
Abstract
Introduction
Little is known about the epidemiology of emergency medical search and rescue incidents globally. The purpose of this study was to describe the epidemiology of emergency medical search and rescue incidents in the North Shore Mountains of Vancouver, British Columbia, Canada.
Methods
This was a retrospective review and descriptive analysis of search and rescue incident reports created by North Shore Rescue over a 25 y period from 1995 to 2019, inclusive. Incident reports were screened for inclusion against a priori criteria defining a medical callout. The National Advisory Committee of Aeronautics (NACA) severity score was used as a method to grade medical acuity of included subjects.
Results
We included 906 subjects. Their median age was 35 y (interquartile range, 24–53), and 65% of subjects were men. Forty-one percent (n=371) of subjects were classified as non-trauma and 54% (n=489) as trauma. The top 3 activities were hiking (53%), biking (10%), and snow sports (10%). Forty-nine percent of incidents were classified as having a NACA score of ≥3. For subjects with trauma, the top 3 body regions were lower limb (52%), head (18%), and torso (12%). For subjects with non-traumatic conditions, the top 3 causes were mental health crises (25%), exposure (25%), and cardiovascular incidents (11%).
Conclusions
Half of the incidents were serious enough to require medical assessment at a hospital (NACA score ≥3). Given this medical acuity, there is a need for evidence-based guidelines and core training competencies for mountain medical search and rescue. Standardized core data sets and outcomes are needed to monitor quality of care over time.
Introduction
Emergency Medical Search And Rescue In Mountain Environments
The field of mountain emergency medicine has gained much interest and growth over the last 2 decades, and in response to the need for advocacy, organization, and research, several organizations have been founded, including the Medical Committee of the International Committee of Alpine Rescue (Switzerland), the Wilderness Medical Society (United States), and the Institute of Emergency Mountain Medicine (Italy). Despite this interest and these developments, there is still a relative paucity of descriptive epidemiology of emergency medical search and rescue incidents in contemporary mountain environments. This limits the development of medical care and care guidelines, quality improvement, and further research in the field.
Our review of the literature identified 8 studies describing trends in medical search and rescue callouts. 1 -8 Although some studies characterized health concerns as only traumatic or medical, others went further to identify the body region of injuries and the system of concern in medical callouts. A study that assessed emergency medical service (EMS) workload in Utah’s national parks from 2001 to 2005 encompassed 4762 EMS incidents, with 79 fatalities and 1148 callouts described as first-aid. 3 Although this view of mountain medicine callouts illustrates the range of severity that search and rescue (SAR) teams need to be prepared for, more detail on the type and frequency of medical concerns and traumatic injuries is essential to inform training to best provide tailored medical care. The most informative study in this regard described search and rescue callouts in New Zealand. This study identified sprains or strains as accounting for 53% of traumatic injuries, followed by fractures (29%), contusions or lacerations (10%), and head injuries (7%). 1 This was the only study that described incidents to this level of detail, and none systematically graded the medical acuity of incidents.
North Shore Rescue And The North Shore Mountains Of Vancouver, Canada
Operational since 1965, North Shore Rescue (
North Shore Rescue is activated by government agencies, such as local police, ambulance service, and fire service, to assist hikers, skiers, snowshoers, mountain bikers, and others who are reported to be lost or in distress. It also provides education on mountain safety and assists in urban search and rescue. As extreme sports and other wilderness activities have become seemingly more popular in the region, the need for rescues has risen dramatically, with the yearly call volume tripling in the last 25 y, according to our records. This makes North Shore Rescue one of the busiest mountain search and rescue organizations in the world, to our knowledge.
Rationale And Purpose
It is clear that there is a need for foundational epidemiology of mountain emergency medicine to inform and optimize the current provision of care in these environments and, subsequently, inform the development of standardized data collection systems and key indicators for monitoring, evaluation, and quality improvement of these services. The purpose of this study was to describe the epidemiology of emergency medical search and rescue incidents in the North Shore Mountains of Vancouver, British Columbia, Canada, from 1995 to 2019, inclusive.
