
Abstract
The cause of atopic dermatitis (AD) is multifactorial and a number of genes including cytokines have been involved. We genotyped 315 subjects for polymorphisms in TNF-α and TNF-β and IL-10 genes. Patients had significantly higher frequency of GA genotype of TNF-α (−308 G/A) than healthy controls. Patients with AD and controls had similar distribution of A and G alleles. Genotype AA was found in 7.11% of controls while completely absent in cases. The frequencies of genotypes GG and AA of TNF-β (+252 A/G) polymorphism were higher whereas the frequency of genotype GA was significantly lower in patients than the controls. The frequencies of genotypes GG and AA of IL-10 (1082 G/A) polymorphism were significantly increased whereas genotype GA was decreased in patients than the controls. It is concluded that TNF-α (−308 G/A), TNF-β (+252 A/G), and IL-10 (−1082 G/A) polymorphisms are linked with the susceptibility of AD in Saudis and can be a risk factor.
Introduction
Atopic dermatitis (AD) or atopic eczema is a chronic inflammatory skin disease with characteristic pruritic and eczematous skin lesions involving cutaneous inflammatory hypersensitivity, disturbances in the antimicrobial immune defense, and skin barrier functions. 1 Atopic dermatitis is considered to be the early sign of the atopic march followed by asthma and/or allergic rhinitis and it has been ranked among the top 5 skin diseases. 2 Acute critical and constant allergic symptoms have been reported in about 20% to 30% of infants with eczema.3,4
In general, the prevalence of allergic diseases has increased steadily in recent years. The prevalence of AD is 15% in developed countries and is substantially higher among children. 5 Due to high prevalence of AD in a number of countries, it is considered a major problem worldwide.6,7 Moreover, there is a strong association of AD with atopy and about 80% of infants with AD have been found to have atopy. 8
The cause of AD is multifactorial with genetic as well as environmental factors influencing disease development. It involves activation of multiple immunologic and inflammatory pathways. 9 A genetic linkage to AD has been demonstrated in various populations and genetic factors have been reported to play a significant role in the etiopathogenesis of AD.10–12 Several candidate genes have been associated with the susceptibility of AD. Studies based on single nucleotide polymorphism (SNP) and genome-wide association in different population worldwide have shown that a number of genes including cytokines, chemokines, human leukocyte antigens, drug-metabolizing, and many other genes of innate/adaptive immune systems are associated with AD susceptibility.2,5,10,13 The cytokines are known as key role players in the development of the clinical manifestations of several chronic inflammatory diseases. A population-dependent association between chronic inflammatory diseases and cytokine gene polymorphisms has been reported.10,14–18
Tumor necrosis factor (TNF)-α (MIM 191160) and TNF-β (also known as lymphotoxin alpha, LT-α; MIM 153440), on chromosome 6p21, share a common receptor. 19 Tumor necrosis factors are generally associated with cell-mediated immunologic reactions. The role of functional polymorphisms of these cytokine genes in the occurrence and course of AD has been investigated by several researchers, but the results are inconsistent.11,13,20–23
Interleukin-10 (IL-10) is involved in immunosuppression of the acquired immune response, and decreased IL-10 serum concentration in patients has been associated with higher activity AD. 24 IL-10 gene maps to the junction of 1q31-q32 and its promoter region is substantially polymorphic and has been correlated to the transcriptional variations.25–27 The literature on the role of IL-10 gene polymorphisms in AD development is scarce and inconsistance.28–30
To the best of our knowledge, no study has been performed to analyze the association of TNF-α, TNF-β, and IL-10 polymorphisms in Saudi patients with AD. This study was undertaken to evaluate the association of SNPs in TNF-α and TNF-β at positions −308 and +252, respectively, and IL-10 at positions −592, −819, and −1082 with the AD in a Saudi cohort.
