
Abstract
Objective:
Thyroid ectopy is a rare condition resulting from abnormal embryologic development and migration of the gland. Sublingual is the most common thyroid ectopy; all other ectopic thyroid locations occur very rare. There are no reports in the literature that describe the clinical course of patients with congenital hypothyroidism due to thyroid ectopy.
Methods and Results:
We present a child with congenital hypothyroidism detected on neonatal screening which had a subclinical course during follow-up. Scintigraphy revealed submental thyroid ectopy, a rare ectopic location and no orthotopic thyroid gland.
Conclusion:
Our case is unique because of the rare ectopic thyroid location but also of the unexpected clinical course; however, further thyroid monitoring is required for the therapy adjustment and detection of any changes in the ectopic tissue.
Introduction
Thyroid dysgenesis (TD) accounts 80%–85% of the cases of permanent congenital hypothyroidism (CH). The different forms include athyreosis, ectopic gland, hypoplasia and hemiagenesis. 1 Nearly 60% of TD cases are due to thyroid ectopia,2,3 a rare condition affecting 1:100,000–300,000 individuals of the general population and 1:4000–8000 patients with thyroid disease. 4 Thyroid ectopia results from a developmental defect in the early stages of thyroid embryogenesis, during its passage from the floor of the primitive foregut to the final pretracheal position. The most common location is the sublingual region reported in 90% of cases. 4 Occasionally, a dual thyroid gland is found, with one orthotopic part and an ectopic part located elsewhere in the neck region.4,5 Submental thyroid ectopy is extremely rare. 6
The clinical presentation of thyroid ectopy is quite variable. It might go unrecognized for decades and be detected by chance or during the diagnostic investigation of subclinical hypothyroidism or later in life when an infection or tumor in the neck region is revealed. 7 Most of the ectopic thyroids became symptomatic during pregnancy and puberty because these conditions result in hypertrophy of the thyroid tissue. Sudke et al. 8 reported a very rare case of lingual thyroid presenting with hematemesis in a pregnant woman.
Thyroid scintigraphy with 123-iodine or 99m-technetium pertechnetate is the imaging standard and the only reliable method for precise localization and evaluation of the anatomical structure of an ectopic thyroid gland. 9
Depending on the amount of ectopic tissue, the thyroid-stimulating hormone (TSH) values on neonatal screening can be as high as in thyroid agenesis, only slightly elevated or normal. It almost always occurs sporadically. Transcription factors encoding genes PAX8, TTF-2, NKX2.1 and NKX2.5 may be implicated in TD in a small number of cases, 1 although recent evidence showed that NKX2.5 mutations do not play a major pathogenic role in TD. 10 However, no specific mutations have been associated with thyroid ectopia. 1 Here, we present a child with CH detected on neonatal screening following an unexpected clinical course and a submentally located thyroid gland.
Case report
A 5.5-year-old girl was diagnosed with primary CH through screening at the age of 2 weeks. She was a firstborn child of young, healthy parents. The child was delivered after 39 weeks of gestation with forceps-assisted vaginal delivery. The anthropometric parameters were adequate for the gestational age. The Apgar score was 5 and 7 in the first and fifth minute, respectively; thus, initial oxygen stabilization was required. The heel-prick blood test for CH screening performed 72 h after birth showed an elevated TSH value of 12.3 mIU/L (DELFIA neonatal TSH, LKB). Confirmatory serum tests performed at 14th postnatal day (IMMULITE 2000 chemiluminescent enzyme immunoassay system; Siemens Healthcare Diagnostics Inc., NY, USA) showed high TSH level, 30.9 mIU/L (normal: 0.4–5.0 mIU/L) and low T4, 4.38 µg/dL (normal: 6.4–13.3 µg/dL). Ultrasound examination revealed no visible thyroid gland in the usual position and the patient was diagnosed with primary CH due to TD. Therapy with levothyroxine (10.5 µg/kg/day) was initiated and thyroid hormone levels normalized within 2 weeks. The patient was subsequently followed up at 3-month intervals. Several higher values of TSH were noted (up to 6.19 mIU/L). After the first year, she remained euthyroid with a levothyroxine dose tapered down to 1.8 µg/kg/day. Results of thyroid tests and levothyroxine dose during the follow-up are presented in Table 1. The growth and neurodevelopment were completely normal. At the age of 3 years, after several consecutive normal serum thyroid results, the levothyroxine dose was gradually decreased and then discontinued at the age of 3.5 years. At this point, she was lost from follow-up.
Thyroid hormone test results during the child’s follow-up.
