
Abstract
Objectives
This two-part study investigates the relationship between risk factors, injury patterns and survival rates in cats affected by high-rise syndrome (HRS). By identifying key prognostic and predictive factors, such as age, fall height and impact surface, we aim to enhance veterinarians’ ability to provide accurate prognoses and optimise patient management. In addition, this study seeks to address inconsistencies in the literature by re-evaluating the influence of these factors on injury severity and survival outcomes.
Methods
We analysed medical records and radiographs from 1125 cases of feline HRS treated at the Freie Universität Berlin’s small animal clinic between 2004 and 2013. All cases involved falls from a minimum height of 4 m. Data collected included sex, age, body weight, fall height, impact surface, injury details, prior treatment, time to veterinary presentation (>4 h or <4 h), radiographic findings and survival outcome.
Results
Among the 1125 HRS cases, circulatory shock was observed in 48.6%, craniocerebral injury in 2.8%, thoracic trauma in 58.3%, orofacial lesions in 51.1% and blunt abdominal trauma in 14.6%. Musculoskeletal injuries were common, with limb fractures occurring in 47.2% of cases and pelvic fractures in 11.1%. The overall survival rate was 87%, while 13.3% of cats died or were euthanased as a result of trauma severity or poor prognosis. Significant correlations were found between injury severity, age, impact surface and fall height.
Conclusions and relevance
This study includes the largest sample of HRS cases in cats to date, providing essential insights for veterinarians and pet owners regarding prognosis and treatment protocols. Although survival rates are high, euthanasia as a result of severe trauma and financial constraints remains a concern. The identified risk factors and injury patterns can help veterinarians provide more accurate and individualised prognoses, ultimately improving patient care and opening new avenues for future research, such as the importance of preventive measures at home and the role of treatment protocols for initial stabilisation before referral.
Plain language summary
High-rise syndrome refers to injuries that cats suffer when they fall from significant heights, often from the windows or balconies of apartment buildings. Although many cats survive these falls, their injuries can range from mild to severe, and some do not recover. This two-part study examines the factors that influence survival and injury severity, such as the height of the fall, the surface they land on and the cat’s age. Understanding these factors can help veterinarians provide better treatment and more accurate predictions for recovery.
Researchers reviewed medical records and radiographs from 1125 cases of HRS treated at a veterinary hospital in Berlin between 2004 and 2013. All cats fell from a height of at least 4 m (about the second floor or higher of new buildings, or first floor in older buildings). The study analysed age, weight, fall height, landing surface, types of injuries, survival rates and how quickly the cats received medical attention.
Common injuries included circulatory shock (48.6%), head injuries (2.8%), chest trauma (58.3%), broken teeth or jaw injuries (51.1%), abdominal trauma (14.6%), limb fractures (47.2%) and pelvic fractures (11.1%). Most cats survived (87%), but 13.3% either died or were euthanased because of the severity of their injuries. Cats’ age, fall height and landing surface influenced how severe the injuries were.
While most cats survive high-rise falls, many suffer serious injuries, some requiring euthanasia because of trauma severity or financial limitations. This study helps veterinarians better predict which cats are more likely to recover and tailor treatments accordingly. It also highlights the importance of preventive measures, such as window and balcony barriers, to reduce the risk of falls. Early treatment and stabilisation before referral may improve survival outcomes, making timely veterinary care crucial.
Introduction
Feline high-rise syndrome (HRS), a term introduced by Robinson, 1 refers to the group of traumatic injuries suffered by cats falling from balconies or windows two or more floors high. 1 These falls often result in life-threatening trauma, including damage to vital organs and multiple organ systems, individually or in combination.2–5 Despite the potential for severe injuries, many cats survive such incidents, thanks in part to the air-righting reflex, an evolutionary adaptation that allows cats to reorient their bodies mid-air to land on their feet.6,7
Survival after a fall is influenced by numerous factors beyond fall height, such as body orientation during the fall, force distribution, impact surface, limb positioning, velocity at impact, body weight, air resistance and even meteorological conditions.8,9 In addition, the cat’s overall health, including age and bone integrity, plays a crucial role in determining injury severity.8,10 Although the characteristic triad of injuries in HRS includes epistaxis, traumatic cleft palate and pneumothorax, the injury spectrum is broad and may include thoracic, abdominal and spinal trauma, as well as limb fractures and dislocations.11,12 The severity and distribution of injuries in HRS often correlate with fall height; however, conflicting findings in the literature underscore the complexity of these relationships.4,11 Although some studies report a linear increase in injury severity with greater fall height, others suggest more nuanced patterns.4,13 Moreover, previous studies on HRS have been limited by small sample sizes, heterogeneous study designs and regional biases, leaving significant gaps in our understanding of the condition.2,4,14 Compounding these challenges, critical factors, such as the characteristics of the impact surface or time to veterinary presentation, remain underexplored. These limitations hinder the development of robust prognostic models and evidence-based prevention strategies.
Another limitation in the existing literature is the lack of a standardised and universally accepted injury severity scoring system for HRS cases. Although some scoring systems, such as the Animal Trauma Triage Score (ATTS), have been validated as predictive for severity and outcome, they often rely on complex physiological and blood test parameters, limiting their practicality for rapid assessment in clinical settings. 15 In addition, radiological findings – critical for diagnosing traumatic injuries – are not integrated into these scoring models. Given the high prevalence of skeletal and thoracic injuries in HRS cases, incorporating radiographic assessments alongside clinical criteria may improve injury classification and prognostic accuracy.
This second part of the study aims to address these gaps by conducting a comprehensive analysis of a large population of feline HRS cases treated over nearly a decade. The primary objectives are to evaluate the relationships between fall height, injury patterns, severity of injuries and survival rates, while identifying key prognostic factors that influence outcomes. Secondary outcomes include the exploration of associations between other factors (eg, time of year, impact surface, time to veterinary presentation and prior treatment) and injury severity patterns. By systematically analysing these variables, we aim to provide actionable insights that enhance clinical decision-making, improve prognostic accuracy and inform prevention strategies, ultimately advancing veterinary care for cats affected by HRS. We also propose a severity scoring system based on radiological findings and clear clinical parameters, allowing for a practical, reproducible and clinically relevant evaluation of trauma severity in cases of feline HRS.
Materials and methods
This retrospective observational study is a continuation of the analysis of medical records and radiographs of 1125 falls in cats admitted to the Small Animal Clinic at Freie Universität Berlin (Berlin, Germany) between 2004 and 2013 as a result of HRS. The methodology, including case identification, data extraction, inclusion and exclusion criteria, and variables recorded, has been described in detail in the first part of this study.
Briefly, cases were identified using the Vetera practice management system through keyword searches (‘high-rise syndrome (HRS)’, ‘fall’ and ‘Fenstersturz’) and reviewed to confirm eligibility. Data extraction was performed by a single reviewer (AN) using a standardised form. Radiographs were evaluated by a certified radiologist (LB) and experienced clinicians. Injuries were classified in a standardised way based on expert assessment, consistent criteria and in accordance with the guidelines of previous manuals. 16
The following variables were collected for each case: breed, sex (male or female), age groups (<1 year, 1–8 years, >8 years), time of the accident (time of day, day vs night), prior treatment before presentation, time elapsed before presentation to the clinic (<4 h or >4 h), fall height (in metres), impact surface (hard or soft), accompanying circumstances, type, number and severity of injuries, and survival outcome. The collection and classification of these variables are further detailed in the ‘Materials and methods’ section of this study and the first part of the study.
