
Abstract
Practical relevance:
The ‘2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques’ (hereafter the ‘Cat Friendly Veterinary Interaction Guidelines’) support veterinary professionals with feline interactions and handling to reduce the impact of fear and other protective (negative) emotions, in so doing enhancing feline welfare and In implementing these Guidelines, team satisfaction and cat caregiver confidence in the veterinary team will increase as the result of efficient examinations, better experience, more reliable diagnostic testing and improved feline wellbeing. Veterinary professionals will learn the importance of understanding and appropriately responding to the current emotional state of the cat and tailoring each visit to the individual.
Clinical challenges:
Cats have evolved with emotions and behaviors that are necessary for their survival as both a predator and prey species. A clinical setting and the required examinations and procedures to meet their physical health needs can result in behavioral responses to protective emotions. Cat friendly interactions require understanding, interpreting and appropriately responding to cats’ emotional states and giving them a perceived sense of control while performing the required assessment.
Evidence base:
These Guidelines have been created by a Task Force of experts convened by the American Association of Feline Practitioners and the International Society of Feline Medicine, based on an extensive literature review and, where evidence is lacking, the authors’ experience.
Endorsements:
These Guidelines have been endorsed by a number of groups and organizations, as detailed on page 1127 and at catvets.com/interactions and icatcare.org/cat-friendly-guidelines.
Keywords
Introduction
In 2011, the American Association of Feline Practitioners (AAFP) and international Society of Feline Medicine (ISFM) published the ‘AAFP and ISFM Feline-Friendly Handling Guidelines’ 1 and in the interim the understanding of what is ‘cat friendly’ has expanded considerably. As numerous studies have advanced our knowledge in this field, these Guidelines replace the previous handling guidelines. A cat friendly approach encompasses both non-physical and physical interactions, which in a veterinary context usually includes ‘handling’. Mod erating the impact that non-physical interactions (eg, visual, auditory, olfactory) have on the cat is equally as important as considering interactions involving physical contact. Hence, there is the new name of ‘Cat Friendly Veterinary Interactions’ for these Guidelines. (Additional terminology is listed in the ‘definitions’ box on page 1095.) The other notable change in this set of Guidelines reflects concerns around the concept of restraint. The former guidelines used the term ‘minimal restraint’, but restraint implies a lack of control or consent on behalf of the cat, and there is evidence to prove that interactions without restraint are more efficient and effective. 7 Understanding, interpreting and appropriately responding to cats’ emotional states and giving them a sense of control through cooperative care are fundamental to being cat friendly.
Because cats are non-verbal mammals, we rely on their proxies to understand what causes patient distress surrounding veterinary appointments/visits. Proxies include veterinary professionals, animal welfare researchers and cat caregivers. A survey of over 1000 caregivers indicated that most cats (88.7%) had impaired welfare at all stages of the visit, including before and after the appointment, 8 as well as during the veterinary examination. A further, very recent survey study of caregivers reports that travel to the practice, the waiting room and examination itself are the most stressful events for the cat, with one-third of respondents indicating that witnessing their cat’s stress discouraged them from bringing their cat to the practice. 9 In both surveys, the caregivers reported that they, themselves, experienced stress.8,9 Caregiver stress influences the perception of their cat’s stress. 10 Surveyed veterinarians and animal welfare researchers also determined that feline welfare was impaired, starting at home and during practice visits. 11 The key stress-causing factors that were suggested to impair welfare in the clinical setting were auditory and olfactory stimulation, lack of analgesia and the use of restraint. 11 Those surveyed also said that the majority of factors impairing welfare in the veterinary practice and home can be improved through practical approaches, including recognition of species-specific signs of fear and pain, use of cognitive techniques to prepare cats prior to veterinary visits, and use of food to cue positive (engaging) emotions as well as to provide positive reinforcement of specific desired feline behaviors during the visit. 11

Adhering to these ‘Cat Friendly Veterinary Interaction Guidelines’ reduces distress for cats, caregivers and veterinary professionals. This is critically important. Cats have good long-term memory and can remember a single event, such as a negative experience during a veterinary visit. 12 Our interactions, therefore, not only affect the cat at that time but will also influence their emotional responses and behaviors at subsequent veterinary visits.12-14 Classical conditioning will lead to emotional associations with the veterinary experience even when there has not been any one specific negative experience. For example, if a cat is painful or fearful during a veterinary visit, which may be as a result of their physical health condition, that protective emotional bias will become associated with the veterinary context and the cat may, therefore, respond protectively at future visits. Simply avoiding obvious negative interactions, such as excessive restraint or scruffing, is not enough. It is important to enhance a positive emotional bias.