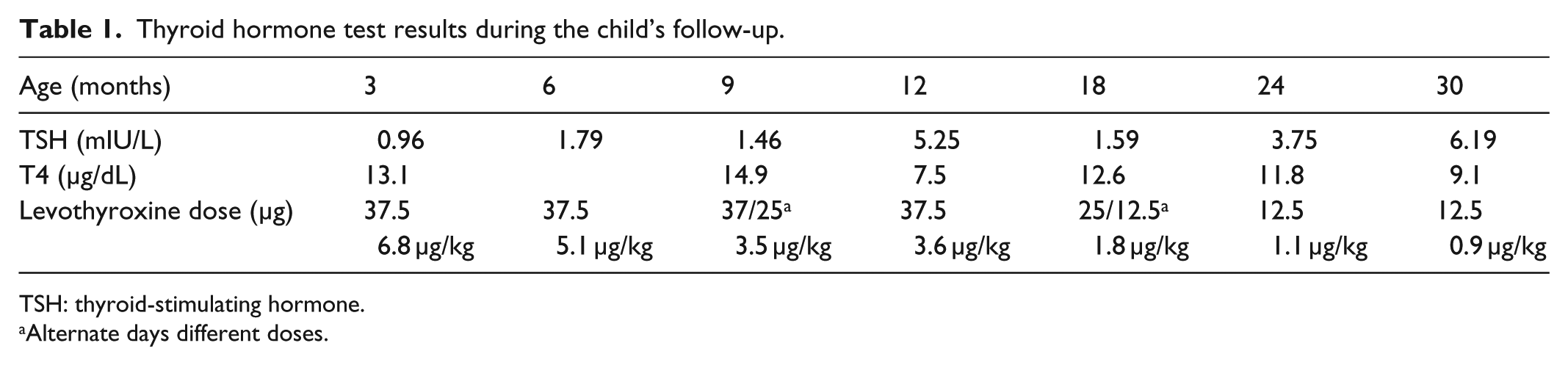
TSH: thyroid-stimulating hormone.
Alternate days different doses.
After 2 years off therapy (at the age of 5.5 years), the girl was referred for investigation of anemia with the following blood counts: hemoglobin (Hb), 10.0 g/dL (normal: 11.5–14.0 g/dL); red blood cell count (RBC), 4.98 × 106/µL (normal: 4.0–5.3 × 106/µL); serum iron, 3.7 µmol/L (normal: 6.6–26 µmol/L). Her height and weight were on the 50th percentile for age, there were no signs of clinical hypothyroidism, and she had normal neurocognitive development. The thyroid testing showed mildly elevated TSH (7.8 mIU/L) and low FT4 level 0.856 ng/dL (normal: 0.89–1.76 ng/dL). Thyroid peroxidase (TPO) antibodies were within normal range, 20 IU/mL (reference range: 10–35 IU/mL).
Ultrasonographic investigation of the neck (Figure 1) detected no thyroid tissue at the normal pretracheal thyroid location but presence of submentally located oval formation (12 mm × 18 mm) of iso- and hypoechoic, nonhomogeneous thyroid-like tissue, mostly with peripheral vascularization.

Ultrasonographic appearance of submentally located ectopic thyroid tissue.
A thyroid scan was performed by a double-head Mediso gamma camera after an intravenous injection of 99m-technetium pertechnetate (2 MBq/kg), and standard images (anterior, lateral) were obtained in supine position. Scintigraphy showed ectopic thyroid tissue located submentally without any uptake in the normal thyroid location (Figure 2). Magnetic resonance imaging (MRI) showed marked round formation in the submental region, in the projection of the floor of the mouth (Figure 3). The follow-up thyroid hormone tests after 1 month were consistent with subclinical hypothyroidism; thus, low dose levothyroxine was re-introduced. Furthermore, close thyroid follow-up is scheduled to access child’s need for therapy and dose adjustment.

99mTcO4− thyroid scintigraphy revealed no radioactivity at the normal thyroid location but very intensive accumulation of the radiotracer in the middle neck line, submentally, suggesting the ectopic thyroid tissue.
