
Abstract
Objectives
Cat Friendly Practices (CFPs) were compared with non-CFP control practices to determine whether CFPs had an increased proportion of clinical visits, number of visits per cat per year and inclusion of diagnostic testing. To measure diagnostic testing behavior, the numbers and types of tests analyzed and clinically relevant findings were compared.
Methods
In a retrospective analysis comparing CFPs and non-CFPs, clinic financial data and associated diagnostic tests from a commercial laboratory for 2018 and 2021 were analyzed. Data were stratified based on visit type and included revenue per visit type, revenue per patient, the number of visits per year and the proportion of visits that included diagnostic testing. Analyses of clinical findings for June 2021 to June 2022 examined clinical findings associated with biochemistry, complete blood count, urinalysis and thyroid testing categories at diagnostic patient visits, the proportion of clinical visits in which each finding was observed, the volume of testing categories as a proportion of clinical visits, and the proportion of diagnostic visits with one, two, three or four testing categories.
Results
The average revenue per feline visit and visits that included diagnostic testing were higher at CFPs. There was no difference in the proportion of wellness visits; however, CFPs had higher mean visits per year per patient. CFPs performed diagnostic testing at 12% more clinical visits, and had higher annual revenue per feline patient for all visits and for visits including diagnostic testing. CFPs had higher odds of patients having >1 visit that included bloodwork or urinalysis. They were more likely to include all four testing categories and less likely to include only one category at a diagnostic visit. CFPs identified a higher number of cats with clinical findings.
Conclusions and relevance
CFPs exhibited unique diagnostic testing behavior by performing more diagnostic tests more frequently and identifying a higher number of cats with abnormal findings.
Introduction
Demographic studies of pet ownership in the USA over the past 5 years have demonstrated the percentage of pet cats in homes to be fairly consistent, with 25–26% of households reported to have cats as pets, with an overall increase in the owned cat population of approximately 3% each year between 2016 and 2020.1,2 In spite of the consistent popularity of the pet cat, the Bayer Veterinary Care Usage study found that 52% of cats had not visited a veterinary practice for any reason in the prior year and only 37% of cats visited the veterinarian for routine examination. 3 Fear-anxiety associated with veterinary visits were the main contributors to care avoidance, 4 with caregivers’ concern about stress to their cat during a hospital visit being an important factor even when deciding whether to vaccinate. 5 A lack of knowledge of the importance of routine examinations, cost of visits and the cat’s ability to hide signs of illness, injury or pain also contributed.4,6
Many aspects of visits to a veterinary practice can negatively affect feline welfare.7 –10 Cats have excellent abilities to sense and avoid danger, hiding illness and pain as a survival strategy. They are territorial animals that require a sense of control, safety and familiarity in their physical and social environment. Taking a cat from its own territory to an unfamiliar place such as a veterinary practice, where it experiences unfamiliar sounds, smells, sights and movements, gives rise to protective (negative) emotions 11 and increases distress.12,13 Protective emotions including frustration, fear-anxiety and/or pain may be triggered when a cat feels it lacks control over a situation, or is separated unnecessarily from its caregiver and/or restrained for examination/diagnostic procedures, at times without appropriate analgesia.8,9,11–13 In addition, stress associated with veterinary visits can lead to changes in patients’ physiologic parameters, leukogram and biochemistry results, cortisol levels and behavior,14–17 potentially leading to inaccurate findings. 7