Cat friendly interactions involve considering emotional and cognitive health throughout the journey of the veterinary visit, even before leaving the patient’s home. Mounting evidence suggests that first veterinary visits can impact a young animal for life. A negative veterinary experience in young puppies can impact their long-term welfare, leading to chronic fear or anxiety regardless of the environment; the same is likely to be true in kittens. 15 The investment to incorporate these Guidelines into practice also enhances appointment efficiency7,16 and human safety.1,17-20 See Box 1 for a summary of the wide-ranging benefits of cat friendly interactions, and always keep in mind that:
✜ Working cooperatively with cats increases human safety by reducing the intensity, and thus minimizing the impact, of fear and other negative (protective) emotions. Restraint increases negative emotions and undesirable behavioral responses.
✜ With consistent positive handling, cats become safer and easier to work with, which means that appointments can be completed more quickly and with minimal handlers.

Feline behavioral needs during human-cat interactions
Our interactions with cats must take into consideration species-specific behavior as well as individual differences.
The cat as a species
Cats are solitary survivors and territorial animals who need a sense of control, safety, choice and familiarity, not only in their physical environment but also in their social environment.

Examples of places and opportunities for cats to hide during their visit. (a) High-sided cat weighing scales, (b) blankets and towels, (c) igloo beds or (d) high-sided beds, with or without an added blanket/towel, are all excellent options and items that can easily be washed and dried in the veterinary practice. (e) An additional towel or blanket ‘roll’ draped over the neck can also give cats a sensation of being hidden. Images courtesy of Kelly St Denis (a,b,e) and Ilona Rodan (c,d)

(a,b) A veterinary team member approaching a cat in their carrier with a soft hand; note the curved fingers. Images courtesy of Ellen Carozza

Feline facial glands are preferred areas of touch for the head region. Image courtesy of International Cat Care
The individual cat
An individual cat’s sociability toward humans, other cats and other species, and their ability to cope in different situations is influenced by a number of factors, including genetics, their parents’ sociability to humans, the queen’s health and experiences during pregnancy, and the cat’s own experiences. If the father is bold or friendly toward people, the probability that the kittens will respond well to socialization increases. 40 The queen impacts kittens genetically, prenatally and through her behavior and interactions with them after birth. Prenatally, kittens are negatively impacted if the queen is malnourished, suffering from physical illness, or has a negative emotional bias during pregnancy. Her emotional bias will be influenced by her general emotional health as well as any specific experiences during her pregnancy and can likely cause epigenetic changes and influence physical and behavioral development of the kittens. 41
Kitten experiences between 2 and 9 weeks of age can have a significant impact on the behavior of the individual throughout life.40,42 If handled positively and frequently during this time period, and by a diverse range of humans including children, the kitten will be more likely to develop into a cat who is more amenable to handling and less fearful of people, including those who are unfamiliar.40,42
In contrast, cats who are not appropriately introduced to people early in life will have a significant risk factor for being more fearful, including during veterinary visits. 40 While learning is most influential during these early weeks of development, kittens will continue to learn throughout their lives. Age of weaning may have an impact on behavior, but further work is needed to ascertain this.43-46
Above all, handling needs to respect natural feline behavior and all interactions need to be considered from a feline perspective. An adverse experience during a veterinary visit, such as tight restraint or triggering of pain or fear, can lead to the cat becoming highly reactive at future visits. If not well socialized to humans as a kitten, it may only take a single negative experience for a cat to become wary of humans vs many positive ones to become friendly toward them.15,47 Thus, even in cat friendly environments, many cats who were not adequately and appropriately socialized to humans and habituated to human environments can benefit from the use of anxiolytics to reduce their protective emotional bias during veterinary visits. The negative factors that can impact a cat’s emotional state at the veterinary practice are numerous and some examples are listed in Box 2.

