
Abstract
Intraductal papillary mucinous neoplasms (IPMNs) are cystic neoplasms with the potential for progression to pancreatic cancer. Accurate prediction of the malignant potential is challenging and a proper treatment strategy has not been well established. Preoperative neutrophil-to-lymphocyte ratio (NLR) is a biomarker of the malignant potential in patients with several types of malignancy. We explored malignant potential in patients with IPMN. The present study included 56 patients aged of 73 ± 9 years (mean ± standard deviation) who underwent curative resection for IPMN from 1996 to 2017. We analyzed the relationship between the characteristics including NLR and malignant component for predicting pathological results. The nonmalignant IPMN group (N = 21) included patients with low-grade dysplasia (LGD) and intermediate-grade dysplasia (IGD), and the malignant IPMN group (N = 35) included patients with high-grade dysplasia (HGD) and invasive carcinoma. In a univariate analysis, NLR ⩾ 2.2 (P = .001), prognostic nutritional index (PNI) < 45 (P = .016), CA 19-9 > 37 U/mL (P = .039), and cystic diameter ⩾ 30 mm (P = .010), and mural nodule (P = .010) were significantly different between the malignant IPMN and the nonmalignant IPMN groups. Multivariate analysis showed that high NLR (⩾2.2) (odds ratio 9.79; 95% confidence interval: 2.06-45.6), cystic diameter ⩾ 30 mm (4.65; 1.14-18.9), and mural nodule (4.91; 1.20-20.1) were independently predictive of malignant IPMN. These results suggest that preoperative NLR is a useful predictive biomarker for evaluating malignant potential in patients with IPMN.1
Background
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas that was first defined as a mucous-producing tumor in 1982 by Ohhashi et al 1 has malignant potential and progresses via the adenoma-carcinoma sequence. Revisions of the International Consensus Guideline (ICG) for the Management of IPMN indicated that IPMNs were pathologically classified as low-, intermediate-, to high-grade dysplasia (LGD, IGD, and HGD, respectively) and invasive carcinoma based on the degree of dysplasia.2–4 Malignant IPMNs have a poorer prognosis compared with benign IPMNs, and thus, accurate prediction of a malignant potential is of importance at the time of first diagnosis or follow-up.
An invasive carcinoma may lead to impairment of the patient’s immune system through systemic inflammation.5,6 Previous studies have reported that elevated preoperative neutrophil-to-lymphocyte ratio (NLR) is correlated with a poor prognosis in patients with several types of malignancies.6–12 The aim of this study is to explore the significance of preoperative NLR for biomarkers of malignancy in patients with IPMN.
Materials and Methods
Subjects
We retrospectively collected data of 103 consecutive patients with pathologically proven IPMN after surgical resection between May 1996 and December 2017 at the Department of Gastroenterological Surgery, Ehime Prefectural Central Hospital (EPCH). Before the publication of the guidelines, surgical resection was indicated on the base of (1) the presence of symptom, (2) the degree of dilation of the main pancreatic duct, (3) the size of cyst diameters, (4) the presence of mural nodule, and (5) changes over time in cysts, After the publication of the guidelines in 2006 (revised in 2012), the surgery was indicated according to the standards. During this period, 99 patients excluding cases of concomitant pancreatic cancer, bile duct cancer, and gastric cancer underwent curative pancreatectomy. Thirty-seven patients were pathologically diagnosed with nonmalignant IPMN (eg, intraductal papillary mucinous adenoma [IPMA]) and 62 with malignant IPMN (eg, intraductal papillary mucinous adenocarcinoma [IPMC]). Patients who had acute coronary artery disease; myocardial infarction, heart failure; active infection; severe tissue damage; acute massive hemorrhage; acute poisoning; cancer other than IPMN; and blood diseases that affect neutrophil and lymphocyte (eg, myeloproliferative disease and leukemia) were excluded. Patients on medication that may affect neutrophil and lymphocyte were excluded as well. After excluding patients who were not preoperatively examined for NLR, 56 patients (21 with nonmalignant IPMN and 35 with malignant IPMN) were enrolled in this study. The research protocol was approved by the ethics committee of EPCH and each patient provided written informed consent before surgery.