Subjects And Methods
Subjects
Three hundred fifteen Saudi subjects were recruited from Dermatology Clinic of Prince Sultan Military Medical City (PSMMC), Riyadh, Saudi Arabia. One hundred four unrelated patients with AD aged 1 to 63 years (mean age 21 years) and 211 unrelated healthy controls (aged 5-60 years) with no evidence of atopy or any autoimmune diseases were genotyped for TNF-α, TNF-β, and IL-10 gene polymorphisms. Exclusion criteria were subjects with history of any other autoimmune or inflammatory diseases. Inclusion criteria were patients with moderate to severe AD who consented to participate in this genetic study. The patients with AD were diagnosed following the standard criteria of Hanifin and Rajka. 31 The approval for this study was obtained from the research and ethical committee of the hospital and prior written informed consent was obtained from all the subjects. All the subjects were interviewed and their medical records were checked to get detail information about demographic and clinical features. Patients with AD were divided into the 2 groups depending on the clinical features as with moderate or with severe AD.
PCR amplification
Standard methods were used to extract genomic DNA from the peripheral blood of patients with AD and controls. According to the study protocol, TNF-α, TNF-β, and IL-10 genes were amplified using amplification refractory mutation systems (ARMS)-PCR methodology. 32 PCR amplification was carried out with specific optimized reaction conditions as described elsewhere. 33 Genotyping was repeated for 25% of the random samples for quality control.
Statistical analysis
Statistical significance was calculated by Fisher’s exact test and P values ⩽.05 were considered significant. Odds ratios, relative risk (RR), etiologic fraction (EF), and preventive fraction (PF) were calculated following the Woolf method as mentioned in our earlier publication. 34
Results
The demographic and clinical features of patients with AD are summarized in Table 1. The male to female ratio in patients with AD was 55:49 (1:1.6). The clinical manifestation or prognosis of the disease was quite similar in men and women. The mean duration of disease was 7.2 ± 5.5 years. The distribution of TNF-α (−308 G/A) and TNF-β (+252 A/G) variants in patients and controls are summarized in Tables 2 and 3. Genotype distributions in cases and control were in Hardy-Weinberg equilibrium. It can be seen from Table 2 that the frequency of GA genotype of TNF-α (−308 G/A) was significantly increased in patients than control (P = .02). Although the genotype GG of TNF-α (−308 G/A) was lower in patients with AD than controls, the difference was statistically insignificant (P = .32). The distribution of alleles A and G was almost similar in patients and controls. The genotype AA was present in 7.11% of the controls whereas completely absent in patients with AD (Figure 1).
Demographic/clinical features of atopic dermatitis patients.

Abbreviation: AD, atopic dermatitis.
Genotype and allele frequencies of TNF-α (G−308 A) variants in patients with AD and matched controls.

Abbreviations: AD, atopic dermatitis; EF, etiologic fraction; n, number of subjects, PF, preventive fraction; RR, relative risk; TNF, tumor necrosis factor.
Data for EF.
Statistically significant.
Genotype and allele frequencies of TNF-β (LTα) – interon1 + 252 variants in patients with AD and matched controls.

Abbreviations: AD, atopic dermatitis; EF, etiologic fraction; n, number of subjects, PF, preventive fraction; RR, relative risk; TNF, tumor necrosis factor.
Data for EF.
Statistically significant.

TNF-α (−308 G/A) variants in atopic dermatitis patients and controls. TNF indicates tumor necrosis factor.
On the contrary, the frequency of GG genotype of TNF-β (+252 A/G) promoter polymorphism was significantly higher in patients with AD than controls (P = .02) whereas heterozygous GA genotype was significantly lower in patients with AD than controls (P < .01) as indicated in Table 3. Significantly higher frequency of genotype AA was found in patients with AD than controls (P = .02). No difference was detected between the frequencies of TNF-β A and G alleles between patients with AD and healthy controls as shown in Table 3 and Figure 2.

TNF-β (+252 A/G) variants in atopic dermatitis patients and controls. TNF indicates tumor necrosis factor.