In 2011, the Feline-Friendly Handling Guidelines 18 were published by the American Association of Feline Practitioners (AAFP) and the International Society of Feline Medicine (ISFM). In 2012, the AAFP’s Cat Friendly Practice (CFP) and ISFM’s Cat Friendly Clinic (CFC) programs were launched, followed by the AAFP Cat Friendly Certificate Program in 2020. These programs provide veterinary practices and professionals with a checklist of criteria and foundational resources to improve feline veterinary care, minimize stress and create a more positive veterinary experience for cats, their caregivers and the entire veterinary team. Generally, the CFP and CFC are managed geographically by the AAFP in the Americas and the ISFM throughout the UK, Europe, Asia, Africa, Australia and New Zealand. Recently, the 2011 Guidelines were updated and released as the 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines 13 and the 2022 ISFM/AAFP Cat Friendly Veterinary Environment Guidelines. 19
The principal goal of the cat friendly approach is to ‘elevate care for cats by enhancing the environment and experience, as well as reducing stress for the cat, caregiver, and also the entire veterinary team’. Accumulating data have demonstrated benefits to caregivers,20–22 veterinary teams 23 and veterinary businesses.20,22,23 In addition to providing a cat friendly veterinary environment, 19 CFPs are intended to interact with feline patients in a compassionate, cat friendly manner, 13 which is supported by various studies.8,14 –16 For example, gentle passive restraint of cats resulted in eight times less struggling, shorter examination time, an increased likelihood of the cat staying on the table after examination and fewer postures indicating distress. 14 In another study, cats preferred to spend time in locations where they experienced passive restraint. 16 In comparison to control groups, reduced-stress transport and handling protocols resulted in quicker sedation and lower dosages of induction drugs to achieve general anesthesia in cats. 24
The 2022 CFP Survey conducted by the AAFP reported that veterinary teams in CFPs have improved knowledge about cats, reduced stress associated with visits for feline patients, higher caregiver satisfaction and more positive team dynamics. 21 In addition, team members also had fewer injuries at CFCs 20 and CFPs 23 and a lower overall cost per workers’ compensation claim at CFPs. 23
In Spain, CFCs had a higher percentage of feline patients and a higher percentage of revenue from feline patients. 22 The same study found that CFCs achieved a 30% higher frequency of feline patient visits, an increased average number of transactions (visits) per year per feline patient and a 12% higher average transaction value. Finally, feline caregivers spent 45% more per year at CFCs compared with non-CFCs, with 40% more caregivers purchasing their pet food at CFCs. 22
Given previous positive findings, we hypothesized that CFPs might exhibit differences in medical practices compared with non-CFPs. We hypothesized that feline patients at CFPs would have more visits per year, a higher rate of diagnostic testing and more wellness visits. We also sought to determine whether CFPs had differences in diagnostic testing behavior, hypothesizing that CFPs would have increased numbers and types of tests analyzed per feline patient. A final aim was to assess whether CFPs detected more clinically relevant findings compared with non-CFPs.
Materials and methods
Identification of practices
Practice and result data were derived from the IDEXX Laboratories database. CFPs were identified through information provided by the AAFP. CFPs were included if they had an active practice account with IDEXX, available practice information management systems (PIMS) data and had a single location associated with the practice account. Further inclusion criteria differed for the financial and individual results analysis arms of the study (Figure 1 and Table 1). For the financial analysis, non-CFPs were included if they met the above criteria and feline visits comprised ⩾20% of total visits between 1 January 2016 and 31 December 2021, to align with the median percentage of feline visits at included CFPs. For the individual results analysis, non-CFPs were matched to CFPs by total cat visit volume with a ratio of seven control practices to one CFP. The 7:1 matching ratio was chosen to maximize the statistical efficiency of the study with as many controls as could be supported by the data set. Visit volumes and diagnostic test results were compiled for the period between 1 June 2021 and 1 June 2022.
