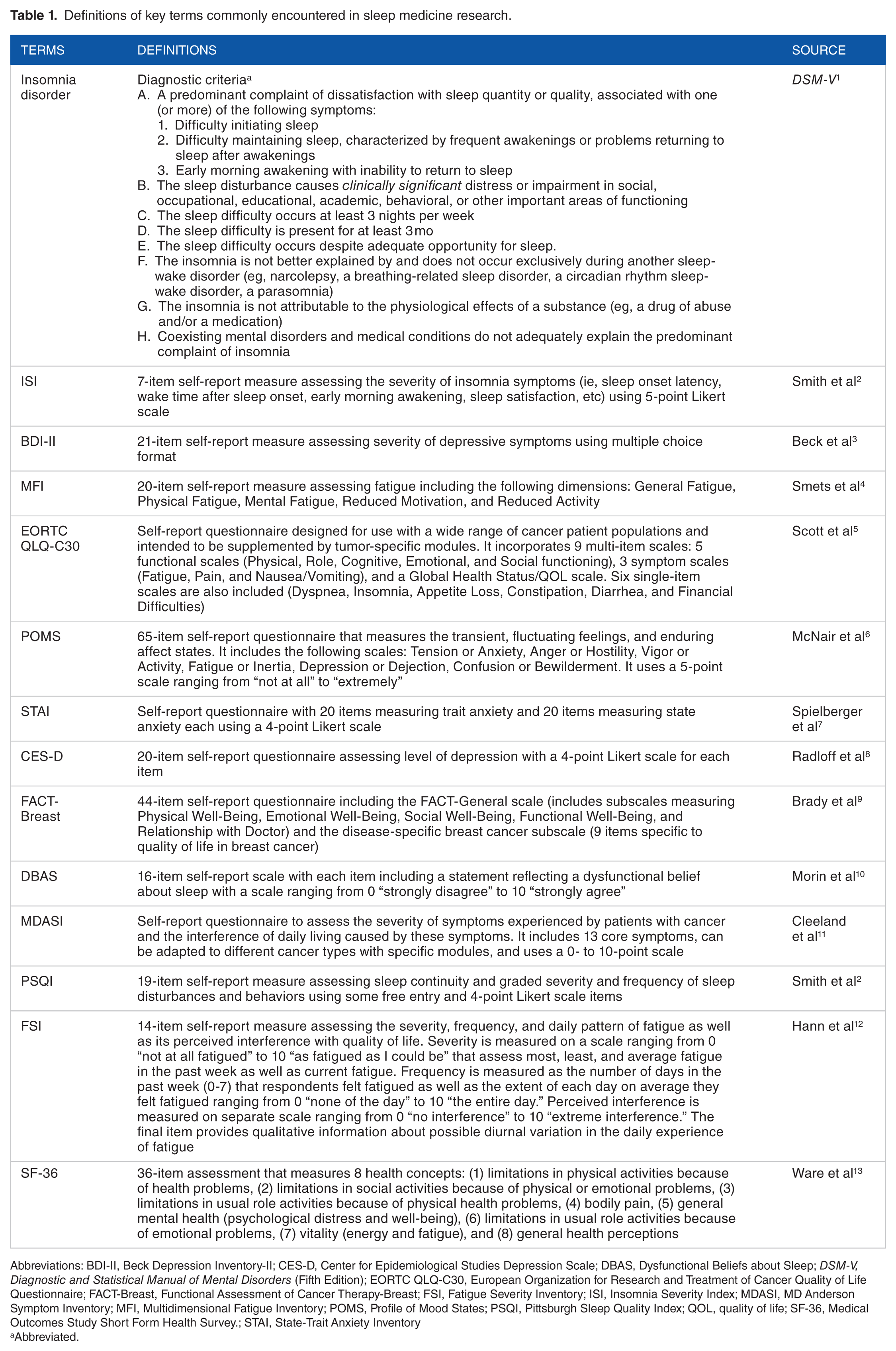
Abbreviations: BDI-II, Beck Depression Inventory-II; CES-D, Center for Epidemiological Studies Depression Scale; DBAS, Dysfunctional Beliefs about Sleep; DSM-V, Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition); EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; FACT-Breast, Functional Assessment of Cancer Therapy-Breast; FSI, Fatigue Severity Inventory; ISI, Insomnia Severity Index; MDASI, MD Anderson Symptom Inventory; MFI, Multidimensional Fatigue Inventory; POMS, Profile of Mood States; PSQI, Pittsburgh Sleep Quality Index; QOL, quality of life; SF-36, Medical Outcomes Study Short Form Health Survey.; STAI, State-Trait Anxiety Inventory
Abbreviated.
