
Abstract
Objectives
The aim of this study was to describe the clinical, laboratory and thyroid imaging features of 17 adult cats with spontaneous hypothyroidism diagnosed over a 4-year period in four countries.
Methods
This multicenter case series included cats diagnosed with spontaneous hypothyroidism between 2021 and 2025. We collected data on cats’ signalment, clinical signs, results of physical examination, routine laboratory and thyroid hormone testing, and thyroid imaging (scintigraphy, ultrasonography or CT). We also reviewed treatment data, including levothyroxine dosage, changes in serum thyroid hormone and creatinine concentrations, clinical progression and follow-up scintigraphy.
Results
Cats were aged 2–14 years, with no breed predilection; 10 (58.8%) were male and seven (41.2%) female. Common clinical signs included lethargy, dermatologic signs (unkempt hair coat, increased shedding, dandruff, hair thinning), weight gain or obesity, and palpable goiter. The most common laboratory findings included azotemia (five cats), anemia (three cats) and worsening of pre-existing diabetes mellitus (two cats). A total of 13 (76.5%) cats had low serum thyroxine (T4), whereas all cats had high thyroid-stimulating hormone (TSH) concentrations. Thyroid imaging confirmed undetectable or atrophic thyroid tissue in 10 (58.8%) cats and bilateral thyroid enlargement in seven (41.2%). After levothyroxine treatment (median 133 µg/cat/day) in 15 cats, serum total T4 concentration increased and TSH fell. Treated cats became more alert and active, goiter resolved, azotemia resolved or improved, and two achieved remission of concurrent diabetes mellitus.
Conclusions and relevance
This study broadens current knowledge of spontaneous hypothyroidism in adult cats, a condition that remains underrecognized in clinical practice. Atrophic hypothyroidism appears more common than previously recognized, although goitrous hypothyroidism was identified in more than 40% of cats. Spontaneous hypothyroidism should be considered in cats with unexplained azotemia and in diabetic cats with worsening glycemic control. Levothyroxine supplementation reliably improved or resolved clinical signs in all treated cats.
Plain language summary
Why was the study done? Spontaneous hypothyroidism (an underactive thyroid gland) is common in people and dogs but has been thought to be very rare in cats. However, it may actually occur more often than most veterinarians realize. In this study, we describe the signs, test results and response to treatment in 17 adult cats with newly diagnosed hypothyroidism. What did the researchers do? We reviewed medical records from 17 adult cats diagnosed with hypothyroidism between 2021 and 2025 in four different countries. We collected information about their age, sex, clinical signs, blood test results, thyroid hormone levels and imaging tests (such as ultrasound and thyroid scans). We also looked at how well the cats responded to thyroid hormone replacement therapy (levothyroxine). What did the researchers find? The cats were aged 2–14 years. Most were domestic shorthair or longhair cats, with a slight male predilection. The most common problems were lethargy, weight gain and a poor-quality hair coat. Routine blood tests often showed anemia, kidney problems and low thyroid hormone levels. Imaging revealed that some cats had enlarged thyroid glands (goiter), while others had shrunken glands (atrophy). Once thyroid hormone treatment started, the cats became more active, their blood tests improved and kidney function often returned to normal. Remarkably, two cats with diabetes even went into remission after starting thyroid therapy. What do the findings mean? This study shows that naturally occurring hypothyroidism does happen in adult cats and may be more common than previously thought. With the right diagnosis and thyroid hormone treatment, affected cats usually recover well, with an improved quality of life.