Evaluation of risk factors
Information on the demographic characteristics and risk factors was collected using the clinical files. Body mass index was calculated by dividing weight (in kilograms) by the square of the height (in meters). Blood was collected 2-7 days before surgery, and complete blood count, albumin, C-reactive protein (CRP), glycated hemoglobin (HbA1c), and tumor markers (eg, carcinoembryonic antigen [CEA] and carbohydrate antigen 19-9 [CA 19-9]) were measured before surgery. For cases that have cholangitis with obstructive jaundice, NLR was calculated by blood test after relieving cholangitis by drainage. HbA1c was measured using an automatic biochemistry analyzer and CRP was measured by immunoturbidimetry (JCA BM6070, BioMajesty; JEOL). Serum
Radiological findings of IPMN were preoperatively evaluated by diagnostic imaging modalities including contrast-enhanced computed tomography (CT), magnetic resonance imaging (MRI), and endoscopic ultrasound (EUS). The standardized criteria included anatomic location of the main lesion, IPMN morphology (main duct type, mixed type, branch duct type), main pancreatic duct size, cyst size, presence of mural nodule, abrupt change in caliber of duct, and presence of lymph node swelling. Evaluations of these factors were based mainly on abdominal CT and MRI, and information from other methods was used to support the information gained from them.
In this study, according to the ICG of 2017, “high-risk stigmata” (HS) was defined as IPMN with obstructive jaundice in the head of the pancreas, enhancing mural nodule ⩾ 5 mm or main pancreatic duct ⩾ 10 mm. Similarly, “worrisome features” (WF) was defined as IPMN with pancreatitis, cyst ⩾ 30 mm, enhancing mural nodule < 5 mm, thickened/enhancing cyst walls, main duct size 5-9 mm, abrupt change in caliber of duct with distal pancreatic atrophy, lymph node swelling, increased serum level of CA 19-9, or cyst growth rate ⩾ 5 mm/2 years.
All surgical specimens were analyzed by a single faculty pathologist experienced in the histopathologic classification of IPMN. The specimens were classified into four categories using the World Health Organization IPMN grading system (LGD, IGD, HGD, or invasive carcinoma). When more than one pathological type was present, the tumor was classified according to the worst lesion present. LGD and IGD were considered to be nonmalignant IPMNs, whereas HGD and invasive carcinoma were classified malignant IPMNs. The correlations between malignancy of IPMN and perioperative clinicopathological findings including NLR were assessed retrospectively. In addition, we evaluated the availability of NLR for malignant predictors when combined with the ICG criteria of 2017.
Follow-up and outcome assessment
Patients were followed-up in the Department of Gastroenterological Surgery, Ehime Prefectural Central Hospital. The follow-up time was calculated from the date of diagnosis to the date of death or was censored at the end of follow-up (March 2018). Recurrences were defined as convincing clinical or radiographic evidence of disease.
Statistical analysis
Data are presented as the mean ± standard deviation (SD) unless otherwise specified, and for parameters with non-normal distributions (eg, neutrophil count, lymphocyte count, NLR, albumin, CRP, CEA, and CA 19-9), the data are shown as median (interquartile range) values. In all the analyses, parameters with non-normal distributions were used after log-transformation. Statistical analysis was performed using IBM SPSS Statistics Version 21 (Statistical Package for Social Science Japan, Inc., Tokyo, Japan). Differences among two groups were analyzed by Student’s t test for continuous variables or Pearson’s χ2 test for categorical variables. The statistical correlation between continuous/categorical variables and malignant component was determined using logistic regression analysis. Parameters identified P < .05 by univariate analysis were entered into multivariate analysis to identify independent malignant predicting factors. In addition, areas under the receiver operating characteristic (ROC) curves were determined for each variable to identify the predictors of malignant IPMN. An ROC curve is a plot of the sensitivity (true positive) vs 1 – specificity (false positive) for each potential marker tested. The best markers have ROC curves that are shifted to the left with areas under the curve near unity. Nondiagnostic markers are represented by diagonals with areas under the ROC curves close to 0.5. Likelihood ratios were calculated as the ratios of sensitivity/(1 – specificity) (positive likelihood ratio) and (1 – sensitivity)/specificity (negative likelihood ratio). To determine the optimal cutoffs for the risk of malignancy, the Youden index (sensitivity + specificity − 1) was calculated, and the corresponding value for the maximum of the Youden index was considered as the optimal cutoff point. For the survival analysis, data were censored to determine whether a patient was alive or lost to follow-up (the date of censoring was the date for assessing the last adequate tumor). Overall survival (OS) analysis was performed using the Kaplan-Meier method, and the results were compared by log-rank test. P-value < .05 was considered significant.
