
Abstract
Objectives
Urine specific gravity (USG) is the most common method for the estimation of urine concentration in cats. Utilization of USG as a screening tool is easily accessible and is of low cost to the client if strategically utilized in settings of higher diagnostic value. There is currently minimal population information regarding how USG changes across ages in cats.
Methods
Data were collected from electronic pet medical records from more than 1000 hospitals and screened for cats with an apparently healthy clinical status and complete diagnostic information. USG was compared with age in multiple analyses to examine the relationship between the variables.
Results
In the absence of other indicators of disease, renal concentrating ability begins to diminish, on average, starting at approximately 9 years of age. By age group, cats aged 11–15 years (1.044, 95% confidence interval [CI] 1.043–1.044) had statistically significantly lower mean USGs compared with cats aged less than 1 year (1.049, 95% CI 1.048–1.051; P <0.001), 1–6 years (1.049, 95% CI 1.049–1.050; P <0.001) or 7–10 years (1.049, 95% CI 1.048–1.049; P <0.001). Cats aged ⩾15 years (1.038, 95% CI 1.036–1.040) had statistically significantly lower mean USGs compared with cats aged less than 1 year (P <0.001), 1–6 years (P <0.001), 7–10 years (P <0.001) or 11–15 years (P <0.001).
Conclusions and relevance
Renal concentrating ability begins to diminish, on average, starting at approximately 9 years of age and is progressive as cat age increases. This study provides important and new information to help improve screening practices for disorders of concentrating ability in cats.
Introduction
Current guidelines recommend that cats be evaluated every 6–12 months for preventive wellness screening once they are >7 years of age.1 –4 This evaluation should include a physical examination, body weight, body condition score and blood pressure every 6–12 months, as well as screening diagnostics, including a minimum database (complete blood count [CBC], serum biochemistry and urinalysis [UA]), performed every 12 months.1 –4 As the cat ages from the ‘mature adult’ range (7–10 years) to ‘senior’ (>10 years), the frequency of these screening evaluations increases. 2 One goal of preventive wellness plans includes the early detection of disease in otherwise apparently healthy cats. Although this represents an ideal preventive monitoring program for cats, it may also be cost prohibitive for some owners, particularly at the more frequent evaluations recommended in older cats. 2 As such, more targeted or individualized approaches are still required to optimize feline healthcare and monitoring across the spectrum of care. 5
Among the screening diagnostics, a complete UA aids in screening asymptomatic cats for diseases that affect renal concentrating ability. 6 Among the data obtained with this test, urine specific gravity (USG) is one of the most important physical properties evaluated on the UA and is the most common method for the estimation of urine concentration in cats. 6 USG is a cost-effective, readily available and procedurally simple method of obtaining vital information during veterinary evaluations, as it pertains to the evaluation of kidney function.6,7 As chronic kidney disease (CKD) is one of the most common chronic disorders in cats, USG represents an accessible screening approach for cats in preventive programs.8,9
The key to effective utilization of USG as a screening tool relies upon epidemiologic principles to optimize the clinical utility. Previous consensus statements have suggested performing USG in cats aged over 7 years.8,10 –12 However, currently there are few data regarding trends in USG among otherwise apparently healthy cats. If an inadequately concentrated USG is identified, it may suggest inadequate renal concentrating ability and highlight a patient population that requires additional diagnostics, more intensive monitoring or early intervention. This has the potential to be impactful on the prognosis for cats with CKD as the prognosis is closely correlated to disease severity based on International Renal Interest Society (IRIS) stage and early intervention may possibly be associated with improved outcomes.13,14 The aim of the present study was to evaluate trends in USG by age and age group using large-scale data from a nationwide network of primary care veterinary hospitals to identify when USG may be most effectively utilized as a screening tool for renal concentrating ability.
Materials and methods
A retrospective study was performed on medical records from cats determined to be apparently healthy, as outlined below, to evaluate changes in USG by age. Cats of all ages, breeds and sexes that were seen in a Banfield pet hospital were eligible for enrollment. The initial data acquisition was performed across the Banfield nationwide database and did not exclude any cases.