Introduction
Spontaneous primary hypothyroidism in adult cats remains an uncommon but likely underdiagnosed endocrine disease, with only 18 cases reported in the global literature to date.1 –10 In contrast to the more frequently reported congenital hypothyroidism, which typically manifests in kittens within the first few months of life with signs of disproportionate dwarfism and mental dullness,11,12 the adult-onset form presents quite differently. Most adult hypothyroid cats exhibit vague and subtle clinical signs – such as lethargy, poor hair coat and weight gain – that are easily overlooked or misattributed.1 –10
Kittens usually develop congenital hypothyroidism due to dyshormonogenesis,13,14 a defect in thyroid hormone biosynthesis that results in low serum thyroxine (T4) concentrations, high thyroid-stimulating hormone (TSH) concentrations and bilateral thyroid gland enlargement (goiter).11,12,15 In adult cats, however, spontaneous primary hypothyroidism may arise from a broader spectrum of underlying thyroid pathology, including lymphocytic thyroiditis, idiopathic atrophy and diffuse follicular hyperplasia (goitrous hypothyroidism), but again resulting in low serum T4 and high TSH concentrations.1 –5,11,12
In this study, we sought to expand knowledge of spontaneous primary hypothyroidism in adult cats by characterizing clinical features, laboratory abnormalities, thyroid imaging findings and response to levothyroxine therapy in 17 additional cases diagnosed across four countries over a 4-year period.
Materials and methods
Case selection and data collection
We compiled a multicenter, observational, descriptive case series (ambispective data collection 16 ) of 17 adult cats (aged >1 year 17 ) diagnosed with spontaneous primary hypothyroidism between 2021 and 2025. A total of 10 cats had been referred to two specialized centers in nuclear medicine and endocrinology. To identify additional cases, the primary investigators (GCC and MEP) contacted approximately 30 veterinary endocrinologists and invited them to contribute unpublished cats with hypothyroidism confirmed by documenting low to low–normal serum total T4 and high TSH concentrations. Cases originated from four countries: Brazil (n = 8), USA (n = 4), Argentina (n = 4) and Italy (n = 1).
Each submission was reviewed to confirm that hypothyroidism had been diagnosed in the absence of prior treatment with sulfonamides/trimethoprim, methimazole, radioactive iodine (131I) or thyroidectomy (exclusion criteria). Required data for enrollment included age, breed, sex, clinical signs, duration and onset of signs, primary reason for evaluation, body condition score, presence of palpable goiter, routine laboratory testing (complete blood count, serum biochemistry, urinalysis), and serum T4 and TSH concentrations. Thyroid imaging by scintigraphy, ultrasonography or CT was also required to differentiate goitrous from atrophic hypothyroidism (see S1 in the supplementary material).5,15,18
After pretreatment data collection, cats receiving levothyroxine were re-evaluated at intervals of approximately 3 months with the goal of normalizing serum thyroid values. Treatment-related data recorded for this study included initial levothyroxine dosage, changes in serum thyroid hormone and creatinine concentrations, levothyroxine dose adjustments, clinical response, follow-up scintigraphy images, survival time and cause of death, when known.
Serum T4 and TSH assays
Serum T4 concentration was measured either by chemiluminescent enzyme immunoassay (CEIA), homogenous enzyme immunoassay or radioimmunoassay, with all methods validated for use in cats.5,19 –24 Serum TSH was measured by CEIA using a canine TSH assay, validated for use in cats as previously described.5,21,24,25
Data and statistical analyses
Statistical analyses were performed using GraphPad Prism version 10.61 (GraphPad Software). Data were assessed for normality using the D’Agostino–Pearson test. 26 Most data were not normally distributed; therefore, all analyses were performed using non-parametric tests.
Most data are presented with descriptive and summary statistics (median, interquartile range [IQR; 25th–75th percentile], range, proportions). Wilcoxon signed-rank tests were used to compare serum concentrations of total T4, TSH and creatinine before and after levothyroxine administration. For all analysis, statistical significance was defined as P ⩽0.05.
Results
Signalment of hypothyroid cats
The 17 adult cats were aged 2–14 years (median 8, IQR 6.5–10.5) at the time of diagnosis. Of the cats, 16 (94.1%) were domestic shorthairs and one was Siamese. Ten (68.8%) cats were male and seven (41.2%) were female; all were neutered.