For statistical analysis, cats were classified as light (<4 kg) or heavy (>4 kg) to assess the influence of body weight on injury severity. These categories were chosen to reflect clinical thresholds relevant to body condition scoring and the size variation commonly observed in feline patients.
Fall height
A more detailed explanation of the fall height calculation is provided in the first part of the study. Fall height was initially reported by pet owners in terms of floors, and the corresponding height in metres was then calculated. To improve accuracy in determining fall height, a distinction was made between building types: old or new.
Impact surface
A more extensive explanation regarding the impact surface was provided in the first part of the study. Based on the patient files reviewed, a distinction was drawn between ‘hard’ and ‘soft’ impact surfaces. Surfaces classified as ‘hard’ include concrete, asphalt, stone floors, bicycles, cars, canopies, grilles, railings, fences, garbage cans, chairs, grating and stairs. Surfaces categorised as ‘soft’ comprise awnings, gravel, leaves, sand, bushes, lawns, chairs, sofas and beds.
Radiographic images
Radiographs from the patient medical records were used to validate, grade and, where necessary, supplement or correct findings documented in the clinical records. Standardised imaging protocols were employed for the thorax and abdomen, with laterolateral beam paths capturing individual images. Ventrodorsal views were used for non-dyspnoeic patients, whereas dorsoventral views were taken for dyspnoeic patients. Additional imaging was performed when clinically indicated, including standard orthogonal views (two planes perpendicular to each other) for the skull, spine and limbs.
Type of injuries
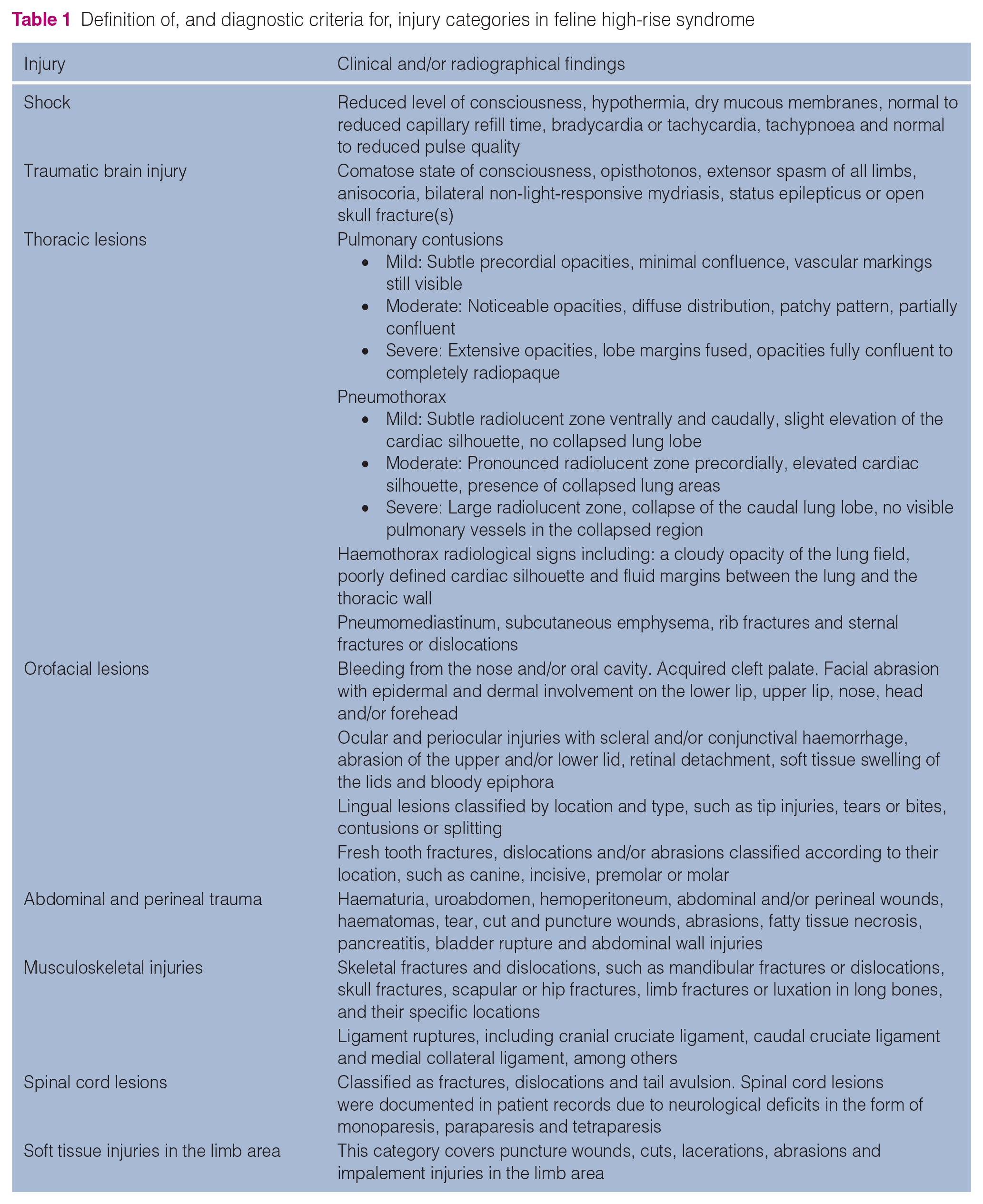
Injuries and/or injury patterns were determined from patient records and all available radiographic images. The complete set of injuries is listed in Table 1.
Definition of, and diagnostic criteria for, injury categories in feline high-rise syndrome
Survival rate
The study examined the outcomes of cats after HRS, categorising them into those that survived the incident, those that died or those that were euthanased, along with the reasons for euthanasia.
Severity of injuries
The injury severity scoring system originally developed by Kolata 11 was adapted to incorporate a radiographic focus and align with our clinic’s clinical protocols, allowing its application retrospectively using radiographs and minimising reliance on physiological parameters that are often absent from medical records (Table 2). Key modifications include detailed descriptions of thoracic injuries, such as pneumothorax, haemothorax and pulmonary contusion, with radiographic findings to standardise assessment and account for respiratory compromise. Specific lesion classifications were expanded to include puncture and impalement injuries, while neurological deficits for skull and vertebral fractures were more clearly defined at higher severity grades. Fracture classifications were refined, distinguishing stable pelvic fractures (grade 1) from complex disruptions like pelvic ring fractures (grade 4). Systemic shock and respiratory failure were explicitly included in grade 4 to address the life-threatening nature of severe injuries.