The emotional state
The information contained in these Guidelines regarding emotional motivations and the behavioral responses to those emotions is based on the work of Jaak Panksepp and on the recently described Heath Model of emotional health.49-51
Both positive and negative emotions can occur in relation to the veterinary visit and recognizing these emotions is important in tailoring the approach to the individual cat (Algorithm 1). Sarah Heath, one of the Task Force members, has developed new terminology in relation to emotional health in order to explain the purpose of the emotional motivations and the behavioral responses they lead to. 5 This terminology, and the Heath Model explanatory approach to emotional health, 50 are being used throughout these Guidelines.
Although the scientific terms for emotions are positive and negative, the emotional motivations aid the cat’s welfare and these terms may erroneously imply that the emotions and subsequent behaviors are good or bad. Heath, therefore, refers to positive emotions as ‘engaging emotions’. These are emotions that cause the cat to actively seek out something that results in benefit to their survival; an example would include desire-seeking in relation to food, attention or comfort.
Negative emotions occur in environments and with interactions that are perceived to be threatening, and their goal is self-protection to enhance the cat’s survival. 51 Heath uses the term ‘protective emotions’ to emphasize why they occur.5,50 Although a predominantly protective emotional state in a feline patient can lead to behavioral responses that are considered undesirable, the cat is responding to their emotions by employing behaviors that are designed to protect them and ensure their survival in the face of what they perceive as a threatening experience. To this end, the terms ‘aggressive’ and ‘fight’ are not used within the Heath Model, in the context of cat handling. These behaviors are referred to as repelling responses, and have the aim of increasing distance from, and decreasing interaction with, a potential threat.5,50
It is important that veterinary professionals use terminology that reinforces understanding of the underlying emotions that lead to cats’ behavioral responses; hence these Guidelines emphasize the terms ‘protective’ and ‘engaging’ emotions. Use of negative terminology when describing feline patients, such as evil, nasty or aggressive, erroneously labels them and can negatively impact our response, leading to a lack of sensitivity among team members toward cats in general or to individual feline patients. Negative terms such as these also prevent us from understanding the feline perspective, identifying underlying stressors and establishing what works to minimize or resolve the situation rather than exacerbate it. Behavioral responses are driven by the cat’s emotional state at that specific point in time (Algorithm 1). A combination of the environment, interactions and the individual cat’s previous experiences influence the immediate emotional state.

Cats can experience more than one emotion at any one time, and positive (engaging) and negative (protective) emotions can be triggered by the same stimulus or during the same experience, resulting in emotional conflict. 5 A good example is the offering of a treat to a highly fearful feline patient. The treat will trigger an engaging emotion, but if it is being offered by a person who triggers a protective emotion, the resulting emotional conflict can be detrimental to the cat and negate any potential benefit of offering a treat. 6 If a treat is to be offered, it should be done passively and placed on the floor or table, rather than given directly from the human hand, in order to reduce the potential for inducing conflict. The cat then is able to choose whether to take the treat and will only do so if the engaging emotional response to the treat is the predominant emotion they are experiencing (S Heath, personal communication).
Carrier training, cooperative care, and a cat friendly veterinary environment and interactions that help cats feel safe, greatly increase the potential for feline positive (engaging) emotional states. For more information on how the veterinary practice environment can be manipulated to minimize feline patient distress, see the accompanying ‘2022 ISFM/ AAFP Cat Friendly Veterinary Environment Guidelines’ 60 (hereafter the ‘Cat Friendly Veterinary Environment Guidelines’).
Although it is often easier to work with cats in a positive emotional state, some kittens and young confident cats are very active, which can make it more challenging to complete the necessary examinations and treatment. In the Heath Model there is an emphasis on the equal significance of emotional valence (the extent to which an emotion is positive or negative) and emotional arousal (the intensity of the emotion) in terms of the emotional health of the individual (see supporting material at bit.ly/ JFMSCatFriendly).61,62 The wriggly kitten illustrates the importance of considering both emotional arousal and the valence of an emotional stimulus. Too much emotional arousal, even when it is engaging in nature, can lead to behavioral responses that make handling prob-lematic. 63 The aim, therefore, is to encourage a positive, engaging emotional bias while keeping levels of emotional arousal low.