Data were collected from electronic pet medical records from more than 1000 hospitals geographically dispersed across the USA (43 states, District of Columbia and Puerto Rico). On average, approximately 750,000 unique feline patients are seen each year. All hospitals in the network use a proprietary pet medical record system (PetWare). Data are uploaded nightly to a centralized data warehouse making it available for analysis. The system contains structured and unstructured fields. Structured fields include data such as physical examination findings, diagnostic codes and invoice information. Unstructured fields include free-text information, such as interpretive findings and communication records. Patients may be recorded as healthy by the providing veterinarian, and hospital visits may also be screened for appointment type (healthy, illness, surgery, etc).
The original data acquisition obtained 159,378 cases over the study period (1 January 2010 to 31 December 2020) that were presumed to be healthy based on structured codes in the medical record and/or having no presenting medical complaint. Cats were required to have USG obtained during the study period, as well as additional clinical pathology results, including hematocrit/total solids or CBC, biochemical profile, total thyroxine (in cats aged >7 years) and complete UA. Data collected for each case included patient age (years), weight (kg), sex and neuter status, and body condition score. The exclusion criteria consisted of ever having had a diagnosis of diabetes mellitus, hyperthyroidism, administration of fluid therapy at the hospital visit when urine and blood samples were obtained, and positive results for urine glucose. Additional exclusion criteria were any record of administration of methimazole, steroids, diuretics, insulin or insulin supplies. Each case was then reviewed individually by a Diplomate of the American College of Veterinary Internal Medicine to verify health status and ensure all required laboratory results were present. Cases were removed in a stepwise fashion based on laboratory abnormalities, absent diagnostic results and medical diagnoses. Hyperglycemia was permitted up to values of 200 mg/dl in the absence of glucosuria. Finally, USG values were included regardless of results (Figure 1).

CONSORT diagram. After all inclusion and exclusion criteria were satisfied, cases were then removed in a stepwise fashion based on laboratory abnormalities, absent diagnostic results and medical diagnoses. RBC = red blood cell; USG = urine specific gravity
All hospitals had the same fleet of in-house laboratory equipment. Serum biochemistry tests were performed on the Catalyst Dx Chemistry Analyzer (IDEXX), CBCs were performed on the VetScan HM5 (Zoetis) and urinalyses were performed via manual refractometer (Clinical Refractometer 7 Inch, MWI; Jorgensen) and UA reagent strip testing. Thyroid hormone tests were measured using the Catalyst Dx Chemistry Analyzer (IDEXX).
Variables of interest
USG was the outcome of interest, where adequate concentrating ability was defined as USG >1.035, and USG ⩽1.035 was considered inadequately concentrated. 8 The primary independent variable of interest was age at visit, which was evaluated as both a continuous variable as well as a categorical variable based on International Society of Feline Medicine (ISFM) age group categorization. 2 The relationship between and USG was also investigated.
Statistical analysis
Descriptive statistics were assessed by adequacy of concentrating ability. Categorical variables were described using frequencies and percentages, where differences in proportions were assessed using a χ2 test. Continuous variables were described using medians and interquartile ranges (IQR) and differences in the distributions between groups were evaluated using the Mann–Whitney U-test. Scatter plots were used to assess trends in USG across all ages. Locally estimated scatterplot smoothing (LOESS) was used to assess the trend in USG across age as a continuous variable and means with corresponding 95% confidence intervals (CIs) were plotted to assess age as a categorical variable. The sensitivity and specificity of classifying cats with inadequate urine concentrating ability was plotted for each age of the cat. In addition, the Spearman correlation coefficient was used to determine whether creatinine was associated with USG, and the impact of ‘high-normal’ creatinine (ie, creatinine ⩾1.5) was assessed by evaluating the correlation between creatinine and USG with and without high–normal creatinine values. Significance was assessed at the 0.05 level, and all statistical analyses were performed using SAS (version 9.4; SAS Institute).
