
Abstract
Background:
Our previous research have identified Interleukin (IL)-7 and IL-15 as prognostic biomarkers for elderly septic patients, however, little is known about the link between the serum levels of IL-7, IL-15, and lactate as well as their potential roles in the regulation of inflammation in elderly septic patients.
Objectives:
This study aimed at investigating the link between the serum levels of IL-7, IL-15, and lactate as well as with other factors in elderly septic patients.
Design:
This is a retrospective study including 129 elderly patients with sepsis who were divided into the survival group (N = 34) and the nonsurvival group (N = 95) and further subgrouped based on the Acute Physiology and Chronic Health Evaluation II (APACHE II) scores.
Methods:
The baseline data and clinical parameters were recorded within 24 h upon admission. Serum levels of the cytokines were quantified by the Luminex assay. Spearman correlation analysis were performed.
Results:
Serum levels of IL-6, IL-7, IL-15, and tumor necrosis factor-α (TNF-α) were significantly higher in the nonsurvival group (P < .05). Correlations between serum levels of IL-7 and platelet-derived growth factor-AA (PDGF-AA), as well as correlations between IL-15, IL-6, and TNF-α were confirmed (P < .05). Both the serum levels of lactate and IL-15 correlated with the total counts of platelet (PLT) in the survival subgroup with low APACHE Ⅱ scores while the serum levels of IL-7, IL-15, and total counts of monocytes correlated with each other in the nonsurvival subgroup with different APACHE Ⅱ scores (P < .05).
Conclusion:
Knowledge of the regulation networks between serum levels of IL-7, IL-15, lactate, and other cytokines may provide insights into potential mechanisms in the modulation of inflammation in elderly septic patients and facilitate more prompt and accurate treatment to reduce the mortality rate.
Introduction
The Third International Consensus Definitions for Sepsis and Septic shock (Sepsis-3.0) has defined sepsis as life-threatening organ dysfunction resulted from a dysregulated host response to infection. 1 As a major public health concern, sepsis accounts for an estimated number of 50 million incident cases worldwide with a mounting rate of occurrence in elderly patients. 2 The mortality rate of sepsis rises with increased age, especially for those over 60 years. 3 Septic patients experience an initial death period characterized by a cytokine storm mediated by hyperinflammation and enter an immunosuppressive state which is prone to new secondary infections. 4 Animal model studies have indicated the apoptosis-induced loss of immune cells as a defining feature and vital pathophysiologic factor for the immunosuppression state and subsequent mortality of sepsis.5-7
Another significant characteristic of sepsis is the elevated levels of lactate as a result of increased catecholamine secretion, impaired pyruvate dehydrogenase activity, tissue hypoperfusion, and increased immune cell activation. 8 Several studies have found that increased serum level and impaired clearance of lactate are independently associated with elevated mortality in patients with sepsis.9,10 Although many studies have revealed the role of lactate in immune cell activation within one specific disease context, it is not entirely understood for the fact that the concurrent inflammatory effects and anti-inflammatory effects were both reported.8,11,12 Also, role of lactate in sepsis is not clear for its immunomodulatory aspects during the immunosuppressive phase of the disease, especially in human studies. Exact understanding of the immunoregulatory mechanisms as well as therapeutics aiming at the relative targets may facilitate treatment of sepsis and improvement of the high mortality.
The cytokine-based immunostimulating therapies, which aim at restoration of immune-homeostasis by stimulating the innate or adaptive immunity, have been studied for years.13,14 Recombinant human IL-7 (rhIL-7) administration has also been performed in patients with septic shock and induced an increase in the number of T lymphocyte and the proliferative capacity of both CD4 and CD8 T cells. 15 As potent antiapoptotic cyokines essential for the lymphocyte survival and expansion, IL-7 and IL-15 can similarly enhance function of multiple diverse immune effector cells and block cell apoptosis.16-18 In our previous studies, IL-7 and IL-15 have been identified as prognostic biomarkers for short-term mortality in elderly septic patients.19,20 Despite the above studies, little is known about the link between the serum levels of IL-7, IL-15, and lactate as well as their potential roles in the regulation of inflammation in elderly septic patients which are essential for the improvement of mortality in a context of precision medicine in sepsis. This study aimed to study on the expression patterns as well as correlations between serum levels of IL-7, IL-15, lactate, and other cytokines. Knowledge of the regulation networks may provide insights into the potential mechanisms in the modulation of inflammation in elderly septic patients and facilitate more prompt and accurate treatment to reduce the mortality rate.