It should also be remembered that positive emotions can lead to behavioral responses that can be problematic if they occur in an inappropriate context. One example is the emotion of desire-seeking, motivating the behavior of predatory play. If a caregiver encourages predatory play through the use of hand play, it can lead to kittens or cats attempting to play with the hands of veterinary team members during physical interactions. To prevent these types of problems, caregivers should be encouraged to engage in object play with their kittens, and direct playful interactions toward appropriate toys. Object play may be used to facilitate veterinary visits, but it is important to avoid high levels of arousal.
Positive (engaging) emotions
The desire-seeking system is the positive emotion most commonly seen in the veterinary practice (Box 3). This emotional state motivates cats (and other animals) to move to locations where they are more likely to find resources for survival, such as food, water, shelter, warmth or coolness. 52 It is also the emotional system that is triggered in reward-based or positive reinforcement learning and training, such as carrier training. 53
Negative (protective) emotions
Negative or protective emotions that can be relevant to feline behavior in the veterinary practice are fear, anxiety, pain and frustration. When we identify the cause of protective emotion(s), especially early on, we can often minimize the cat’s perception of threat, and sometimes even activate positive emotions instead. 64
✜
There are four primary behavioral responses to protective emotions. Using the Heath Model terminology, these are referred to as inhibition, appeasement, avoidance and repulsion, and they are of equal significance when considering feline emotional health and welfare. 5 Within the context of the veterinary experience the three responses that are of most importance are inhibition, avoidance and repelling behaviors.


Example of an inhibited cat. The cat is passively gathering information, with eyes half-shut and ears rotated laterally. Image courtesy of Sarah Heath

Splayed whiskers is one of the signs a cat may display when experiencing protective emotions. Image courtesy of Ilona Rodan
The selection of the response is based on the individual cat, their previous and current experiences, and the context in which they experience the emotion. 51 Their selection is not directly related to the intensity of the emotional response and, therefore, all three responses are of equal importance when assessing a patient’s emotional health. Inhibition is a passive response and is often not recognized by people interacting with the cat (Figure 4; see also Video 2 in the supplementary material). As such, the inhibition response may not succeed in protecting the cat from the perceived threat and the cat remains in a negative (protective) emotional state. When this happens, the cat must turn to one of the other responses – avoidance (escaping from the perceived threat) or repelling the perceived threat (eg, growling, hissing, striking, biting). These behaviors can have more significant consequences for veterinary professionals, making examination and any necessary procedures more difficult to complete. There may also be an increased risk of cat or human injury.17,51 See Box 4 and Figure 6a-c for signs of fear-anxiety.


Behavioral responses to protective emotions are shown in images (a-c), while image (d) shows a behavioral response to engaging emotions. If avoidance and inhibition responses have not been successful for the cat, this increases the probability that repelling responses will then be selected. In this case, an anxiolytic within a treat was offered passively and the cat was left alone for 2 h, which was successful (see image d). The alternative would have been to sedate the cat for the procedure to be carried out, or send the cat home with advice for the caregiver to carry out carrier training and administer anxiolytic medication (eg, gabapentin) before the next visit. Images courtesy of Ilona Rodan

Young cat becoming frustrated in relation to their desire-seeking system due to confinement and the presence of the soft collar. Strategies to prevent frustration aim to increase fulfillment of the desire-seeking system; for example, through providing social interactions at consistent times by one or two veterinary team members and, for some patients, allowing the caregiver to visit. Consistency in the timing of feeding and playing is also helpful; remove the soft collar for feeding. If the cat is hospitalized for more than 24 h, ensure that all environmental needs are met, either in the cage or a small room environment (see the accompanying Cat Friendly Veterinary Environment Guidelines). 60 Image courtesy of Sam Taylor
Every cat friendly visit should be framed around providing the cat with a sense of control, emphasizing positive experiences while lessening the potential for negative experiences through alternative approaches. As addressed in these Guidelines, key areas of focus for ensuring this sense of control include developing a plan in advance based on the cat’s history and preferences, minimizing potential physical and emotional disturbances, appropriately managing introductions and handler interactions, and allowing the cat to move and position themselves in ways that are most comfortable for them.