Results
There were 159,378 presumed healthy feline patient visits during the study search period. The data set was reviewed for verification of complete medical records as well as screening for clinically significant abnormalities on the CBC, biochemistry profile, thyroxine level and UA (Figure 1). After data verification, a total of 15,027 cats remained, which were included in this study as apparently healthy. This population comprised cats of varying ages (Table 1, Figure 2a). There were 13,694 (91.1%) cats that were classified as having adequate concentrating ability (Table 1, Figure 2b). Cats with a USG ⩽1.035 were significantly older than cats with a USG >1.035 (P <0.001). The percentage of cats retaining a USG >1.035 per age group were as follows: age <1 year (95.2%); 1–6 years (94.3%); 7–10 years (93.4%); 11–15 years (77.5%); and ⩾15 years (57.9%). By age group, there were no statistically significant differences in mean USG measurements between cats aged less than 1 year (1.049, 95% CI 1.048–1.051); 1–6 years (1.049, 95% CI 1.049–1.050) or 7–10 years ( 1.049, 95% CI 1.048–1.049; P = 0.13) (Figure 3). Cats in the age group of 11–15 years (1.044, 95% CI 1.043–1.044) had statistically significantly lower mean USGs compared with cats aged <1 year (1.049, 95% CI 1.048–1.051; P <0.001), 1–6 years (1.049, 95% CI 1.049–1.050; P <0.001) and 7–10 years (1.049, 95% CI 1.048–1.049; P <0.001) (Figure 3). Similarly, cats in the group aged ⩾15 years (1.038, 95% CI 1.036–1.040) had statistically significantly lower mean USGs compared with cats aged <1 year (1.049, 95% CI 1.048–1.051; P <0.001), 1–6 years (1.049, 95% CI 1.049–1.050; P <0.001), 7–10 years (1.049, 95% CI 1.048–1.049; P <0.001) and 11–15 years (1.044, 95% CI 1.043–1.044; P <0.001) (Figure 3). By inspection, USG estimates began to decrease at the age of 9 years, and the LOESS curve indicated that the estimated mean USG was equal to 1.035 at 18.7 years (Figure 4). The proportion of cats with inadequate urine concentrating ability varied by age (Table 2).
Significant population characteristics and laboratory results at wellness visit (n = 15,027)

Data are n (%) or median (IQR) unless otherwise indicated. The table describes the analyzed variables as a whole (all cats regardless of USG) as well as divided by the cut-off USG of 1.035
IQR = interquartile range; USG = urine specific gravity

(a) Distribution of cat ages (in years) in the sample. (b) Proportion of cats with inadequate urine concentrating ability for each age in years