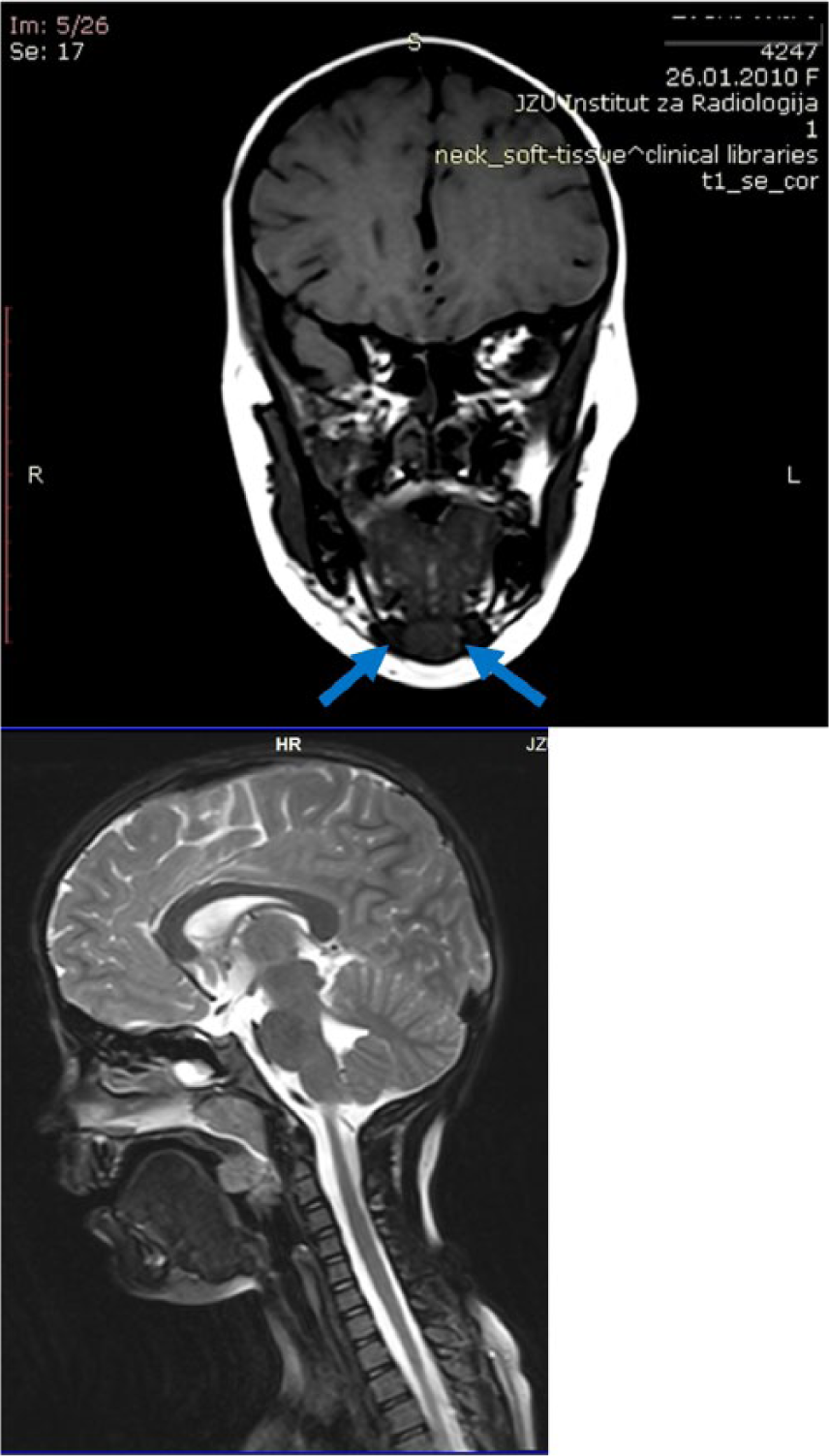
MRI imaging of the head and neck showed an oval mass submentally at the level of the floor of the mouth and no thyroid in usual neck position.
Discussion
Our patient is unique because of not only the extremely rare location of the ectopic thyroid tissue but also the high TSH level at neonatal screening that subsided upon introduction of therapy and remained normal with a very low levothyroxine maintenance dose. Her TSH value at birth on screening was 12.3 mIU/L which is slightly above the cut-off level. Following the international screening trends, 11 we adopted TSH cut-off level 10 mIU/L in our country since 2010. Lowering the TSH cut-off level to 10 mIU/L raised an important clinical issue, whether the increased number of mild cases are transient or require permanent treatment. 12 Olivieri et al. 13 reviewed 1676 cases with CH and found that 21.6% of patients with permanent CH had only mild TSH elevation (<15 mIU/L) on screening. Surprisingly, 19.6% of these patients had TD. These data point to a conclusion that even newborns with mild abnormalities on neonatal screening have a significant risk of permanent CH since the variations in the neonatal TSH are quite common.12,13 Our patient is another supportive case that lower TSH cut-off level on screening is really beneficial for some patients.