Results
Clinical characteristics of patients with IMPN
Clinical characteristics of 56 patients are presented in Table 1. The subjects were divided into two groups: nonmalignant and malignant IPMNs. The nonmalignant IPMN group (N = 21) included patients with LGD and IGD, and the malignant IPMN group (N = 35) included patients with HGD and invasive carcinoma.
Clinical characteristics of patients with IPMN.

Abbreviations: IPMN, intraductal papillary mucinous neoplasm; CA, carbohydrate antigen; CEA, carcinoembryonic antigen; NLR, neutrophil-to-lymphocyte ratio; PNI, prognostic nutritional index.
Data are shown as the means ± standard deviation.
Data for neutrophil count, lymphocyte count, NLR, PNI, CEA, and CA 19-9 were skewed, and are presented as median (interquartile range) values, and the values were log-transformed for analysis.
P-value: Student’s t test for continuous variables or Pearson’s χ2 test for categorical variables. Significant values (P < .05) are presented in bold.
Forty of these 56 patients were asymptomatic at diagnosis (71.4%), and the remaining 16 patients had either pancreatitis or jaundice. Neutrophil count, NLR, prevalence of NLR ⩾ 2.2, prevalence of PNI < 45, CA 19-9, and prevalence of CA 19-9 ⩾
Radiological characteristics of patients with IPMN
Radiological characteristics of 56 patients are illustrated in Table 2. Thirty-seven patients (66.1%) had a main duct involvement (main duct type + mixed type) and 19 (33.9%) a branch duct type IPMN. Presence of mural nodule and cystic diameter ⩾ 30 mm were significantly higher in the malignant IPMN group than in the nonmalignant IPMN group.
Radiological characteristics of the patients with IPMN.

Abbreviations: MD, main duct type; mixed, mixed type; Ph, pancreatic head.
P-value: Student’s t test for continuous variables or Pearson’s χ2 test for categorical variables. Significant values (P < .05) are presented in bold.
Optimal NLR value for predicting malignant IPMN
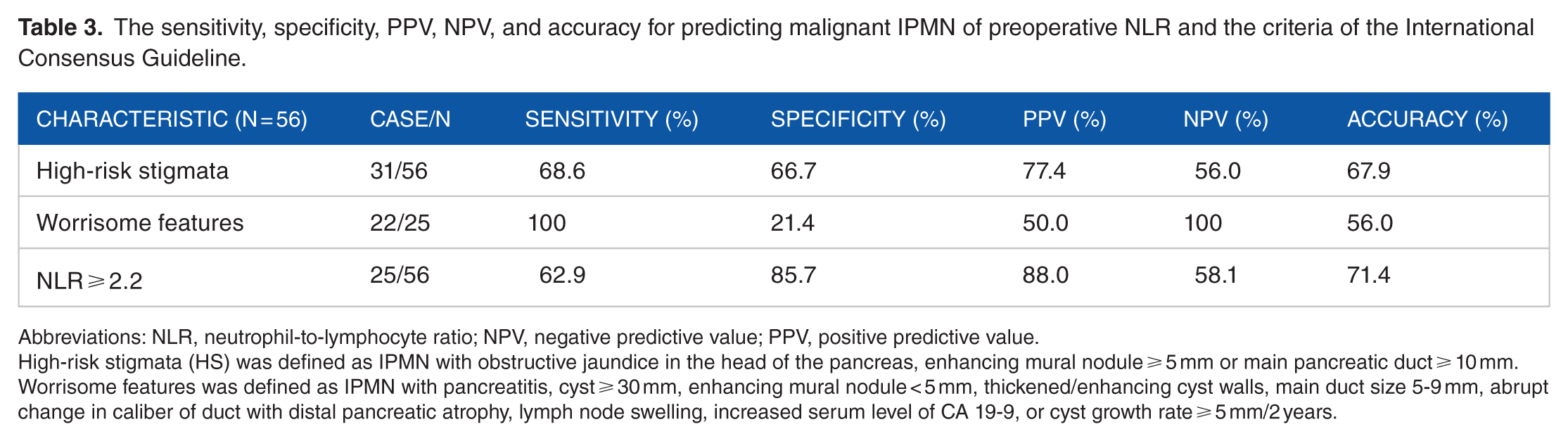
Receiver operating characteristic curve analysis for determining the NLR cutoff value predictive of malignancy in patients with IPMN is shown in Figure 1 (AUC = 0.799, P < .001). The patients were divided into two groups, a low (<2.2) and a high (⩾2.2) NLR group. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy of NLR for predicting malignant IPMN were 62.9%, 85.7%, 88.0%, 58.1%, and 71.4%, respectively (Table 3).