Mean USG with 95% confidence intervals based on International Society of Feline Medicine age group categories. There were no statistically significant differences in mean USG measurements between cats aged less than 1 year, 1–6 years or 7–10 years (P = 0.13). Cats aged 11–15 years had statistically significantly lower mean USGs compared with cats aged <1 year (P <0.001), 1–6 years (P <0.001) and 7–10 years (P <0.001). Cats aged ⩾15 years had statistically significantly lower mean USGs compared with cats aged <1 year (P <0.001), 1–6 years (P <0.001), 7–10 years (P <0.001) and 11–15 years (P <0.001). CI = confidence interval; USG = urine specific gravity
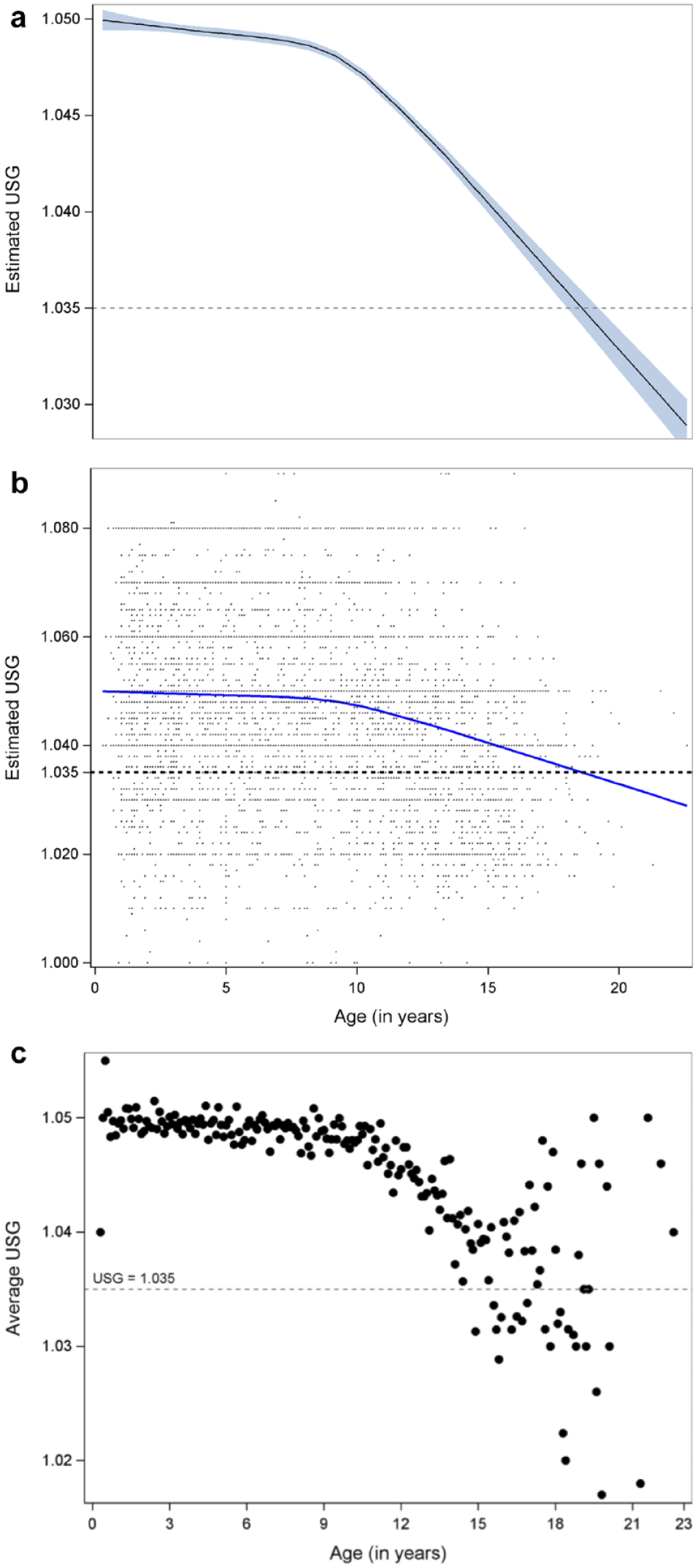
(a) LOESS curve and 95% confidence bands (blue) of USG vs age. By inspection, USG estimates began to rapidly decrease at 9 years old, and the LOESS curve indicated that the estimated USG was equal to 1.035 at 18.7 years. (b) Scatterplot of USG vs age and estimated LOESS curve (blue). (c) Mean USG per age (rounded to the 10th of a year). LOESS = locally estimated scatterplot smoothing; USG = urine specific gravity
The first age of cats to reach a specific proportion with inadequate urine concentrating ability (USG <1.035); the number of total cats at the identified age was also reported

No ages had 90% of cats with inadequate urine concentrating ability
USG = urine specific gravity
A contingency analysis using the χ2 test found statistically significant differences in proportions of the sample based on body condition by urine concentrating ability (P <0.001). The remainder of categorical variables evaluated were not statistically significantly different between cats with a USG >1.035 and those with a USG ⩽1.035 (all P values >0.05) or the differences were not clinically significant (Table 1). Body weight was statistically significantly different between cats with a USG >1.035 and those with a USG ⩽1.035 (P <0.01). The remainder of the continuous variables evaluated were not statistically significantly different between cats with a USG >1.035 and those with a USG ⩽1.035 (all P values >0.05) or the differences were not clinically significant (Table 1).
In addition, creatinine was found to be weakly and negatively correlated with USG (ρ = −0.020) and this correlation was significant (P = 0.012). A repeat analysis with the removal of cats with creatinine <1.6 mg/dl as well as an analysis with the removal of cats with creatinine <1.5 mg/dl did not affect the results of the group comparisons. There were still statistical differences between mean USG among age groups. However, after removing all cats with a creatinine level of 1.6, the Spearman correlation was no longer significant (ρ = −0.006; P = 0.518). Similarly, the correlation between USG and creatinine remained insignificant after removing all cats with creatinine ⩾1.5 (ρ = −0.007; P = 0.659).