Modified Kolata scoring system defining injury severity, with newly included clinical and radiographic factors underlined
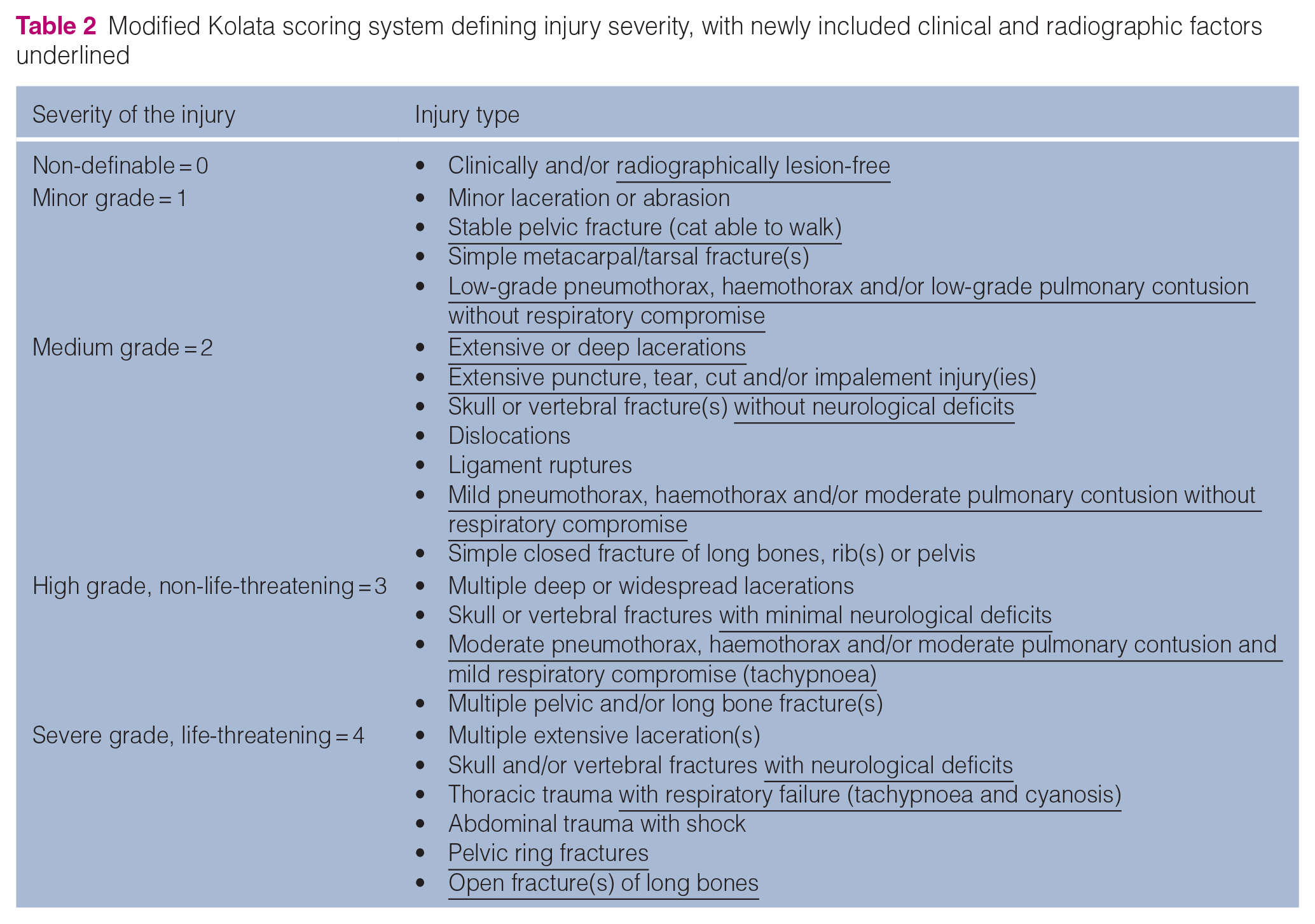
These adaptations enhance the original system by integrating retrospective radiographic data, enabling a more precise evaluation of injury severity and supporting better prognostic modelling and treatment planning.
To classify the severity of injuries, patients were divided into two groups: ‘mildly injured’ (low severity; grades 0 and 1) and ‘severely injured’ (moderate severity; high severity, non-life-threatening; and high severity, life-threatening; grades 2, 3 and 4).
Statistical analysis
Data were analysed using SPSS Statistics software version 23.0 for Windows (IBM). Continuous or ordinal variables based on rating scales such as fall height were summarised as median, mean ± SD. Categorical and ordinal variables were summarised as frequencies and percentages.
The differences between the two groups in terms of severity grade rated on a five-step scale or fall height rated on a seven-step scale were analysed using the Mann–Whitney U-test. In the case of age groups with three categories, the monotonous association with the severity grade was analysed using the Jonckheere–Terpstra test. The relationship between ordinal variables (severity grade rated on a five-step scale and fall height rated on a seven-step scale) was analysed using Spearman’s rank correlation coefficient.
All tests were two-tailed, and a P value <0.05 was considered statistically significant. The logistic regression model was used to analyse the relationship between survival rated on a dichotomous scale and the fall height rated on a seven-step scale.
Results
Patients, time elapsed from fall to presentation and availability of radiographic information
The breed distribution for 1122 falls was recorded, with European Shorthairs being the most represented breed, accounting for 911/1122 (81.2%) cases. The age range of cats was 0.1–20.3 years (mean age 3.68 ± 3.70; median age 2.3). Age data were available for 1085/1125 (96.4%) cases, with 296/1085 (27.3%) aged under 1 year, 645/1085 (59.4%) aged 1–8 years and 144/1085 (13.3%) aged over 8 years.
Weight data were available for 978/1125 (86.6%) cases. Weight was in the range of 1–10 kg (mean weight 4.28 ± 1.43; median weight 4.1). Cats were classified into light (⩽4 kg) and heavy (>4 kg) categories, with 489/974 (50.2%) classified as light and 485/974 (49.8%) as heavy.
Sex information was available for 1112/1125 (98.8%) cases. Among these, 150 (13.5%) were intact males, 451 (40.6%) were castrated males, 267 (24.0%) were intact females and 244 (21.9%) were spayed females.
Time elapsed from fall to presentation was available for 856/1125 (76.1%) cases.
Among the 1125 cases, radiographs were unavailable for 148 (13.2%) cats. Of these, 35 cats either died or were euthanased before radiographs could be taken. A further 30 cats were not radiographed for other reasons. Specifically, 21/30 cats had clinical findings available and nine cats were clinically healthy, with no indications for imaging. In addition, radiographs for 83 cats were taken but were not available in the system for review. The remaining 977/1125 (87%) cases had injuries and/or injury patterns determined from patient records and available radiographs.
Fall height
Among the 1125 cases, the most frequent falls, in descending order, occurred from a height of 8–11 m (348/1125, 30.9%), followed by 12–15 m (288/1125, 25.6%) and 5–7 m (245/1125, 21.8%). There were 137/1125 (12.2%) falls from less than 5 m and 85/1125 (7.6%) falls from 16–21 m.
Falls from greater heights were notably rare, with 14/1125 (1.2%) occurring from 22–24 m, and only 8/1125 (0.7%) from heights exceeding 24 m. Further detailed discussion regarding fall height distribution and its implications is included in the first part of this study.
Impact surface
Information regarding the impact surface was available in the patient records for 227/1125 (20.2%) cases. Among these, 165 (72.7%) cats fell onto hard surfaces or objects, while 62 (27.3%) encountered soft surfaces. Detailed discussion regarding the impact surface and its implications in cats affected by HRS is included in the first part of this study.
Injury patterns
The injuries and injury patterns were documented from patient records and available radiographic images. The most common injuries, along with their frequencies, are presented in Figure 1 and categorised into several types: shock, thoracic lesions, orofacial lesions and musculoskeletal injuries. In addition, less frequent injuries, such as traumatic brain injury, abdominal and perineal trauma, soft tissue injuries in the limb area and spinal cord lesions, were also recorded. A more detailed description of all injuries, including less frequent lesions, is provided in the following section.

Distribution and frequency of the most common injuries in cases of high-rise syndrome (n = 1125)
Shock
Post-traumatic shock was observed in 547/1125 (48.6%) HRS cases.