Methods and Materials
Ethics
This study was in compliance with the Declaration of Helsinki and all methods were performed in accordance with the relevant guidelines and regulations. And the protocol was approved by the Ethics Committee of Beijing Chaoyang Hospital (approval number: 2021-ke-636). All patients have given their informed consent to participate in this study.
Study design and inclusion criteria
Among the patients admitted to the emergency department of Beijing Chaoyang Hospital in Beijing between November 2021 and May 2022, a total of 129 septic patients with the Sequential Organ Failure Assessment (SOFA) score ⩾2 points were included in this single-center retrospective study according to the Sepsis-3 criteria. 1 Based on the clinical outcome at the 28 day interval, the patients were classified into the survival group (N = 34) and nonsurvival group (N = 95). The survival group was then divided into the survival group with high Acute Physiology and Chronic Health Evaluation II (APACHE II) scores (⩾16, N = 18) and the survival group with low APACHE II scores (<16, N = 16). The nonsurvival group was divided into the nonsurvival group with high APACHE II scores (⩾23, N = 45) and the nonsurvival group with low APACHE II scores (<23, N = 50).
Exclusion criteria
Patients below the age of 60 and patients with missing data or abnormal data, and those with hematological diseases, malignant tumors, or connective tissue diseases, and those who were receiving immunosuppressive therapy were excluded.
Clinical parameters
The baseline data of the patients, such as sex, age, blood pressure, were collected upon admission. Values of APACHE II and SOFA were calculated and documented for all patients enrolled. The blood samples of the patients were also collected within 24 h upon admission to the emergency department for the analysis of the following laboratory results: platelet (PLT), albumin (ALB), lactate (LAC).
Measurement of the serum levels of IL-7, IL-15, and other cytokines
Blood samples of the patients were drawn by venous puncture and added into the serum separator tubes on admission. The tubes were put at room temperature for 30 minutes to clot. The serum was then centrifuged at 1000g for 15 minutes and aliquots were stored at −80°C until analysis.
Serum levels of PDGF-AA, TNF-α, IL-6, IL-7, IL-15 were quantified by using Human XL Cytokine Luminex Performance Assay 46-plex Fixed Panel (Cat. No. LKTM014B, R&D Systems, Minneapolis, USA) according to the manufacturer’s instructions.
Statistical analysis
The SPSS software was used to perform the statistical analyses. The Kolmogorov-Smirnov goodness of fit test was performed to ensure the parametric distribution of the data. The results were demonstrated as medians and interquatile ranges. Removal of the outliers was made for those individual values over the third quartile + 1.5* interquartile range. The unpaired Student’s t test or the Mann-Whitney U test was performed for analysis of the data, respectively. Categorical data were analyzed by the χ2 test. For the correlation analysis, Spearman correlation analysis was performed. P < .05 was considered statistically significant.
Results
Baseline characteristics
As shown in Table 1, this study enrolled 73 male and 56 female patients, with 95 patients died after the follow-up period. A flow chart of the patients was shown in Figure 1. The survival group (N = 34) consisted of 21 male and 13 female patients while the nonsurvival group (N = 95) consisted of 52 male and 43 female patients. The median ages of the survival group and the nonsurvival group was 74.0 (69.0, 84.0) and 79.0 (70.0, 84.0). And no significant differences in either sex or age were shown between the 2 groups (P > .05).
Baseline data of the patients.

Abbreviations: ALB, albumin; APACHE Ⅱ, the acute physiology and chronic health evaluation Ⅱ score; PLT, thrombocyte count; SBP, systolic pressure; SOFA, the sequential organ failure assessment score; TNF-α, tumor necrosis factor-α.