A round, oval or dumbbell-shaped ectopic lingual thyroid lacking lateral lobes is the most common form of thyroid ectopy and is usually the sole thyroid tissue without an orthotopic thyroid gland. 5 All other ectopic thyroid locations are very rare. The largest study in the literature on thyroid ectopy by Gu et al. included an analysis of 42 patients aged 6–85 years over a 34-year period. The location of the ectopic thyroid in their study was lingual (64%), sublingual (17%), dual (12%) and other locations (7%). None of the patients had submental ectopy. Most of the analyzed patients were asymptomatic and euthyreotic. 14 Other rare ectopic thyroid locations described in the literature are as follows: adrenal gland, 15 mediastinum 16 and submandibular region. 17
Patil et al. 18 analyzed 17 patients with thyroid ectopy; they found mostly sublingual location and there was no case of submental ectopy. Of all patients, 41.1% of the cases had CH, whereas 52.9% had acquired pubertal or adult-onset hypothyroidism.
In another study that evaluated 82 patients with CH due to TD, an ectopic thyroid gland was present in 32 patients and only three children had submental ectopy; however, the age or hormonal values in these children were not specifically described. 6
Most of the data available in the literature report high initial TSH values at birth in CH children with thyroid ectopy.6,19 Perry et al. reported only 2 out of 12 patients with thyroid ectopy, with screening TSH levels between 15 and 50 mIU/L; all others had a mean TSH level of 144 mIU/L. 19 There are no reports that describe the clinical course of CH patients due to thyroid ectopy, especially those with mildly increased TSH at screening.
Scintigraphy is the standard method for diagnosis of ectopic thyroid tissue and should be performed as a part of the diagnostic procedure of CH in newborns. Our patient underwent thyroid ultrasonography at the time of diagnosis of CH and was classified as having TD without any further differentiation. The technique used for imaging in newborns differs between centers and depends mostly on local experience and availability. Ultrasonography is less invasive, more available and sufficient to differentiate between a structural defect and a normal or enlarged thyroid gland, whereas scintigraphy, either with radioactive iodine or technetium, performed when the TSH concentration is still high enables an exact localization of an ectopic thyroid gland. 20 However, as the demonstration of an ectopic gland versus athyreosis does not change the need for therapy initiation, in our center, as in many other pediatric centers, scintigraphy is not performed at diagnosis but is postponed until a later age when children are off treatment and are being re-evaluated. Scintigraphy in our patient showed that the submental tissue was the sole thyroid tissue present, as there was no uptake in the normal thyroid location. Kim et al. 21 reported subclinical hypothyroidism in a 7-year-old girl with dual thyroid ectopy. Submental ectopy with normal thyroid function tests was reported by El-Shafie et al. in a 27-year-old woman. She presented with large non-tender swelling at the base of the tongue, increasing in size and affecting the speech. The patient was treated with single-dose radioactive Iodine-131 therapy and was prescribed lifelong thyroxine replacement therapy. 22
Nodular goiter, adenoma, Hashimoto’s thyroiditis, colloid goiter and thyroid cysts might occur in ectopic thyroid glands similar to orthotopic thyroid glands, leading to thyroid dysfunction in patients, such as hypothyroidism or subclinical hyperthyroidism. 14 Another clinical concern regarding ectopic thyroid glands is their potential risk for malignant transformation which is rare, but described in the literature even in children.23,24
In conclusion, although thyroid ectopy is common cause of TD, it still remains enigma in the pathophysiology of thyroid disease. Our patient presents a rare case of submental thyroid ectopy without orthotopic thyroid gland diagnosed as CH, but had an unexpected subclinical course during the follow-up. Thus, patients with TD presented with one form of abnormal thyroid function may progress or develop other forms of thyroid dysfunction. Regular thyroid monitoring and imaging follow-up is warranted, as for adjustment of the hormone replacement therapy, also for detection of any changes in the ectopic tissue.
Footnotes
Acknowledgements
All the authors have accepted responsibility for the entire content of this submitted manuscript and approved submission. M.K. helped in diagnosing, following and treating the patient, ultrasound check-up, designing and writing and editing of the manuscript; N.Z. helped in designing, writing and editing of the manuscript, searching literature and following the patient; M.Z. helped in performing scintigraphy, ultrasound and editing of the manuscript; V.A. is responsible for newborn thyroid screening, detecting the patient and editing of the manuscript; D.P.G. helped in performing scintigraphy and ultrasound, interpretation of the results and writing and editing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
All procedures performed in study were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments. Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was obtained from child parents. Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.