History, clinical presentation and physical examination findings
The most common clinical signs reported by owners included lethargy, weight gain and hair coat changes, such as an unkempt appearance, increased shedding, dandruff, hair thinning or coat lightening (Table 1, Figure 1). Less frequently reported signs included upper respiratory stridor and voice change. Owners reported that clinical signs had been present for 2–96 months before diagnosis (median 12 months, IQR 4–24), with first signs noticed when they were aged 2–11 years.
Clinical presentation, routine laboratory findings and pituitary–thyroid axis hormone concentrations in 17 adult cats diagnosed with spontaneous hypothyroidism

Data are n (%)
BCS = body condition score; T4 = thyroxine; TSH = thyroid-stimulating hormone

Images of three adult domestic shorthair cats diagnosed with spontaneous hypothyroidism. (a,b) A 2-year-old male cat initially presented with hair coat lightening, lethargy and weight gain (body condition score 7/9). After treatment with levothyroxine, the cat’s lethargy resolved, and the normal darker coat color returned to its normal pigmentation. (c) A 3-year-old female cat showing clinical signs of weight gain, lethargy, seborrhea and dandruff. (d) An 11-year-old female cat with lethargy, weight gain and a poor-quality hair coat
The primary reason for the initial clinical work-up by the referring veterinarian included lethargy, dermatologic changes and obesity (BCS >6/9), followed by palpable goiter or worsening of pre-existing diabetes mellitus (Table 1). Less common reasons included respiratory stridor, voice change or bradycardia. Both thyroid lobes were palpable (goiter) in seven (41.2%) cats, while thyroid lobes were not palpable in 10 (58.8%) cats (Table 1).
Laboratory findings and diagnosis
Of the 17 cats, the most common routine clinicopathology abnormality was azotemia (serum creatinine >2.0 mg/dl) in five cats (Table 1, Figure 2). Serum cholesterol concentration was high (>300 mg/dl) in three cats, glucose concentration was high (>300 mg/dl) in three, whereas three had mild non-regenerativive anemia (Table 1).

Serum concentrations of total thyroxine (T4) (a), thyroid-stimulating hormone (TSH) (b) and creatinine (c) in hypothyroid cats, measured before (n = 17) and after initiation of treatment with levothyroxine (n = 15). Note the increase in total T4 concentration and the decrease in serum TSH and creatinine concentrations after levothyroxine therapy. Shaded areas indicate reference intervals. To convert T4 concentration from μg/dl to nmol/l, multiply by 12.87. To convert creatinine concentration from mg/dl to nmol/l, multiply by 88.4
Of the 17 cats, 13 (76.5%) had low total serum T4 concentrations, whereas three had low–normal concentrations (Table 1, Figure 2). All cats had high TSH concentrations (Table 1, Figure 2), in the range of 1.10–>12 ng/ml (median 4.25).
In one cat, hypothyroidism was also confirmed by TSH stimulation testing, with low baseline T4 concentration remaining below 1.0 µg/dl 6 h after intravenous administration of 25 µg recombinant human TSH. 27
Thyroid imaging findings
Thyroid scintigraphy was performed in 10/17 cats. In 5/10 (50%) cats, qualitative analysis revealed bilateral thyroid enlargement (goiter) along with markedly increased 99mTc-pertechnetate uptake (%TcTU) by thyroid tissue (Figure 3). In one cat with bilateral goiter, scintigraphy also revealed two distinct foci of ectopic thyroid tissue exhibiting radionuclide uptake – one located at the base of the tongue and another in the cervical region – the last one visible exclusively on images obtained by a pin-hole collimator (Figure 4a).15,28 Quantitative scintigraphic analysis of cats with goitrous hypothyroidism demonstrated that all evaluated parameters – including %TcTU, thyroid:salivary gland (T:S) ratio and thyroid volume – exceeded upper reference limits (Figures 3 and 4).