N, number of patients; results were demonstrated as medians and interquartile ranges.

Flow chart of the patients in the study.
Comparison of the clinical parameters
The SOFA and APACHE II scores in the nonsurvival group were significantly higher than those of the survival group (median value: 8.0 vs 4.4, 22.0 vs 16.0, both P < .05). The systolic pressure (SBP) in the nonsurvival group were significantly lower than those of the survival group (median value: 131.0 mmHg vs 145.0 mmHg, P < .05). The serum levels of PLT and those of ALB were not significantly different but trended lower in the nonsurvival group (median value: 173.0 × 109/l vs 201.0 × 109/l, 32.6 g/l vs 36.3 g/l, both P > .05). There were no significant differences in the total counts of lymphocytes, monocytes, neutrophils and the serum levels of lactate between the 2 groups (P > .05).
Expression patterns of the cytokines
There was an increased trend in the serum levels of PDGF-AA in the nonsurvival group (median value: 4546.7 pg/ml vs 3295.0 pg/ml, P > .05). And the levels of TNF-α and IL-6 in the nonsurvival group were significantly higher than those in the survival group (median value: 8.1 vs 4.3, 125.9 pg/ml vs 10.2 pg/ml, both P < .001). IL-7 and IL-15 were both significantly higher in the nonsurvival group (median value = 6.7 and 1.6 pg/ml) compared with the survival group (median value = 3.7 and 0.9 pg/ml) (P < .01) (Table 1).
Correlation analyses between the risk factors, cytokines, and immune cells between the survival and nonsurvival group of patients
There were correlations between IL-15 and IL-6 (r = .582, P < .001) and correlations between IL-15 and TNF-α (0.428, P < .001) in the nonsurvival group (Table 2). The correlations between IL-7 and PDGF-AA were demonstrated both in the survival group (r = .534, P < .001) and in the nonsurvival group (r = .710, P < .001). There was correlation between IL-7 and IL-15 in the nonsurvival group (r = .210, P = .041) while no correlation was shown in the survival group (r = .034, P = .851) (Table 2). No correlations were shown between serum levels of lactate and other factors in both groups (Table 3).
Correlation analysis of IL-7, IL-15 and other biomarkers for patients in the survival and nonsurvival group.

Abbreviations: ALB, albumin; APACHE Ⅱ, the acute physiology and chronic health evaluation Ⅱ score; SOFA, the sequential organ failure assessment score; IL, interleukin; PDGF-AA, platelet-derived growth factor-AA; PLT, thrombocyte count; TNF-α, tumor necrosis factor-α.
P < .05 was considered statistically significant.
Correlation analysis of lactate and other biomarkers for patients in the survival and nonsurvival group.

Abbreviations: ALB, albumin; APACHE Ⅱ, the acute physiology and chronic health evaluation Ⅱ score; SOFA, the sequential organ failure assessment score; IL, interleukin; PDGF-AA, platelet-derived growth factor-AA; PLT, thrombocyte count; TNF-α, tumor necrosis factor-α.
P < .05 was considered statistically significant.
Comparison of lactate, IL-7, IL-15, and other factors in the survival and nonsurvival subgroups based on the APACHE II scores
The median serum levels of lactate were slightly higher in the survival group with APACHE II ⩾ 16 (N = 22) than those with APACHE II < 16 (N = 22) (median value: 1.40 vs 1.10, P = .341) and the same in the nonsurvival group with APACHE II ⩾ 23 (N = 45) than those with APACHE II < 23 (N = 50) (median value: 1.20 vs 1.20, P = .920) (Table 4). The median serum levels of IL-7, IL-15, and TNF-α were all higher in the nonsurvival groups either with APACHE II ⩾ 23 (N = 45) (median value: 6.7, 1.9, and 8.6 pg/ml) or with APACHE II < 23 (N = 50) (median value: 6.9, 1.4, and 8.1 pg/ml) compared with their survival counterparts (P > .05) (Table 4).
Comparison of the serum levels of lactate, IL-7, IL-15, and other factors for patients in the survival and nonsurvival group with different APACHE II scores.