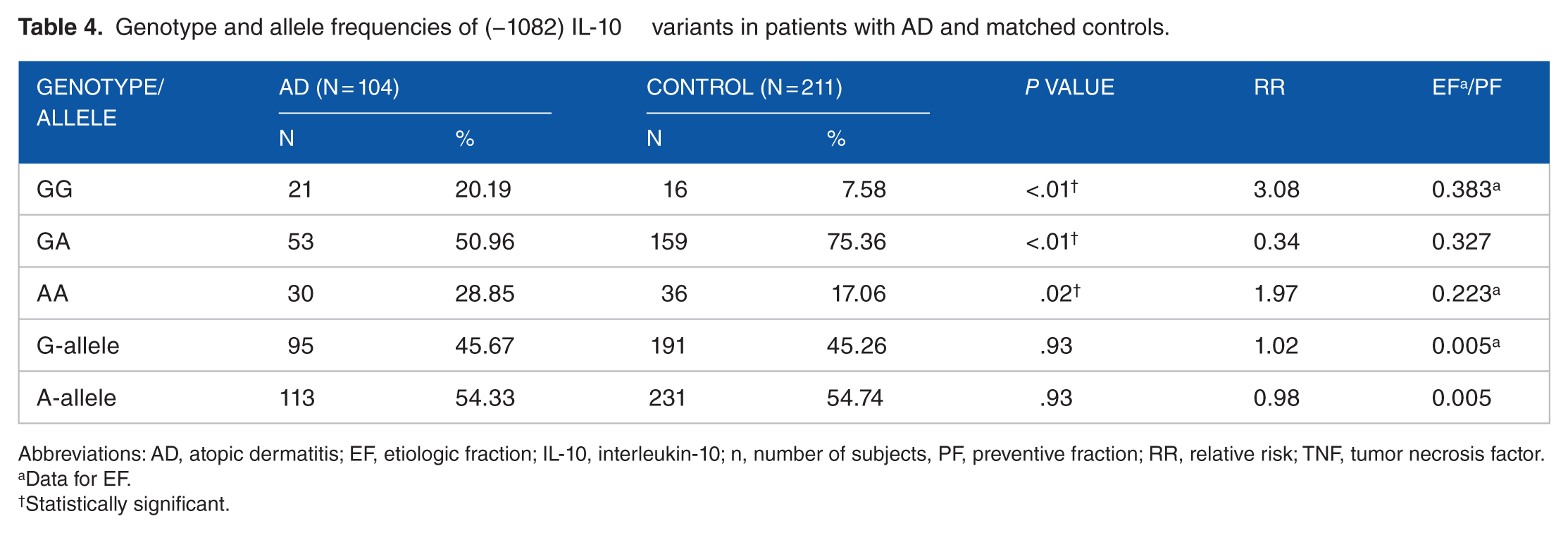
The genotyping results for IL-10 polymorphisms at positions −1082, −592, and 819 are presented in Tables 4 to 6. In comparison with controls, the genotypes GG and AA of IL-10 (−1082 G/A) were significantly increased whereas genotype GA was decreased in patients with AD (P = .01) as shown in Table 4 and Figure 3.
Genotype and allele frequencies of (−1082) IL-10 variants in patients with AD and matched controls.
Abbreviations: AD, atopic dermatitis; EF, etiologic fraction; IL-10, interleukin-10; n, number of subjects, PF, preventive fraction; RR, relative risk; TNF, tumor necrosis factor.
Data for EF.
Statistically significant.
Genotype and allele frequencies of (592 C/A) IL-10 variants in patients with AD and matched controls.

Abbreviations: AD, atopic dermatitis; EF, etiologic fraction; IL-10, interleukin-10; n, number of subjects, PF, preventive fraction; RR, relative risk; TNF, tumor necrosis factor.
Data for EF.
Genotype and allele frequencies of (819 C/T) IL-10 variants in atopic dermatitis patients and matched controls.

Abbreviations: AD, atopic dermatitis; EF, etiologic fraction; IL-10, interleukin-10; n, number of subjects, PF, preventive fraction; RR, relative risk; TNF, tumor necrosis factor.