Thoracic lesions
Thoracic trauma was present in 656/1125 (58.3%) cases. Among these, 466 (71.0%) had a single thoracic lesion, 156 (23.8%) had two lesions, 25 (3.8%) had three lesions, seven (1.1%) had four lesions and two (0.3%) had five lesions.
The most common thoracic lesions observed were as follows: lung contusion (527/1125, 46.8%), pneumothorax (277/1125, 24.6%), subcutaneous emphysema (21/1125, 1.9%), haemothorax (20/1125, 1.8%), pneumomediastinum (16/1125, 1.4%), sternal fracture/dislocation (16/1125, 1.4%), rib fracture (14/1125, 1.2%) and vertebral fracture/dislocation in the thoracic or thoracolumbar transition area (48/1125, 4.3%).
Orofacial lesions
The orofacial area was injured in 575/1125 (51.1%) cases of HRS. Of these, 333 (57.9%) had between two and seven injuries in the head area. The most common orofacial lesions observed were as follows: abrasion wounds (244/1125, 21.7%), epistaxis (208/1125, 18.5%), mouth bleeding (147/1125, 13.1%), teeth injury (147/1125, 13.1%), cleft palate (144/1125, 12.8%), lower jaw fracture (114/1125, 10.1%), tongue lesions (46/1125, 4.1%), periocular area lesions (32/1125, 2.8%) and lower jaw dislocation (11/1125, 1.0%).
Musculoskeletal injuries
The fall affected the musculoskeletal system in 1040/1125 (92.4%) cases, resulting in 899 limb fractures. Hindlimbs were slightly more affected (497/899, 55.3%) than forelimbs (402/899, 44.7%). Among the 531/1040 (51.0%) cases with fractures, single fractures were detected in 322 (60.6%), two fractures in 111 (20.9%) and three fractures in 41 (7.7%). There were 57/531 (10.7%) polyfractured cases. Of the 531 fractures, 102 (19.2%) were open fractures. Of the 152 radial and ulnar fractures, 72 (47.0%) occurred in the diaphyseal region. Distal fractures were observed in 38/152 (25.0%) cases, while proximal fractures were the least common (14/152, 9.0%). Similarly, tibial and fibular fractures were most frequently diaphyseal, found in 75/144 (52.0%) cases. There were 40/144 (28.0%) distal fractures, whereas proximal fractures were rare, occurring in 3/144 (2.0%) cases. Out of the 1125 HRS incidents, humeral fractures were observed in 38 (3.0%), while femoral fractures occurred in 146 (13.0%). Fractures involving the distal area with joint involvement were the most common, accounting for 23/38 (61.0%) humeral fractures and 79/146 (54.0%) femoral fractures. Diaphyseal or proximal fractures were less frequent, accounting for 8/38 (22.0%) humeral fractures and 32/146 (22.0%) femoral fractures. Table 3 and Figure 2 show the frequency of different fractures and affected bones.
Distribution and frequency of musculoskeletal injuries among 1125 cases of high-rise syndrome

Pelvic fractures with more than one bone involved (Ilium, Ischium and Pubis). The fracture area/bone was not applicable for limb ligament rupture

Anatomic distribution of limb fractures in 1125 cases of high-rise syndrome. **Pelvic fractures with more than one bone involved (Ilium, Ischium and Pubis)
Other, less common injuries in cats with HRS
Traumatic brain injury
Of the 1125 cases of HRS, 32 (2.8%) suffered a traumatic brain injury.
Abdominal and perineal trauma
Abdominal trauma was observed in 164/1125 (14.6%) cases of HRS. Of these, 145 (88.4%) suffered monotrauma, while 18 (11.0%) had two abdominal injuries and one (0.6%) had three injuries. Abdominal and perineal injury frequencies are shown in Table 4.
Distribution and frequency of abdominal and perineal injuries and their location in 1125 cases of high-rise syndrome

NA = not applicable
Soft tissue injuries in the limbs
Soft tissue injuries in the limb area were observed in 92/1125 (8.2%) cases, most commonly in the form of abrasion wounds (45/92, 48.9%). The tarsal joint region (16/45, 35.6%) and the ball of the foot (11/45, 24.4%) were particularly affected.
Of the 92 lesions, 14 (15.2%) were lacerations, three (3.2%) were cuts, two (2.2%) were stab wounds and two (2.2%) were impalement injuries. The location or type of lesion could not be identified in 26/92 (28.3%) cases because of missing information in the clinical files.
Spinal cord lesion(s)
Spinal lesions were observed in 48/1125 (4.3%) cases. Among these, 33 (68.8%) had one or more fractured vertebrae, while 15 (31.3%) suffered vertebral dislocations. The majority of dislocations (4/15, 26.7%) occurred in the thoracolumbar junction. After the fall, 26/1125 (2.3%) cases exhibited spinal trauma accompanied by paresis, with 22 (84.6%) presenting with paraparesis and four (15.4%) displaying monoparesis or tetraparesis.
Fall height and injury patterns
Variations in the occurrence of the most frequent injuries were observed across fall heights.
Several injuries, including shock, pulmonary contusion, pneumothorax, haemothorax, lower jaw fractures, haematuria, spinal trauma, femoral fractures, radial and ulnar fractures, carpal and metacarpal fractures, pelvic fractures and tibial/fibular fractures, showed a tendency to increase with fall height.
An exception was noted for head abrasions, which were most frequent in falls from the lowest height group (<5 m) and decreased as fall height increased.
Figure 3 presents the injury patterns in descending order of risk, along with their corresponding fall heights.

Frequency of the most common injuries at different fall heights in cats with high-rise syndrome
Severity of injuries
Injury severity among the 1125 cases of HRS was evaluated as follows (Figure 4):
– 42 (3.7%) cases involved no injury associated with the fall (grade 0);
– 283 (25.2%) cases suffered grade 1 minor injuries, which included abrasion injuries, simple metacarpal and/or metatarsal fractures, and/or low-grade thoracic injury without respiratory impairment;
– 282 (25.1%) cases were classified as grade 2, experiencing medium-severity injuries, such as dislocations, ligament ruptures and/or simple fractures of long bones, ribs and/or the hip;
– 227 (20.2%) cases suffered severe but non-life-threatening injuries, categorised as grade 3, which included thoracic injuries with respiratory insufficiency and multiple pelvic or long bone fractures;
– 291 (25.9%) cases experienced grade 4 life-threatening injuries, including skull and/or vertebral fractures, neurological deficits, thoracic trauma with respiratory insufficiency, abdominal trauma with shock, pelvic ring fractures and open fractures of long bones.