Abbreviations: APACHE Ⅱ, the acute physiology and chronic health evaluation Ⅱ score; IL, interleukin; SOFA, the sequential organ failure assessment score; TNF-α, tumor necrosis factor-α.
N, number of patients; results were demonstrated as medians and interquartile ranges.
Correlation analyses between lactate, IL-7, IL-15, and other factors in the survival and nonsurvival subgroups based on the APACHE II scores
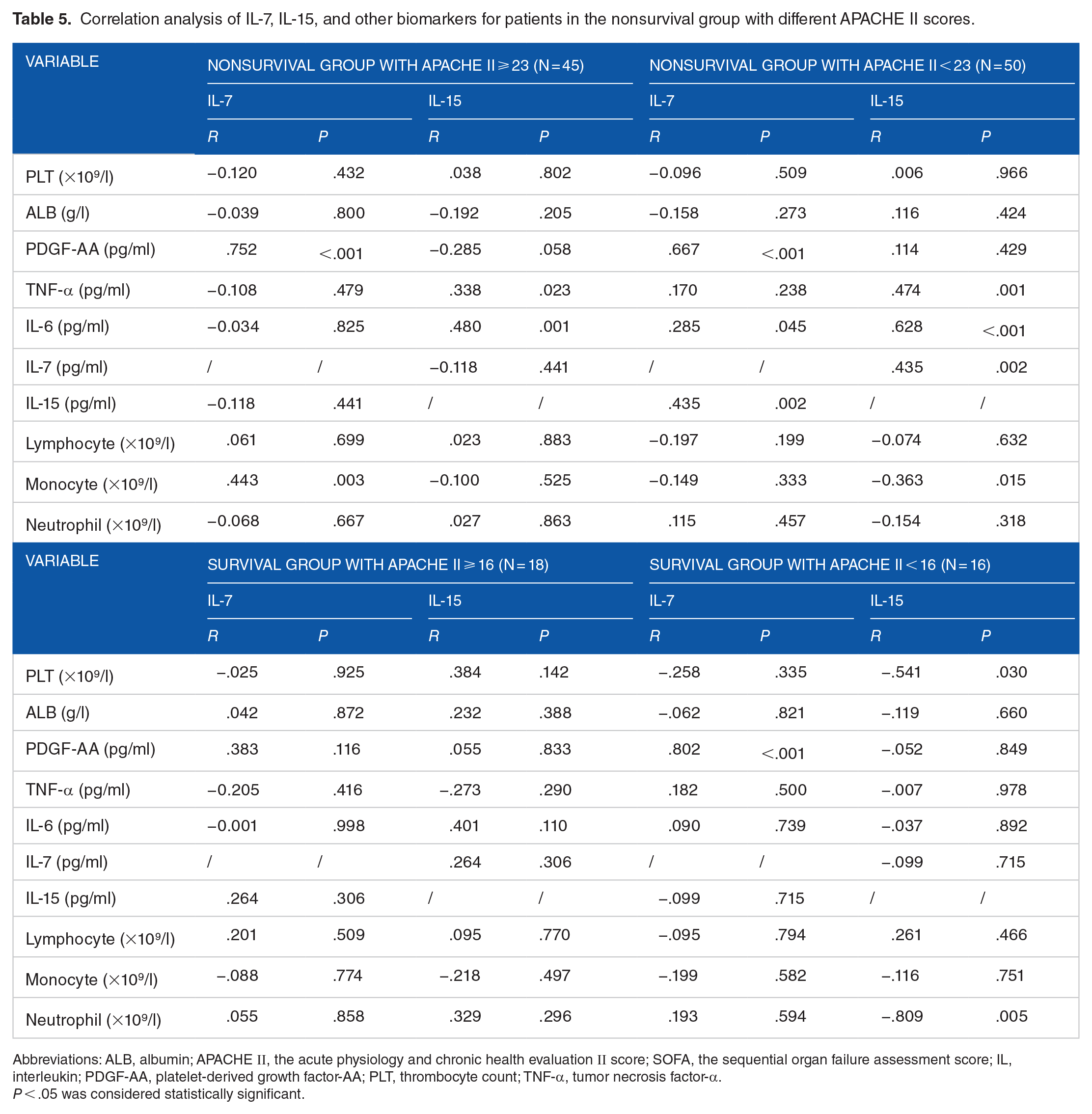
Correlations between IL-7 and PDGF-AA were demonstrated in the survival group with APACHE II < 16 (N = 16) (r = .802, P < .001), in the nonsurvival group with APACHE II ⩾ 23 (N = 45) (r = .752, P < .001) and in the nonsurvival group with APACHE II < 23 (N = 50) (r = .667, P < .001) (Table 5). Correlations between IL-15 and IL-6 were found in the nonsurvival subgroups divided by the APACHE II scores (all P < .01) (Table 5). Correlations between IL-15 and TNF-α were both shown in the nonsurvival groups either with APACHE II ⩾ 23 (N = 45) and with APACHE II < 23 (N = 50) (both P < .05) (Table 5). Serum levels of IL-7 were correlated with those of IL-15 in the nonsurvival group with APACHE II < 23 (N = 50) (P < .05) (Table 5). Total counts of monocytes were correlated with serum levels of IL-7 in the nonsurvival group with APACHE II ⩾ 23 (N = 45) and correlated with those of IL-15 in the nonsurvival group with APACHE II < 23 (N = 50) (P < .05) (Table 5). Serum levels of lactate were