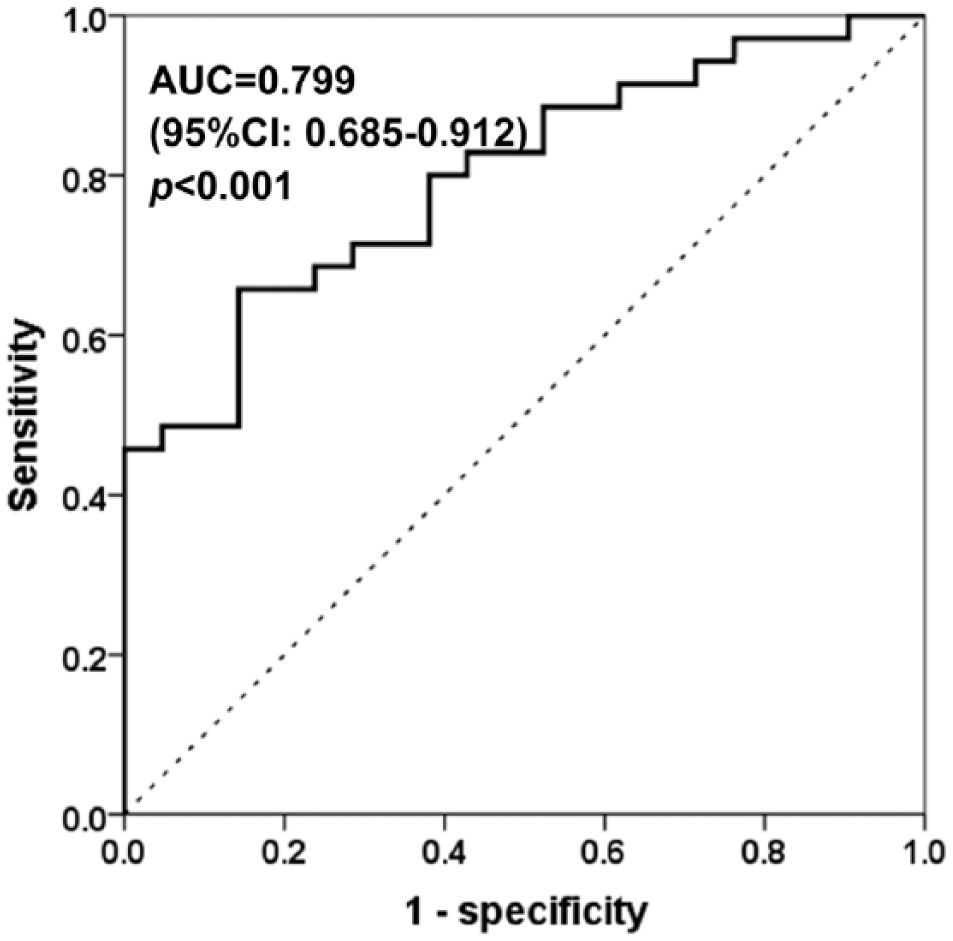
Optimal NLR value for predicting malignant IMPN. Receiver operating characteristic (ROC) curve analysis for determining the NLR cutoff value predictive of malignant potential in patients with IPMN is shown. The curved line is the ROC curve. CI indicates confidence interval.
The sensitivity, specificity, PPV, NPV, and accuracy for predicting malignant IPMN of preoperative NLR and the criteria of the International Consensus Guideline.
Abbreviations: NLR, neutrophil-to-lymphocyte ratio; NPV, negative predictive value; PPV, positive predictive value.
High-risk stigmata (HS) was defined as IPMN with obstructive jaundice in the head of the pancreas, enhancing mural nodule ⩾ 5 mm or main pancreatic duct ⩾ 10 mm.
Worrisome features was defined as IPMN with pancreatitis, cyst ⩾ 30 mm, enhancing mural nodule < 5 mm, thickened/enhancing cyst walls, main duct size 5-9 mm, abrupt change in caliber of duct with distal pancreatic atrophy, lymph node swelling, increased serum level of CA 19-9, or cyst growth rate ⩾ 5 mm/2 years.
Univariate and multivariate analysis for predicting malignant IPMN
Table 4 presents the univariate and multivariate analyses for predicting malignant IPMN. The univariate analysis showed that high NLR (⩾2.2), low PNI (<45), cystic diameter ⩾ 30 mm, and presence of mural nodule were significantly associated with malignant IMPN. The multivariate analysis showed that high NLR, cystic diameter ⩾ 30 mm, and presence of mural nodule were independently predictive of malignant IPMN.
