
Abstract
Background and purposes:
Evidence regarding patients’ perception of fall risk is scarce. This study aimed to investigate the current situation and the associated factors of patients’ perception of fall risk, explore the mechanisms, and identify the subgroup of patients who may be at greater risk of having an erroneous perception.
Methods:
Participants were recruited from three wards of two tertiary general hospitals in China. Three-step multiple linear regression analyses were conducted including the demographic characteristics, health status factors, and fall-related factors as independent variables and Fall Risk Perception Questionnaire scores as dependent variable. The interactions of age, gender, and ward with fall-related factors were explored to test the potential moderating effects. We also examined the mediating role of fear of falling in the relationship of previous falls and age and perception of fall risk.
Results:
Patients who were in their older age, female, from endocrinology ward, had comorbidities, ambulatory aids, and fear of falling demonstrated a higher perception of fall risk which may or may not align with their actual risk of fall. The impact of previous fall injuries on perception of fall risk was significantly higher in older adults. The effects of fall-related training on patients’ perception of fall risk varied across wards. The fear of falling is a significant mediator between age and perception of fall risk.
Conclusion:
By understanding the self-perception of fall risk, health professionals would identify the population at higher risk of having an erroneous perception of their fall risk. This study increases health professional’s awareness and informs administrators to design and implement effective intervention and strategies that target patients’ perception of fall risk to promote patient safety.
Keywords
Introduction
Falls are the most common and serious adverse events for patients during hospitalization and may incur soft tissue injuries, fractures, 1 head trauma, 2 psychological trauma, 3 and even death. 4 Inpatients in the emergency, endocrinology, and neurology wards are at higher risk of falls compared to the general population, due to factors such as poor physical performance, diabetic peripheral neuropathy, and cognitive impairment.5 –7 The world guidelines for falls prevention and management also support that patient after stroke would be at high risk of fall, indicating the high risks in neurology ward. 8 Falls represent a major public health issue, leading to increased medical costs, prolonged hospitalization, reduced quality of life, and substantial social and economic burdens. 9
Although a considerable body of research have examined the risk factors of fall among high-risk populations including the patient’s physical condition, psychological factors, and environmental characteristics,10,11 few studies focused on patients’ perception of fall risk and associated factors. Perception of fall risk refers to the patient’s perception of the uncertainty and severity of falls. However, previous research has shown that only 61.9% of the patients’ perceived risk of fall matched with the assessment of nurses. 12 Approximately, 55.1% of the hospitalized patients did not perceive a high likelihood of fall out of a group of patients of whom all had been deemed to be high risk by nurses. 13 Decreased fear of fall was associated with decreased intentions to engage in fall prevention, 14 which may impede the effectiveness of fall-related education and intervention. As patients play a vital role in ensuring their own safety, their active participation should be motivated. 15 Therefore, identifying what population may have the tendency to perceive their fall risk less accurately would inform nurses and other health professionals to implement target intervention to reduce the incidence of fall and increase their engagement in fall prevention.
Previous research has shown that more past falls were related to higher levels of fear of falling and fall risk. 16 However, they did not investigate the severity of past falls (e.g., previous fall injuries/sequela), which may also influence patient’s fear of falling independent of the frequency of previous falls. Additionally, the associations between fall-related factors and patient’s perception of fall risk remain unknown (e.g., whether fear of falling may mediate the association of frequency and severity of past falls with risk perception). Although older adults tend to have a higher perception of perceived fall risk, 17 exploring what might explain the association of age and risk perception would help motivate patients to take actions to prevent falls, especially for those with high risk of fall due to illness but in younger age.
At present, there is still a lack of research on the perception of fall risk in high-risk patients in China. This study aimed to investigate the current situation and associated factors of patients’ perception of fall risk in three high-risk wards (emergency, endocrinology, and neurology) and explored potential moderating and mediating effects. Understanding the mechanisms would help identify the modifiable mediating factors to reduce the negative impacts of unmodifiable predictors on the outcome (fall risk perception). The exploration of vulnerable subgroups would provide nuanced information for prevention. Overall, the findings could provide evidence for the development of intervention and strategies to help patients develop accurate self-perceived fall risk and promote patients’ engagement in behaviors to prevent falls during hospitalization.
