
Abstract
Objectives
The purpose of this study was to prospectively evaluate the prognostic utility of the Animal Trauma Triage Score (ATTS) and Modified Glasgow Coma Scale (MGCS) in cats with high-rise syndrome.
Methods
ATTS and MGCS were obtained upon arrival from 25 client-owned cats presented for high-rise syndrome. Cases were followed during hospitalisation and several variables, including outcome, were recorded.
Results
The mortality rate in this cohort of cats with high-rise syndrome was 16%. Univariate statistical analysis showed that lactate (P = 0.022), creatinine (P = 0.01), body weight (P = 0.036) and ATTS (P = 0.02) were higher and MGCS (P = 0.011) lower among non-survivors. Multivariable statistical analysis showed that ATTS was the only factor significantly associated with mortality (odds ratio 2.41, 95% confidence interval [CI] 1.02–5.71; P = 0.046). A receiver operating characteristics curve showed that ATTS was an excellent predictor of mortality (area under the curve 0.917, 95% CI 0.8–1.0; P = 0.009). An ATTS cut-off of 6.0 had a 75% sensitivity and 90% specificity for non-survival and a cut-off of 10 had a 25% sensitivity and 100% specificity for non-survival.
Conclusions and relevance
ATTS is predictive of severity and outcome in cats with high-rise syndrome and can help facilitate decision-making by owners and veterinarians.
Introduction
The Animal Trauma Triage Score (ATTS) is an injury severity grading scale that was developed in the 1990s to classify traumatised patients. 1 The score is calculated using physical examination findings from six body systems: perfusion, cardiac, respiratory, eye/muscle/integument, skeletal and neurological. Its initial validation showed that each point increase in ATTS was associated with a 2.3–2.6 times decreased chance of survival. 1 A recent multicentre study showed that an ATTS ⩾5 had an 83% sensitivity and 91% specificity in predicting mortality in dogs suffering from trauma. 2 Since the score was developed, multiple prospective and retrospective studies have shown its utility in different populations of dogs suffering from trauma.3–7 ATTS is a useful predictor of surgery requirement, blood product requirement, length of hospitalisation and likelihood of survival in dogs.3–7 Similarly to dogs, ATTS at admission has been associated with survival to discharge in cats.8–13 However, most studies have been retrospective and there is a lack of prospective studies evaluating ATTS in cats with trauma.
Traumatic brain injury (TBI) is a common condition in veterinary medicine,14,15 and severe brain injury is associated with high mortality in animals.1,15,16 The Modified Glasgow Coma Scale (MGCS) is an illness severity score that has been validated in dogs and cats with TBI.9,10,17 The score is calculated evaluating motor activity, brainstem reflexes and level of consciousness, and a score up to 18 is given. Higher scores reflect better neurological function and are associated with a higher survival rate. 17
High-rise syndrome refers to the traumatic lesions produced by falling from balconies or windows of high-rise buildings in urban areas. 18 Retrospective studies of cats with high-rise syndrome have previously reported that thoracic trauma occurs in 90% of cases, abdominal injuries in 7% of cases and survival rates reported up to 97%.18,19 A study of high-rise syndrome in dogs showed that the height of the fall and the type of landing surface affected the severity of the injuries, with dogs falling from a height of less than three floors having more limb fractures and those with higher falls having more spinal injuries. 20
To our knowledge there are have been no previous studies evaluating ATTS or MGCS in cats with high-rise syndrome. The aim of this study was to evaluate the prognostic utility of both scores in cats suffering from high-rise syndrome. A secondary objective was to evaluate other predictors of mortality such as age, weight, body condition score (BCS), height of fall, blood product requirement, vasopressor requirement, systolic blood pressure (SBP) and bloodwork results. We hypothesised that both scores (MGCS and ATTS) would predict outcome in cats with high-rise syndrome with acceptable sensitivity and specificity.
Materials and methods
Case selection
Cats were prospectively recruited for this study between July 2018 and December 2020. Owner consent was not required for the participation in the study. To be included in the study cats had to be diagnosed with high-rise syndrome within a 24 h interval since the fall. Cats were excluded if they received any treatment prior to the evaluation of ATTS and MGCS. The assessment of both scales and the inclusion of the case was performed by either a house officer or an emergency and critical care board-certified specialist present at the time of admission. Recorded variables in all cats were age, breed, sex, weight, BCS (from 1 to 9), height of fall (number of floors), MGCS and ATTS at admission, mortality and length of hospital stay. Venous blood gas parameters, creatinine, packed cell volume (PCV), total solids (TS), electrolyte panel and SBP were recorded at admission when available. All samples were analysed immediately. Venous blood gas parameters were obtained with the epoc Blood Analysis System (Siemens). SBP was determined using the Doppler method. Other data recorded in all cats were blood product administration (packed red blood cells [pRBC] or fresh frozen plasma [FFP]), vasopressor use and surgery requirement, which was classified as orthopaedic, soft tissue or both. Our criterion for the administration of FFP was the presence of a coagulopathy with prolongation of clotting times above 25% of the upper reference interval paired with clinical suspicion of bleeding. Vasopressors were used in the face of hypotension despite appropriate fluid resuscitation.