Univariate and multivariate analyses for predicting malignant IPMN.

Abbreviations: CI, confidence interval.
Stepwise logistic regression analysis. “—” did not remain in the final model by logistic regression analysis.
Significant values (P < .05) are presented in bold.
Outcome of patients and survival analysis after surgical resection
Mean OS estimate of all the patients in the Kaplan-Meier curve was 189 (95% confidence interval [CI], 147-231) months. Mean time to postoperative recurrence of the 8 patients with recurrence was 38 (95% CI, 18-58) months. There was a significant difference between the patients with nonmalignant IPMN and those with malignant IPMN regarding RFS (log-rank P = .034). However, RFS showed no significant difference between patients with a high NLR (⩾2.2) and those with a low NLR (<2.2) (log-rank P = .580) (Figure 2).

Disease-specific recurrence probability estimated by the Kaplan-Meier method. There was no difference in recurrence rate between patients with a high NLR (⩾2.2) and low NLR (<2.2) (log-rank test P = .580). There was a significant difference in recurrence rate between patients with a nonmalignant IMPN and those with a malignant IPMN (log-rank test P = .034). IPMA indicates intraductal papillary mucinous adenoma; IPMC, intraductal papillary mucinous adenocarcinoma; NLR, neutrophil-to-lymphocyte ratio.
Malignant potential of IPMN by combining the criteria of ICG and preoperative NLR
The sensitivity, specificity, PPV, NPV, and overall accuracy of “HS” for predicting malignant IPMN were 68.6%, 66.7%, 77.4%, 56.0%, and 67.9%, respectively. With the exception of IPMN with “HS,” those of “WF” for predicting malignant IPMN were 100%, 21.4%, 50.0%, 100%, and 56.0%, respectively. In both the “HS” and “WF” groups, high NLR was significantly associated with malignant IPMN than low NLR (Tables 3 and 5).
Malignant potential of IPMN by combining the criteria of the International Consensus Guideline and the preoperative NLR.

Three cases were excluded from the criteria of the International Consensus Guideline.
Significant values (P < .05) are presented in bold.
Discussion
IPMN of the pancreas has potential of malignancy and most patients with IPMN undergo a series of surgical resections for a long time. However, IPMN exhibits a spectrum of neoplastic transformations ranging from LGD that is benign or low-grade malignancy to invasive carcinoma.13,14 To avoid undergoing pancreatectomy that is associated with a high risk of perioperative complications in patients with such a benign IPMN, the surgical indications of IPMN have changed from early resection to more deliberate observation as proposed by the ICGs of 2006 and 2012 by the International Association of Pancreatology (IAP).2,3 Furthermore, the recently proposed ICGs of 2017 restricted surgical indications more stringently making them more conservative. 4 Even then, the predictive value of ICGs for the presence of malignancy in IPMN can be improved.
NLR is an inflammatory biomarker and elevated NLR has been previously associated with a poor prognostic effect and poor response to chemotherapy in patients with various malignancies.6–12 Similarly, NLR is an independent poor prognostic factor in pancreatic cancer.15–20 On the other hand, reports on the association of NLR and malignant predictive value in IPMN are few. Therefore, we attempted to investigate this relationship.
Our study demonstrated that NLR value of malignant IPMN is significantly higher than that of nonmalignant IPMN (P < .001) and NLR ⩾ 2.2 is an independent predictive marker of malignant IPMN. Recently, some studies have stated that NLR > 2.074, NLR ⩾ 2.551, and NLR > 4 are significance malignant predictors.20–22 The optimal cut-off values have remained controversial. The study that set a cutoff value of 4 for NLR evaluated the malignant prediction of only invasive carcinoma with the exception of HGD. 22 In addition, Arima et al 20 reported that NLR is significantly higher in patients with nonmalignant IPMN than in healthy volunteers. Hata et al 23 demonstrated that preoperative NLR, combined with tumor markers (eg, CEA and AC 19-9) and image findings, can be a useful predictive marker for the presence of HGD/invasive carcinoma in IPMNs. The result suggested that NLR value is correlated with the degree of dysplasia in the adenoma-carcinoma sequence of IPMN.