Thyroid scintigraphy in goitrous hypothyroidism. (a) Normal thyroid scintigraphic image in a euthyroid cat. The rostral arrow indicates the salivary glands and the caudal arrow indicates both thyroid lobes, which exhibit normal volume, morphology and radionuclide (99mTc-pertechnetate) uptake. (b–d) Thyroid scintigraphy scans of three adult cats diagnosed with spontaneous goitrous hypothyroidism. In all cats, both thyroid lobes are symmetrically enlarged and exhibit intense and homogeneous radionuclide uptake, which is markedly higher compared with the uptake observed in the salivary glands. Scans were acquired using a low-energy high-resolution collimator5,15,28

Thyroid scintigraphy scans from a 9-year-old female domestic shorthair cat with spontaneous goitrous hypothyroidism. (a) The black and white image represents a planar scintigraphic image acquired using a low-energy high-resolution collimator, while the color image was obtained using a pin-hole collimator in the same cat. The thyroid lobes appear bilaterally enlarged and demonstrate a high 99mTc-pertechnetate uptake (11.24%, reference interval [RI] 0.05–0.8), high thyroid:salivary gland (T:S) ratio (5.71, RI 0.5–1.5) and large thyroid lobe volume (1.74 cm3, RI 0.2–1.0). In addition, two foci of ectopic thyroid tissues are seen: one at the base of the tongue (upper arrow) and another in the cervical region (lower arrow). (b) Repeat scintigraphy of the same cat after levothyroxine therapy (100 µg once daily). The thyroid lobe volume, 99mTc-pertechnetate uptake (0.5%) and T:S ratio (0.64) have all returned to normal. The previously ectopic foci of thyroid tissue could no longer be visualized
In contrast, thyroid scintigraphy in 5/10 (50%) cats showed no detectable thyroid tissue, with %TcTU and T:S values below the reference interval (RI), consistent with atrophic hypothyroidism (Figure 5).
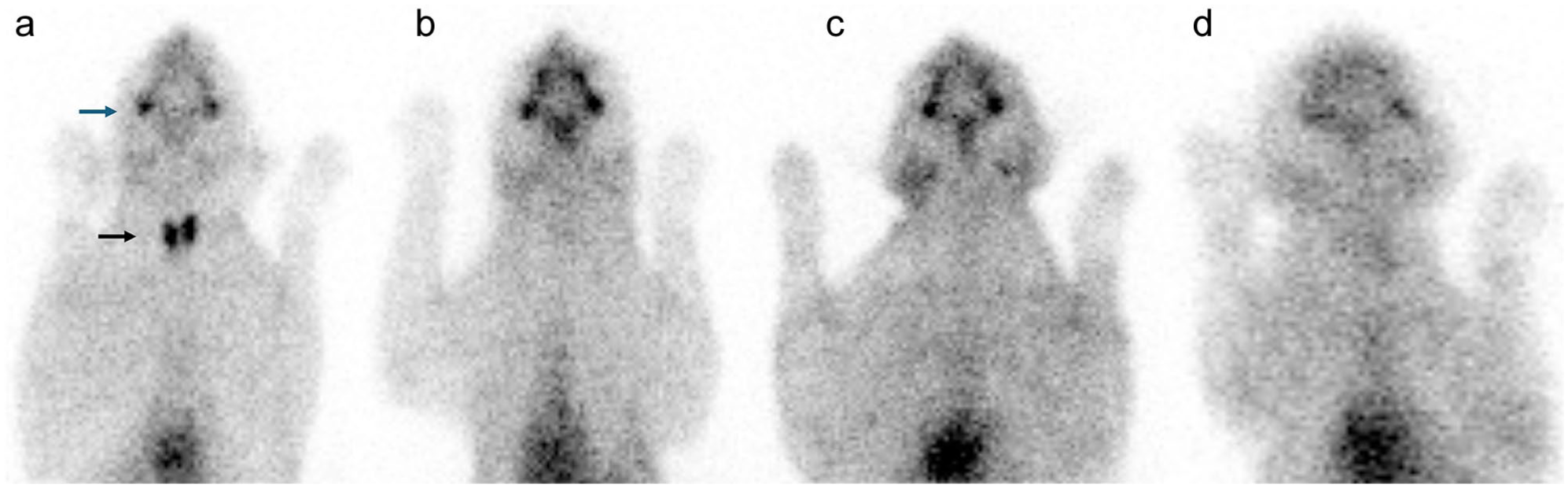
Thyroid scintigraphy in atrophic hypothyroidism. (a) Normal thyroid scintigraphy scan of a euthyroid cat. The upper arrow indicates the salivary glands and the lower arrow highlights both thyroid lobes, which exhibit normal volume, morphology and radionuclide uptake. (b–d) Thyroid scintigraphy scans of three adult cats diagnosed with spontaneous atrophic hypothyroidism. No radionuclide uptake by thyroid tissue is observed in these images, supporting the diagnosis of hypothyroidism due to thyroid atrophy. Scans were acquired using a low-energy high-resolution collimator
Of the seven cats that did not undergo thyroid scintigraphy, six had cervical ultrasonography. Bilateral thyroid enlargement was observed in 2/6 (33.3%) of these cats, with total thyroid volume in the range of 4.5–8.2 cm3. In the other 4/6 cats, ultrasonography showed reduced thyroid volume (range 0.05–1.14 cm3), diagnostic for thyroid atrophy. Finally, in the remaining cat that did not undergo scintigraphy or ultrasonography, no thyroid tissue was visualized on CT, supporting the diagnosis of thyroid atrophy.