correlated with APACHE II scores in the nonsurvival group with APACHE II < 23 (N = 50) (P < .05) (Table 6). The number of PLT was correlated with serum levels of IL-15 (r = −.541, P =.030) and correlated with serum levels of lactate (r = −.553, P = .026) in the nonsurvival group with APACHE II < 16 (N = 16) (Table 6). The possible links between the cytokines and lactate were demonstrated as shown in Figure 2.
Correlation analysis of IL-7, IL-15, and other biomarkers for patients in the nonsurvival group with different APACHE II scores.
Abbreviations: ALB, albumin; APACHE Ⅱ, the acute physiology and chronic health evaluation Ⅱ score; SOFA, the sequential organ failure assessment score; IL, interleukin; PDGF-AA, platelet-derived growth factor-AA; PLT, thrombocyte count; TNF-α, tumor necrosis factor-α.
P < .05 was considered statistically significant.
Correlation analysis of lactate and other biomarkers for patients in the survival and nonsurvival group with different APACHE II scores.

Abbreviations: ALB, albumin; APACHE Ⅱ, the acute physiology and chronic health evaluation Ⅱ score; SOFA, the sequential organ failure assessment score; IL, interleukin; PDGF-AA, platelet-derived growth factor-AA; PLT, thrombocyte count; TNF-α: tumor necrosis factor-α.
P < .05 was considered statistically significant.
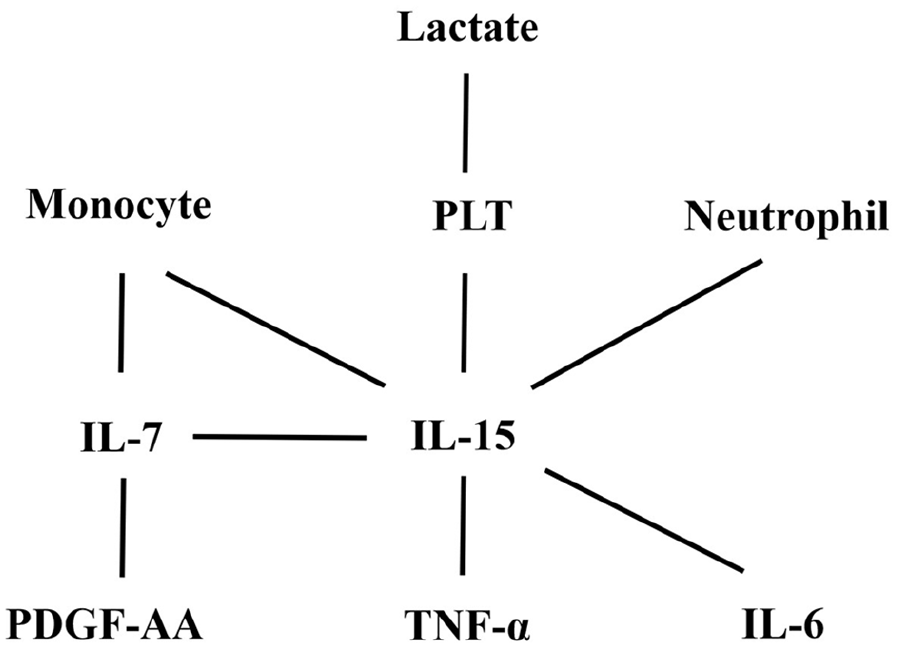
The correlation network between the cytokines and lactate in the patients of this study.