With 246 660 new diagnoses and 40 450 deaths in 2016, breast cancer remains the most commonly occurring and third most lethal cancer among women in the United States. 14 Approximately 12.3% of women will be diagnosed with breast cancer at some point in their lifetime, and it is estimated that there are currently 3 053 450 women in the United States living with the diagnosis. Due to improved screening protocols and advances in multimodality treatment, the 5-year survival for patients with breast cancer of all stages has increased significantly over the past 40 years and is now close to 90%. 15
Sleep disturbance, a broad term that encompasses patient complaints of difficulty falling asleep and/or maintaining sleep (insomnia) and daytime fatigue, is one of the most common symptoms faced by US patients with breast cancer (20%-40% vs 10% in age-matched controls) and long-term survivors (23%-44% of patients 2-5 years following the completion of their cancer treatment),16–23 regardless of disease stage or type of treatment received. Even though sleep disturbance is one of the most distressing symptoms faced by patients, it is frequently underreported and/or overlooked in both clinical trials and practice. 24 Furthermore, studies have found that untreated sleep disturbance among patients with breast cancer is associated with increased distress, anxiety/depression, immunosuppression/infection, substance abuse, pain, perception of comorbid psychological/medical condition severity, cardiovascular morbidity, and increased health care utilization and costs. In addition, untreated sleep disturbance has been associated with decreased quality of life (QOL), cognitive function, verbal and motor skill function, work productivity, cancer-free survival, and cancer-specific overall survival.25–32
Some of the most efficacious and/or promising of the psychologic interventions are cognitive behavioral therapy for insomnia (CBT-I), mindfulness, and yoga. In this article, we will outline the treatment approach used in patients with breast cancer diagnosed with sleep disturbance and conduct a comprehensive review of CBT-I, mindfulness, and yoga as they pertain to this patient population.
Methods
A search of the PsycINFO database was conducted using the following search terms: (1) breast cancer AND insomnia AND cognitive behavioral therapy; breast cancer AND sleep AND cognitive behavioral therapy; (2) breast cancer AND insomnia AND mindfulness; breast cancer AND sleep AND mindfulness; and (3) breast cancer AND insomnia AND yoga; breast cancer AND sleep AND yoga. Articles were evaluated using the following inclusion criteria: (1) written in the English language, (2) published between 2000 and 2016, (3) published in a peer-reviewed journal, (4) included all the search terms in the text, (5) full text available via Emory University e-library, (6) addressed the efficacy of the relevant intervention for women with breast cancer, and (7) had pre- and postintervention measures regarding insomnia/sleep disturbance.
Treatment Approach
According to the Behavioral Model of Insomnia, there are 3 factors that contribute to the development of chronic insomnia, which include the following: (1) predisposing factors (eg, family history, hyperarousal trait), (2) precipitating factors (ie, stressful life events, including but not limited to sudden unexpected changes in sleep schedule, or cancer-related disease and treatment factors), and (3) perpetuating factors (eg, spending excessive time in bed, anxious thoughts about sleep. 33 Given disease, patient, resource, and clinician heterogeneity, the first step in the treatment of patients with breast cancer diagnosed with sleep disturbance involves the identification and removal of potential reversible inciting factors, which often must be individualized to meet the unique needs/situation of the patient.17–21 As they can have a tremendous influence on a patient’s sleep pattern, clinicians should assess for and address the following confounding factors during their initial patient assessment: (1) disease-related (ie, laboratory and radiographic studies and where patients are in their cancer diagnosis/treatment timeline: untreated vs actively receiving treatment vs in a period of active surveillance vs a long-term survivor); (2) medication-related (ie, receipt of sleep disturbance–inducing medications); (3) situational (eg, hospitalization, inconsistent sleep-wake schedules); (4) psychological (eg, distress levels, coping with a cancer diagnosis, and underlying or concurrent anxiety/depression); (5) financial (ie, high cost of cancer diagnosis and treatment); (6) family/friend relationships (ie, conflict stemming from being newly dependent on others for activities of daily living [ADLs] and a cancer treatment scheduling burden); (7) professional (ie, patient personal dissatisfaction associated with the ability or inability to continue working in their profession/earn a steady income); (8) existential (ie, fear/uncertainty of the future); (9) hormonal, which is commonly seen with chemotherapy (ie, associated with early menopause) and/or endocrine therapy (ie, estrogen-depleting agents associated with sleep disturbance); (10) clinically relevant comorbidities (ie, the presence, or lack thereof, of a concurrent pain disorder, obstructive sleep apnea, or substance use disorder); and (11) patient-related factors (ie, nutritional and functional status).
After these factors are considered, but before active psychologic or medication-based treatment is employed, clinicians generally recommend environmental and/or behavioral interventions that promote an environment that fosters sleep and sleep-compatible behaviors. Patients are often instructed to sleep in an environment that is cool, well ventilated, dark, and quiet (ie, a white-noise machine is commonly recommended for patients living in noisy environments).34–38 In an effort to modulate their normal circadian rhythm/sleep-wake cycle, patients are encouraged to increase their exercise/daytime activity and daylight exposure (ie, artificial full spectrum or blue light are commonly recommended for patients unable to increase their daylight exposure).39,40 Patients are also encouraged to avoid certain activities before bed (ie, watching television, listening to loud music, using computers), make lifestyle modifications (ie, reducing or avoiding daytime naps, large meals or excessive fluids at bedtime, and caffeine), and maintain or slightly alter their familiar bedtime/wind-down routines (ie, showering, light snack, listening to soothing music) as needed to allow for a feasible wind-down period that takes into account any changes in performance status. For the hospitalized patient with breast cancer with sleep disturbance, to maintain a more calm, comfortable, quiet, and sleep-promoting environment, it is recommended that clinicians/staff (1) perform patient assessments and/or administer/dose-adjust medication/fluid/nutrition while the patients are awake, (2) establish sleep-conducive visiting hours that allow for a bedtime wind-down period, (3) provide the patient with a comfortable memory foam mattress, and (4) dim the lights in the vicinity of the patient’s room starting in the early evening.