Methods
Study Design
We conducted a retrospective review and descriptive analysis of incident reports created by North Shore Rescue over a 25-y period from 1995 to 2019, inclusive.
Data Source
For each callout, the rescue manager documented key features in an incident report. There is 1 incident report per callout, stored as paper records in the North Shore Rescue office. The incident reports were the source of all data collected. The incident report format changed significantly through the sampling time frame (ie, January 1, 1995 to December 31, 2019) from narrative notes to a standardized template designed by the BC Search and Rescue Information Centre. All incident reports were reviewed manually and screened for inclusion using all available information in the incident reports based on a priori inclusion criteria (Table 1).
Inclusion criteria
AMP, advanced medical provider.
Data Extraction And Management
Data were extracted and coded by members of the research team from paper records, manually, into a standardized electronic data entry template in Microsoft Excel.
The National Advisory Committee of Aeronautics (NACA) severity score was used as a method to grade medical acuity of included subjects. 9 This scoring system was originally developed in the United States in the 1950s as a simple and rapid way to characterize injury severity in wartime aviation crashes. It is a 7-point scale (1–7) that ranges from no injury or illness (NACA score=0) to lethal injuries (NACA score=7); a score of ≥3 is defined as requiring physician assessment (Table 2). It has since seen widespread international use in helicopter EMSs and rescue medicine, primarily in Europe. Performed in the prehospital setting, the NACA score has been shown to correlate well with morbidity and mortality. 10 Grading was performed at the time of data extraction using all available information in the incident reports by authors (DC, KB, DA, and MC) with significant emergency medicine experience, and these were verified by an experienced emergency physician with significant search and rescue experience (AR).
National Advisory Committee of Aeronautics scoring system
NACA, National Advisory Committee of Aeronautics.
Data were managed, cleaned, coded, and analyzed using a combination of Microsoft Excel and R. 11 Missing data were not imputed. If patients were found dead but the disposition was not documented, it was assumed that patients were dispositioned to the coroner, per standard practice in British Columbia.
This project was reviewed and approved by the Clinical Research Ethics Board at The University of British Columbia (No. H19-00177).
Results
Included Cases
Over the 25-y period from 1995 to 2019, inclusive, there were a total of 2078 callouts, of which 848 (41%) were classified as medical callouts. The percentage of calls that were medical in nature ranged from 14 to 60% over the 25-y span. The vast majority (89%) were for search and rescue, followed by known body recoveries (6%) and evidence searching (<1%). These 848 medical callouts collectively included a total of 906 subjects. Their median age was 35 y (interquartile range [IQR], 24–53), and 65% of subjects were men.
Of the 906 included subjects, 41% (n=371) were classified as non-traumatic conditions, 54% (n=489) were classified as trauma, and 3% (n=25) were classified as body recovery. Only 2% (n=21) of the subjects were unable to be classified (Table 3).
Summary of subjects by category
Incident Details And Conditions
The location of all medical callouts across all years is illustrated in Figure 1. Although the majority of callouts were located in the North Shore Mountains, they were not limited to these areas. The average callout duration was 12 h (SD, 1.3 h), and this ranged from 9±0.8 h for trauma calls to 18±7 h for body recoveries, with non-trauma calls taking 15±3 h on average.