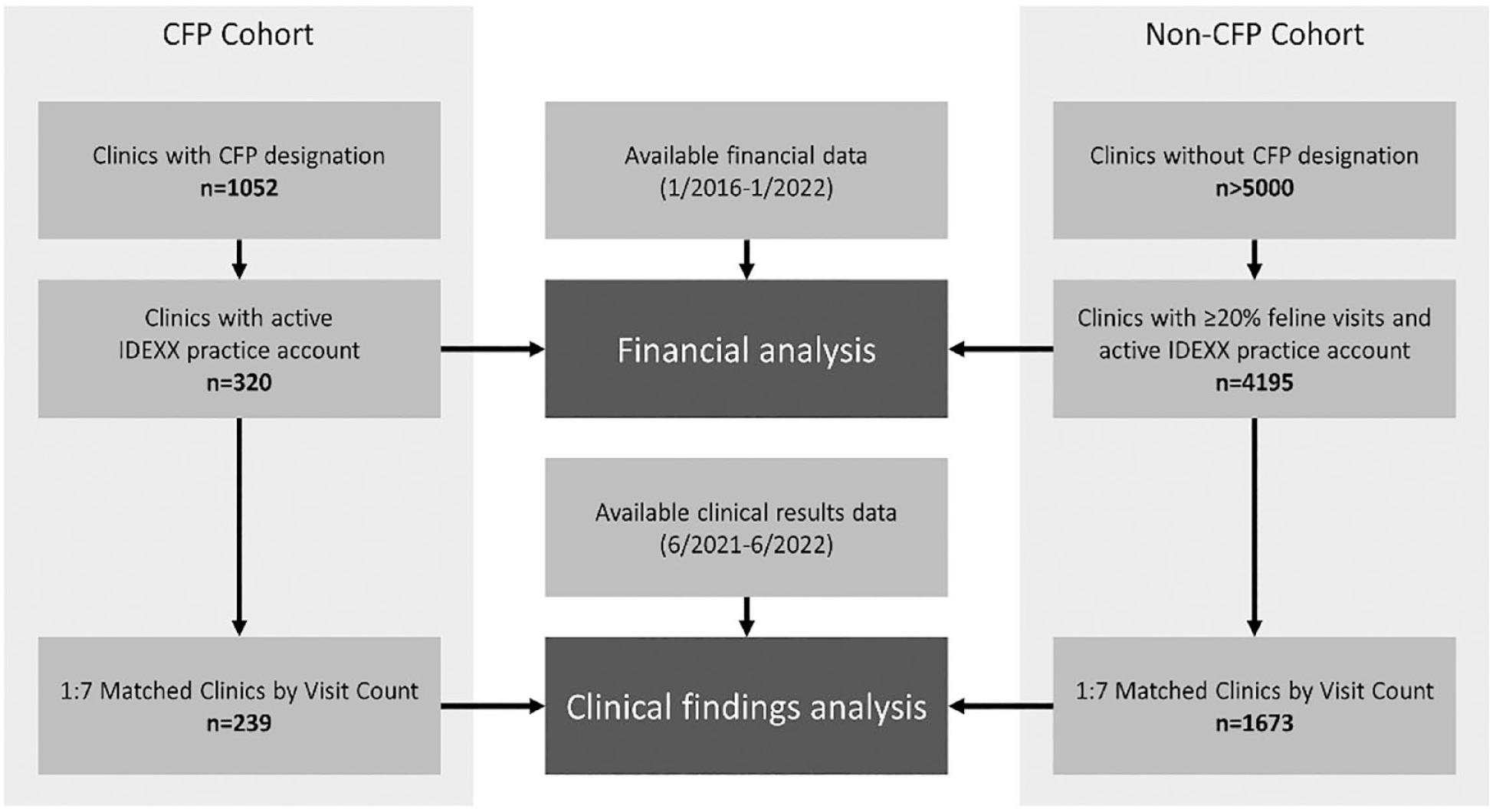
Diagram of clinic inclusion in the financial analysis and clinical findings analysis arms of the study
Study dates for inclusion of CFPs and non-CFP controls, criteria for non-CFP inclusion and type of diagnostic test results included in the financial analysis and individual results analysis arms of the study

CBC = complete blood count; CFP = Cat Friendly Practice; T4 = thyroxine; UA = urinalysis
Visit type classification
Data from PIMS in the USA were used to exclude ‘non-clinical’ (ie, interactions with only food or supply purchases, pre-approved prescription refills, boarding, grooming, etc) visits. Clinical visits were further divided into ‘wellness’ and ‘non-wellness’ based on the caregiver’s reason(s) for bringing the cat to the practice. ‘Diagnostic’ visits were any clinical visits with diagnostic test results.
Financial analysis
A financial analysis was completed for all clinical visits (wellness and non-wellness) and separately for wellness visits. Visits per year, proportion of visits that included any diagnostic test results (including any imaging, blood, fecal or urine tests), revenue per visit type and yearly revenue per patient were investigated for the 2018 and 2021 calendar years to control for COVID-19 pandemic-associated macroeconomic factors. The financial analysis was an exploratory analysis, and no statistical hypothesis was tested; therefore, no statistical significance was calculated.