Statistical analysis
Statistical analysis was performed using a commercially available computer program (IBM SPSS statistics version 23). Data normality was assessed with histograms and the Shapiro–Wilk test. Normally distributed data were expressed as mean ± SD and non-normally distributed data were expressed as median and range. Categorical data were expressed as frequencies and percentages. Univariable statistical analysis was performed using the Student’s t-test, Mann–Whitney U-test or Fisher’s exact test as appropriate to compare variables between survivors and non-survivors. A Spearman’s correlation coefficient was calculated to evaluate a possible relationship between higher height of fall and higher respiratory scores of the ATTS. Multivariable statistical analysis was performed using logistic regression. Data included in the multivariable model were age, breed, sex, weight, BCS, height of fall, MGCS and ATTS at admission, length of hospital stay, blood product administration, vasopressor use and surgery requirement. For all comparisons, P values <0.05 were considered statistically significant. Receiver operating characteristic (ROC) curves were generated posteriorly for any statistically significant predictors of mortality.
Results
Twenty-five cats were enrolled during the study period. The median age was 11 months (range 3–102). Ten of 25 (40%) cats were entire males, 6/25 (24%) spayed females, 5/25 (20%) castrated males and 4/25 (16%) entire females. Twenty cats (80%) were domestic shorthair, 2/25 (8%) were Siamese, 1/25 (4%) was Bengal, 1/25 (4%) was Sphynx and 1/25 (4%) was Persian. Mean weight was 3.86 ± 1.47 kg and median BCS was 4 (range 3–9). Mean height of the fall was 4 ± 2 floors (range 1–7). Median MGCS was 18 (range 10–18). Mean ATTS was 4 ± 2 (see Table 1 in the supplementary material for the demographic variables, height of fall, survival and specific ATTS and MGCS for each case). Venous blood gases, creatinine, lactate and SBP were obtained in 20 cases and PCV/TS in 19 cases. Bloodwork results are summarised in Table 1. Univariate analysis showed that lactate (P = 0.022) and creatinine (P = 0.01) were significantly higher among non-survivors.
Comparison of blood test results and blood pressure between survivors and non-survivors of high-rise syndrome

Results are expressed as mean ± SD or median (range)
RI = reference interval; PvCO2 = partial pressure of venous carbon dioxide; HCO3– = bicarbonate; PCV = packed cell volume; TS = total solids; SBP = systolic blood pressure
Cats were hospitalised for a mean of 4 ± 2 days. One of 25 cats (4%) required an FFP transfusion; the same cat required vasopressor therapy (noradrenaline [norepinephrine]). This cat had coagulation tests performed because it deteriorated following admission. This cat was euthanased. No cat required a pRBC transfusion. Nine of 25 cats (36%) required surgery; eight of these underwent orthopaedic surgery (repair of appendicular bone fractures), and one cat (4%) had orthopaedic and soft tissue surgery (enucleation of an eye and appendicular bone fracture repair). Four of 25 (16%) cats did not survive to discharge. Euthanasia was the most prevalent cause of death: three cats (12%) were euthanased, and one (4%) suffered natural death. Length of hospitalisation was not statistically significant between survivors and non-survivors (P = 0.181). Univariate statistical analysis of illness severity scores, demographic variables and treatments is given in Table 2. Cats with higher ATTS (P = 0.02), higher body weight (P = 0.036) and lower MGCS (P = 0.011) were more likely to die. There was no statistically significant correlation between height of fall and ATTS respiratory scores (P = 0.546). Logistic regression was posteriorly performed to compare the multivariable model between survivors and non-survivors. The three statistically significant variables included in the model were ATTS, MGCS and body weight. Finally, the only significant equation variable was ATTS (P = 0.046). Cats with higher ATTS were less likely to survive (odds ratio 2.41, 95% confidence interval [CI] 1.02–5.71). A ROC curve was performed to evaluate the sensitivity and specificity of ATTS in relation with non-survival (Figure 1). The ROC curve showed that ATTS is an outstanding predictor of mortality (area under the curve [AUC] 0.917, 95% CI 0.8–1.0; P = 0.009). An ATTS cut-off of 6 had a 75% of sensitivity and 90% of specificity for non-survival, and a cut-off of 10 had an 25% of sensitivity and 100% of specificity for non-survival. Despite the lack of statistical significance of MGCS in the multivariable model, 2/3 cats with an MGCS of ⩽10 did not survive.