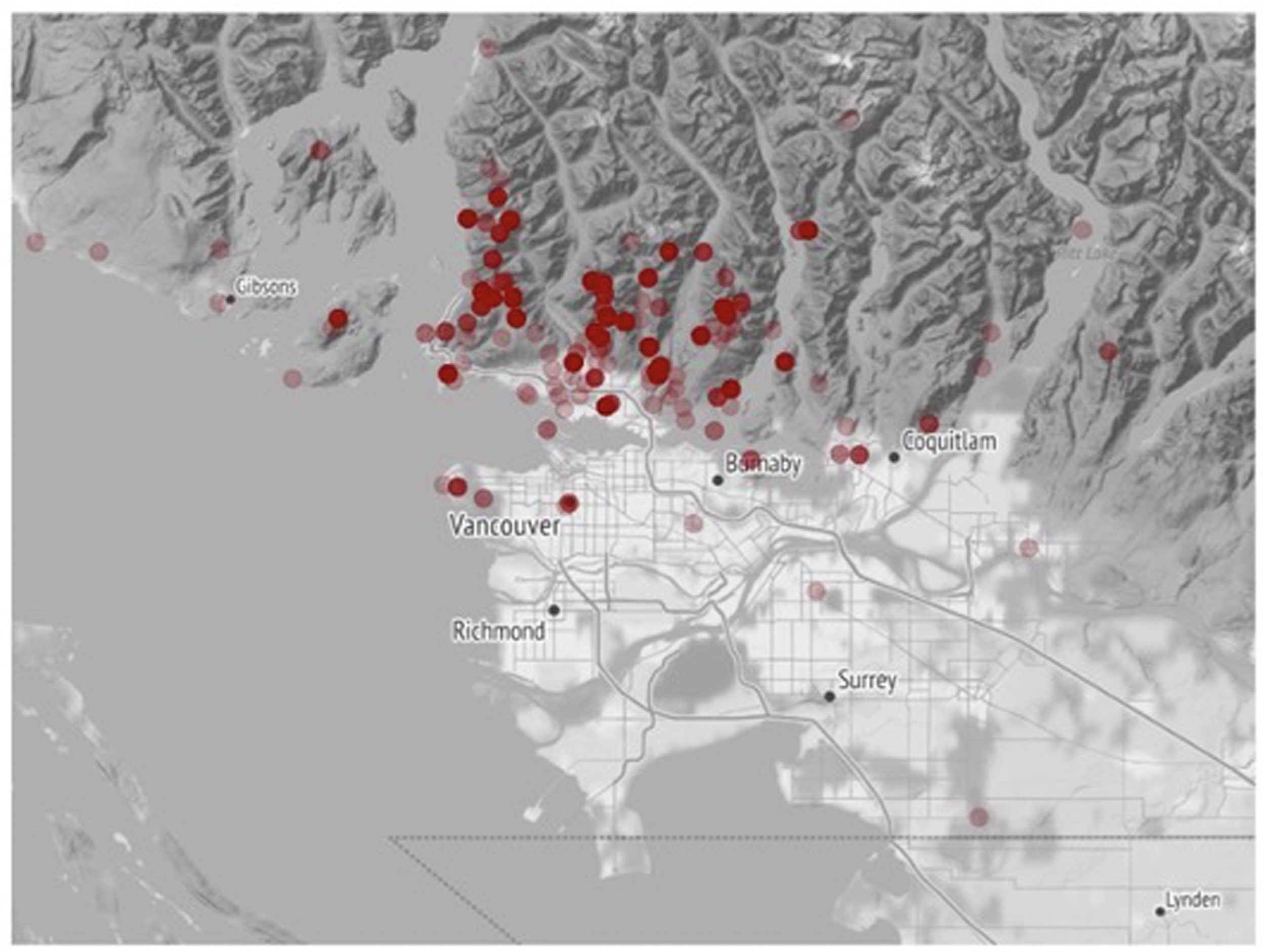
Map of medical callouts.
The top 3 activities (excluding “other”) leading to a medical callout were hiking (53%), biking (10%), and snow sports (10%) (Table 4). A significant number of injuries (3%) were also sustained by elderly subjects wandering in urban environments. Callouts predominantly occurred in mountain environments (82%), followed by urban (11%) and shoreline environments (7%).
Summary of activities that subjects were involved in at the time of the callout, as a percentage of total medical calls over 25 y and in 5-y epochs
Medical Subject Information And Outcomes
The median NACA score was 2 (IQR, 2–5) over the sampling period. We were unable to calculate NACA scores for 9% (n=82) of the included subjects. The absolute number of calls and percent of calls in each NACA category by 5-y epochs is shown in Figure 2. Just less than half (49%) of medical calls were classified as having a NACA score of ≥3. Death (ie, NACA score=7) was the outcome of 15% (n=72) of trauma calls and 18% (n=68) of non-trauma calls. The leading causes of non-traumatic death for those who were found dead were suicide (29%), cardiac arrest (27%), and drowning (22%).