Data for EF.

IL-10 (–1082 G/A) variants in atopic dermatitis patients and controls. IL-10 indicates interleukin-10.
On the contrary, the difference in the frequencies of alleles and genotypes of IL-10 (−819 C/T) and IL-10 (−592 C/A) polymorphisms between patients with AD and controls was not significant as indicted in Tables 4 to 6. Although the frequencies of genotypes −819 CC and −592 CC were lower, those of −819 CT, −819 TT, 592 CA, and 592 AA were higher in patients with AD than controls (Tables 4-6).
Discussion
The results of present study indicated that GA genotype of TNF-α (308 G/A) polymorphism is significantly associated with susceptibility of AD whereas GG genotype may be protective to the disease. A similar association has been reported with occupational allergic dermatoses in Russian patients. 35 However, GA genotype of TNF-α (308 G/A) is significantly decreased and the frequency of GG genotype is increased in the patients showing a negative association of this polymorphism with AD and atopic asthma in Iranian 23 and Croatian patients. 36 On the contrary, some studies have indicated no association of TNF-α (308 G/A) polymorphism with AD susceptibility in English, 37 German, 20 Americans. 14 Chinese, 38 and Macedonians subjects. 11
These differences in associations of TNF-α (−308 G/A) polymorphism with disease might be due to variations in sample size, genotyping methods, and/or ethnicity, as frequencies of TNF (−308) alleles and genotypes also vary in different ethnic healthy populations worldwide. 39 Saudi population being a closed and isolated society with high rate of consanguinity (inbreeding) is ideal for such genetic associations as it has also been suggested earlier that special attention should be paid on genetic association studies in ethnic groups like Saudi Arabians that have remained isolated from the rest of the world populations and has retained their own cultural characteristics, lifestyle, and traditions. 40
Our results of TNF-β (+252 A/G) polymorphism indicated that the GG genotype was significantly associated with AD (P = .02) whereas heterozygous GA genotype was protective to patients with AD (P < .01). The TNF-β (+252 A/G) polymorphism has also been reported to be associated with atopy in Italian 41 and atopic asthma in Taiwanese. 42 However, no association between polymorphisms in the TNF-β gene and atopic diseases in the Czech population was reported by Izakovicová Hollá et al. 43
The production of TNF-α and TNF-β is influenced by genetic factors. TNF-α (308 G/A) polymorphism has been associated with variations in TNF-α levels by various researchers.44-46 The AG genotype of TNF-α (308 G/A) is considered as high TNF producing whereas the GG genotype as low TNF producing. 23
The TNF-β (+252 A/G) polymorphism consists of 2 alleles, Adenine (A) and Guanine (G) at position +252 in the first intron of the gene. Allele G is mutant allele known as TNF-β *1 (allele-1) which is rare and associated with higher production of TNF-α and TNF-β.47,48
These 2 polymorphisms in TNF-α and TNF-β genes due to their specific location regulate the TNF-α/TNF-β gene expression and ultimately affect the amount of cytokines produced and make an individual susceptible to atopic diseases. Genetic polymorphism of TNF-α (308 G/A) has earlier been reported to change cytokine expression in the stratum corneum, and consequently affecting susceptibility to chronic dermatitis.49,50
The higher frequency of genotype GA of TNF-α (308 G/A) polymorphism in our cases as compared with controls indicated the susceptible role of this polymorphism in the occurrence of AD. It has also been reported to be associated with increased risk of related diseases including asthma, 51 atopy, 52 bronchial hyperreactivity, 53 and allergic rhinitis. 54