After reversible inciting factors are addressed and it is determined that active treatment for sleep disturbance is indicated, psychologic and/or pharmacologic interventions (long-term response rates ranging from 30% to 40%) are often then considered.31,41 The order in which specific treatments are used varies considerably, depending on provider training/experience, resources available, socioeconomic factors, patient-related factors, and disease-related factors. Psychologic interventions are often recommended first in the treatment of sleep disturbance among patients with breast cancer, as they are noninvasive, can safely be used long term, and are associated with a similar efficacy to pharmacologic interventions.42–48 This is important to consider as pharmacological approaches can be associated with significant adverse effects (ie, cognitive impairment, fractures, and accidental injury), and such effects may be compounded in vulnerable patient populations (ie, drug-drug interactions in patients taking numerous medications, patients with renal and/or hepatic organ dysfunction causing impaired drug metabolism and elimination, and patients aged >65 who are more sensitive to the drug’s adverse effects).42–48 This recommendation is supported by the following organizations: (1) American Society of Clinical Oncology (ASCO) 49 ; (2) American Academy of Sleep Medicine (AASM) 50 ; (3) American College of Physicians (ACP)51,52; (4) National Comprehensive Cancer Network (NCCN), 41 which issued an algorithm-based, expert, and evidence-derived treatment guideline specifically for patients with cancer diagnosed with sleep disturbance; (5) the Pan-Canadian Public Health Network (PHN), 53 an organization that gives appraisals of health care interventions in Canada, based on cost-effectiveness; and (6) National Institute for Health and Care Excellence (NICE), 54 an organization that gives appraisals of health care interventions for the United Kingdom, based on cost-effectiveness. As is the case for most treatment recommendations, there are certain exceptions where pharmacologic interventions may be used before psychologic interventions (ie, need for fast-acting intervention or patients with advanced disease who may have poor functional status and are unable to participate in active psychologic therapy).
Cognitive Behavioral Therapy for Insomnia
Cognitive behavioral therapy for insomnia is one of the most effective therapeutic modalities for sleep disturbance in patients with breast cancer55–60 and has been associated with the improvement not only in patient-reported sleep measures but also in patient psychological distress levels and QOL. Cognitive behavioral therapy for insomnia is sustained over a longer time, when compared with pharmacologic therapies, because it addresses the cause of the sleep disturbance and requires active patient participation in acquiring and maintaining skills to prevent and treat it. Based on the theory that maladaptive behaviors and dysfunctional thoughts perpetuate sleep disturbance to the point at which a patient can have symptoms without the presence of precipitating factors, CBT-I works to examine and change these thoughts and behaviors through a structured program that incorporates several different steps.61–63 It is administered over a time span of 4 to 12 weeks, emphasizes behavioral change (ie, stimulus control, sleep restriction) and cognitive restructuring (modifying dysfunctional thoughts about sleep and the impact of limited sleep on daytime functioning, developing realistic sleep expectations), allows for the review and integration of treatment skills, encourages patient troubleshooting with the clinician, and incorporates treatment components that help to maintain the desired treatment effect and prevent disease relapse. To gauge treatment effect, patients are encouraged to complete sleep logs as they learn and apply various treatment strategies.64–67 Cognitive behavioral therapy for insomnia, as is the case with any intervention, has certain limitations, which include lacking enough adequately trained clinicians, being somewhat time-intensive to administer when compared with pharmacologic interventions, being potentially more expensive in the short term, and requiring complete patient participation in treatment (which may not be feasible for some patients related to disease factors, scheduling issues, or in cases of limited cognitive functioning in which family/friend supports are not available to attend appointments and help the patient perform the treatment recommendations). Modifications to certain CBT-I treatment components (ie, Sleep Restriction) may also be indicated in certain patient populations (ie, as sleep deprivation may be associated with lowered threshold for mania/hypomania, seizures, and panic attacks in patients with a history of such events). 57
There are several studies supporting the use of CBT-I for sleep disturbance. One study looked at 10 women with nonmetastatic breast cancer who completed chemotherapy and radiotherapy at least 1 month before and who endorsed symptoms of sleep disturbances, which were determined by expert clinicians to be caused or exacerbated by the cancer diagnosis and/or treatment. 