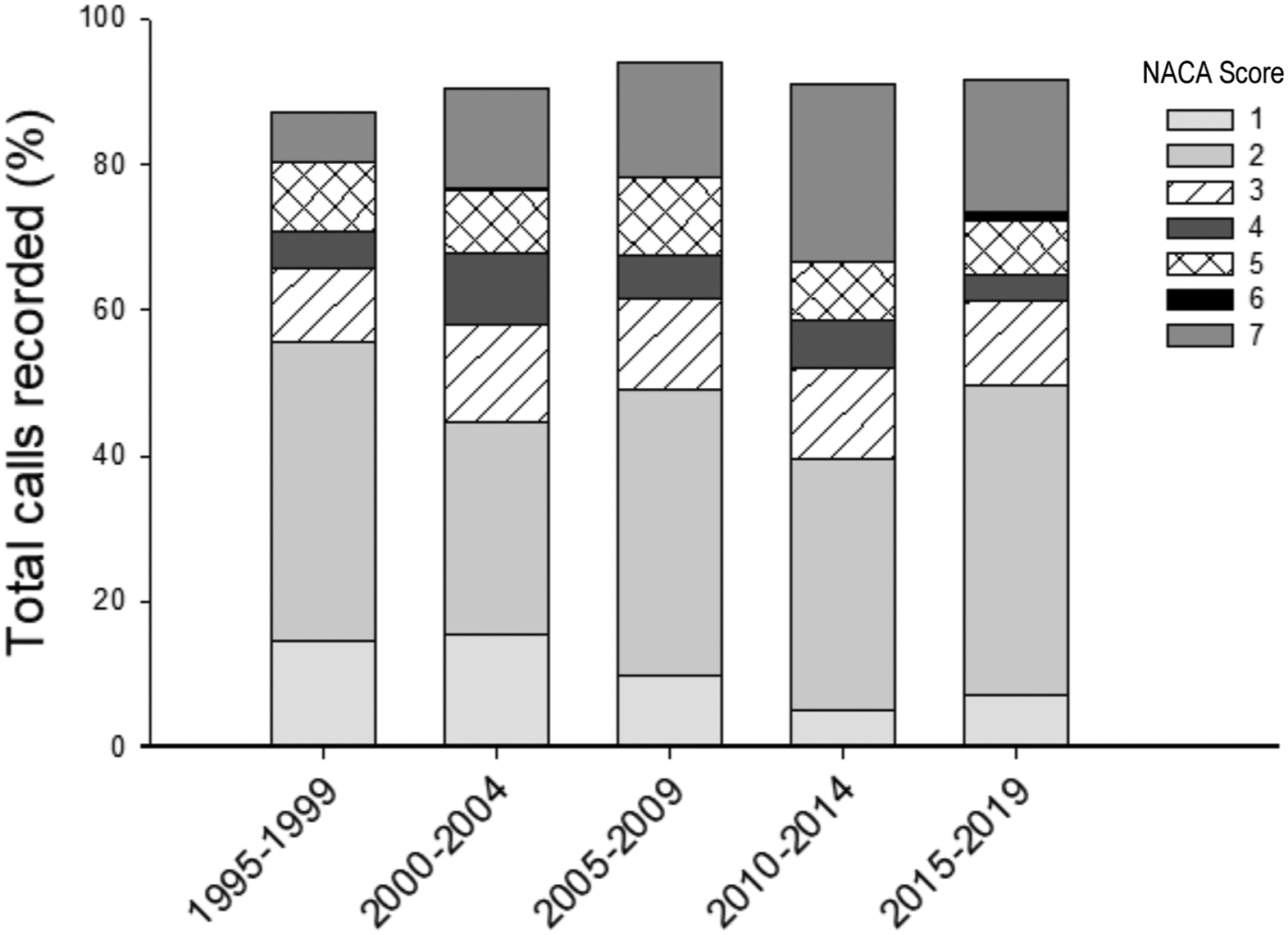
Summary of National Advisory Committee of Aeronautics scores as a percentage of total medical callouts by 5-y epochs. NACA, National Advisory Committee of Aeronautics.
