
Abstract
Background:
Inflammation plays a critical role in sepsis. The integration of neutrophil-to-lymphocyte ratio (NLR) and platelets-to-lymphocytes ratio (PLR) from multiple cell types offers a novel approach to rapidly assess inflammation status. However, the predictive role of NLR and PLR in sepsis with lymphopenia remains uncertain.
Objectives:
The purpose of this study was to explore the prognostic value of NLR and PLR in sepsis patients with lymphopenia.
Design and methods:
In this observational retrospective study, we included 172 sepsis patients with lymphopenia and collected clinical characteristics for analysis. Through binary logistic regression analysis, we identified independent factors. Receiver-operating characteristic curves (ROC) and areas under the curves (AUC) were employed to assess the ability to predict hospital mortality risk.
Results:
Our results showed a total hospital mortality rate of 53.49%. Multivariate analysis demonstrated that NLR (OR = 1.11, P < .001) and PLR (OR = 1.01, P = .003) were independent predictors associated with hospital mortality in sepsis patients with lymphopenia. The AUCs of NLR and PLR were 0.750 (95% CI: 0.634-0.788, P < .001) and 0.662 (95% CI: 0.580-0.743, P < .001), respectively. Notably, an optimal cut-off value of 18.93 for NLR displayed a sensitivity of 75.0% and specificity of 63.0% in discriminating hospital mortality in sepsis patients with lymphopenia, while the optimal cut-off value for PLR was 377.50, with a sensitivity of 67.5% and specificity of 64.1%.
Conclusion:
NLR and PLR serve as independent predictors of hospital mortality in sepsis patients with lymphopenia.
Introduction
Sepsis is a global health concern characterized by life-threatening organ dysfunction resulting from a dysregulated host response to infection.1,2 Current data indicate that sepsis occurs at rates of 288 to 535 cases per 100 000 person-years,3,4 with mortality rates as high as 25% to 30% despite advancements in diagnosis and therapy. 5 In sepsis, the host immune system becomes complex and compromised, leading to organ dysfunction and even death.6,7 Immunological suppression plays a pivotal role in sepsis development; however, there is presently no reliable and convenient test available for detecting immunosuppression in sepsis patients.
The neutrophil-to-lymphocyte ratio (NLR) has emerged as a promising biomarker in biomedical research. It is calculated by dividing the number of neutrophils by the number of lymphocytes in peripheral blood. The NLR reflects the combined influence of both the innate immune response, primarily mediated by neutrophils, and the adaptive immunity supported by lymphocytes. 8 Elevated NLR has been observed in various conditions, including bacterial or fungal infections, acute stroke, myocardial infarction, atherosclerosis, severe trauma, cancer, post-surgery complications, and any condition characterized by tissue damage. This easily obtainable marker from routine laboratory tests provides valuable information about the systemic inflammatory status. Furthermore, numerous studies have demonstrated the predictive value of NLR in mortality across diverse populations, including the general population, 8 inflammatory bowel disease, 9 pneumonia, 10 and COVID-19 pneumonia. 11 These association findings likely reflect the detrimental effects of severe inflammation and impaired immune function on the progression of these diseases. Moreover, several studies have highlighted the prognostic utility of the platelet-to-lymphocyte ratio (PLR) in assessing systemic inflammatory responses, indicating its ability to reflect the intricate interplay between inflammation, coagulation, and the immune response.12 -14
Numerous studies have aimed to investigate the impact of NLR and PLR on mortality in patients with sepsis. Liu et al conducted a study that demonstrated an association between NLR and 28-day mortality in sepsis patients. 15 Lymphopenia always induces the NLR and PLR elevation, while lymphopenia in sepsis patients is considered to be immunosuppression, which affects the prognosis of sepsis patients. However, the complete understanding of the prognostic value of NLR and PLR in sepsis patients with lymphopenia is still lacking. Therefore, the objective of this study is to assess the predictive accuracy of NLR and PLR in determining mortality outcomes specifically in sepsis patients with lymphopenia.
Material and Methods
Study design
We conducted a retrospective cohort study with hospitalized patients in ICU department, First Affiliated Hospital of Shandong First Medical & Shandong Provincial Qianfoshan Hospital, Jinan, China. Medical records between April 2019 and December 2021 were reviewed.