Discussion
USG assessment is a helpful component in screening older cats and determining the ability of the kidney to concentrate urine, which facilitates the diagnosis of CKD and other disorders.6,8 The results of this study indicate that in the absence of other indicators of disease, on a population basis, renal concentrating ability begins to diminish, on average, starting at approximately 9 years of age. However, most cats had adequate concentrating ability regardless of age, and loss of concentrating ability (defined as USG <1.035), on average, in the population was not identified in the analysis until cats were aged >15 years. Taken together, this allows practitioners a better understanding of the utility of using USG as a screening test to determine the ability of the kidney to concentrate urine across different age ranges in cats evaluated in clinic. In addition, from a patient-centered approach, the single time point USG is a screening test, and once an inadequate USG is identified, it should then be documented to be a persistent finding as well as interpreted in the light of the patient’s clinical status. If inadequate concentration is persistent, this may allow for specific interventions in the diagnosis, management and monitoring of both the health status of cats as well as various disease states.
The results of this study show a decrease in renal concentrating ability with age, but the study is unable to distinguish between age-related decline in renal function vs early renal disease. Aging-associated degenerative changes in the kidneys are well established in people.15,16 These changes include physical changes to the kidneys (ie, glomerulosclerosis, interstitial fibrosis, tubular atrophy and arteriosclerosis) as well as changes in renal functional ability. 16 In contrast, there is limited research on the specific effects of aging on feline kidneys, both physically and functionally. 17 Recent work has shown evidence that renal aging exists in cats and shares some histologic features seen in humans.16 –18 Whether a correlation between renal age-related phenotypic and functional changes and progression to clinically relevant kidney disease is present is unknown in cats; however, guidelines for feline medicine recommend monitoring these changes during routine wellness examinations. 19 The USG findings across age in this study may indicate age-related changes, early non-clinical kidney disease or a combination of both factors. This underscores the potential importance of the USG in monitoring feline patients as they age.
Based on studies from the UK, one of the most prevalent diseases in older cat populations affecting renal concentrating ability is CKD.9,20 As such, early detection of inadequate concentrating ability is most likely to be useful in the early detection of CKD. 8 This is further supported in this data set based on the inclusion of high normal creatinine values and their greater impact on the relationship between loss of concentrating ability and creatinine. Further studies should examine whether the early detection of inadequate USG and serial monitoring in a longitudinal prospective study could result in the earlier diagnosis of CKD, particularly in comparison with other detection methods such as symmetric dimethylarginine (SDMA).
Other disorders that commonly affect USG, such as diabetes mellitus and hyperthyroidism, were ruled out to the best of our ability in the data sorting process in this study.21,22 However, it is possible that subclinical hyperthyroid cats or pre-diabetic cats were included in the analysis and affected the results; for example, based on the study inclusion criteria, only cats aged ⩾7 years were required to have a thyroid level evaluated. Cats aged <7 years, while not the most common age range for hyperthyroidism, could have inadvertently been included. USG can also be affected by diet, and data on dietary history was inconsistently captured in the electronic medical record system from this study. 23 Thus, analysis on the potential impact of diet on USG results was not able to be performed. Lastly, USG can be marginally affected by other variables, including glucose and protein in the urine; as such, cats with glucosuria and proteinuria were removed from the analysis when screening each case for a presumed apparently healthy status.23,24
Interpretation of the data from this study must consider that the results are based upon a single time point assessment of USG. Documenting repeatable and consistently inadequate USG is important, as an intermittent inadequate specific gravity may be situationally appropriate for some cats in the absence of azotemia. Previous work has shown that clinically significant day-to-day variation in USG measurement exists in both cats and other species.25,26 Even urine sampled twice within the same 15 h time frame can result in clinically significant variation in feline USG results. 27 Regardless, the data presented in this manuscript emphasize the use of USG assessment for crude screening purposes and when this is most likely to be useful. Once an inadequate USG is identified, the clinician must still interpret this result in the context of the patient, establish it as a consistent finding, as well as differentiate between age-related functional changes or early CKD using serial monitoring.