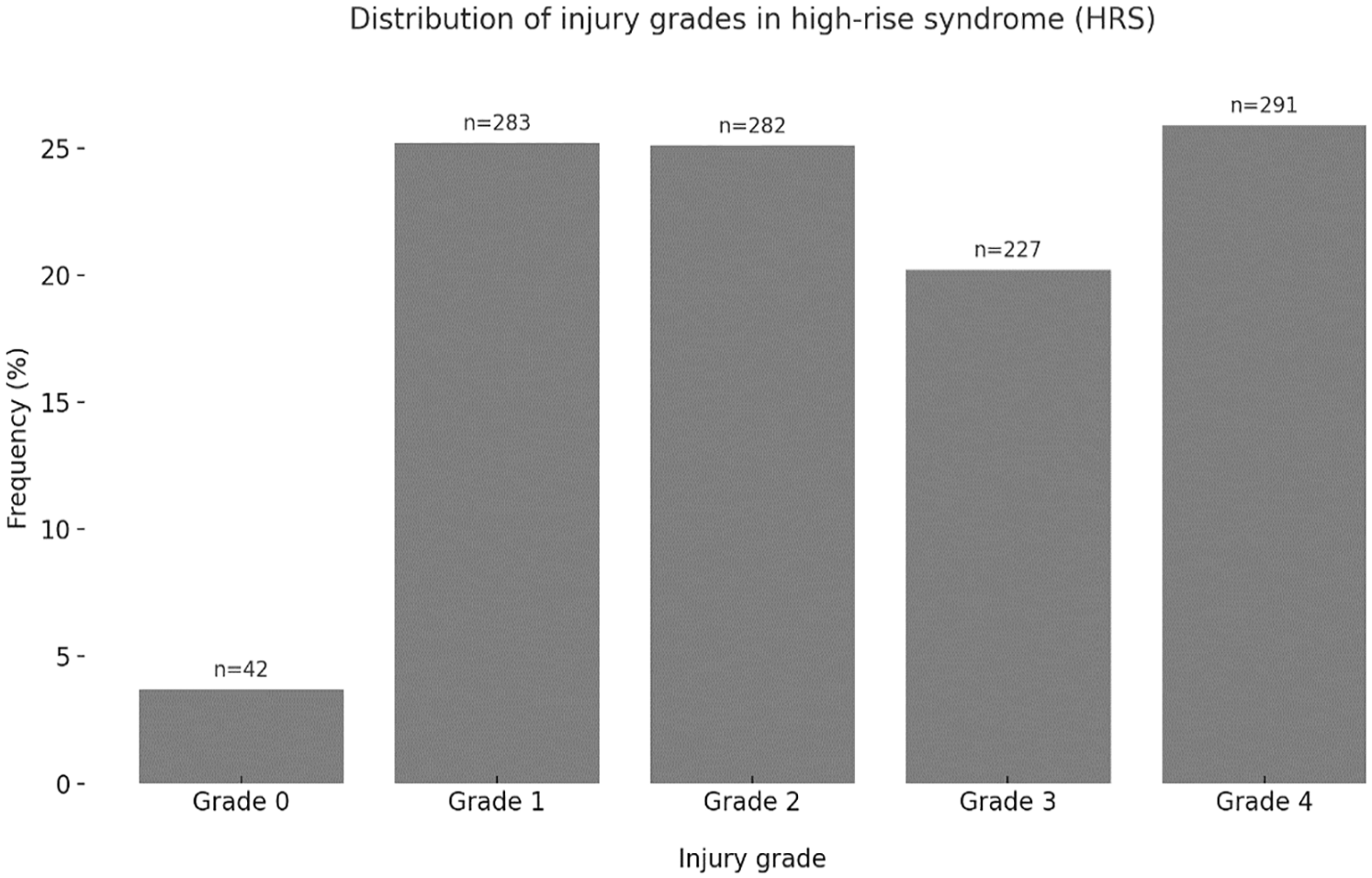
Frequency and distribution of injury severity grades observed in the study (n = 1125)
Severity of injuries and age
Age groups were categorised as follows: among the 1125 cases of HRS, 296 (26.3%) were aged under 1 year, 645 (57.3%) were aged 1–8 years and 144 (12.8%) were aged over 8 years.
A significant association was found between age and injury severity (Jonckheere–Terpstra test, P = 0.019; n = 1085) (Table 5). These findings indicate that cats aged under 1 year experienced less severe injuries compared with those in older age groups.
Summary of statistical analysis for age groups and injury severity (Jonckheere–Terpstra test)

Severity of injuries and gender
The mean injury severity score for all 1125 cases of HRS was 2.39 ± 1.22 (median 2.00).
When analysed by sex, male cats had a mean severity score of 2.35 ± 1.19 (median 2.00; n = 601), while female cats had a mean severity score of 2.44 ± 1.24 (median 2.00; n = 511). The medians of both sexes were nearly equal (2.00), and the Mann–Whitney U-test showed no statistically significant difference (P = 0.183; n = 1112).
Severity of injuries and body weight
The mean injury severity score for all 1125 cases of HRS was 2.39 ± 1.22 (median 2.00). When analysed by weight category, lighter cats had a mean severity of 2.40 ± 1.16 (median 2.00; n = 489), while heavier cats had a mean severity of 2.45 ± 1.19 (median 2.00; n = 485). The Mann–Whitney U-test was used to analyse the relationship between injury severity and body weight, but no statistically significant difference was found (P = 0.549).
Severity of injuries and fall height
The distribution of injury severity across different fall heights revealed a clear trend: as fall height increased, the proportion of severe injuries became more prominent, as shown in Figure 5.

Severity of injuries distribution by fall height in cases of high-rise syndrome (n = 1125)
Among the 137 cats that fell from <5 m, 66 (48.2%) sustained mild injuries, while 71 (51.8%) suffered severe injuries. As the fall height increased, the proportion of mild injuries steadily declined, while severe injuries became predominant.
For falls from 8–11 m, 82/348 (23.6%) cats had mild injuries, whereas 266/348 (76.4%) had severe injuries. This trend continued with falls from 22–24 m, where 13/14 (92.9%) cats sustained severe injuries.
In cases where falls exceeded 24 m, 8/8 (100%) cats had severe injuries, with no recorded cases of mild injuries.
A significant relationship was identified between the severity of injuries and fall height through Spearman’s correlation analysis (Spearman’s correlation ρ = 0.259; P ⩽0.001; n = 1125). This finding indicates a consistent association, suggesting that greater fall height correlates with increased injury severity.
Severity of injuries and impact surface
Details regarding the impact surface were available for 227/1125 (20.2%) cases. The surfaces were categorised as either ‘hard’ or ‘soft’.
The mean injury severity score was 2.02 ± 1.37 (median 1.50; n = 62) for cats landing on soft surfaces and 2.45 ± 1.16 (median 2.00; n = 165) for those landing on hard surfaces. Across all cases (n = 1125), the mean severity score was 2.39 ± 1.22 (median 2.00).
The Mann–Whitney U-test revealed a statistically significant difference in injury severity between the two surface categories (P = 0.016). Among 165 cats landing on hard surfaces, 124 (75.2%) sustained severe injuries, while 41 (24.8%) had mild injuries. In contrast, among 62 cats landing on soft surfaces, 31 (50.0%) suffered severe injuries, while the other 31 (50.0%) had mild injuries.
These findings suggest that landing on a soft surface reduces the likelihood of severe injuries compared with a hard surface.
Survival rate
A total of 975/1125 (86.7%) cases of HRS survived, while 150 (13.3%) either succumbed to their injuries or were euthanased. Among those euthanased, 79 (7.0%) were as a result of severe injuries and a poor prognosis. In addition, 16/1125 (1.4%) were euthanased at the owner’s request, primarily because of high treatment costs. Furthermore, 55/1125 (4.9%) cases died despite receiving veterinary care.
Our findings indicate that survival rates remain above 80% for falls up to 21 m but drop to approximately 60% for falls beyond this height. Logistic regression revealed a significant association between survival rate and fall height (P ⩽0.001; n = 1125). The survival rate declined as fall height increased (Figure 6).