31 The treatment program consisted of 8 weekly 90-minute group sessions. The assessment time points were immediately pre- and posttreatment, at 3 and 6 months after therapy, and included both subjective (ie, sleep diary, self-report questionnaires) and objective (ie, polysomnography) measures. There were significant improvements in the patient’s total wake time (87.8 minutes [SD = 28.8] pretreatment vs 63.9 minutes [SD = 19.9] posttreatment; P = .02), which improved even further at 6 months posttreatment (mean of 53.8 minutes [SD = 9.6] vs 63.9 minutes [SD = 19.9] posttreatment; P = ns), and sleep efficiency (see Table 1; mean of 81.4% [SD = 5.9] pretreatment vs 85.1% [SD = 4.3] posttreatment; P = .04), which improved even further at 6 months posttreatment (mean of 87.7% [SD = 2.0] vs 85.1% [SD = 4.3] posttreatment; P = .04). These findings were further supported by the significant improvement in Insomnia Severity Index (ISI) scores among patients treated with CBT-I (pretreatment 16.9 vs immediately posttreatment 6.1; P = .004), which were sustained for 6 months posttreatment (6.1 vs 6.9; P = ns). In addition, CBT-I in patients with breast cancer diagnosed with sleep disturbance was associated with a sustained (at least 6 months) improvement in the following: (1) mood, as measured by the Beck Depression Inventory-II (BDI-II; Table 1); (2) vitality, as measured by the Multidimensional Fatigue Inventory (MFI; Table 1); and (3) QOL, as measured by the European Organization for Research and Treatment (EORTC) of Cancer QOL Global and Cognitive subscales. Another randomized controlled trial (RCT) by Savard et al 61 supported these findings in this patient population and showed improvements not only in sleep assessment parameters but also in emotional well-being and QOL more than 1 year following initial CBT-I treatment. Another research group conducted an RCT comparing CBT-I (included sleep education, sleep restriction, stimulus control, and sleep hygiene) with placebo (included only sleep education and hygiene) in patients with breast cancer diagnosed with sleep disturbance. 68 Patients in both groups (CBT-I: n = 38; placebo: n = 34) first underwent a 2-week pretreatment evaluation, which was then followed by 4 weekly group sessions, and was finally concluded by a 2-week posttreatment evaluation. From pretreatment to immediately posttreatment, patients in the CBT-I group (compared with the placebo group) had statistically significant improvements in fatigue (as measured by the Profile of Mood States [POMS] fatigue scale; Table 1), trait anxiety (as measured by the State-Trait Anxiety Inventory [STAI] trait scale; Table 1), depression (as measured by the Center for Epidemiological Studies Depression scale [CES-D], and QOL [as measured by the Functional Assessment of Cancer Therapy [FACT]-Breast; Table 1). Another RCT of patients with breast cancer diagnosed with sleep disturbance showed that treatment with CBT-I (vs placebo) resulted in statistically significant improvement in the components of sleep disturbance including sleep latency (immediately posttreatment: P = .007; 3 months posttreatment: P = .0005; and 6 months posttreatment: P = .003), generalized insomnia, physical functioning, sleep attitudes, sleep hygiene, and cognitive functioning. 22 There were no significant posttreatment differences between the 2 groups in terms of QOL, mood, or fatigue. However, this may have been due to a ceiling effect where patient’s QOL was very high at baseline, even before treatment.
One of the major difficulties in clinical practice is trying to individualize patient care so that there are unbiased tools available to help clinicians determine what treatment will lead to the best response (short term and long term), what therapy is most likely to be associated with better patient adherence, what side effects each treatment has, etc. Tremblay et al 62 attempted to answer these questions by examining predictive factors associated with CBT-I response for patients with breast cancer diagnosed with sleep disturbance. The study treatment program included 8 weekly 90-minute individualized sessions and assessments (via subjective questionnaires and objective polysomnography), at 3 time points (pretreatment, immediately posttreatment, and 6 months posttreatment). Patients who napped frequently during the daytime (during more than half of the days of the week) and who had baseline maladaptive, irrational, and pessimistic thoughts regarding sleep (Dysfunctional Beliefs about Sleep [DBAS]) and CBT-I efficacy were significantly less likely to have a treatment response. When controlling for other variables, adherence to behavioral strategies best predicted the subjective improvement in sleep disturbance and other related symptoms (ie, emotional well-being, QOL, etc), and these effects were maintained for at least 3 months posttreatment. Similarly, Matthews et al 64 found that during a CBT-I program of 6 weekly sessions, there was a significant decline in adherence to behavioral strategies such as the prescribed rise time (P < .05) and the total time in bed (P < .05). In this study, improved adherence was associated not only with fewer posttreatment awakenings after sleep onset (P < .05) but also with improved energy, motivation, and overall sleep quality.
To address the relative time-intensive nature of CBT-I and the patient’s treatment adherence, an RCT was performed which compared the following 3 groups: (1) individual face-to-face CBT-I (6 weekly sessions of about 50 minutes each, n = 81), (2) video-based CBT-I (60-minute video broken into 6 segments + 6 booklets, n = 80), (3) and no treatment (n = 81) in patients with breast cancer who had received radiation therapy in the past 18 months and who endorsed symptoms of sleep disturbance or were using pharmacologic medications to address the problem. 65 When compared with those who received the placebo, patients in the 2 treatment arms had improvements in ISI scores, daily sleep diary content, and actigraphy assessments. Patients who received face-to-face CBT-I (vs video-based or no treatment group) had a significantly greater sleep disturbance remission rate (71.3% vs 44.3%, P = .005), along with a statistically significant decrease in early morning awakenings, symptoms of depression, daytime fatigue, and irrational thought/beliefs about sleep. As a result of this study, face-to-face format for CBT-I delivery in patients with breast cancer diagnosed with sleep disturbance remains the standard approach; however, self-help treatment formats still appear valuable and may constitute an appropriate entry level of care in a stepped care model.