In one cat with goitrous hypothyroidism, repeat scintigraphy after 12 months of levothyroxine treatment showed reduced thyroid size, normalization of uptake parameters and disappearance of ectopic nodules (Figure 4a,b).
Levothyroxine treatment and outcome
After diagnosis, 15/17 cats were treated with levothyroxine. One cat did not receive treatment because of aggressive behavior and the owner’s inability to administer oral medication. At 26 months after diagnosis, the cat was euthanized because of poor quality of life. Another cat developed diabetes mellitus with poor appetite 1 month after diagnosis of hypothyroidism; the owner elected euthanasia because of poor quality of life.
Levothyroxine treatment was initiated at a median dose of 100 µg/cat/day (range 50–150). After 6 months, this median dose increased to 150 µg/cat/day (range 100–300). When adjusted for body weight, the median starting dose was 20.3 µg/kg/day (range 10.5–34.9) and the 6-month dose was 27.2 µg/kg/day (range 13.3–42.9). Of the 15 treated cats, 10 received levothyroxine once daily and five were treated twice daily.
Of the 15 cats treated, 13 became more alert and active within 4–6 weeks of starting levothyroxine. Goiter resolved in six affected cats, four lost weight and three regained normal hair coat texture. Two cats with concurrent diabetes achieved remission. Less common signs – including bradycardia, vomiting, constipation, voice change and respiratory stridor – also resolved. In addition, the cat with coat lightening regained its original color (Figure 1b). No adverse effects from levothyroxine were observed.
After levothyroxine treatment, serum concentrations of total T4 increased and TSH decreased (Figure 2a,b). All treated cats achieved normal T4 concentrations, although four maintained slightly high TSH concentrations. Serum creatinine also decreased (Figure 2c), normalizing in all but one cat with pretreatment azotemia.
The median treatment time of the 15 treated with levothyroxine was 15.5 months (IQR 7.0–24). Of the 17 cats, four are known dead: two were euthanized owing to poor quality of life, one died of pulmonary adenocarcinoma and one succumbed to sepsis secondary to a limb abscess.
Discussion
This study expands the limited veterinary literature on spontaneous hypothyroidism in adult cats. Although considered rare, the diagnosis of 8/17 cases in a single country (Brazil) over only 4 years suggests that most general practitioners still fail to include naturally occurring hypothyroidism in adult cats in the differential diagnosis. The addition of four new cases from the USA further reinforces that spontaneous hypothyroidism remains an ongoing and underdiagnosed disease in this adult population of cats.