Survival rates by different height falls in cats with high-rise syndrome
Survival rate, time to presentation, prior treatment and shock
Information about time to veterinary presentation was available for 856/1125 cases. Among these, 458 (53.5%) cats presented within 4 h were in shock, compared with 316 (36.9%) of those presented after 4 h.
Prior treatment information was available for all 1125 cases. Among these, 184/441 (41.8%) cats that received prior treatment elsewhere were in shock, whereas 353/684 (51.6%) cats without prior treatment were in shock.
Cats that either received prior treatment elsewhere and/or presented after more than 4 h tended to be less frequently in shock than those that did not receive prior treatment and/or presented within 4 h.
In cases of severe injury, 433/801 (54.1%) cats were in shock, whereas in mild injury cases, shock was observed in only 114/324 (35.1%) cats. In addition, 431/547 (78.8%) cats that experienced shock survived the fall, while the survival rate was 545/579 (94.1%) in cats without shock.
A significant relationship was observed between shock, injury severity and survival rate, as shown in Tables 6 and 7. Cats in shock tended to have more severe injuries and a lower survival rate.
Correlation between shock and severity of injuries

Data are n (%)
Correlation between shock and survival rate

Data are n (%)
Discussion
This study provides a comprehensive analysis of HRS in cats, examining injury patterns, severity and associated factors in a large data set of 1125 cases. Consistent with prior studies, we found that the most commonly affected systems were the musculoskeletal (92%), thoracic (58%) and head (51%).
The overall survival rate (87%), based on analysis of this large data set of feline falls, aligned with previous research and provides new insights into HRS. We found no correlation between body weight and injury severity, indicating that weight alone does not influence trauma outcomes, contradicting previous statements that suggested heavier cats might suffer more severe injuries.17,18 Unlike previous studies2,5 that reported a curvilinear relationship – with injury severity decreasing at extreme heights – or failed to establish a correlation, our findings demonstrate a linear increase in injury severity with greater fall height. In addition, we observed a higher incidence of pulmonary contusions than previously reported, emphasising the significant impact of thoracic trauma in these cases. Finally, younger cats sustained less severe injuries compared with older ones, suggesting potential differences in physiological resilience or impact absorption. These findings contribute to the ongoing discussion of HRS injury patterns and provide a clearer understanding of key risk factors.
HRS is one of the leading causes of traumatic injury in cats, accounting for up to 70% of cases involving various types of injuries, including head, thorax, abdominal, spine and musculoskeletal lesions.17,19–24 According to Kolata, 11 injuries of unknown origin make up 40% of feline traumatic injuries, followed by traffic accidents (16%) and falls (14%). Despite the widespread occurrence of HRS, current understanding of the condition remains limited due to a scarcity of large-scale epidemiological and clinical studies. Although the severity and distribution of injuries are generally associated with fall height, the literature presents conflicting evidence, with some studies indicating a linear relationship and others suggesting more complex patterns.4,11 In addition, many existing studies2,4,14 are limited by smaller sample sizes, inconsistent methodologies and regional biases, further emphasising the need for robust research on large populations to clarify these discrepancies and improve our understanding of HRS.
Our study approach, similar to that of Vnuk et al, 5 involved reviewing radiographic images of the thorax and abdomen in trauma patients whenever possible. We primarily used laterolateral views, supplementing with dorsoventral or ventrodorsal views as necessary. In cases where unstable or fractured areas were suspected, we reviewed extra two-view radiographs when possible. Although we obtained radiographs for many patients, some previous studies performed thoracic imaging on all cats with HRS, regardless of clinical need.2,4 This more comprehensive imaging strategy in other studies often uncovered additional findings unrelated to HRS.
Our analysis of lesions, injury patterns and severity – ranging from no injury to life-threatening conditions – did not reveal a significant correlation with body weight. Although body weight is often considered a key factor in HRS, supporting literature remains limited beyond the findings of Meyer zu Erpen 17 and Warner and Demling. 18 These studies acknowledge that impact energy is influenced by both mass and fall height, but real-world scenarios involve additional variables, such as air resistance, body position and terminal velocity, which limit a purely linear relationship between height and impact energy. Upon landing, kinetic energy converts into static energy, affecting the force experienced at impact. Although theoretical models suggest that a cat falling from the 14th floor experiences greater impact energy than one falling from the second floor, actual energy transfer is influenced by fall dynamics and the cat’s ability to slow its descent.17,18 Despite these biomechanical factors, our study found no significant association between body weight and injury severity, suggesting that other variables – such as impact surface or the air-righting reflex – may play a more critical role in determining injury outcomes. Survival after a fall depends on multiple factors beyond height, including body orientation, force distribution, impact surface, limb positioning, velocity at impact, body weight, air resistance and even meteorological conditions.8,9
The impact surface, whether soft or hard, was documented in only 20% of our patient population. Our observations indicate that cats sustained more severe injuries when landing on harder surfaces, a finding consistent with previous literature.2,4,10,12,18,25 Specifically, 75.2% of cats that landed on hard surfaces suffered severe injuries, showing a significantly higher injury severity compared with those that landed on soft ground (50%).
In our study, cats aged less than 1 year sustained less severe injuries compared with older cats. Similar observations have been made in studies on bite wounds in cats, where older age was associated with increased injury severity and worse outcomes. 26 The higher injury severity in older cats could be due to multiple factors, including pre-existing conditions (eg, osteoarthritis, cardiovascular issues) that may reduce resilience to trauma, reduced physiologic reserves, making recovery from injury more difficult, weakened immune function, increasing susceptibility to secondary complications and lower tissue elasticity and slower healing, contributing to prolonged recovery. In addition, it is possible that older cats experience greater forces upon impact because of biomechanical differences. 26 Younger cats may have greater flexibility, muscle elasticity and a more effective righting reflex, which could help them better absorb the impact of a fall and sustain less severe injuries. Further prospective studies are needed to explore the impact of aging on trauma outcomes in feline patients.
Only 3.7% of the cats in our cohort survived the fall without any injury, which is consistent with the findings of Papazoglou et al, 4 who reported 1.9% of animals were uninjured. Flagstad et al 14 noted a higher percentage of 10%; however, their study included all cats regardless of the height from which they fell.
Shock was diagnosed in almost half (48.6%) of the patients in our study, a percentage lower than reported in some other studies, which was in the range of 58–70%.13,25,27 Conversely, there are studies that have documented lower rates, in the range of 3–24%.2,4,5,14,28 These discrepancies, spanning from 3% to 70%, have no immediate explanation. In our study, 458/856 (53.5%) cats presented to the veterinary clinic within 4 h were in shock, compared with 316/856 (36.9%) presented after 4 h. In addition, cats that received prior treatment had a lower shock rate (184/441, 41.8%) compared with those without prior treatment (353/684, 51.6%). These findings suggest that severely injured cats are brought to the clinic more quickly because of the perceived urgency of their condition. However, time to presentation should not be assumed to be an independent predictor of shock occurrence, as injury severity is likely the primary determining factor. Clinicians should be cautious in attributing worse shock status solely to delayed presentation without considering injury severity.
The observed difference in shock rates between cats that did and did not receive prior treatment may indicate that pretreatment reduces shock occurrence by providing initial stabilisation. However, case selection bias may also play a role, as less severely injured cats may have been more likely to receive initial treatment in smaller practices before referral. In addition, cats from urban areas may be presented more quickly owing to greater clinic availability, potentially allowing for early stabilisation and reducing shock prevalence compared with those examined more than 4 h after trauma. Conversely, cats that succumbed to injuries or shock shortly after the fall may not have been presented for care, leading to their exclusion from the data set.