Trauma Calls
Among the 489 included subjects who were classified as trauma and had sufficient details to be classified (n=366), the top 3 body regions affected were lower limb (n=191, 52%), head (n=65, 18%), and torso (n=43, 12%) (Figure 3). Polytrauma accounted for 7% of subjects included in this category (n=25). Death (or presumed dead) was the outcome of 15% (n=72) of all subjects with trauma.
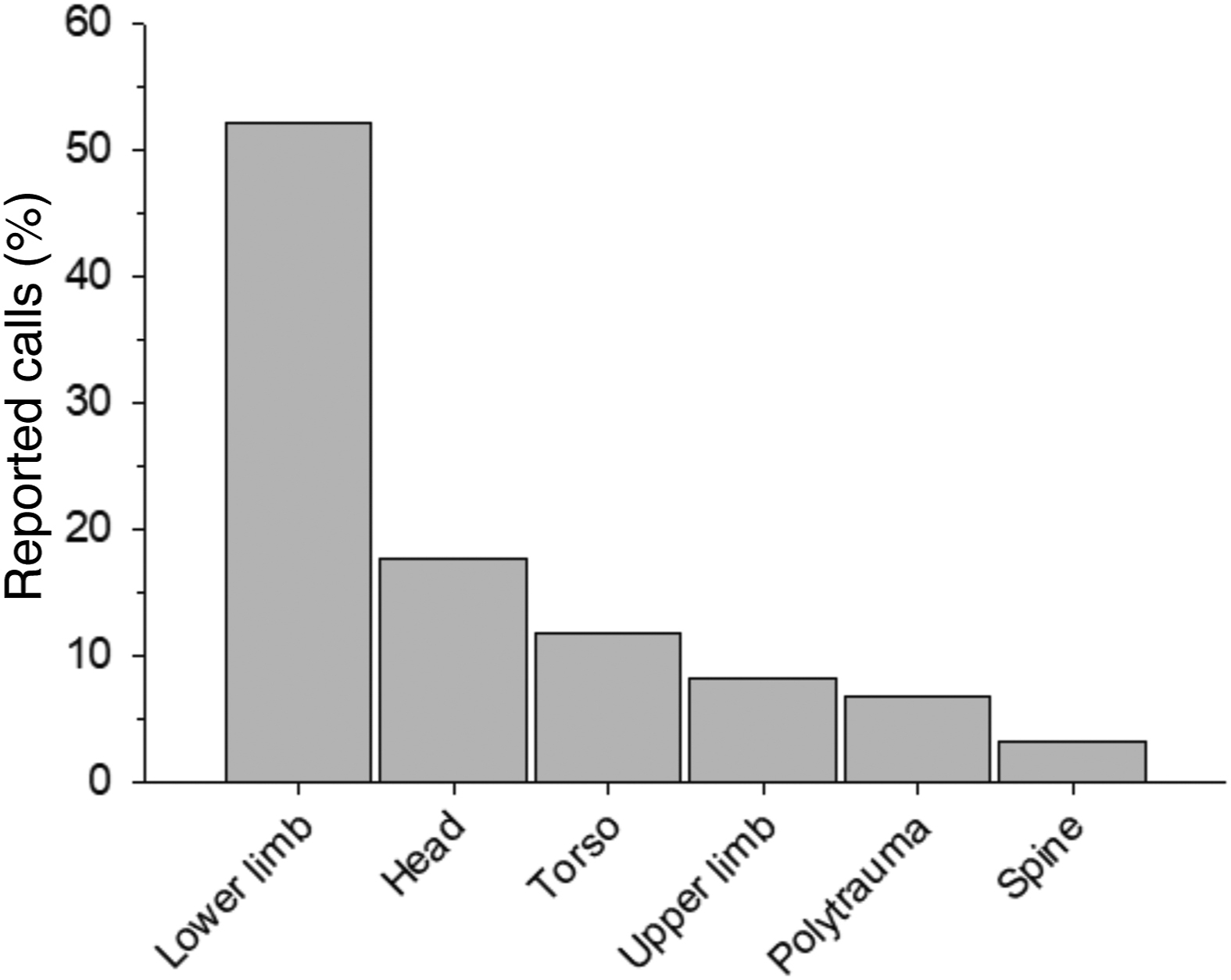
Summary of primary trauma body region, as a percentage of trauma calls.