Inclusion and exclusion criteria
Patients were eligible for enrollment if they met the following criteria: (1) age of at least 18 years and a diagnosis of sepsis. Sepsis was defined based on the sepsis-3 criteria, which considers a dysregulated host response resulting from infection and leading to life-threatening organ dysfunction. 2 (2) lymphocyte count below 1.0 × 109/L. We pre-defined criteria to exclude patients based on the following factors: (1) missing neutrophil and lymphocyte data upon admission to the ICU; (2) lymphocyte count exceeding 1.0 × 109/L; (3) patients diagnosed with HIV; (4) patients who had already been in the ICU for an extended period.
Data extraction
Data were collected on the patient’s age, gender, underlying disease, vasoactive agent use, mechanical ventilation use, and laboratory results. Record the patient’s peripheral blood neutrophil, lymphocyte, and platelet counts for ICU admission day. NLR was defined as absolute neutrophil count divided by absolute lymphocyte count. PLR was defined as absolute platelet count divided by absolute lymphocyte count. SII =platelet count × neutrophil count/lymphocyte count. Hospital mortality was identified through the electronic medical record.
Statistical analysis
No statistical sample size calculation was performed, and sample size was equal to the number of patients admitted to hospital during the study period. Statistical analysis was performed using IBM SPSS Statistics version 26.0 (IBM SPSS Statistics for Macintosh, Armonk, New York). The Kolmogorov–Smirnov test was used to assess normal distribution. Continuous data with normal distributions were presented with mean ± standard deviation (SD) or medians and quartiles, and the difference between groups was analyzed using t-test or Mann–Whitney U test. Categories data were presented with frequencies and percentages and compared using Chi-square test. Logistic regression analysis was used to identify potential predictors associated with mortality in patients. The predictive prognostic values were evaluated by the receiver operating characteristic (ROC) curve method and area under the curve (AUC). The optimal cutoff value affecting prognosis was determined by the receiver operator characteristic (ROC) curve. All statistical tests were 2-sided and a P < .05 was considered statistically significant.
Results
Baseline Characteristics of the study patients
A total of 172 sepsis with lymphopenia patients were included in this study, 80 cases in the survivors group and 92 in the non-survivors group, with a total hospital mortality rate of 53.49%. The baseline characteristic comparison between the survivors group and the non-survivors group is shown in Table 1. The average age of the included patients was 57.57 years, with 130 cases in males and 42 in females, and 75.58% of males. 41 (23.84%) solid tumor, 23 (13.37%) patients suffered hematological malignancies, and 17 (9.88%) had organ transplantation. Regarding the type of immunosuppressive treatment, 60 (34.88%) had received immunosuppressive agents and 82 (47.67%) had received corticosteroid treatment. There were statistical differences in vasoactive agent use and mechanical ventilation use between the survivors group and the non-survivors group (P = .001).