Cats in this study were aged 2–14 years (median 8) at diagnosis, consistent with previously reported age ranges for adult cats diagnosed with spontaneous hypothyroidism.1 –7,10 Males accounted for 10/17 (58.8%) cases, aligning with the male predominance (6/7, 86%) reported in one case series. 5 Although the cause of this apparent sex bias remains unknown, the findings from both studies indicate a male predisposition for adult-onset hypothyroidism in cats.
In this study, the most common reasons for initiating a clinical work-up were dermatological changes (eg, dull or unkempt coat, increased shedding, dandruff or seborrhea), lethargy, weight gain or obesity, palpable goiter and worsening of pre-existing diabetes mellitus. Similar to previous reports, most cats exhibited only mild dermatologic changes and none developed total alopecia.1 –7,10 A distinctive finding in this series was one cat whose primary clinical sign was coat lightening, which fully resolved and returned to normal coloration after levothyroxine supplementation. In humans, thyroid hormones have been reported to restore pigmentation in terminal hair, reversing graying – an effect likely mediated by their action on follicular melanocytes. 29
Two of our cats initially presented with worsening diabetes mellitus, both of which achieved diabetic remission after treatment with levothyroxine for hypothyroidism. Thyroid atrophy was confirmed in both cats by CT or scintigraphy. A third cat also developed diabetes mellitus 1 month after the initial diagnosis of hypothyroidism but was not treated. To our knowledge, this is the first study to report an association between adult-onset hypothyroidism and diabetes mellitus in cats. In humans and dogs, however, primary hypothyroidism has been linked to peripheral insulin resistance and poor glycemic control in diabetic patients.30 –35 Furthermore, studies in dogs have shown that levothyroxine supplementation can reduce insulin resistance.30,36
Although the pathogenesis of diabetes in hypothyroid cats requires further study, thyroid hormone deficiency likely impairs insulin-mediated glucose uptake in skeletal muscle and adipose tissue and perturbs hepatic lipid metabolism – changes that promote peripheral insulin resistance which can improve with levothyroxine replacement. These findings suggest that hypothyroidism should be considered in diabetic cats with worsening glycemic control, particularly when accompanied by dermatologic abnormalities.
One of our cats developed voice change and another developed respiratory stridor as major clinical features. After levothyroxine treatment, signs resolved in both cats. Similar reversible respiratory abnormalities occur in human patients with hypothyroidism, likely due to naso-oropharynx and larynx narrowing from myxedema or goiter.37 –39
Thyroid atrophy as a cause of spontaneous adult-onset hypothyroidism has previously been reported in four cats – two associated with lymphocytic thyroiditis1,4 and two with absent radionuclide uptake on scintigraphy.2,5 In a previous report, only 1/7 affected cats had thyroid atrophy, while the remaining 6/7 showed goitrous hypothyroidism. 5 This is in contrast to the present study, in which imaging (ultrasound, CT or scintigraphy) showed that 10/17 (58.8%) cats had thyroid lobes that were either not visible or markedly reduced in size. Although none of our cats underwent thyroid biopsy or had histopathologic examination, these findings suggest thyroid atrophy may be a more common cause of adult-onset hypothyroidism in cats than previously recognized.
Of our 17 cats, seven had palpable bilateral goiter, confirmed with thyroid imaging (ultrasonography or scintigraphy). In five of these goitrous hypothyroid cats, scintigraphy demonstrated bilateral, symmetrical thyroid lobe enlargement with homogeneously increased %TcTU – a pattern similar to that seen in kittens with congenital hypothyroidism due to thyroid peroxidase (TPO) gene mutations causing dyshormonogenesis,13,14 as well as in cats with drug-induced hypothyroidism from TPO inhibition by sulfonamides.23,40 These findings highlight the need to consider inherited enzymatic defects and sulfa drugs as a potential cause of goitrous hypothyroidism in adult cats. None of our cats had a history of sulfonamides therapy, which is known to interfere with TPO activity.