Non-trauma Calls
Among the included subjects who were classified as non-traumatic conditions and who had sufficient details to be classified (n=371), the top 3 causes were mental health (25%), exposure (ie, hypothermia) (25%), and cardiovascular (11%). Of note, 8% of callouts in this category were for wandering (eg, people with dementia) (Figure 4). Death was the outcome for 18% (n=68) of all subjects with non-traumatic conditions.
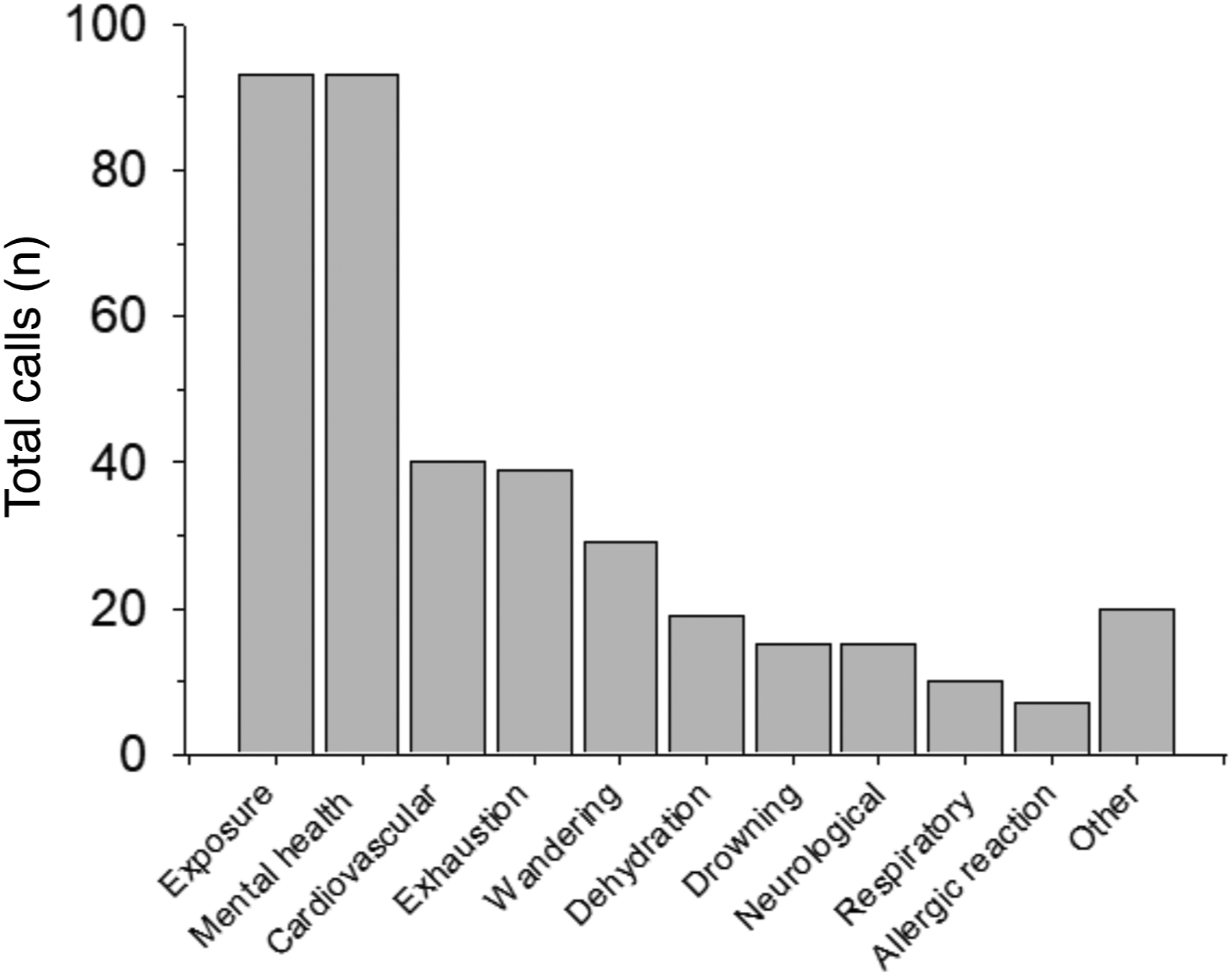
Summary of primary nontrauma medical indications, as a percentage of nontrauma calls.