For these strategies to be effective, examinations and procedures should take place in quiet and secure enclosed spaces (eg, an examination room) where the cat has the opportunity to move freely without any form of physical interaction, if required – for example, if the cat is becoming aroused and needs a break. Releasing the cat must always be an option, without putting anyone, including the cat, in danger. The examination room has been demonstrated to be the most appropriate location for physical examinations to be per-formed. 67 Unless insurmountable barriers exist, any additional outpatient procedures required should also be performed in the examination room, to increase the accuracy of certain diagnostic tests, to reduce sensory arousal and exposure to unfamilar animals, and to avoid separation of cats from their caregivers. 67
All veterinary visits are likely to induce protective emotions to some degree, as these are natural and necessary responses to experiences the cat perceives as threatening. It is important to minimize the triggering of these emotions, including fear-anxiety, pain and frustration, and to enable the cat to select appropriate behavioral responses. For example, the provision of places and opportunities to hide enables the successful selection of an avoidance response. When protective behavioral responses occur, it is essential for the veterinary team to recognize them and ensure that they react appropriately. The aim of the cat’s behavioral responses to protective emotions is to reach a physical and emotional place of safety and security, and it is the job of the veterinary team to facilitate this. Cats become stressed when they are not able to respond successfully to protective emotions and resolve them. Cat friendly interactions aim to enable the cat to cope and thereby prevent them from becoming stressed. The overarching objective is to protect cat welfare in the current moment and encourage ongoing improvement during future visits.
When cats are showing low-intensity behavioral responses of inhibition and avoidance (passive eye avoidance rather than fleeing), 5 it is often possible to ensure success through simple measures such as allowing the cat to hide in the bottom of their carrier, using towels or a high-sided cat bed to encourage a sensation of being hidden and protected (see Figure 1), and maintaining the cat’s sensation of comfort by allowing them to select their chosen location for examination. This is discussed further in ‘Principles for interacting with cats’.
When repelling behaviors are the primary response, it can be more difficult for the cat to use them successfully without risking injury to themselves or the veterinary team members. In these situations it is more appropriate to select chemical restraint to enable handling to continue without intensifying the protective emotional state and resulting physiological stress.68,69 In some cases, chemical restraint can be employed in the moment, but this may not be appropriate if the cat has already reached a state of extreme emotional arousal. In these cases, and if the procedure is not urgent, the caregiver can be asked to take the cat home and schedule a return visit. An appropriate approach to chemical restraint can then be discussed and anxiolytic medication dispensed to be given at home before the visit, with the caregiver also encouraged to provide carrier training, if possible; if still needed, suitable chemical restraint can be employed on arrival.
If rescheduling is not an option, it is necessary to minimize arousal by leaving the cat in a quiet and secluded location for at least an hour, where possible, before administering chemical restraint. In extreme cases it might be necessary to momentarily use higher levels of handling to deliver required medications for chemical restraint (eg, restraint cages for feral cats; loose towel wraps or coverage with blankets in the bottom of the carrier for companion cats), always ensuring that all required supplies are immediately available so that the handling time is the absolute minimum necessary to administer the medication.
When caregivers are resistant to chemical restraint or rescheduling the appointment, the veterinarian must advocate for the cat’s welfare and explain that this approach is necessary to reduce the risk of negative emotional associations with the veterinary visit, which can seriously threaten the ability to provide quality veterinary care now and in the future. Care-givers can also be offered advice and materials to assist them with training their cat at home for carrier travel and handling in order to improve responses during future visits (see later). 16
It is important to remember that protective emotions are normal when they are justified. While avoidance behaviors and repelling responses may be easy to identify and are more commonly recognized as being problematic, the response of inhibition is also associated with protective emotion and must be recognized as such. Inhibition can certainly make cats easy to handle and work with, but those showing this response are indicating that they feel the need to protect themselves. Thus, they too are in need of assistance through alternative approaches.