Discussion
Sepsis, which occurs more frequently in elderly patients with higher mortality, has been regarded as a major cause of death as well as a life-threatening health crisis in the geriatric population. 2 Approximately 58% to 65% septic patients were reported to be elderly patients with a mortality rate of 26% for patients between the age of 60 to 64 and the mortality rate of 38% for patients over 85 years.21,22 Thus, it is necessary to give early diagnosis as well as accurate prediction of the clinical outcomes for elderly patients with sepsis.
Septic patients first enter a hyperinflammation phase characterized by a cytokine storm and a prolonged immunosuppression state accompanied by a persistent T cell exhaustion phenotype characterized by reduced number of T cells, impaired T lymphocyte function, and increased proportion of regulatory T cells (Tregs) and increased expression of co-inhibitory molecule.23,24 In the clinical set, the persistent T cell exhaustion is mainly responsible for the high mortality in elderly septic patients. As potent antiapoptotic cyokines essential for the lymphocyte survival and expansion, IL-7 and IL-15 can similarly enhance function of multiple diverse immune effector cells and block cell apoptosis.25-29 Our previous research have demonstrated that IL-7 and IL-15 can be both used as prognostic biomarkers for short-term mortality in elderly septic patients.19,20 Despite the above findings, little is known about the link between the serum levels of IL-7, IL-15, and other cytokines as well as their potential roles in the regulation of inflammation in elderly septic patients.
In this study, we examined the routine indices, such as platelets and albumin, which have been shown to be indicators of the outcome for septic patients. Changes in platelet function and impairment of blood rheology might play a role in the pathogenesis of multiple organ dysfunction syndrome (MODS) by reducing microvascular blood flow followed by hypoperfusion. 30 Albumin plays vital regulatory roles in acid‒base physiology and fluid distribution and lower plasma albumin levels were found in septic patients than in nonseptic patients.31,32 We also analyzed the SBP variation which has been used as a guide to fluid therapy in patients with sepsis-induced hypotension. 33 Our data showed that PLT, ALB, and SBP in the nonsurvival group were lower than those of the survival group of elderly septic patients. Next, we investigated the expression patterns as well as the correlations between serum levels of IL-7, IL-15, lactate, and other cytokines. Our results showed that the nonsurvival group possessed significantly higher serum levels of IL-7, IL-15, TNF-α, and IL-6 when compared with the survival group. Comparisons between the subgroups based on the APACHE II scores did not show significant differences or similar trends in the mean value changes of serum IL-7, IL-15, TNF-α. Actions of IL-15 on memory cell persistence and inhibition on the immunological checkpoint or activation-induced cell death enable the maintenance of long-lasting immune responses to vaccines. 34 Also, IL-15 has been shown to induce the inflammatory factors TNF-α and IL-1β. 35 Our data confirmed the correlations between IL-15 and IL-6 as well as the correlations between IL-15 and TNF-α in different subgroups indicating the pro-inflammatory roles of IL-15 in elderly septic patients. We also found that IL-7 correlated with PDGF-AA, a factor participating in enhanced angiogenesis, vascularization, differentiation and tissue remodeling. 36 This reflects a potential protective role of IL-7 in the feedback regulation of the excessive inflammation during sepsis through the action of PDGF-AA. Our results also confirmed the positive correlation between IL-7 and IL-15 in the nonsurvival group. As IL-7 and IL-15 share the common cytokine receptor γ-chain as part of the receptor and can be secreted by some common cell types, such as the epithelial cells, we conclude a common stimulating pathway exists for this simultaneous upregulation of IL-7 and IL-15 in elderly patients with sepsis. A previous study has shown that IL-7 and IL-15 can differentially regulate CD8 T cell subsets defined by KLRG1 and CD127 expression during the specific phase of the immune response. 37 Our study showed the differences in which IL-7 was correlated with PDGF-AA while IL-15 was correlated with IL-6 and TNF-α, which may provide insights about different roles of IL-7 and IL-15 in the regulation of inflammation in elderly septic patients.