Methods
Study design and participants
This was a cross-sectional study using a convenient sampling method. Participants were recruited from three wards (emergency, endocrinology, and neurology wards) of two tertiary general hospitals in Hangzhou and Quzhou, Zhejiang Province China, from January 2023 to May 2023. The two sites were one new first-tier city and one third-tier city. The two tertiary hospitals include about 220 and 160 patients in the three wards, respectively, which were larger than the primary hospitals. The inclusion criteria were (a) age ⩾ 18 years old; (b) completed the survey within 24 h after admission; (c) able to communicate normally; and (d) voluntarily participated. We excluded the patients with cognitive impairment or unclear consciousness according to diagnose history and current assessment. Nurses in the wards assessed patients’ cognition according to the Mini-Cog which is a standardized cognitive screening tool widely used in clinical settings. Patients who scored ⩽3 out of 5 were excluded from participating in the study. 18 This ensured that participants had the necessary cognitive ability to fully understand the questions, thereby reducing the risk of confounding due to cognitive limitations. Our study aimed to better understand people whose perception of falling is not aligned to their actual risk of falling and identify those with higher risk of having an erroneous perception of their fall risk. Therefore, we recruited adult patients at all ages. The sample size was determined based on at least 10 times the number of predictors in regression analysis, plus 20% extension in case of sample loss. 19 There are 18 predictors in the full model, so the sample size would be at least 216. Finally, 340 individuals were administered the survey and 330 participants completed the survey (response rate 97.1%) with 178 (81%) from Hangzhou and 152 (95%) from Quzhou. We deleted the sample with all the same answers, remaining 324 valid questionnaires.
Measurements
Basic information
Basic information were obtained including age, gender, educational level, number of comorbidities (more than one diagnosed disease, i.e., if patients had only one disease, their comorbidities are none), clinical ward, smoking, ambulatory aids, fall-related training in the hospital, fear of falling, falls within 1 year prior to the study, and previous fall injuries. Fear of falling was assessed by a single-item question: “Do you experience any concern or worry about falling?” with dichotomous answer “yes” or “no,” which was consistent with other published literature in the field. 20 While direct asking about fear of falling might lead to some degree of response bias, we minimized its potential impact by embedding the question within the measures of other variables rather than isolating it. This approach may reduce the likelihood of patients feeling pressured to provide a socially desirable response. Fall-related training was measured as a dichotomous (received or not) variable. There was standardization of training across wards and hospitals released by the Chinese National Health Commission,21,22 which minimized the likelihood that differences in training influenced patients’ fall risk perception. The patients were able to understand and finish the questionnaire on their own indicating that they had normal cognitive or arousal level, which would not influence training effect.
Fall risk perception questionnaire
We adopted the Fall Risk Perception Questionnaire (FRPQ) (Supplemental file 1) to measure patients’ perception of fall risk with 27 items 3 dimensions (personal mobility, personal chronic condition, and environmental factors). 23 All items were rated on a 4-point Likert scale ranging from 0 (absolutely not true) to 3 (absolutely true). 23 Higher summed item scores indicate a higher perception of fall risk. The possible range of scores was 0–81. The Cronbach’s α of total questionnaire was 0.948 (subscales ranging from 0.828 to 0.917). 24 The Cronbach’s α in our study was 0.921.
Data collection
All participants provided written informed consent before participating in the study. Two nurses were selected in each ward to collect the data after receiving standard training of research methodology and physical assessment. They explained the purpose and content of the survey to the patients who were admitted to the hospital within 24 h and obtained their informed consent. We guaranteed the ethical principles of voluntary participation, anonymity, and confidentiality. The basic information and the FRPQ were distributed via an online survey platform (www.wjx.cn). Interview survey was adopted when patients had difficulty in reading and completing the questionnaires on their own. We also set the minimum time to finish the questionnaire to avoid invalid answers. This meant that participants had to finish the questionnaire in more than the minimum time, and this could avoid the situation that participants finish it too quickly. We also set all the questions as compulsory which helped avoid missing data. Participants could not submit the questionnaire if they did not answer all the questions. The platform would show message to remind the participants to finish all the questions.