Mindfulness
Mindfulness is an ancient practice that has existed for more than 2500 years and involves paying attention “on purpose, in the present moment, and non-judgmentally.” 69 It can be characterized by attitudinal foundations including nonjudging, patience, seeing things as if for the first time, trust, nonstriving, acceptance, letting go, and compassion. Mindfulness-based therapy for insomnia (MBT-I) is a meditation-based program that integrates not only mindfulness but also behavioral techniques, delivered through meditations and group discussions.69,70 It is thought that MBT-I improves sleep disturbances in patients with breast cancer by one or more of the following: (1) increasing melatonin levels, (2) reducing hyperarousal through metacognition shifting, and (3) by addressing the cardiac (ie, palpitations) and respiratory abnormalities (ie, false suffocation alarm [see Table 1], hyperventilation, etc) associated with anxiety and rumination. Evidence supporting these findings came from studies that showed that mindfulness treatment reduced patients’ cortisol and catecholamine levels (that were increased by sleep disturbance). Mindfulness also helped to create a newly conditioned response that was not disruptive in the patients’ day-to-day life (reciprocal inhibition), as it allowed them to remain detached, yet able to detect and correct the cognitive distortions that accompany sleep disturbance (ie, overestimation of sleep deprivation and its potential consequences).71–73
Mindfulness-based stress reduction (MBSR), the most commonly practiced mindfulness program in the United States, teaches individuals how to cope with stressors more effectively and foster present-moment awareness. It is an 8-week course that incorporates mindful meditation, Hatha yoga, and previously mentioned mindfulness attitudinal foundations 74 (see Table 1). Among patients with breast cancer diagnosed with sleep disturbance, mindfulness treatment programs have been shown to decrease not only sleep disturbance-related symptoms (ie, excessive daytime fatigue) but also psychological distress and fears of cancer diagnosis/recurrence/progression, health-related QOL including physical pain and the ability to perform ADLs, social functioning, and emotional well-being (anxiety and depression). Given the unique hardships faced by patients with breast cancer, Lengacher et al 70 created an MBSR for breast cancer (MBSR-BC) protocol, which was specific for patients with breast cancer and shown to improve (1) sleep onset latency and maintenance, (2) emotional stability, (3) present-moment awareness, (4) ability to be open to one’s own experience without judgment, and (5) ability to think purposefully rather than ruminating.
Shapiro et al 75 conducted an RCT evaluating MBSR as a treatment for the stress associated with a diagnosis of sleep disturbance in patients with breast cancer. Participants were randomized to an MBSR treatment program (six 2-hour weekly sessions and a 6-hour silent retreat) or a control group (using a workbook of resources and a self-monitoring diary of coping strategies), and assessments were made at 4 time points (baseline, immediately posttreatment, 3 months posttreatment, and 9 months posttreatment). Both treatment groups were found to have significant improvements on subjective measures of sleep quality (ie, perception of refreshing sleep) but not sleep efficiency (see Table 1). However, participants in the MBSR group who reported more mindfulness practice had significantly improved sleep quality and were more likely to self-report a feeling of being well rested, but only when their sleep disturbance was associated with stress. In patients with breast and prostate cancer, Carlson et al evaluated the effect of an 8-week MBSR intervention (relaxation, meditation, yoga, and daily home practice) on various parameters including QOL, mood, stress, serum cortisol (measured 3 times per day), dehydroepiandrosterone sulfate (DHEAS), melatonin, lymphocyte counts, and various cytokine levels.76–81 The researchers found that the treatment group (vs placebo) self-reported statistically significant posttreatment improvements in overall QOL, symptoms of stress, sleep quality, and sleep duration (7.1 hours pretreatment vs 7.6 hours posttreatment), which were irrespective to patient adherence to treatment. With treatment, the following observations were made: (1) no significant changes in the patient’s mood or serum laboratory cortisol, DHEAS, melatonin, or lymphocyte count; (2) normalization of the 24-hour serum cortisol pattern; (3) improvement in QOL, which correlated with a decrease in afternoon cortisol (but not with morning/evening cortisol); (4) an increase in the T-cell–mediated interleukin 4 production; (5) a decrease in T-cell–mediated interferon gamma production; and (6) a decrease in the natural killer cell–mediated production of interleukin 10. The changes seen in the laboratory parameters associated with immune function were similar to those that were previously described in patients with an improvement in depression. Study limitations included lack of a control group and high levels of psychological and immunological functioning of participants at the start of the study, thus leaving little room for additional improvement.