Another significant characteristic of sepsis is increased levels of lactate. The serum lactate levels ranged from 2 to 10 mM during sepsis which can even reached 20 mM in different circumstances.38-41 Several studies have shown that elevated serum lactate (⩾4 mM) and impaired clearance are independently associated with increased mortality in septic patients.9,10 Our data showed that patients with higher APACHE II scores possessed relatively higher serum levels of lactate which correlated with the APACHE II scores in the nonsurvival subgroup with low APACHE II scores. As APACHE II scores reflect disease severity in septic patients, these results suggested that serum levels of lactate can indicate disease severity to some extent in the nonsurvival subgroup. Several animal models have investigated the relationship between lactate and sepsis. Lactate has been shown to suppress LPS-induced cell metabolism, immune cell function, and cytokine production in mice.42,43 Similarly, sodium lactate suppressed cytokine production in a rat model of sepsis. 44 Intratracheal acidic aspiration has also been shown to impair clearance of S. pneumoniae and E. coli. 45 Despite the above findings, the effects of lactate in different stages of sepsis are not fully understood. And the roles of lactate in sepsis is not clear especially for its immunomodulatory aspects during the immunosuppressive phase of the disease, for the fact that the inflammatory effects and anti-inflammatory effects of lactate were both reported. 8 A recent study by Leśnik et al 46 investigated IL-7 and IL-15 as prognostic biomarkers in patients with sepsis and septic shock, and the correlation between the serum levels of lactate and IL-15 was also demonstrated. Although we did not find a direct correlation between serum levels of lactate and IL-15, the correlations between lactate and PLT as well as correlations between IL-15 and PLT were demonstrated in the survival group with APACHE II < 16 but not in other subgroups in our study. Also, our data showed that total counts of monocytes correlated with the serum levels of IL-7 in the nonsurvival group with APACHE II ⩾ 23 and correlated with the serum levels of IL-15 in nonsurvival group with APACHE II < 23. Extracellular lactate has been shown to induce metabolic reprograming in innate immune cells, as evidenced by reduced glycolytic and increased oxidative rates of monocytes immediately after exposure to lactate. 47 Thus, it is probable that lactate can exert different immunomodulatory roles through PLT or monocyte which may involve the actions of IL-15 or IL-7 under different conditions and may together contribute to the varying outcomes for individual septic patient. Our results in this study depict a network of cytokines in which IL-7, IL-15 and lactate are at the center and may provide insights into their potential roles in the regulation of inflammation as well as in a novel immunomodulatory pathway of lactate in elderly patients with sepsis. This is meaningful for the possible intervention of the inflammation response in sepsis and improvement of mortality in a context of precision medicine.
Limitations
This study has limitations, such as the small sample size, lack of healthy and elderly controls and the fact that it was a single-center study. Also, sample size calculation was not conducted for the lack of an expected estimate of Spearman correlation coefficient either from previous similar research or expert opinion. Further multi-center studies with larger sample sizes as well as determination of the baseline levels in healthy controls are still needed. And the dynamic monitoring in septic patients should also be investigated. Future research should verify these immunoregulatory mechanisms in in vitro human immune cells or in vivo animal models.
Conclusion
Knowledge of the regulation networks between serum levels of IL-7, IL-15, lactate, other cytokines may provide insights into the potential mechanisms in the modulation of inflammation in elderly septic patients and facilitate more prompt and accurate treatment to reduce the mortality rate.
Footnotes
Acknowledgements
Not applicable.