As would be expected, at most ages, the majority of cats retained adequate renal concentrating ability. In the context of this study, the USG as a screening tool is used to detect the smaller percentage of cats that have inadequate renal concentrating ability. Importantly, the USG represents a cost-effective screening option for many cats and is most useful when interpreted in conjunction with client goals and resources. The cutoff of 9 years of age in this paper for increased clinical utility was established based on when there is the first detection of an increase in frequency of inadequate USG based on age. This highlights the earliest time that the frequency of increased inadequate USG values was noted, despite still comprising a small proportion of the overall population at that age. The utility of this information needs to be applied individually to each patient seen in clinic to maximize benefit to the cats’ healthcare and clinical value in the context of the goals of the cats’ guardians.
These data also describe cats with no clinical signs or known laboratory abnormalities on screening diagnostics. This was done to limit the interference of other disease processes on USG assessment; therefore, these data should not be extrapolated to cats with known clinical signs or laboratory abnormalities. It should be applied as a screening diagnostic in the context of evaluation of annual wellness evaluations and preventive medicine approaches. Importantly, there are no currently published data to show that the detection of inadequate USG in this manner predicts development of azotemic kidney disease or is separate from normal aging or biologic variability. Further study should examine the long-term implications of early identification of inadequate renal concentrating ability on health outcomes.
The data from this study should also not be interpreted as a surrogate for previous aging preventive wellness recommendations.1,2 The remainder of the wellness diagnostics recommended should still be considered when possible; for example, some cats with azotemic CKD will produce a USG ⩾1.035 and would be missed by utilizing only USG in a screening process.28,29 This highlights the importance of obtaining biochemical parameters to facilitate a more complete interpretation of renal function and screening of other disease when possible, with a particular focus on trends in variables of interest. 1
Data were collected from electronic pet medical records from the Banfield Hospital system. The vast majority (>80%) of pets visiting Banfield participate in a wellness plan program, which consists of a suite of pre-paid services, available at multiple levels, with options for additional services based on owner preference and individual patient needs. Wellness plans offer unlimited office visits, which may help remove barriers to frequent veterinary visits, but may also introduce detection bias in a population. Routine clinical pathology testing (CBC, serum biochemistry and UA) is included in many wellness plans, with additional testing available based on the plan (eg, serum thyroid concentration in senior cats). Regardless, challenges continue to exist to encourage routine veterinary care for feline patients, and this may be exceptionally true for apparently healthy cats, if owners do not see the need to bring these cats to a veterinary clinic. While the population represented in this study was hypothesized to be representative of a healthy population seen in primary care veterinary practice, it remains possible that different types of bias may have been present in this retrospective analysis.
The limitations of the study include its retrospective nature, the potential introduction of bias, and data entry dispersed by time and geography. Pet ages are also recorded into the medical record by hospital teams using owner-provided information, and it remains possible that specific dates of birth were not known or were estimated in many cases. Cats in the group aged 11–15 years had a lower USG compared to younger cats, even with USG remaining above 1.035. Loss of concentrating ability (defined as USG <1.035), on average, in the population was not identified in the analysis until cats were aged >15 years. This also supports the proposed potential benefit of serial monitoring of USG for trends over time vs specific cutoffs at single time points. Additional analyses would need to be performed to determine whether the monitoring of trends would aid in the early identification of CKD or other disease development in the sub-population of cats aged 11–15 years with decreased USG compared with younger age groups who are not yet below the threshold of 1.035. Lastly, both the refractometer itself as well as the individual reading the result have been shown to impact USG results and it is possible that these variables effected the results in this study.30 –32
Conclusions
This study provides important and new information to help improve screening practices for CKD and other disorders of urine concentrating ability in cats, facilitate earlier disease detection, and inform more individualized and targeted diagnostics to feline patients. This study also suggests evaluating USG in feline patients in conjunction with the age of the patient, as well as the creatinine.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.