Meanwhile, Lengacher et al 82 conducted another RCT which examined the psychological and physical symptoms of breast cancer survivors following 6 weeks of treatment with MBSR (vs no treatment). Among patients who received MBSR (vs without MBSR), there was a significantly smaller percentage of patients who reported depression (6.3% vs 9.6%), anxiety (28.3% vs 33.0%), and fear of cancer recurrence (9.3% vs 11.6%). There was also a significantly higher percentage of patients that received MBSR (vs without MBSR) who reported increased energy levels (53.5% vs 49.2%), physical functioning (50.1% vs 47.0%), and ability to perform their ADLs (49.1% vs 42.8%), especially among those who were most adherent to the MBSR treatment protocol. Specific parameters/components of MBSR, including total minutes of sitting meditation and body scan (a form of mindfulness meditation practice involving bringing present-moment awareness to different parts of the body), were significantly associated with improved patient well-being and QOL. Meanwhile, minutes of walking meditation (a form of mindfulness meditation practice involving bringing present awareness to walking) were associated with a decreased fear of recurrence and improved physical functioning. In a follow-up study using the MD Anderson Symptom Inventory (MDASI), which includes measures of symptom severity and degree of interference with daily functioning, assessments occurred at baseline and within 2 weeks of completion of an MBSR treatment program. Patients who received MBSR (vs those who did not) were found to have statistically significant reductions in sleep disturbance and reductions in 3 symptom clusters including (1) gastrointestinal (ie, nausea, vomiting, lack of appetite, dry mouth, shortness of breath, numbness), (2) cognitive/psychological (ie, distress, sadness, remembering, pain), and (3) fatigue (ie, fatigue, disturbed sleep, drowsiness). Another RCT, which incorporated a 6-week MBSR-BC treatment group and a group that did not receive MBSR-BC, used both subjective (ie, sleep diaries, the Pittsburgh Sleep Quality Index [PSQI]) and objective (ie, actigraphy) sleep measures and took assessments at various time points (baseline, immediately postintervention, and at 12-week follow-up). 83 Patients who received MBSR-BC (vs those who did not) were found to have a significant improvement in their self-reported and actigraphy-associated sleep parameters at 12 weeks posttreatment, including sleep efficiency (78.2% vs 74.6%, P = .02) and number of awakenings (93.5 vs 118.6 minutes, P < .01). Minutes of MBSR-BC practice were not found to be associated with any of the objective or subjective sleep parameters.
Recently, Bower et al 84 conducted an RCT of women diagnosed with early-stage breast cancer at or before age 50 and who completed their cancer treatment. The patients were randomly assigned to either a 6-week Mindful Awareness Practices (MAPS) intervention group or a wait list control group, and assessments of stress, depression, and inflammation were done at 3 time points (baseline, 6 weeks posttreatment, and 3 months posttreatment). The intervention included 6 weekly 2-hour group sessions (patients were also encouraged to engage in daily home practice), which were focused on psychoeducation of mindfulness, relaxation, the mind-body connection, maintaining health, preventing breast cancer recurrence, meditation, and gentle movement exercises. Those patients in the intervention group (vs no intervention) had the following significant effects which were maintained at 3 months posttreatment: (1) decreased perceived stress, cancer-related distress and intrusive thoughts (P = .002), and reduced fear of recurrence (P = .048); (2) decreased pro-inflammatory gene expression and inflammatory signaling; (3) decreased fatigue (P = .007) and sleep disturbance (P = .015); (4) decreased hot flashes/night sweats (P = .015); and (5) improved affect (P = .03) and sense of peace and meaning (P = .001). This study suggests that a 6-week mindfulness-based program supports short-term improvements in stress, behavioral symptoms, and pro-inflammatory signaling in premenopausal patients with breast cancer. Participants in mindfulness interventions have reported an overall positive experience. Kvillemo and Bränström 74 used a semistructured interview format to evaluate the perceived experiences of patients with cancer who participated in an 8-week mindfulness training course. Most patients reported that they enjoyed the program because it was nonjudgmental, emphasized acceptance, involved group process/sharing experiences with peers with similar experiences, and emphasized present-moment awareness. Participation in the program was associated with increased calmness and sense of well-being, improved sleep quality, increased energy, and less physical pain. Thus, not only do patients appear to derive benefit from the intervention in terms of sleep disturbance but it is also acceptable to participants and may translate to improved attendance and active participation.
Yoga
Yoga, derived from the Sanskrit word YUJ meaning “to join the mind,” is an ancient tradition that has been practiced for thousands of years in East Asia. 85 However, it had not become a mainstream practice within the United States and other Western societies until recently. In fact, the National Health Interview Survey estimated in 2012 that 8.9% and 13.2% of the US population practiced yoga in the previous year and/or during their lifetime, respectively.86–90 Compared with nonpractitioners, US yoga practitioners were more likely to be young, female, non-Hispanic white, college educated, have a higher socioeconomic status, and have a better overall health status. 86 Despite these practice disparities, yoga has been found to be not only feasible but also well accepted by low-income minorities (when made available). Yoga, through its 3 main components (postures, breathing, and meditation), has been found to be beneficial in terms of increased muscle strength, flexibility, range of motion, balance, energy, relaxation, sense of well-being, pain control, stress control, and sleep quality.90–92 It has been theorized that yoga improves sleep disturbance in patients with breast cancer by inducing deep relaxation, reducing sympathetic arousal and anxiety, and improving oxygen consumption, relaxation awareness, emotional stability, and sleep quality.