Baseline characteristics of the study patients.
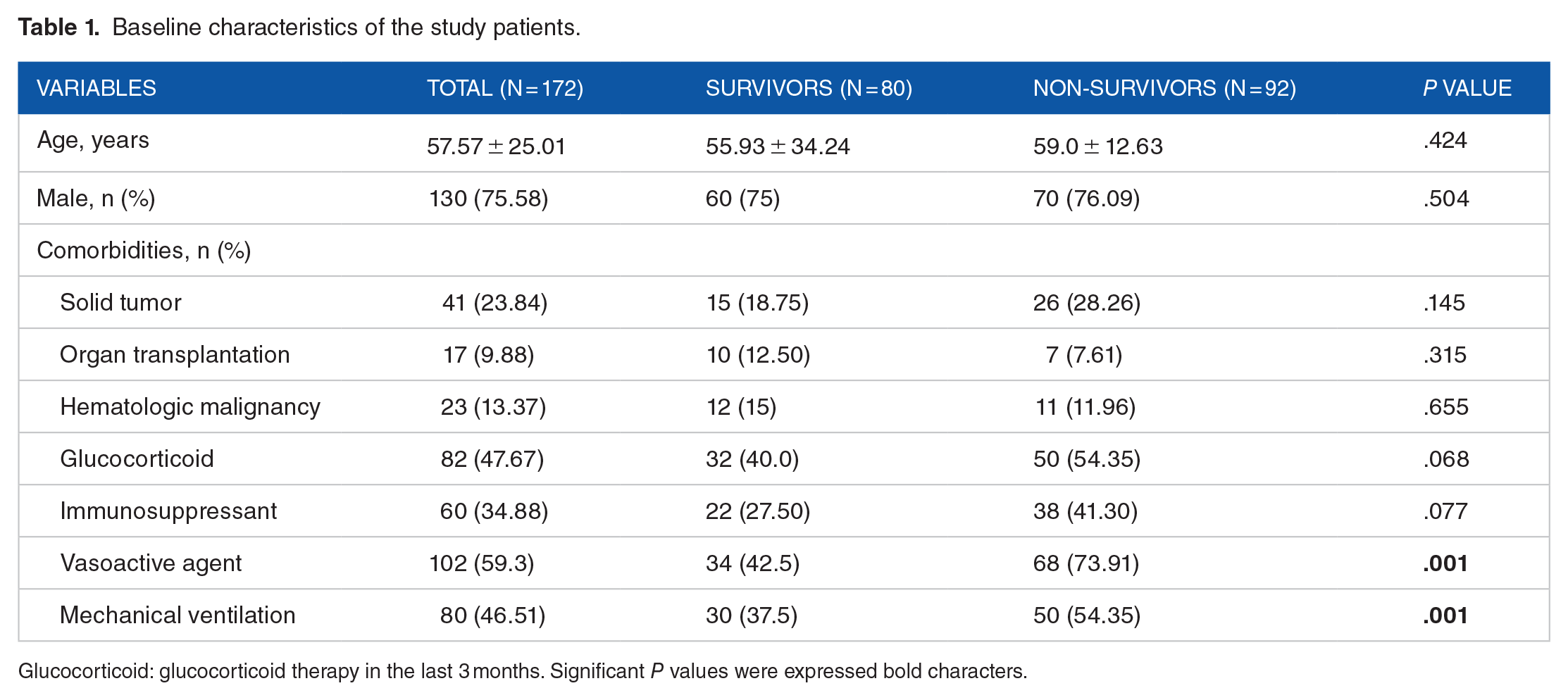
Glucocorticoid: glucocorticoid therapy in the last 3 months. Significant P values were expressed bold characters.
Laboratory characteristics of the study subjects
The laboratory characteristic comparison between the survivors group and the non-survivors group is shown in Table 2. There was no significant difference in white blood cell count and neutrophil counts between the survivors group and the non-survivors group. Of note, the lymphocyte count of non-survivors was less than that of survivors(P = .002). Meanwhile, compared with the survivors group, the NLR, PLR, and SII had increased in the non-survivors group. However, there was no statistically significant difference with respect to other conventional inflammatory markers including procalcitonin (P = .407), C-reactive protein (P = .863), complement C3 (P = .198), and C4 (P = .108) in non-survivors versus survivors.
Clinical and laboratory data of study population.

Abbreviations: WBC, white blood cell count; NEU, neutrophil count; LYM, lymphocyte count; HGB, hemoglobin; PLT, platelet count; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic immune-inflammation index.
Significant P values were expressed bold characters.
Data are presented as mean ± standard deviation. Significant differences are marked by *(P < .05).
Identification of the independent predictor for mortality in sepsis with lymphopenia patients
Binary logistic regression analyses were performed to identify independent predictors of mortality in sepsis with lymphopenia patients. As shown in Table 3, NLR (OR = 6.302, 95% CI: 2.407-16.499, P < .001) and PLR (OR = 3.860, 95% CI: 1.656-8.998, P = .002) were independent predictors associated with mortality in sepsis with lymphopenia patients. Therefore, ROC curve and Youden index analyses were further performed to assess the predictive performance of the predictors and to identify their optimal cut-off values. As shown in Figure 1, NLR showed the largest area under the curve, followed by NLR and then platelet count. In addition, comparisons of the ROC curves of NLR, PLR, and SII further showed that the AUC of NLR was significantly higher than the AUC of PLR and SII. Table 4 showed the best cut-off value of NLR, PLR, and SII established by the Youden index. The AUCs of the NLR, PLR and SII were 0.750 (95% CI: 0.634-0.788, P < .001), 0.662 (95% CI: 0.580-0.743, P < .001), and 0.700 (95% CI: 0.533-0.700, P = .009). When the optimal cut-off value of NLR was 18.93 to discriminate the mortality in sepsis with lymphopenia patients, the sensitivity and specificity were 75.0% and 63.0%, respectively. The optimal cut-off value for PLR was 377.50, with a sensitivity of 67.5% and a specificity of 64.1%.
Binary logistic regression analysis of mortality prediction for study patients.

Abbreviations: LYM, lymphocyte count; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic immune-inflammation index.