Given this focus on ‘cooperative care’ (see ‘Cooperative care, the future of cat friendly’), handling methods that cause discomfort or elevate a cat’s fear or frustration levels should be avoided. Studies have demonstrated that cats examined with minimal handling show fewer negative responses than cats handled with more heavy restraint methods (Figure 8).7,70,71 A survey of Canadian and American veterinary teams found that most respondents reported using a range of handling methods, with both calm and fearful cats, aimed at minimizing restraint and improving the cat’s experience during examinations and procedures. 70 However, many respondents also reported routine use of heavy restraint (eg, full body restraint, scruffing) with calm and fearful cats, and a majority reported using these approaches with cats showing repelling behaviors. While heavy restraint and scruffing are still commonly used with cats in veterinary practice,9,70 cats show signs of fear-anxiety during such interactions, which should be avoided to safeguard feline welfare.
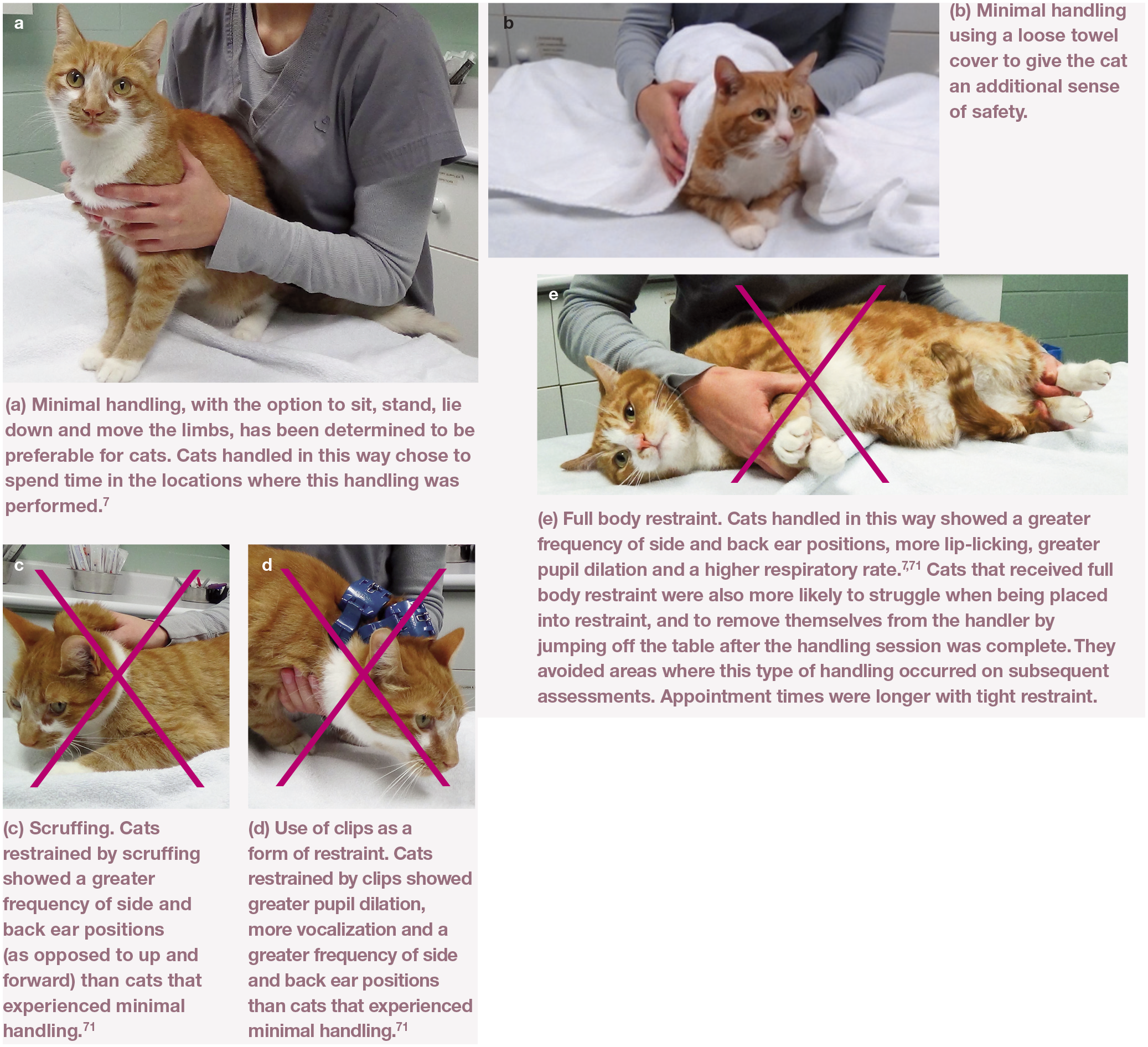
Images from Couture et al 72 provide evidence to support the benefit of minimal feline handling (a,b) over restraint. Blinded observers reviewed video clips and pictures, including those shown here. The methods of restraint illustrated in images (c-e) resulted in increased objective indicators of fear and aversion.7,71 Images courtesy of Lee Niel
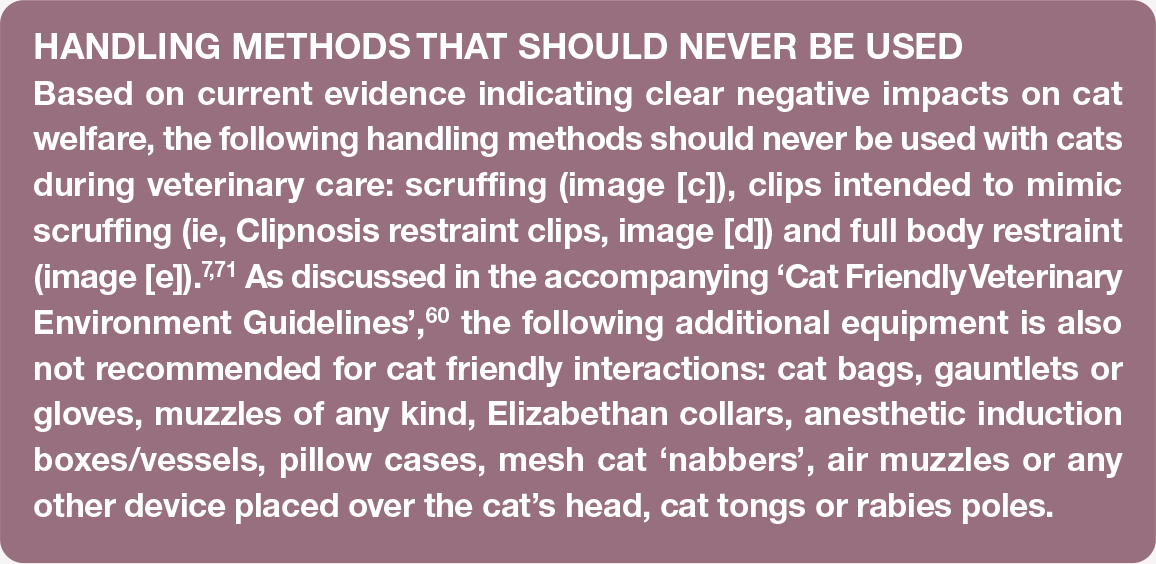