Future studies should take injury severity into account when evaluating the effect of prior treatment on shock to ensure accurate results. In our study, we were unable to directly evaluate the severity of injuries in externally treated cases, as referring veterinarians did not provide this information. This highlights the need for standardised data collection across clinical settings to improve the assessment of pretreatment effectiveness.
Furthermore, shock was significantly associated with both injury severity and survival rate, as indicated by our statistical analysis. This suggests that shock is not merely a secondary consequence of severe injuries but also a risk factor for mortality. Early and aggressive shock therapy is therefore essential, as it may have a direct impact on survival outcomes.
Blunt thoracic trauma is a common consequence of falls, with incidence rates ranging widely from 13–90%.2,13,14 In our study, nearly 60% of the cats exhibited thoracic lesions. Notably, clinical signs often do not align with radiographic findings, emphasising the importance of routine chest radiography in cases of HRS. The most frequently observed injuries in our cohort included lung contusion (46.8%), pneumothorax (24.6%) and subcutaneous emphysema (1.9%). Although single thoracic injuries were predominant, approximately 29% of cases presented with multiple lesions. Meyer zu Erpen 17 reported multiple thoracic lesions in 75% of HRS cases, primarily pneumothorax, which is consistent with findings from other authors.5,25 In contrast to these studies, our findings indicated a higher prevalence of pulmonary contusions. The time between the accident and presentation at the clinic may influence these results. For instance, in Munich, 17 the clinic is centrally located, whereas in Berlin it may take longer for patients to reach a hospital. This delay may allow air (pneumothorax) to be absorbed more rapidly than fluid (haemothorax or lung contusion). Nevertheless, our standard practice of performing chest radiographs in two planes likely reduces the risk of missing lesions, which may explain the higher detection rate of pulmonary contusions in our study.
Head injuries were present in 51.1% of patients in this study, aligning closely with previous research reporting incidences in the range of 56–66%.2,29 However, lower percentages, in the range of 5–32%, have been reported in other studies.4,5,13,14,27,28 Bonner et al 29 suggested that discrepancies may arise from underestimating certain injuries, such as tooth fractures or skin lesions, and bleeding without recognisable wounds, which are inconsistently recorded in the literature. Blunt abdominal trauma involves injuries resulting from blunt force to the abdominal cavity, affecting various structures, such as the abdominal wall, diaphragm and organs like the liver, spleen and urinary tract. Brunnberg et al 23 found that the most commonly injured abdominal structures in cats were the diaphragm and abdominal wall, with the urinary tract being the most frequently affected organ. The causes of blunt abdominal trauma in that study varied, including unknown factors, car accidents and HRS. In this study of 1125 cases of HRS in cats, 15% suffered blunt abdominal trauma, similar to the results obtained by other authors.2,13,27,28
The most common intra-abdominal injuries in our patient population were urinary tract injuries, observed in 93/1125 (8.3%) cases, with haematuria being the cardinal sign (7.5%). Ruptured urinary tract organs and uroabdomen were rare, occurring in only nine (0.8%) cats. These findings are consistent with those of previous studies,2,5,13,14,27 although Barth 25 reported a higher frequency of 40.1% for urinary tract injuries. Incidence rates of urinary bladder rupture during HRS are very low, in the range of 0.2–2.3% in the literature.1,2,4,5,13,27,28,30 Similarly, renal lesions are infrequently described, and traumatic pancreatitis affected 1.3% of the cats in our study, aligning with previous findings.13,27,30–32 Injuries to gastrointestinal tract organs, liver and spleen are also rare in cases of HRS. Lettow et al 30 reported low rates of liver and spleen ruptures, at 0.6% and 0.4%, respectively. Injuries to the uterus, stomach and intestines were infrequently observed as well. 28 Buriko 9 concluded that the presence of abdominal trauma in feline HRS indicates a more severe injury and serves as a negative prognostic indicator. This emphasises the critical need for prompt intervention, as the prolonged time between the accident and presentation in 40% of cases suggests that severe abdominal injuries may lead to fatalities before reaching veterinary care.
Guided by the air-righting reflex, kinetic energy from a fall is absorbed rapidly by the forelimbs and then gradually by the hindlimbs. This energy is transmitted dorsally through the limb segments and eventually converted into static energy within the skeletal structure via the paws, zeugopodium (distal limb) and stylopodium (proximal limb), contributing to the overall stability of the limbs. In the forelimb, the residual energy is dispersed within the flexible shoulder joint, enabling extensive mobility and adjustment of the scapula relative to the thoracic spine. 7 Consequently, scapular and proximal humeral fractures were infrequently observed. In contrast, in the hindlimb, the residual energy impacts the largely immobile pelvis, particularly at the sacroiliac joint, which cannot absorb the force. Sacroiliac joint dislocations and pelvic fractures were relatively frequent, often due to tears in the sacroiliac dorsal ligaments. 7
During impact, the carpal and tarsal joints experience dorsal flexion, which maximises palmar and plantar hyperextension. The carpal joints exhibit a greater range of motion compared with the tarsal joints, leading to a higher incidence of ligament ruptures and metacarpal bone fractures. 7 Our study found 44 hyperextension lesions but only one fracture, suggesting that compensation in the carpal joint can mitigate fracture risk. Metacarpal bone fractures may occur more frequently because of their dorsal convex curvature. In contrast, fractures in the distal radius and ulna are rarely observed proximal to the carpal joint. In total, HRS in our patient population accounted for 271 carpal joint areas injured, while only 152 tarsal joint areas were affected. The number of distal tibial/fibular fractures was recorded at 41, whereas rear metatarsal fractures occurred five times less frequently than metacarpal fractures. Interestingly, tarsal joint injuries occurred almost twice as often as carpal joint injuries. Although the ankle joint is less prone to tearing, the ligaments of the tarsocrural joint are more susceptible to injury. The bones of the ankle joint, particularly the talus and calcaneus, are at high risk of fracture because of their limited range of motion and interlocking structure. This indicates that the destructive energy from falls significantly impacts these joint bones; consequently, distal and proximal bone fractures in the ankle joint are quite rare.
Most radial and ulnar fractures occurred in the diaphyseal region (72/152, 47.0%), while tibial and fibular fractures were also predominantly diaphyseal (75/144, 52.0%). Distal fractures were less frequent, and proximal fractures were rare across all bones. The convex shape of the radius and ulna and the side profile of the tibia may influence fracture patterns, with excessive stress during impact exceeding load tolerance and leading to fractures caused by shearing, bending and torsional forces. Among humeral (38/1125, 3.0%) and femoral fractures (146/1125, 13.0%), distal fractures with joint involvement were the most common (humerus, 61.0%; femur, 54.0%), while diaphyseal and proximal fractures were less frequent. The higher prevalence of femoral fractures may result from impact forces being absorbed by the hindlimbs during landing. Femoral luxations were rare (24/1125, 2.0%), suggesting inherent hip joint stability. These findings emphasise the need for thorough radiographic assessments, particularly of the hindlimbs, where fractures are more frequent in HRS cases.