As previously described, serum TSH measurement proved to be a valuable diagnostic tool for identifying hypothyroidism in the cats in this study, similar to other reports of kittens with congenital or adults with natural or iatrogenic hypothyroidism.2 –7,10 –12,41,42 All 17 of our cats showed very high serum TSH concentrations. A total of 13 cats had low total T4 concentrations (ie, overt hypothyroidism12,25,43), whereas the remaining four cats had T4 concentrations that remained within the lower RI (ie, subclinical hypothyroidism12,25,43).
In dogs, concurrent disease may lower T4 levels – a phenomenon known as non-thyroidal illness syndrome.44,45 In the recovery phase from severe illness in these dogs, serum TSH can rise to slightly high concentrations (but generally remains <0.8 ng/ml).44,45 In cats, high TSH concentrations associated with non-thyroidal illness have not yet been documented, 46 although further investigation is warranted in cats recovering from critical illness. In our study, none of the cats had severe comorbidities or were in a recovery phase at the time of hypothyroidism diagnosis, and most had very high TSH concentrations (>1.0 ng/ml).
Azotemia was the most common abnormality found on routine laboratory testing, present in 5/17 of our untreated hypothyroid cats. After levothyroxine replacement, serum creatinine concentrations returned to within the RI in 4/5 of these cats. In humans, dogs and cats, hypothyroidism can reduce the glomerular filtration rate (GFR), leading to pre-renal azotemia.47 –53 In dogs and humans, levothyroxine treatment increases GFR and lowers serum creatinine concentrations.49,54 In cats, an association between adult-onset hypothyroidism and azotemia is also well established, with renal parameters improving after levothyroxine.5,41 Based on these findings, hypothyroidism should be included in the differential diagnosis of azotemic CKD and serum T4 and TSH measured in adult cats with unexplained azotemia.
After levothyroxine, all treated cats showed clinical improvement as serum T4 increased and TSH fell. In addition, follow-up scintigraphy in one cat with goitrous hypothyroidism demonstrated a return of parameters to within normal RIs (Figure 4). The median levothyroxine dose administered to our cats was 138 µg/cat/day or 33 µg/kg/day, which is comparable to the 32.7 µg/kg/day dose reported in another series of cats with spontaneous, adult hypothyroidism. 5 Other case reports have described similar treatment doses, ranging from 100–200 µg/cat/day, with both clinical and laboratory improvement observed in all treated cats.1 –4,6,7
This study has several limitations, including its observational design, participation of multiple clinicians in different countries, variability in laboratory methods for T4 measurement and thyroid imaging modalities, and incomplete follow-up data. Because inclusion required biochemical confirmation of primary hypothyroidism (low to low–normal T4 with high serum TSH concentrations), cats with early or central hypothyroidism and normal TSH concentrations were not studied. Consequently, the frequency and severity of reported abnormalities (eg, lethargy, dermatologic changes, azotemia) may not reflect the full clinical spectrum of adult-onset feline hypothyroidism. These findings should therefore be considered descriptive and hypothesis-generating rather than estimates of prevalence.
Conclusions
This multicenter case series shows that adult cats with spontaneous hypothyroidism present with vague signs such as lethargy, weight gain, dermatologic changes, azotemia or poorly controlled diabetes, highlighting the need for greater clinical suspicion. Diagnosis was confirmed by finding low to low–normal T4 with high TSH concentrations, while imaging distinguished goitrous from atrophic hypothyroidism. Levothyroxine consistently improved clinical and biochemical outcomes, including resolution of azotemia, reversal of goiter and diabetic remission. Spontaneous hypothyroidism should be considered in adult cats with unexplained dermatologic changes, weight gain, azotemia or poor diabetic control.
Supplemental Material
S1
Protocols for thyroid imaging in cats with spontaneous hypothyroidism.
Footnotes
Acknowledgements
The authors thank Dr Letícia Machado for her assistance in identifying feline cases for inclusion in this case series.
Supplementary material
The following file is available as supplementary material:
S1: Protocols for thyroid imaging in cats with spontaneous hypothyroidism.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues or samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.