Statistical analysis
Stata version 17.0 software was employed for statistical analysis. Descriptive statistics were used to describe patients’ basic information and their perception of fall risk. Frequencies (percentages) were shown for categorical variables and means (standard deviations) were shown for continuous variables. Bivariate analysis was performed to compare FRPQ scores between the levels of the independent variables including two independent samples t-test or one-way analysis of variance for data with a normal distribution. Then three-step multiple linear regression analyses were conducted with FRPQ score as dependent variable and demographic characteristics, health status factors, and fall-related factors as independent variables. The interactions of age, gender, and ward with fall-related factors were also explored to test the potential moderating effects. Next, we performed a path analysis using Lavaan package in R to examine the mediating role of fear of falling in the relationship of previous falls and age and perception of fall risk. The structural model fit were evaluated according to the following standards: χ2/degrees of freedom ratio (df) < 5.0, root mean square error of approximation (RMSEA) < 0.08, goodness-of-fit index (GFI) > 0.90, comparative fit index (CFI) > 0.90.25,26 The significant level was set as p < 0.05. We followed the STROBE guideline to report the study.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Ethical considerations
This study was approved by the Ethics Committee of the Quzhou City People’s Hospital (number: 2021-05-003). This study was conducted according to the Declaration of Helsinki. Written informed consent was obtained in accordance with ethical guidelines. Participants were guaranteed the right to withdraw at any time without consequences. No personally identifiable information was collected. Data access was restricted to research team. Participation was entirely voluntary and participants did not receive compensation for their time and effort.
Results
Participant characteristics and bivariate analysis
Among 324 patients, most of them were men (54.3%), aged 61–70 (38.9%), had received secondary school education (54.9%), nonsmoker (68.5%), had one types of comorbidities (50.4%), not used ambulatory aids (73.5%), and received fall-related training (72.5%), were afraid of falling (68.8%). Approximately 21.0% (68/324) of the patients had fall within 1 year prior to the study and 11.4% (37/324) of them had previous fall injuries. The average total score (SD) of FRPQ was 32.55 (16.19). The average scores (SD) on the subscales ranked from the highest to the lowest were environmental factors (12.94 (7.50)), personal mobility (12.46 (6.69)), and personal chronic condition (7.15 (4.21)), respectively. Bivariate analysis showed that age, educational level, clinical ward, comorbidities, ambulatory aids, fear of falling, falls within 1 year prior to the study, and previous fall injuries were significantly associated with FRPQ scores (all p < 0.05). Further detailed information is presented in Table 1.
Participant characteristics and bivariate analysis (n = 324).

We compared FRPQ scores between levels of the variables listed in column 1.
Multiple regression analysis
In multiple regression analyses (Table 2), we included demographic characteristics, health status factors, fall-related factors, and interaction terms step by step. Patients’ age, gender, and ward were significant associated with their perception of fall risk in all the models. Patients who were older, female, from endocrinology, and neurology tended to have higher perception of fall risk (all p < 0.05). When considering health status factors, more types of comorbidities and using ambulatory aids might increase patients’ perception of fall risk (p < 0.01), which explained 12% variance in total. In terms of fall-related factors, patients who had fear of falling may perceive 8-score higher level of fall risk compared with those who did not (p < 0.001), which additionally explained 5% variance. There were also significant interaction effect of age with previous fall injuries (p = 0.033) and marginal significant interaction effect of neurology ward with fall-related training (p = 0.079) on patients’ perception of fall risk (although the finding did not reach conventional levels of significance). Specifically, the difference between patients aged ⩾ 60 and <60 in the effect of previous fall injuries on perception of fall risk was 10.46 scores (stronger effect in patients aged ⩾ 60). The difference in the effect of fall-related training on patients’ perception of fall risk was the most in the neurology ward (7.293-score higher than that in the emergency ward), which may be due to the type of patients being treated. There were no interactive effects of age, gender, and ward with other fall-related factors (data not shown due to nonsignificant results).
Multiple regression analysis* (n = 324).

The dependent variable is FRPQ score.
Path analysis
As falls within 1 year and previous fall injuries were not significantly associated with perception of fall risk, hypothesis 1 was not tested (Figure 1). Results of hypothesis 2 showed that the association between age and perception of fall risk was significantly mediated by fear of falling (p < 0.05). As Figure 2 illustrates, the standardized indirect effect was 0.296 * 0.137 = 0.041. The standardized direct effect was 0.237 after controlling for mediation. The standardized total effect was 0.278. The fear of falling is a significant mediator between age and perception of fall risk. The model produced adequate fit (χ2/df = 5.47, p < 0.001, RMSEA = 0.01, GFI = 0.96, CFI = 1.00).

Hypothesis 1.