The multivariate analysis in our study showed that cystic diameter ⩾ 30 mm and presence of mural nodule are independent malignant predictors apart from high NLR. Although pancreatic juice cytology was not evaluated in the analysis for predictors of malignancy, a positive cytology was a high PPV of 100% in our study. Moreover, Hirono et al 24 reported that CEA level in pancreatic juice is an independent factor associated with malignancy. However, routine endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) for sampling of fluid in IPMN was not recommended from the viewpoint of a more invasive method and the risk of dissemination.25,26 Meanwhile, NLR is readily available, inexpensive and is less invasive, as it is calculated from neutrophil and lymphocyte counts preoperatively obtained from collected blood. In addition, Arima et al 27 mentioned that NLR should be examined as well as common tumor markers before planning invasive examinations for patients with pancreatic tumors which should be discriminated from pancreatic ductal adenocarcinomas. Although the sensitivity of NLR was low, its specificity, PPV, accuracy were higher than those in the ICGs criteria including “HS” and “WF.” We also attempted to evaluate the clinical utility of NLR in combination with the ICGs criteria. In patients with “HS” and “WF,” the malignant rate of high NLR was 100% and 72.7%, respectively. Furthermore, high NLR had a significantly higher incidence of carcinoma than low NLR in both “HS” and “WF.” These results support the fact that the ICGs criteria is low PPV and reduce the risk of surgical resection for IPMA. In addition, NLR level may be useful for predicting malignant potential in the follow-up of non-resected IPMN.
A previous report showed that preoperative NLR predicts the long-term outcomes in IPMN cases with invasive carcinoma. 23 The current study demonstrated that there was no significant difference in prognosis between high NLR and low NLR. However, 35 patients with a malignant IPMN had a significantly poor prognosis compared with 21 patients with a nonmalignant IPMN. Therefore, further studies are needed to validate the association between NLR and prognosis in IPMN.
Details of the mechanisms underlying the malignant predictive value of NLR are not entirely understood. Neutrophils can produce some types of cytokines, such as transforming growth factor-beta and vascular endothelial growth factor especially after they integrate with cancer cells; this in turn leads to cancer proliferation, infiltration, and metastasis.28–31 In addition, neutrophils can also produce arginase, nitric oxide, reactive oxygen species and inhibit the function of cytotoxic lymphocytes.32,33 On the other hand, lymphocytes are an important factor for the suppression of cancer progression via the induction of cytotoxic cell death.34,35 Thus, it is widely considered that NLR reflects a balance between a tumor-promoting environment associated with inflammation and an anti-tumor immune system. 36 Consequently, it is suggested that elevated NLR represents both an increased neutrophil count and a decreased lymphocyte count, which indicate a high malignant potential for patients with IPMN. Interestingly, few recent studies reported that postoperative NLR change can be a better indicator than preoperative NLR for predicting survival in patients with different types of cancers such as gastric cancer, lung cancer, and renal cell carcinoma.37–40 When the postoperative NLR was higher than the preoperative NLR, the microenvironment supporting cancer growth persisted, even though the factor related to inflammation was removed. Therefore, the prognosis of such a patient with an elevated postoperative NLR is suggested to be worse than that of a patient with a decreased postoperative NLR. In our study, postoperative changes in NLR before and after surgery cannot be considered.
Some limitations of this study must be considered. First, this study was controlled and retrospective from a single institution. Second, a preoperative differential count of leukocytes could not be performed for some patients; therefore, the NLR value could not be obtained for all the patients with IPMN during the study period and that reduced the sample size. Third, a history of metachronous cancer or the presence of other diseases such as metabolic syndrome, coronary artery disease, chronic obstructive pulmonary disease, hepatic disease and any inflammation-related disease (eg, cholangitis) can change the NLR value, and that may have impacted the results of this study.41–44
Conclusions
Our study demonstrated that elevated NLR is an independent predictive factor for the presence of malignancy in IPMN. We also showed that both the PPV and specificity of a high NLR value are also high. In addition, that NLR value is a significant predictor of malignancy in both ICG criteria. Furthermore, NLR values could be easily measured using preoperative peripheral blood samples, suggesting that preoperative NLR can be a supportive biomarker for the ICG criteria in malignant prediction of IPMN.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RO and RK participated in designing the study, performed the statistical analysis, and drafted the manuscript. RO, MK, JW, MF, HO, MH, TK, and HK contributed to the acquisition of data and its interpretation. RO and RK contributed to the conception and design of the statistical analysis. HK conceived of the study, participated in its design, coordination, and helped to draft the manuscript. All authors read and approved the manuscript.
Availability of data and materials
The data from this study can be acquired from the corresponding author upon reasonable request.