Zhang et al 93 conducted a meta-analysis of RCTs evaluating the effect of yoga (ie, Hatha, Integral, Vini) on psychologic functioning and QOL in patients with breast cancer and showed a significant improvement in QOL (P = .03) and perceived stress (P < .01) for participants in the yoga intervention (s. the control group). Although the intervention group appeared to have an improvement in psychologic outcomes, such as anxiety, depression, distress, and sleep disturbance, these were not found to be statistically significant. Another group conducted a pilot study, in which patients with breast cancer were randomized to a restorative yoga intervention group (10 weekly 75-minute classes) or a wait list control group. 94 The restorative yoga intervention was based on the Integral Yoga tradition and included postures, relaxation, breathing practices, and meditation and emphasized awareness and the experience of peace, well-being, and being gentle with oneself. Participants completed assessments at baseline and at week 10, which was immediately postintervention for the yoga group. A trend toward improvements in mood and a sense of peace and meaning was found in the yoga group as compared with the wait list control group. Women who endorsed higher negative affectivity and lower emotional well-being at baseline demonstrated greater benefit from participation in the yoga intervention. According to the FACT fatigue scale, an instrument developed to assess fatigue in patients with cancer, there was a significant within-group improvement in fatigue for the yoga group but not for the control group. Although there were no significant between-group or within-group differences on the PSQI, sleep disturbance had an interaction (P = .028) with the baseline, indicating that class attendance was more beneficial for participants who started out with higher levels of sleep disturbance. There was a similar interaction for use of sleep medication (P = .04), in which those with higher initial use of sleep medication reported more benefit from increased class attendance.
In another pilot study, Jacobsen et al 95 investigated whether a yoga intervention (Iyengar yoga, a traditional form of Hatha yoga, with classes that met for 90 minutes twice weekly for 12 weeks) mitigated some of the adverse effects of aromatase inhibitor treatment in postmenopausal patients with breast cancer who completed chemotherapy and/or radiotherapy at least 1 month earlier. The mean number of classes attended was 13.8 (58%), but patient surveys indicated that this was primarily due to competing family and work demands, rather than disinterest. As a result, the researchers hypothesized that attendance may be improved by a community/Internet-based delivery format to make class times and locations more convenient. Despite the limited overall attendance, significant improvements were found on measures of overall pain severity and hot flash–related distress, whereas there were no changes seen regarding depressive symptoms or insomnia. In addition, significant improvements in fatigue were found in individuals who initially reported mild fatigue but not in those who had reported more severe symptoms of fatigue at baseline. Derry et al 96 conducted an RCT in which patients with breast cancer were placed either in a wait list control group or in a yoga intervention group (twice-weekly Hatha yoga classes for 12 weeks) and completed assessments at 3 time points (pretreatment, posttreatment, and 3 months posttreatment). At the immediate and 3 months posttreatment time points, patients in the yoga intervention group (vs wait list control) had improved sleep quality (using the PSQI) and decreased fatigue (using the Medical Outcomes Study Short Form Health Survey [SF-36] Energy Scale) and inflammation. Although cognitive complaints did not differ significantly between the groups immediately posttreatment (P = .25), at 3 months posttreatment, the patients in the yoga intervention group (vs wait list control group) reported 23% fewer cognitive complaints (using the Breast Cancer Prevention Trial Cognitive Problems Scale; P = .003), which was present even when controlling for possible confounding factors (ie, psychological distress, fatigue, sleep quality, etc), and which was strongly associated with the frequency of home practice between sessions (more vs less practice, P < .001).
Discussion
Taken together, the bulk of the studies on cognitive and behavioral approaches supports the efficacy of CBT-I of varying formats (ie, video-based self-help, group, and individual face-to-face sessions) in the treatment of patients with breast cancer with sleep disturbance. From pre- to posttreatment (and up to at least 3-6 months), CBT-I has been shown to reduce DBAS, as well as to improve symptoms of depression, anxiety, fatigue, and overall QOL. Despite well-supported benefit and incorporation into the sleep disturbance treatment guidelines, there remain limitations that are both patient related (ie, adherence to a long-term treatment plan, high out-of-pocket costs) and provider related (ie, lack resources/infrastructure/trained clinicians in place to support such a program, reimbursement issues, etc). Stronger adherence to CBT-I (especially sleep restriction and stimulus control) among patients with breast cancer (with and without other comorbidities) diagnosed with sleep disturbance has been associated with fewer awakenings, higher sleep efficiency, reduced daytime impairment, as well as sustained improvement in sleep. Within the studies involving mindfulness and yoga interventions, there appeared to be more inconsistency, with some studies finding significant benefits in terms of sleep and fatigue, and others finding only trends toward improvements, or no difference between these interventions and controls. One of the major limitations of the mindfulness and yoga studies was a lack of sleep disturbance pretreatment screen, which allowed for a wide range in severity (ie, patients with minimal sleep disturbance at the beginning of the intervention had much less room for improvement, when compared with those with more severe insomnia). Another limitation of some of the studies was the overlap/lack of a clear distinction between yoga and mindfulness techniques. To directly compare the benefits of mindfulness practice alone vs yoga alone vs a combination approach, these techniques will need to be standardized and broken down into parts. Once an evidence-based approach is established (and only includes techniques/treatments that are found to be beneficial), then an infrastructure can be established with a clear picture of what would be needed as far as support staff and space requirements for such interventions. Many of the yoga interventions varied with respect to the school of yoga (ie, Hatha vs Iyengar), techniques, and duration. To get a better understanding of the beneficial effects of yoga on patients with breast cancer with sleep disturbance, the following factors should be considered: (1) the impact of adherence, (2) the minimum level of active participation (number of classes, frequency), and (3) whether independent practice can be performed to obtain benefits in the different domains (ie, QOL, sleep disturbance, fatigue). Randomized studies comparing CBT-I, mindfulness, and yoga interventions with clear baseline measures of sleep indices and co-existing symptoms common among patients with breast cancer (of similar age, stage, time point in their cancer treatment, menopausal status, etc) are necessary to identify psychological evidence-based approaches to improve sleep disturbance in patients with breast cancer. This will subsequently reduce the downstream negative impact of sleep disturbance on various domains of patients’ lives, including socioeconomic well-being, support and companionship of family and friends, and psychological and medical health.