Rescue Details
The transportation modes used to put rescue team members into the field (primary SAR mode), retrieve subjects from the field (primary subject transport mode), and disperse subjects once out of the field (secondary subject transport mode) are summarized in Table 5. The primary mode of search and rescue (ie, ingress) was predominantly by foot (42%) and helicopter (31%). In terms of egress, the primary subject transport mode was helicopter (35%), foot (17%), and stretcher (17%). After egressing out of the field, 41% of subjects required onward transport via ambulance. Most subjects (42%) were dispositioned to a hospital, but 12% each were dispositioned home and to the coroner service.
Summary of transportation used for primary search and rescue, primary subject transportation, and secondary transportation as a percentage of total callouts
SAR, search and rescue; NSR, North Shore Rescue
Discussion
Comparison With Existing Literature
To our knowledge, this is the first study to report the epidemiology of medical incidents in the North Shore Mountains of Vancouver, Canada. This study is unique in terms of the geography and population sampled, the long and contemporary 25-y time frame, and the use of NACA scoring to score the medical acuity of subjects.
Our results are consistent, however, with previous studies in other Canadian mountain jurisdictions, namely, in the demography of medical subjects, activity type, and traumatic injury location.5,6 A 2008 study reviewed 317 incidents recorded by Parks Canada Rescue in Banff, Yoho, and Kootenay National Parks over a 3-y period (2003–2006). Consistent with our findings, medical subjects were predominantly young (mean age, 35 y) and men (63%), and hiking was the leading activity type (44%). Lower-limb injuries accounted for 54% of traumatic injuries. 5 These findings are similar to those of another Canadian study that used data from the Alpine Club of Canada, with a comparatively larger sample size (n=1088) but older cohort (1970–2005), and was broadly similar to previous studies in North America2,3,4,7,8 and New Zealand. 1
With respect to medical subjects with non-traumatic conditions, our findings are unique, in that mental health crises were the leading cause (25%) of non-traumatic medical incidents. One previous Canadian study reported a 6% prevalence of “parasuicide,” 5 whereas another found that 11% of nontrauma medical calls were for “mental illness” and that in 68% of those found dead, the cause of death was suicide. 1 This discrepancy is likely explained by the North Shore Mountain’s proximity to a large urban area, whereas the subjects reported by the previous study were visitors to national parks. 5
Few previous studies have graded medical acuity, and none has used NACA scoring. Fatality rates (found dead) range from 61 to 31%. 6 Only 1 study attempted to grade acuity of medical subjects and classified 12% of subjects as having potentially life-threatening conditions and 3% as having imminently life-threatening conditions. 5 This roughly translates to NACA scores of 4, 5, or 6, of which 15% of our study population was graded.
Implications For Practice
In light of the relatively high degree of medical acuity, our findings illustrate the need for specialized medical care embedded within search and rescue operations in mountain environments. These findings have implications for both the provision of tailored prehospital medical care specific to this population and the logistics of medical search and rescue callouts.
With respect to tailored prehospital medical care, our results support the integration of advanced medical providers into traditional search and rescue organizations servicing mountain environments. This began in earnest at North Shore Rescue in 2018 after the organization qualitatively perceived an increase in both the number of medical subjects on callouts and increased complexity of medical needs. This called for the ability to bring in high-level medical care using advanced emergency or critical care practitioners (paramedics, registered nurses, and medical doctors), which is something unique in the volunteer search and rescue environment in Canada. This approach may be considered by other search and rescue organizations or at least consideration for investment in specialized medical training of search and rescue volunteers. Our findings will help inform the development of medical care protocols and supply procurement within North Shore Rescue. Notably, we identified the need for development and optimization of care for subjects facing mental health crises and drowning.