Individual results analysis
Diagnostic test results included in the analysis were generated at reference laboratories or using in-clinic analyzers. Selected analytes from complete blood counts (CBCs), biochemistry, urinalysis and total thyroxine (TT4; cats >6 years only) were included in the individual results analysis. All other testing results were excluded from this study arm. The criteria for determining ‘clinically relevant’ abnormalities and grouping them by potential organ system were based on analyte patterns (Table 2). The lower and upper reference limits were based on reference intervals for the test methodology used to generate the result (see Table A in the supplementary material).
Criteria for findings and combinations of findings that identified ‘clinically relevant findings’ and allocated findings to potential system categories

Upper reference limit (URL) and lower reference limit (LRL) were determined by the test methodology
ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; BUN = blood urea nitrogen; GGT = gamma glutamyl transferase; HPF = high power field; RBC = red blood cells; SDMA = symmetric dimethylarginine; T4 = thyroxine; USG = urine specific gravity; WBC = white blood cells
Reference laboratory tests were performed according to standard protocols. Reference laboratory results were generated using XN or XT analyzers (Sysmex Corporation) for CBCs and Clinical Chemistry analyzers (Beckman Coulter) for biochemistry results. Urinalysis at the reference laboratories included a Multistix dipstick analyzed using an automated urine chemistry analyzer (Clinitek Novus or Advantus; IDEXX Laboratories) and manual sediment evaluation. In-clinic results were generated using hematology analyzers (ProCyte One ProCyte Dx or LaserCyte; IDEXX Laboratories) and chemistry analyzers (Catalyst Dx or Catalyst One; IDEXX Laboratories). In-clinic urinalysis could include any combination of dipstick analysis or automated analyzer (VetLab UA Analyzer; IDEXX Laboratories), manual sediment evaluation or sediment evaluation (SediVue Dx; IDEXX Laboratories) and manual specific gravity measurements.
To evaluate for bias in the comparison due to regional or practice setting, practices included in the individual result analysis were grouped into four US Census Bureau geographic regions. Rural-Urban Commuting Area (RUCA) codes (see Table B in the supplementary material) based on ZIP code and 2010 census information were used to identify the type of setting for each clinic. No statistical tests were applied for the exploratory analysis into geographic distribution or practice settings.
Statistical analysis for individual results analysis
The distributions of counts of clinical, wellness and diagnostic visit types were compared between cohorts of clinics using a Kolmogorov–Smirnov (KS) test. The distributions of visits per individual were compared by constructing a hurdle regression model consisting of a logistic regression predicting the odds of multiple visits based on clinic CFP status and a Poisson regression predicting the distribution of visit count given a follow-up occurred.
Each diagnostic visit was evaluated for clinical findings using the criteria described in Table 2. Visits that did not have all the results used in a finding definition were considered negative for that finding. The proportions of clinical visits in which each finding was observed were then calculated for each practice. A mixed effects logistic regression was fitted regressing these proportions on to the fixed effects of ‘CFP status’, and ‘Finding’ nested within ‘Organ/System’. A random intercept was estimated for each practice. Observations were weighted by the number of clinical visits occurring during the study window.
Test volumes of the four testing categories included in this study were calculated as a proportion of clinical visits for each practice. To estimate the CFP effect, a mixed-effects logistic regression was fitted with ‘category’, ‘CFP status’ and their interaction as fixed effects and ‘clinic’ as a random effect. Observations were weighted by the number of clinical visits occurring during the study window.
The proportions of diagnostic visits with one, two, three or four testing categories were calculated for each clinic. A logistic regression was used to regress these proportions on to ‘CFP status’, ‘Number of categories’ and their interaction.
Results
Financial analysis
The per feline visit practice revenue at 320 CFPs and 4195 non-CFPs was compared for 2021 and 2018. The average revenue at CFPs was 20% higher than at non-CFPs in 2018 and 17% higher in 2021 (Figure 2a). The average revenue at visits including any diagnostic testing was also higher at CFPs than non-CFPs in 2018 and in 2021 (Figure 2b).