One study compared the responses of cats that were minimally handled with cats handled with either full body, scruff or clip restraint; 71 the investigators found that all methods of restraint resulted in increased objective indicators of fear and aversion in comparison with minimal handling, and that responses were greatest for full body and clip restraint, followed by scruff restraint (see Figure 8). These heavy restraint methods not only impair cat welfare in the short term, but the effects of repeated use are also likely to be cumulative over time and increase handling aversion and welfare impairment, potentially leading to repelling behaviors in the longer term. Furthermore, a survey of caregiver perceptions of different cat handling methods determined that a majority of respondents disagreed with use of these restraint methods for their own cat. 72
Preparation prior to visiting the veterinary practice Why is this so important to interactions?
Events that precede entry to the veterinary practice commonly increase feline and caregiver distress and the veterinary team’s difficulties in interacting with cats.8,9,11 Feline distress resulting from the emotions of fear-anxiety, pain and/or frustration can be associated with a lack of control getting into the carrier, carrier confinement, carrier instability and movement during the trip, and the transportation itself. Cats with prior negative carrier experiences or other distress triggers at home (eg, intercat tension, inability to perform normal behaviors, caregiver-cat relationship breakdown due to undesired feline behaviors) need additional attention to ensure positive experiences both prior to and during veterinary interactions, and to minimize ‘stressor stacking’ (see image and further discussion in the accompanying ‘Cat Friendly Veterinary Environment Guidelines’ 60 ).