Significant P values were expressed bold characters.
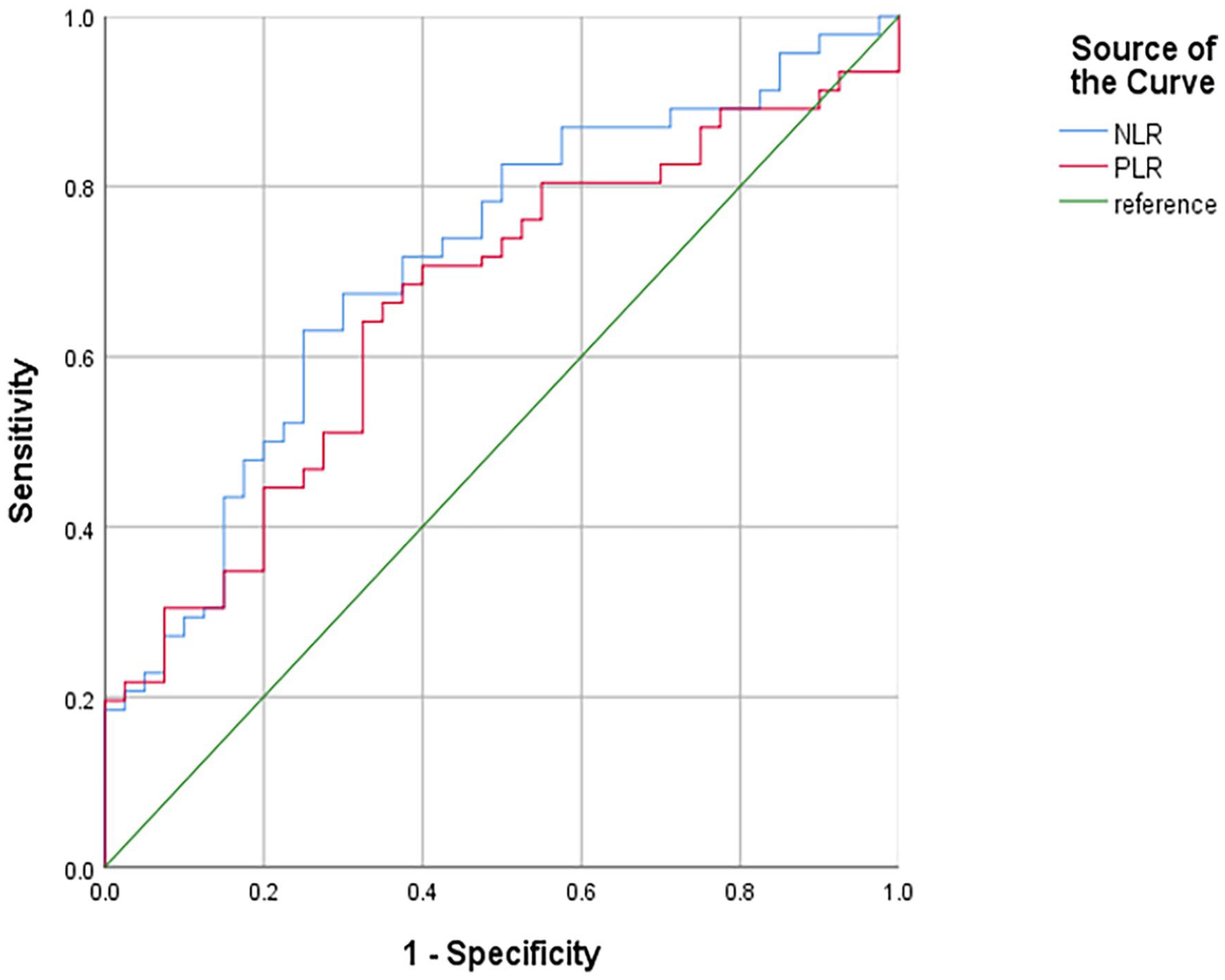
ROC curves for predicting mortality in sepsis with lymphopenia patients.
Predictive value of NLR and PLR for mortality of sepsis patients.

Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Significant P values were expressed bold characters.
Discussion
Sepsis remains the leading cause of death for intensive care unit patients. The complex pathophysiology of sepsis involves the simultaneous activation of inflammation and coagulation disruption in response to pathogens. 16 Sepsis-induced immunosuppression has been implicated as a predisposing factor in the increased susceptibility of patients to secondary infections and mortality. 7 Given the critical role of neutrophils, lymphocytes, and platelets in sepsis development, this study aimed to evaluate the predictive values of NLR, PLR, and SII in sepsis with immunosuppression.