In our study, the injury severity score increased consistently with fall height, showing a linear correlation rather than a curvilinear pattern. This contrasts with previous research that reported a curvilinear relationship,2,4,14 suggesting that injury severity decreases at extreme heights. Vnuk et al 5 did not observe a clear pattern, while Dupre et al 13 found a linear increase in injury severity, aligning more closely with our findings. The literature presents contradictory results regarding the relationship between fall height and injury severity, highlighting the need for the present investigation. Given this inconsistency, our study contributes valuable new data by analysing a large data set, offering a more comprehensive understanding of injury patterns in HRS.
Our analysis highlights significant risks of injury associated with HRS, particularly musculoskeletal injuries (92%), thoracic injuries (58%), head injuries (51%) and shock (49%). These results agree with earlier literature.13,27 Numerous studies suggest that up to 60% of patients experience injuries across multiple organ systems simultaneously. Common injury combinations include the ‘unhappy triad’ of epistaxis, cleft palate and pneumothorax, 1 as well as limb fracture, epistaxis, cleft palate and shock. 5 In our study, shock with pulmonary contusion was the most common injury combination. In some studies, fall height has been shown to correlate linearly, with the number of injuries increasing as the height rises.2,4,14 However, our findings suggest that this pattern is more complex, varying depending on the type of injury. Some injuries increase in a linear fashion, while others follow a curve-like distribution or even decrease at higher falls. For instance, orofacial injuries were more frequently observed at lower heights but decreased with increasing fall height. In contrast, injuries such as spinal trauma and shock exhibited a linear increase with height. At certain thresholds, the number of injuries plateaus or follows a non-linear trajectory, indicating a more complex injury mechanism beyond simple height-dependent forces. The air-righting reflex plays a crucial role in avoiding trauma, directing kinetic energy dorsally and causing injury to various parts of the body. 7 Failure to develop this reflex may result from inexperience in younger cats or from external factors, such as collisions with bushes or trees.
In contrast to some studies,4,13 our findings suggest that the frequency of spinal cord injuries and fractures increases at higher fall heights. Falls from heights of 12–20 m were associated with an increased frequency of fractures. Interestingly, some studies have reported that falls from heights exceeding 20 m may result in fewer fractures, possibly due to increased air resistance and the dissipation of impact energy.2,4,14 However, thoracic trauma remains a significant concern in these cases.
Of the 1125 cases of HRS, a total of 975 (87%) cats survived the fall. Our findings indicate that survival rates remain above 80% for falls up to 21 m but drop to approximately 60% for falls beyond this height. This suggests a critical threshold, where survival remains relatively high at moderate heights but declines significantly with extreme falls. A significant association between fall height and survival rate – indicating that survival decreases as fall height increases – is in line with previous studies.5,33 However, 150/1125 (13.3%) cats died from polytrauma, and factors such as poor prognosis and economic constraints contributed to euthanasia decisions. The literature indicates comparable and slightly higher survival rates in the range of 83–92%.2,4,5,13,15,24,25,29,33 However, unreported cases of feline deaths may be significantly underrepresented, as cat ownership in Germany is tax-exempt and does not require official documentation – such as a death or euthanasia certificate – for reporting the animal’s death. In our study, immediate deaths accounted for 55/150 (36.6%) cases of non-survival, similar to previous research,2,5 while Bonner et al 29 reported no deaths after HRS. According to the literature, euthanasia due to economic constraints and poor prognosis occurs in a significant proportion (36–60%) of cases.2,5,29
This study has several limitations that warrant acknowledgement. One key limitation is the use of a modified injury scoring system, the Kolata classification, 11 which has not been formally validated. This system was chosen because it relies on diagnostic criteria visible on radiographs, which were consistently available in our retrospective data set. In contrast, more recent and validated scoring systems, such as the ATTS 15 and the Modified Glasgow Coma Scale, 34 provide more comprehensive assessments but require detailed physiological and laboratory data that were not recorded in the medical files used for this study. This reliance on radiographic findings, while practical for our data set, underscores a common limitation of retrospective studies and highlights the need for further validation of this adapted scoring system.
To address some of these limitations, we sought to enhance the Kolata classification by incorporating additional criteria derived from radiographic findings. These modifications aimed to improve the system’s applicability to retrospective cases and provide a more nuanced assessment of injury patterns. However, the lack of external validation for these adaptations remains a constraint, and further studies are needed to evaluate their accuracy and reliability.
This study’s retrospective nature introduces inherent limitations, including reliance on pre-existing medical records that varied in data quality and completeness. Missing information in key areas, such as impact surface or fall height, may have influenced the results and reduced statistical power. Selection bias is also a concern, as the study included only cases presented to veterinary clinics, excluding animals that died at the scene or were not brought for care. In addition, the findings may have limited generalisability because of the focus on a specific population and region. Another notable limitation is the absence of information in the medical records regarding preventive measures, such as protective barriers or environmental modifications. Although previous literature 35 suggests these measures reduce the likelihood or severity of injuries, the lack of recorded data prevents a direct assessment of their impact in our cases. These factors underscore the need for prospective studies to confirm and expand upon these findings, as well as to evaluate the role of preventive and owner education strategies in mitigating injuries from HRS.
The early diagnosis of HRS injuries poses difficulties, highlighting the need for a thorough anamnesis, including consideration of factors such as age, fall height and impact surface to assess the severity of the injury. This study highlights the importance of routine radiographic imaging in diagnosing and managing HRS in cats, particularly for detecting thoracic and musculoskeletal injuries that may not be immediately evident. It also emphasises the need for standardised diagnostic protocols and scoring systems tailored to available resources, even in retrospective settings.
Triage should be based on injury severity and shock status to ensure appropriate prioritisation of care. Future studies should reassess the role of prior treatment by considering injury severity at the site of initial care. A standardised pretreatment protocol for initial stabilisation before referral could be beneficial in improving patient outcomes. Shock is a significant predictor of survival, emphasising the importance of early recognition and intervention. Future studies should include case-control comparisons with similar injury severity to accurately determine the impact of presentation time and initial treatment on shock occurrence. Such research could help develop clinical protocols for both primary care veterinarians and referral clinics, optimising the management of trauma patients.
The literature 35 suggests that preventive measures, such as protective barriers and owner education, are effective in reducing HRS incidence and severity. However, the lack of systematic documentation of these measures in our study highlights the need for greater emphasis on prevention and awareness.
Future research should use validated scoring systems, explore biomechanical and environmental factors influencing injury patterns, and evaluate long-term outcomes and the effectiveness of preventive strategies to improve feline welfare and clinical outcomes.
Conclusions
By observing the lesion patterns in this substantial data set of 1125 cases of HRS, this study provides valuable insights that can inform the development of future protocols for diagnosing, treating and managing HRS. The findings emphasise the importance of routine radiographic imaging to identify injury patterns and severity, which could contribute to the creation of evidence-based prognostic tools tailored to HRS cases.
In addition, this study highlights the significant influence of age, fall height and impact surface on injury severity and outcomes. Understanding these key factors is crucial for improving clinical decision-making, risk assessment and preventive strategies in feline HRS cases.
This study highlights the need for validated scoring systems and further research to improve diagnostic and prognostic strategies. Future studies should reassess the role of pretreatment by considering injury severity at the site of initial care. Implementing a standardised pretreatment protocol for initial stabilisation before referral could enhance patient outcomes. In addition, evaluating preventive measures and educational strategies for owners may help reduce the incidence and severity of HRS. Addressing these gaps will enable veterinarians to optimise patient care and advance feline health and welfare in urban environments.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received external funding from the Health and Medical University, Potsdam, to cover publication costs. No specific grant number was assigned.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.