Revenue associated with cat clinical visits during the calendar years of 2018 and 2021 at designated Cat Friendly Practices (CFPs) and non-CFPs. (a) Average revenue for all clinical visits during each calendar year. (b) Average revenue for clinical visits including any diagnostic testing. The results for CFPs are shown in black and for control practices in gray. The standard errors of all average revenue estimates are less than US$1
The type of visit, number of visits and inclusion of diagnostics at visits were evaluated as potential contributors to the differences in revenue between CFPs and non-CFPs. There were no differences in the proportion of wellness visits between the CFPs and non-CFPs (Table 3). Feline patients presenting to CFPs for wellness visits had an average of 1.95 visits/year compared with 1.75 visits/year for cats seen at non-CFPs in both 2018 and 2021 (Table 3). CFPs performed any diagnostic testing at approximately 12% more visits than non-CFPs for both total clinical visits and wellness visits specifically (Table 3 and Figure 3). Similarly, CFPs performed bloodwork at approximately 10% more total clinical visits and 9% more wellness visits (Table 3). CFPs also had higher annual revenue per feline patient for all visits and for diagnostic visits (Figure 4).
Visit breakdown for Cat Friendly Practices (CFPs) and non-CFP control practices during the calendar years of 2018 and 2021

Values in parentheses are 95% confidence intervals

Proportion of cats that had any form of diagnostics performed (a) at any clinical visit and (b) at wellness visits at designated Cat Friendly Practices (CFPs) (black) and at control practices (gray). Standard errors of all feline patient percentage estimates are <0.2%

Annual revenue per patient during the calendar years of 2018 and 2021 at designated Cat Friendly Practices (CFPs) and control practices. (a) Average annual revenue per feline patient for any type of clinical visits. (b) Average annual revenue for feline patients with any diagnostic testing during the year. The results for CFPs are shown in black and those for control practices are in gray
Individual findings analysis and diagnostic testing behavior
After matching, 239 CFPs and 1673 non-CFPs remained. Since only yearly cat visits were used for matching, information about geographical region and practice setting (RUCA classification) for practices is summarized in Table B in the supplementary material. There was a higher proportion of CFPs in the South and in metropolitan areas. A greater percentage of cat-only practices was observed in the CFP cohort than in the non-CFPs (8.4% vs 1.4%).
Similar trends in higher visits per cat and higher diagnostic inclusion for CFPs were noted in this study arm. No significant difference was found in the distribution of wellness visits (KS test, P = 0.063). The distributions of number of diagnostic visits per practice were significantly different (KS test, P <0.0001). Similarly, a cat seen at a CFP had higher odds of having more than one visit including bloodwork and/or urinalysis during the study period (odds ratio [OR] = 1.238, 95% confidence interval [CI] = 1.220–1.257). However, when only cats with more than one visit were considered, there was no difference in the number of repeat visits between the cohorts (OR = 0.992, P = 0.287).
There were also differences in testing behavior between the cohorts. CFPs performed testing at a higher proportion of visits for all analytes (Table 4). CFPs had higher odds of performing a CBC (OR = 1.50, 95% CI = 1.31–1.73), at least one test in the urinalysis category (OR = 1.74, 95% CI = 1.52–2.00), a TT4 measurement (OR = 1.44, 95% CI = 1.26–1.65) or at least one test in the chemistry category (OR = 1.40, 95% CI = 1.22–1.61). When diagnostics were performed, CFPs were more likely to include testing across multiple testing categories, with significantly lower odds of performing tests in only one testing category (OR = 0.863, P <0.0001) and significantly higher odds of performing testing from two (OR = 1.049, P <0.0001), three (OR = 1.079, P <0.0001) or four (OR = 1.713, P <0.0001) categories.