The defective, spontaneous, unstimulated production of TNF-α in skin of patients with AD has been documented55,56 and attributed to the TNF-α−308 GA genotype which has been suggested to be associated with a moderately high production of TNF-α.44,46 Simultaneously GG genotype of TNF-β (+252 A/G) might have resulted in the increase of TNF-α level.47,48 Therefore, it is suggested that in AD, a part of the pathogenesis is related to increased TNF-α production and its higher activity in the skin, due to the presence of TNF-α−308 GA and TNF-β-GG genotypes. Further allergen exposure has been related with the increased production of TNF-α in the epidermis of patients with AD, and an higher level of TNF-α has also been observed in the blood lymphocytes of patients with acute AD as compared with the controls.57,58
Our results on anti-inflammatory cytokine gene IL-10 polymorphism suggested that genotype −1082 GG and genotype −1082 AA are susceptible to AD, whereas genotype −1082 GA may be refractory to AD. Similarly, higher risk for developing AD has been demonstrated with patients carrying G allele of IL-10 (−1082 G/A) polymorphism in Polish30,59 and Czech patients. 22 IL-10 (1082 G/A) polymorphisms has also been associated with increased allergies and risk for persistent late-onset wheezing in young Finish children who suffered from bronchitis in early-life, 60 occupational allergic dermatoses in Russian, 35 and with preschool asthma in early infancy. 61 A recent meta-analysis shows a non-significant association between the IL-10 (−1082 G/A) polymorphism and AD. 62 Stavric et al 11 reported that genotype IL-10 (−1082 AG) is susceptible whereas IL-10 (−1082 AA) is protective to AD in population of Macedonians. Contrarily, no association has been found between AD and the IL-10 (−1082 G/A) polymorphism in German and Japanese20,63 indicating the ethnic variations.
Sohn et al 28 reported an association between IL-10 promoter polymorphism and the clinical picture of AD in children. Lacy et al 29 also suggested an association of this polymorphism with AD after observing higher frequency of thymine-guanine-adenine-cytosine (TGAC) haplotype of the IL-10 gene in patients with AD. Lesiak et al 30 analyzed IL-10 serum concentration and IL-10 (1082 G/A) polymorphism in patients with AD and suggested a role of G allele in synthesis of IL-10 in the patients with moderate to severe AD. IL-10 being immunosuppressive cytokine inhibits the activity of both T (H) cell types in human subjects. 30
On the contrary, results of genotyping for IL-10 (−819 C/T) and IL-10 (−592 C/A) polymorphisms suggested no significant association of these 2 polymorphisms on AD susceptibility as the distribution of their alleles and genotypes was almost same in cases and controls. In accordance to our results, no association of IL-10 (−819 C/T) and IL-10 (−592 C/A) polymorphisms has been documented in moderately severe chronic AD in Caucasian, 64 Chinese, 38 Macedonian, 11 and Japanese patients with AD. 63
Contrarily, −819 C/T, and −592 A/C have been reported to be significantly associated with AD in Czech 22 and Korean population, 28 with increased allergies and risk for persistent late-onset wheezing in young Finish children 60 and with occupational allergic dermatoses in Russian patients. 35
AD has been defined as a biphasic disease including an initial phase predominated by T helper type 2 (Th2) cytokines and later more chronic Th1-dominated eczematous phase.9,65 Lymphocytes T(H)2-type only are activated in acute form of AD whereas lymphocytes of both T(H)1- and T(H)2-type are dominated in more chronic forms of AD. Thus, both innate and adaptive immunity defects may be responsible for the biphasic nature of AD.66,67
Conclusions
It is concluded that TNF-α (−308 G/A), TNF-β (+ 252 A/G), and IL-10 (−1082 G/A) polymorphisms are associated with the susceptibility and can be a risk factor for AD in Saudis.
Footnotes
Acknowledgements
The authors wish to thank the administration of MSD for providing excellent facilities.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceived and designed the experiment: MA. Performed clinical examinations, collected demographic data: GBH, FAH, MAS. Extracted DNA, performed genotyping: SR. Analyzed the data, interpreted the results and drafted the manuscript: MA. Agree with manuscript results and conclusions: GBH, FAH, MAS, AA. Jointly developed the structure and arguments for the paper: MA, SR. Made critical revisions, supervised and approved final version: AA, MA. All authors reviewed and approved of the final manuscript.