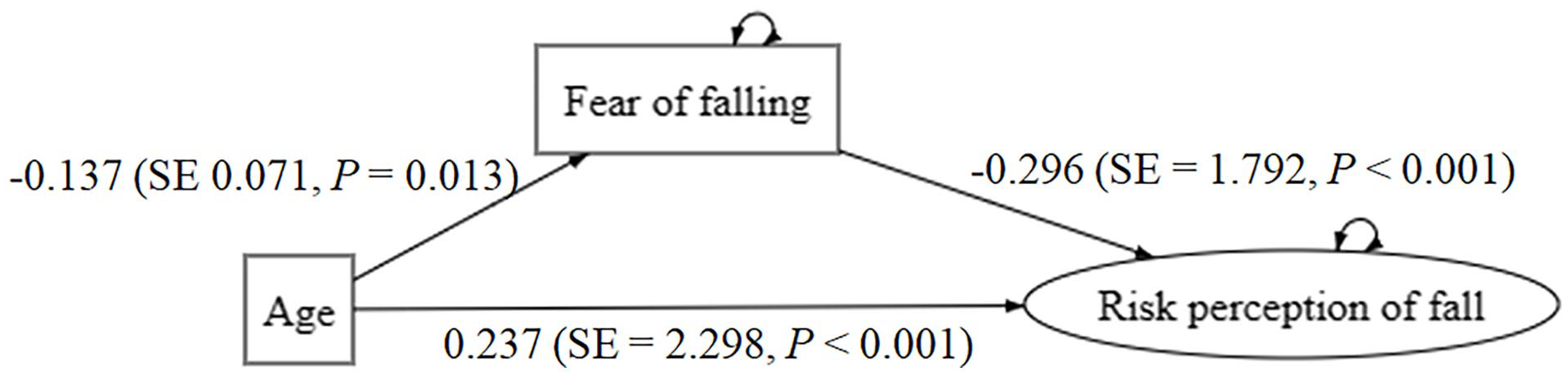
Hypothesis 2 and results.
Discussion
Primary findings
In this study, we investigated the influence of demographic characteristics, health status factors and fall-related factors on the perception of fall risk in patients from the wards with high prevalence of fall and examined the potential moderating and mediating effects. Patients who were in their older age, female, from endocrinology ward, had ⩾1 comorbidities, ambulatory aids, and fear of falling demonstrated a higher perception of fall risk. The impact of previous fall injuries on perception of fall risk was significantly higher in older adults. The effects of fall-related training on patients’ perception of fall risk varied across wards, which may be due to differences in the patients’ receptiveness to the training. The fear of falling is a significant mediator between age and perception of fall risk. These results would help identify the population at higher risk of having an erroneous perception of their fall risk and the intervention target to engage patients in fall prevention programs.
Comparison to prior work
Patients tend to perceive a lower level of fall risk than health professionals at admission and this trend continued at discharge, 24 indicating the importance to examine the factors that influence patients’ perception of fall risk. Our results showed that the average total score of fall risk perception among patients was 32.55 ± 16.19, which was much higher than that in a Korean population (8.40 ± 11.24). 23 This may be due to the difference in the ward of the patients. In this study, participates were from emergency, endocrinology, and neurology wards, while the Korean study recruited patients from acute care hospitals. The result of lower perception of fall risk in emergency ward in our study also supported such disparity. Previous studies mainly used a single question to measure participants’ perceived likelihood of falling when hospitalized.27,28 However, since the perception of fall risk is a multidimensional construct, a universal and validated questionnaire is necessary to discuss patients’ risk perception globally.
As for demographic characteristics, the results showed that female and older patients had a higher level of perceived fall risk. However, this was partially consistent with previous research where perceived fall risk increased with age, while no differences were found between men and women. 14 Considering health status factors, patients with more types of comorbidities and ambulatory aids demonstrated a higher perception of fall risk. This may be because these patients often have severe symptoms, which are related to limited physical activity, reduced self-care ability, and thus a higher perception of fall risk. Evidence showed that middle-aged adults with comorbidities were more likely than those without comorbidities to fall and suffer a fall-related injury. 29 Therefore, clinical nurses should not only pay attention to elderly patients but also younger patients with multiple comorbidities to effectively prevent fall incidence. Potential interventions to promote a matching perception of falling could be developed according to a theoretical framework of fall risk perception such as treating falls appropriately, increasing individual autonomy, and adjusting emotions and mindset. 30
In terms of fall-related factors, patients who have a fear of falling showed significant higher fall risk perceptions after controlling for other demographic characteristics and health status factors. However, falls within 1 year prior to the study and previous fall injuries become nonsignificant. Our results contradicted with previous findings that patients with a history of falls within 3 months before admission were associated with an increased perception of fall risk compared with patients without fall history. 31 The nonsignificant impacts of falls within 1 year and previous fall injuries indicated that the frequency and severity of past falls may not be effective targets to identify the population at risk of having an erroneous perception of their fall risk. There might be some other important factors such as age and comorbidities which can be a robust predictor of risk perception. Furthermore, patients’ fear of falling is a significant mediator between age and their perception of fall risk. This finding adds to the knowledge that age not only directly influences the risk perception but also indirectly influences the risk perception through fear of falling, which could serve as an intervention target to help patients form accurate perception of fall risk.