Visits (given as %) including testing that included a CBC, urinalysis, T4 and selected biochemical analytes at CFPs and non-CFPs

Data are mean (95% confidence interval)
ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; CBC = complete blood count; CFP = Cat Friendly Practice; GGT = gamma glutamyl transferase; SDMA = symmetric dimethylarginine; T4 = thyroxine; UA = urinalysis
CFPs identified a higher number of cats with abnormal results
To identify important abnormalities suggesting disease, criteria were applied to the results to determine clinical relevance and potential organ system or physiologic process (ie, system category) (Table 2). CFPs found a significantly higher number of cats with abnormal results associated with the endocrine, kidney and electrolyte system categories (P <0.0001 for each). The endocrine category findings were almost completely driven by TT4 concentrations in the borderline high range or above the URL. The distribution of test results also varied between the CFPs and non-CFPs. Testing done at CFPs was more likely to have a result within the reference interval for most analytes (Table 5).
Proportion of results within the reference interval for selected analytes at CFPs and non-CFPs

Data are %
ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; BUN = blood urea nitrogen; CFP = Cat Friendly Practice; GGT = gamma glutamyl transferase; SDMA = symmetric dimethylarginine; T4 = thyroxine
Discussion
Following 10 years of the CFP and CFC programs, abundant data have demonstrated the many benefits of these programs.8,20 –24 A previous study found that Spanish CFCs have a higher percentage of their revenue from feline patients, higher caregiver spending and a 12% higher average transaction value from feline patients. 22 This is consistent with our findings of higher average revenue per feline patient at CFPs for clinical visits for both years (Figure 2a) and a higher average revenue per feline patient for diagnostic visits (Figure 2b).
The higher rate of diagnostic testing and tendency towards more comprehensive testing at CFPs may contribute to this higher revenue. Although this study did not investigate why CFPs perform more testing, previous studies suggest that cat friendly interactions and handling may contribute. The CFP checklist and Cat Friendly Certificate Programs provide additional educational resources on the importance of laboratory testing, including minimum database testing based on life stage needs.34,35 In addition to the CFP’s ability to advise caregivers on how to minimize their cat’s stress before the veterinary visit, this added knowledge is expected to contribute to increased recommendations for testing and increased testing overall. In addition, CFPs have higher caregiver satisfaction, 21 which likely also contributes to an increased number of visits. Stress-reducing cat friendly interactions and handling in CFPs may increase patient cooperation during sample collection (eg, phlebotomy). 13 This study was not designed to test whether there was a causal relationship between CFP certification and higher testing rates, and the correlation could be due to other factors, or hospitals with higher rates of testing may be more likely to pursue CFP certification. Additional studies would be needed to compare testing behavior before and after certification to investigate any potential causal relationship.
Where abnormal test results were found, CFPs found a higher number of cats with abnormal results associated with endocrine, kidney and electrolyte systems. The early detection of disease in all life stages, 34 but especially in older cats, 35 provides opportunities for early intervention, decreased morbidity and improved quality of life. Normal test results in healthy cats can provide valuable individual baseline values that can be used to detect subtle trends in analytes and to interpret results in illness. The increased testing and likelihood of results within the reference interval at CFPs suggests increased screening with more opportunity for early intervention.
An unexpected finding was the lack of difference in the proportion or distribution of wellness visits between CFPs and non-CFPs (Table 3). We hypothesized that CFPs’ enhanced knowledge of cat friendly interactions and care and increased caregiver satisfaction 21 would result in higher inclusion of feline wellness visits. Routine vaccination and check-up were the most cited reasons for bringing cats to the veterinarian, 2 potentially driving wellness visits to both practice types. In addition, study inclusion was biased toward technologically advanced practices with veterinary software connected to their laboratory services provider. These practices may have increased access to more advanced reminder systems and/or caregiver education regarding the benefits of wellness visits. Other uncontrolled factors, such as regional and RUCA distributions, may have played a role if there were unexpected regional differences in recommendations for wellness testing or caregiver compliance with those recommendations. Despite the similar proportion of wellness visits, both the financial and individual results analyses showed that feline patients had higher average visits per year at CFPs than at non-CFPs. This suggests that when CFPs are able to interact with caregivers, they have increased success at conveying the benefits of ongoing care. Studies of CFCs found a similar increased frequency of patient visits per year 22 and 86% increased visits from better feline care, experience and CFP marketing. 21
Study limitations
Although the authors attempted to mitigate many factors that may bias the results, several limitations remain.