With respect to logistic considerations of medical search and rescue, the advent of digital technologies, such as mobile phone tracking and global positioning system and cartography software, has allowed easier and more rapid access to search and rescue subjects. Communication via mobile phones, satellite phones, or radio has also improved performance. Helicopter access and egress, including the use of fixed line or hoist capability, can also greatly enhance medical search and rescue performance and, by reducing overall call time, may impact health outcomes. Given the need for expeditious extraction of medical subjects, night vision capability of helicopters now allows for the use of helicopters for medical calls even at night. The use of all these technologies should continue and be expanded.
Implications For Research
Future research should focus on the development of core data sets and indicators for emergency medical search and rescue subjects. This would allow for higher-quality data to examine epidemiological trends over time and for monitoring and evaluation. It would also allow for direct comparison among various jurisdictions and standardize the evaluation of new search and rescue guidelines and methods. There is also a need for greater integration of data with hospital data and long-term patient outcomes. Prospective cohorts of medical subjects from these environments should be developed and studied in order to more fully understand the morbidity and mortality of mountain emergencies and, thus, tailor response efforts and public awareness campaigns.
This study was strengthened by the long time frame (25 y), sample size of medical subjects, and contemporary nature of the data (up to 2020). It is also the first known epidemiological study in the North Shore Mountains, one of Canada’s busiest mountain environments. Furthermore, given its proximity to a large urban environment (ie, Vancouver), it provides more generalizable information to other mountain jurisdictions that have relative ease of access and, therefore, more novice users (rather than remote, isolated mountain environments). We are also the first to grade medical acuity with more detail and to use the validated NACA score to elucidate the overall severity of injuries. We chose to include medical subjects who were ultimately found in urban environments (eg, patients with dementia who were lost wandering) because it helps to provide valuable information to search and rescue organizations covering mountain jurisdictions that abut urban centers about the nature and scope of all medical calls.
Limitations
We were unable to link our data with hospital data, and thus, our results do not reflect the final medical outcome of subjects and may, therefore, underestimate the overall mortality and potentially significant morbidity. In addition, given the narrative and sometimes incomplete information captured in incident reports, we had missing or incomplete information about the nature of some medical subjects and injuries. Although we worked extensively to obtain further information, we were unable to have complete data on all subjects, and this limited some of our analyses. Nonetheless, we reported data from complete cases when needed, and the sample size provided a reasonably representative sample.
Conclusions
This study represents one of the largest and most contemporary reviews of mountain emergency mountain medical search and rescue incidents to date and provides foundational epidemiology of mountain medical emergencies. Almost half of all incidents were serious enough to require medical assessment at a hospital (NACA score ≥3). Given this medical acuity, there is a need for evidence-based guidelines and core training competencies for mountain medical search and rescue. Standardized core data sets and outcomes are needed to monitor quality of care over time, compare mountain jurisdictions, and evaluate new or changing interventions. Continued public engagement and awareness campaigns are needed.
Footnotes
Acknowledgment
We acknowledge Clara Gale for her assistance with finding and summarizing relevant literature.
Author Contributions: Study concept and methods (AR, DC, MC); extraction and verification of data (AR, DC, MC, KB, AB); data cleaning and data analysis (BM, DC); contribution to the interpretation of findings, drafting, reviewing and final approval of the manuscript (DC, MC, KB, DA, AR, WM).
Financial/Material Support: Financial support for this study was provided by North Shore Rescue.
Disclosures: KB reports being a full-time volunteer member of North Shore Rescue since 2013, for which they do not receive any payment for this work; receiving an honorarium for a presentation at the St. Paul’s Emergency Medicine Update Conference in September 2021 regarding their volunteer work with North Shore Rescue; and being a member of the North Shore Rescue Executive from 2016 to 2020, during which time the proposal for this research project was approved. They did not receive any payment for their time on the Executive or for the time working on this submitted work.