This study demonstrates that NLR and PLR are predictors of mortality in sepsis with lymphopenia. The optimal cut-off value of NLR was identified as 18.93, with sensitivity of 75.0% and specificity of 63.0%. The optimal cut-off value for PLR was 377.50, with a sensitivity of 67.5% and a specificity of 64.1%. The overall mortality is 53.49%, higher than previous studies.
So far, the indicators of immunosuppression in sepsis have not been clearly defined. Lymphopenia and HLA-DR have been used as a marker of immunosuppression in patients with sepsis.17,18 This study defined immunosuppression in sepsis as lymphopenia (lymphocyte count below 1.0 × 109/L). Persistent lymphopenia seems to predict early and late mortality for sepsis patients. 19 However, Blot et al found neither lymphocyte count at the onset nor lymphocyte change during the first 4 days was associated with 12-week mortality for Staphylococcus aureus bacteremia patients. 20 Lymphopenia is not a reliable prognostic biomarker in all causes of sepsis. Further research should explore the role of lymphocytopenia in the subgroups of sepsis.
NLR is easy to obtain in clinical practice. Compared with CRP and PCT, several studies have shown that the NLR has greater prognostic power in adult pneumonia patients.21,22 CRP and PCT had a poor predictive value for sepsis and septic shock mortality, 23 but meta-analysis has verified NLR is a helpful prognostic biomarker for sepsis, ranging from 4.36 to 23.8. 24 To the best of our knowledge, this study is the first to demonstrate the clinical value of NLR measurement for assessing the prognosis in sepsis with lymphopenia patients.
Inflammation plays an important role in the occurrence and development of sepsis. In the face of the invasion of pathogenic bacteria, inflammation induces an increase in neutrophil and thrombocyte count, accompanied by a decrease in lymphocyte count. 25 More evidence is growing that neutrophil play the key role of the innate immune system against infectious injury, while lymphocyte is considered as the major line of the adaptive immune system. 15 As shown in our study, non-survivors group has a lower lymphocyte count. Of course, the mechanism of lymphocytopenia is not clear yet. NLR is a novel biomarker to evaluate the immune status of sepsis for clinical physicians. Further study needs to explore the relevant mechanism.
Platelets play a key role in sepsis-induced organ dysfunction. Sepsis can induce platelet activation, and these activated platelets can exacerbate coagulation disorders and systemic inflammation. 26 Platelets interact with different cells to limit bacterial growth in sepsis models, 27 and to influence leukocyte functions. 28 Wang et al found PLR was a promising biomarker to predict sepsis mortality. 29 As shown in the result, we find the same phenomenon in patients with sepsis with lymphopenia. As a result, increased PLR levels are related to severe inflammation in sepsis patients.
SII has been used as a biomarker for assessing inflammatory burden in certain conditions, such as diabetic kidney injury and severe COVID-19.30,31 Compared to survivors group, non-survivors group has a higher SII. Of note, the trend of SII is consistent with that of NLR and PLR. They are thought to provide a more assessment of inflammatory status. Although CRP and PCT has no significant performance, studies found CRP-based biomarker, such as CRP-to-Albumin ratio, is associated with inflammatory conditions like diabetes and its microvascular complications. 30 Inflammation can lead to malnutrition, and malnutrition can lead to exaggerated inflammation during sepsis. 32
There are some limitations to this study. First, we conducted the retrospective, observational analysis with limited sample size. A large prospective study needs to validate our results. Second, we enrolled all ICU departments, the heterogeneity was unavoidable. Meanwhile, we did not exclude those tumor and organ transplantation patients, although there was no statistical difference, the effects of basic therapy (including corticosteroid and immunosuppressant) on neutrophils and lymphocytes were difficult to eliminate. Finally, we only determined the relationship between NLR and mortality in septic patients. Inflammatory biomarkers (such as interleukin-6) were not included in this study. As we all know, the complex cytokine network is an important feature of sepsis, including pro-inflammatory and anti-inflammatory cytokines, which leads to organ injury.33,34
Conclusion
In conclusion, elevated NLR and PLR were associated with all-cause mortality in sepsis with lymphopenia patients. NLR and PLR levels are strongly connected with inflammation. Further studies are needed to elucidate the relevant pathophysiological mechanisms.