As with any retrospective study of this type, only tests that were both recommended by the veterinarian and agreed to by the caregiver could be considered. Veterinarian experience and caregiver socioeconomic factors may contribute to which diagnostics were ultimately pursued. Veterinary testing recommendations may be based on factors including feline-only practices, years since graduation, practice size and setting, and so on. The caregiver’s bond with their cat has been correlated with increased veterinary visits and an increased likelihood of agreeing to recommendations. 36 The caregiver’s preference for a more specialized CFP or feline-only practice may indicate more commitment to comprehensive care. This creates the potential for bias in the observed practice-type differences. In addition, the study design excluded practices not associated with IDEXX. This may have resulted in the underrepresentation of clinical findings, number of follow-up visits and/or testing by category in one or both cohorts.
Geographically, the study data showed more CFPs in the south and fewer in the northeast of the USA, with more CFPs located in metropolitan areas. Interestingly, the distribution of CFPs observed in this study does not reflect the registered CFP data available from the AAFP. This difference might in part be related to the study inclusion criteria, where clinics could only be included if they used IDEXX and had compatible PIMS. While our current observations did detect some differences in geographical distribution, no obvious major sources of bias were detected between CFPs and non-CFPs.
Our study found that CFPs perform more comprehensive testing; however, it is unclear if the location of a practice (rural vs metropolitan) or cat-only practices affected available diagnostic procedures or services. Interestingly, the strength of the human–animal bond and household income were inversely related, suggesting that the relationship between income, practice setting and caregiver willingness to agree to care is complex. 36 The financial analysis was not controlled for practice fee schedules, and differences in the cost of clinical visits, diagnostics or other services could have contributed to overall revenue differences. Future studies could investigate whether CFPs or cat-only practices were more likely to recommend diagnostics, had higher caregiver agreement to recommendations, or performed more advanced diagnostic procedures and/or therapeutics (eg, ultrasonography) compared with non-CFPs.
The time between visits was not considered when comparing the odds of an individual patient having more than one visit. Since the study period was restricted to 1 year, it is possible that the increased visits at CFPs may be due to earlier follow-up.
Lastly, clinical information, including reason for diagnostic testing and history, was not available. Whether a finding influenced diagnosis or management cannot therefore be established.
Conclusions
The first 10 years of CFPs and CFCs have provided support for the benefits associated with these programs to practice finances, veterinary teams, caregivers and patients. The present study has demonstrated that CFPs may have unique diagnostic testing behavior, including increased laboratory testing and increased detection of clinically relevant diagnostic results. Taken together with previous studies, these data support the need for additional investigation into the benefits of CFP status, while at the same time, supporting the need for more interest and the pursuit of CFP status in veterinary practices.
Supplemental Material
Table A:
Reference intervals for analytes tested at IDEXX Reference Laboratories and in-clinic results using IDEXX Catalyst Dx or Catalyst One.
Supplemental Material
Table B:
Geographic and census classification of practices for the Cat Friendly Practice (CFP) and non-CFP cohorts.
Footnotes
Acknowledgements
The authors thank Heather O’Steen, CEO, AAFP, for her assistance with the development of study goals, provision of AAFP CFP information and assistance with manuscript review.
Correction (December 2023):
The paper has been updated to correct the corresponding author's address.
Author note
Preliminary data from this study were presented at the AAFP 2022 Annual Conference in Pittsburgh, PA, under the title of ‘Cat Friendly Practice by the Data’ by Drs Kelly St Denis and Wade Burton.
Supplementary material
The following files are available as supplementary material:
Table A: Reference intervals for analytes tested at IDEXX Reference Laboratories and in-clinic results using IDEXX Catalyst Dx or Catalyst One.
Table B: Geographic and census classification of practices for the Cat Friendly Practice (CFP) and non-CFP cohorts.
Conflict of interest
KSD is a past President of the AAFP (2020–2021) and AS is currently a Director on the AAFP Board (2021–2023). WB, CD and HM are full-time employees of IDEXX Laboratories.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.