In addition, we found that there was a significant interaction between age and previous fall injuries. The female-male difference in the effect of previous fall injuries on their perception of fall risk was around 10-fold, indicating higher impact of fall sequels on risk perception in female. This may be explained by menopause in female in mid- and older age, which may generate a decrease in hormones leading to various symptoms such as reduced bone mineral mass and muscle strength, hot flushes and fatigue, which would make women more concerned about falls. 17 Medical staff should raise awareness of female inpatients to help them develop matching of actual and perceived fall risk. A marginal significant interaction between neurology ward and fall-related training was also found, indicating that the effect of fall-related training on patients’ perception of fall risk might vary in different wards. This finding suggests that tailored education on falls prevention should be delivered as suggested in the World Falls Guidelines. 8 A recent systematic review and meta-analysis also showed that the only intervention that yielded a significant reductive effect on fall was education compared with environment modifications, assistive devices, or therapeutic exercises. 32 Therefore, personalized interventions with novel approaches such as cognitive behavioral therapy 33 should be integrated into fall prevention to increase effectiveness.
Limitations
There were also some limitations in this study. First, this study only recruited patients from two tertiary hospitals, which may reduce the representativeness. Second, the cross-sectional design could not shed light on casual inference among the study variables. Third, although our survey was designed to minimize missing responses by requiring answers for each item, we acknowledge that a proportion of participants did not complete the full survey which may lead to potential bias. We have reported the number of completers and response rate. Given that missing data due to noncompletion was minimal (2.9%) and survey responses from noncompleters are entirely missing, we did not handle missing data statistically. Fourth, training in itself may influence patient perception of fall risk and several leading questions may impact patient responses. We acknowledge that training may confound the study design, data collection, data analysis, findings, and conclusion. Fifth, the direct phrasing of the fear of falling question could have influenced responses. Despite the limitations, this study was still innovative in exploring the associated factors of patients’ perception of fall risk, what might explain these associations and how these effects varied.
Future direction
Future research would validate the influence of frequency and severity of previous falls on patients’ perception of fall risk in another sample as well as explore other possible interactions. Expanding recruitment across multiple hospital levels using probability sampling methods (e.g., stratified random sampling) could ensure a more representative sample, which benefits for greater generalizability. Future studies should consider experimental designs or longitudinal approaches to isolate the causal effects of training on fall risk perception and consider alternative ways of assessing fear of falling such as behavioral indicators to minimize response bias. Multicenter, large-sample studies will be valuable to understand patients’ perception of fall risk and provide evidence for effective intervention.
Conclusion
Understanding patients’ perception of fall risk is crucial to prevent falls. By assessing individuals’ self-perceived fall risk, health professionals can identify those who are more likely to have a misjudged perception of their fall risk. This study would inform healthcare practitioners to design and implement effective intervention and strategies that target patients’ perception of fall risk to promote patient safety.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251335811 – Supplemental material for Perception of fall risk in hospitalized patients and associated factors: A cross-sectional study and path analysis
Supplemental material, sj-docx-1-smo-10.1177_20503121251335811 for Perception of fall risk in hospitalized patients and associated factors: A cross-sectional study and path analysis by Ye Luo, Yuanfei Liu, Suxian Tan, Tian Xu and Guanjun Bao in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank all the patients for their participant in the study.
Ethical considerations
This study was approved by the Ethics Committee of the Quzhou City People’s Hospital (number: 2021-05-003).
Consent to participate
All the participants voluntarily participated and signed informed consent. This study was conducted according to the Declaration of Helsinki. Written informed consent was obtained from all subjects before the study.
Author contributions
Ye Luo and Suxian Tan conducted the research. Ye Luo and Yuanfei Liu wrote the initial paper. Tian Xu and Guanjun Bao gave valuable input in revision.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by 2020 Technology department project of Quzhou city (2020K42).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.