Univariate statistical analysis of illness severity scores, demographic variables and treatments in 25 cats with high-rise syndrome
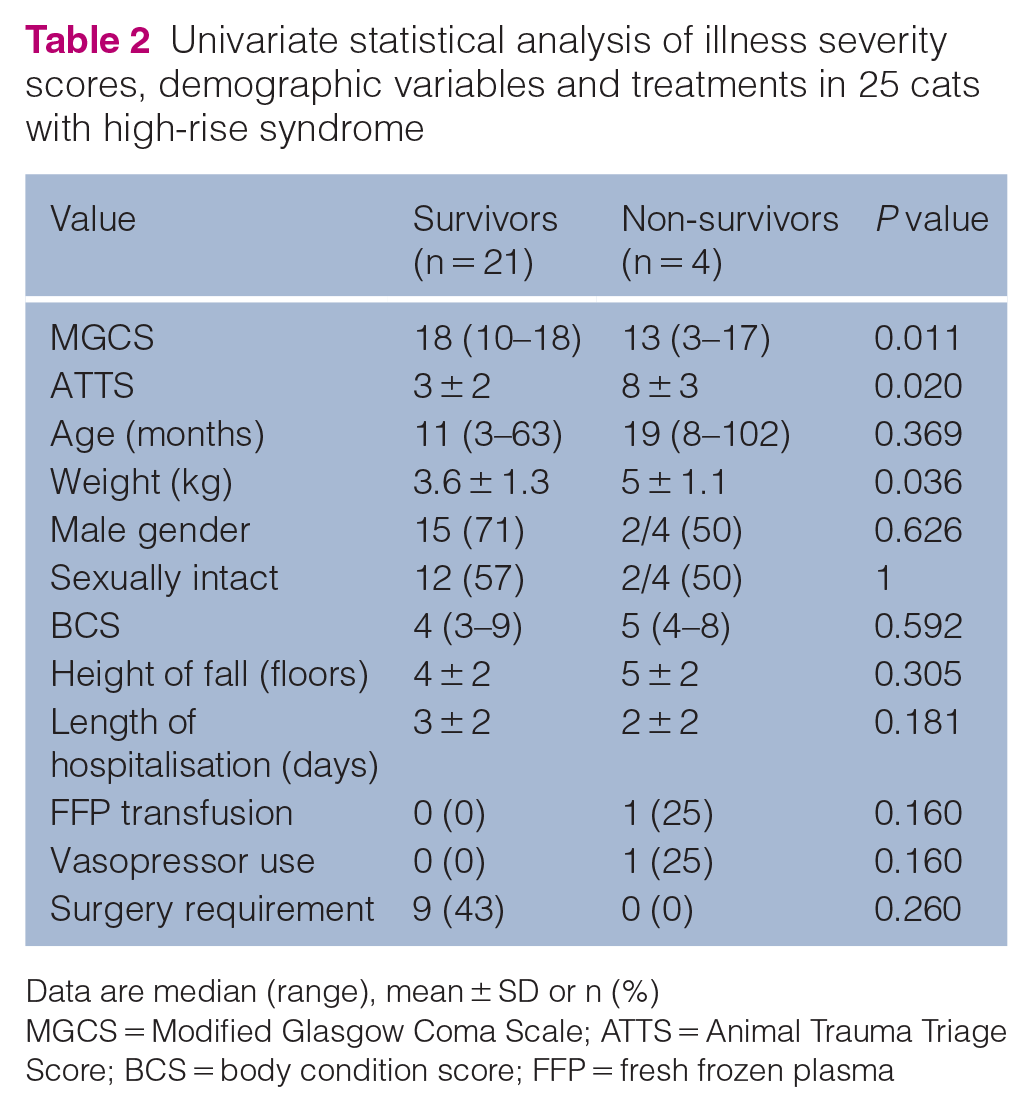
Data are median (range), mean ± SD or n (%)
MGCS = Modified Glasgow Coma Scale; ATTS = Animal Trauma Triage Score; BCS = body condition score; FFP = fresh frozen plasma

Receiver operating characteristic curve was constructed by plotting the sensitivity, also called true positive rate, against 1-specificity, also called the false-positive rate. It shows the trade-off between sensitivity and specificity. Parameters that give curves closer to the top-left corner indicate a better performance, which is numerically expressed as the area under the curve (AUC). The AUC is 0.917, which makes the Animal Trauma Triage Score an outstanding predictor of mortality
Discussion
This study has shown that cats with higher ATTS owing to trauma from high-rise syndrome have higher odds of death. This score has been extensively studied in various traumatic conditions in dogs, but the number of studies evaluating ATTS in cats is small.1–13 To our knowledge, this is the first study to evaluate ATTS and its relationship with mortality in cats with high-rise syndrome. The ROC curve showed that ATTS is an outstanding predictor of mortality (AUC 0.917, 95% CI 0.8–1.0; P = 0.009). An ATTS cut-off of 6 had a 75% of sensitivity and 90% of specificity for non-survival, and a cut-off of 10 had an 25% of sensitivity and 100% of specificity for non-survival. Our results showed that ATTS is a valuable predictor of mortality in cats with high-rise syndrome, similarly to other causes of polytrauma in dogs and cats .1,2,5,6,8,9,11,21,22
Other variables such as MGCS or body weight were statistically significant between survivors and non-survivors in the univariable analysis, but the only significant variable in the multivariable analysis was ATTS. In previous studies, MGCS was found to be a valuable prognosis parameter in dogs and cats with TBI.16,17,23 In our study, only 16% (4/25) of cats had signs compatible with TBI. The relatively low incidence of TBI in this cohort of cats might explain why this score was only statistically significant in the univariable analysis and not in the multivariable model. The fact that cats with higher body weight showed increased mortality in the univariate statistical analysis could be because heavier cats may be less agile and hence less likely to fall appropriately. Another possible explanation might be the higher impact force that a heavier cat will create against the landing surface. It should be noted that whereas body weight was statistically significant between survivors and non-survivors in the univariable analysis, BCS was not. To some extent, this discrepancy could be explained by the relative subjectivity assessing BCS evaluation by different observers.