It is also important to acknowledge real-life issues that patients and providers encounter when considering the feasibility of these behavioral approaches. Some potential challenges to engaging in behavioral treatment approaches, especially among patients with breast cancer diagnosed with sleep disturbance, include time constraints, escalating treatment costs, and decreased patient access to care. Patients are often not eager to engage in behavioral approaches as it takes more time to develop a skill and is not as convenient/easy as taking a pill to address the problem rapidly. This may be particularly significant in terms of competing priorities for patients with multiple appointments, family/childcare/work obligations, and for those with limited transportation. In terms of cost, there is limited research regarding the cost-effectiveness of these therapies as they are used for insomnia. Most of the research revolves around direct cost comparisons, and most of the cost-effectiveness research in the field has come out of the United Kingdom, which is home to NICE. 55 Recently, CBT and MBSR were appraised in the treatment of depression and have thus been covered by health insurance in the United Kingdom for other health conditions, such as insomnia. Meanwhile, only CBT-I is routinely covered by US health insurance after it was featured as an ACP practice guideline this past year.51,52
One study looked at the cost-effectiveness of CBT-I. At a maximum willingness to pay (WTP) per quality-adjusted life-year of £30 000, the probability of the intervention being cost-effective was found to be 80%. 97 If policymakers were willing to pay £150 per point improvement on the ISI, which is approximately the cost of the intervention, there would be a 97% probability of cost-effectiveness. Another study looked at the costs of MBSR vs medication in the treatment of depression and found that MBSR was consistently more expensive than medication (mean: US $457) over the first 12 months, but that the costs converged and MBSR became cheaper from months 12 to 15. Including all health and social services costs and productivity losses, the incremental cost-effectiveness ratio was US $962/relapse prevented and US $50/depression-free day, in favor of MBSR. Mindfulness-based stress reduction had a higher probability of being more cost-effective than medication for WTP threshold of approximately US $1000 and above. Although there was once concern regarding the cost of alternative therapies like yoga, recent cost estimates have shown that they are far below the average costs of standard health care treatment.98,99 As an example, a recent study found that, on average, the amount of money spent by a yoga practitioner on yoga-related expenses was US $1200 per year. 100 Therefore, even though very few US health insurers cover the service, it remains a bargain as a potential insomnia treatment option, with many potential benefits and only a few potential risks.
Research has shown that barriers to the implementation of CBT-I, MBSR, and yoga into a health care system can be classified into the following categories: (1) structural, (2) political, (3) cultural, (4) educational, (5) emotional, (6) physical/technological, and (7) economic. 101 Some of the methods in which it has been proposed that these be addressed include the following: (1) increased translational research that is tailored to clinical needs/questions of the community, (2) engaging local stakeholders, (3) identifying one or more expert(s) with adequate knowledge and access to key networks, (4) ensuring that key evidence and national guidance on the practice are clearly conveyed to staff members, (5) having strong leadership, (6) identifying appropriate and adequately trained staff to run education classes, (7) integrating a local and national implementation strategy for increasing access, and (8) analyzing local context to identify implementation barriers and facilitators. 102
Conclusions
Breast cancer is the most commonly diagnosed cancer in women and sleep disturbance is one of the most common complaints among women with this diagnosis. Interventions to improve sleep could improve QOL and productivity and could reduce comorbidities and decrease use of health care resources. Cognitive behavioral therapy for insomnia, mindfulness, and yoga are 3 behavioral health interventions that have been recommended in the treatment of sleep disturbance in patients with cancer. Depending on cancer disease severity, nonpharmacologic approaches may be more beneficial because efficacy appears to be similar to pharmacological approaches, patients can continue to implement behavioral strategies long after active treatment has ended, and there are fewer adverse effects.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to the research, writing, and editing of this paper.