Plasma lactate was significantly higher in non-survivors in our study. This result is in line with previous studies in dogs and cats with polytrauma.2,8,11 Creatinine was another significant predictor of mortality in univariate analysis. In our study, 2/4 (50%) non-survivors and 1/21 (5%) survivors showed mild azotaemia. Other studies have not found this to be a significant predictor of death. The reason for this finding could be a type 1 statistical error (significant difference found by chance) or it could be due to azotaemic patients having a worse degree of shock and hence higher mortality.
Four cats in the present study were hypotensive on presentation and half of them did not survive to discharge. Admission blood pressure was lower in non-survivors, but this result was not statistically significant in the univariate analysis (P = 0.08). A study that evaluated ATTS in cats suffering from vehicular trauma found that higher ATTS was associated with lower blood pressure measurements. 11 The same study found that there was a significant association between lower PCV, lower total plasma protein concentration, lower venous blood pH, higher plasma lactate concentration, lower plasma bicarbonate concentration, lower base excess and higher whole-blood glucose concentration with higher ATTS. 11 Another study evaluated ATTS in cats with bite wound trauma and found that there were significant associations between higher ATTS and low venous blood pH, high plasma lactate and low ionised calcium.8
In agreement with previous studies, our results showed that high-rise syndrome is seen mostly in young cats.18,19,24–26 The median age of this cohort of cats was 11 months (range 3–102). It is possible that younger cats tend to have more falls as they have less experience and more curiosity. However, the height of fall was not statistically significant between survivors and non-survivors (P = 0.305), and there was no significant correlation between the height of the fall and respiratory scores (P = 0.546). This lack of difference and correlation could be because only 24% (6/25) of cats fell from more than the fifth floor. A previous study concluded that falls from floors seven or higher are associated with more severe injuries and thoracic trauma. 18 Another study found that respiratory system injuries were significantly associated with higher falls (floors 3–6), and that survival was negatively associated with the height of the fall. 27
Our study had a mortality rate of 16%. This rate is similar to previous studies in cats with high-rise trauma, which reported mortality rates ranging from 3% to 17%18,19,23,25,27,28
Some limitations must be recognised when interpreting the results of this study. First, although the incidence of high-rise syndrome in our area is relatively high our study does not have many cases. A higher sample size may have shown significant differences between groups in MGCS or other parameters. Secondly, as previously discussed, bloodwork and blood pressure were not measured in all cats, and, if measured, could have provided valuable information. Thirdly, having a low number of non-survivors could decrease the probability of finding other significant predictors of mortality. Fourthly, time from trauma until hospital admission was not recorded and patients were recruited during the first 24 h following trauma. This timeline could potentially change the outcome. Finally, this was a single centre study. A multicentric study could provide a broader picture of high-rise syndrome in cats.
Conclusions
The current study has shown that high-rise syndrome in cats has a low mortality rate (16%) and that ATTS could be a useful prognostic tool due to the significant association between higher ATTS at admission and mortality in this specific population of cats. ROC curve analysis showed that the ATTS was an excellent predictor of mortality. Additionally, higher plasma lactate, creatinine and body weight, and lower MGCS at admission, were significantly associated with mortality in univariable analysis.
Supplemental Material
Table 1:
Demographic variables, height of fall, ATTS, MGCS and survival from 25 cats with high-rise syndrome.
Footnotes
Supplementary material
The following file is available online:
Table 1: Demographic variables, height of fall, ATTS, MGCS and survival from 25 cats with high-rise syndrome.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.