If caregivers are not educated about carrier training and transport (Box 6), their interactions when moving cats into the carrier and during transportation can increase feline distress prior to arriving at the practice. Over 75% of caregivers report they have not been given travel advice, 9 so this is an area that requires improvement from the veterinary team. Caregiver personality, emotions, moods and behaviors also influence feline patients.73-75 Caregivers are often anxious about various issues – getting their cat(s) to the practice, not knowing how their cat will behave at the practice, an unexpected diagnosis or inability to resolve health issues, and unintentionally harming the relationship they have with their cat. Cats recognize human and conspecific emotions by integrating visual and auditory signals, and change their behaviors based on the perceived emotion. 76 Since caregiver and feline distress are so intertwined, education about carrier training and transport may additionally help reduce caregiver anxiety.
Caregiver role
Caregivers may feel embarrassed by their cat’s response to handling or frustrated if postponement of a procedure is recommended. It should be explained why the cat is likely responding with protective behaviors, emphasizing the cat is not being ‘naughty’, but reacting based on fear-anxiety, pain and/or frustration, and influenced by previous negative experiences in the clinical setting. In addition to teaching the cat to be comfortable in the carrier and administering pre-visit anxiolytics, caregivers can also provide favorite treats to be made available to the cat at the practice to help cue an engaging emotional bias. It can be explained that cooperative care and specific teaching, including carrier training (Boxes 6 and 7), as well as use of pre-visit anxiolytic medication, make visits easier for both caregiver and cat, with the practice and caregiver working as a team to improve the cat’s experience and behavioral response.
Behavioral modification using positive reinforcement to teach cats to voluntarily enter and calmly travel within their carriers is beneficial to feline welfare.16,18,53 The benefits of carrier training (Figure 9) extend to increased positive emotions, as demonstrated by increased searching for food rewards during the veterinary visit and significantly shortened examination times. 16 Behavioral modification using positive reinforcement training prior to the veterinary visit is the gold standard. However, if caregivers are unable or unwilling to undertake this, the advice should be, as a minimum, to prepare the carrier and car with synthetic feline pheromones 15 mins in advance, and to keep the carrier covered and stable during transport. The Center for Pet Safety (centerfor-petsafety.org) recommends that most carriers be placed on the floor behind the front seats, including all hard-sided plastic carriers; details of which carriers have passed crash testing and can be seat-belted in the back seat are also provided. These interventions to improve cats’ experiences with the carrier and during travel have been shown to help reduce both the time required to reach sedation and the induction dose of propofol in cats requiring general anesthesia. 29 Caregivers can use positive reinforcement training at home to teach their cats to enjoy handling that mimics or approximates that conducted during health examinations by the veterinarian. See ‘Cooperative care, the future of cat friendly’ for further information.


Carrier training case study, providing a clear example of how prior negative experiences can influence veterinary interactions, and how the veterinary team can support caregivers to train cats, of any age, to voluntarily enter the cat carrier. Note the facial expression indicating discomfort, which was due to musculoskeletal pain not being well controlled. Image courtesy of Ilona Rodan
Client education
Providing caregivers with a supportive plan or checklist to help them be part of the solution can minimize their anxiety as well as help the cat. This should encompass: information on carrier selection and possible anxiolytic and/or analgesic medications; training advice for calm carrier travel and mini-health examinations at home; and practical tips such as bringing one or more of the cat’s favored items to the appointment, as well as tips to help the caregiver stay calm themselves (making sure they have enough time to travel to the practice, using relaxed body language around the cat, etc).
Practices can use the resources highlighted in Box 6 to facilitate client education about carrier training and transport, adding this information to websites, as well as distributing via social media and handouts. The veterinary team should also take every opportunity to verbally emphasize the cat and caregiver benefits and explain that all training must be positive in order to reinforce desired behaviors. Techniques can be demonstrated by team members with the appropriate training expertise.
Pre-visit anxiolytics and other useful pharmacotherapy
Pharmacotherapy can significantly lessen a cat’s protective emotional bias and resulting potential for distress. It does not replace positive modifications to minimize distress during feline interactions, and so it must be used concurrently when indicated. Cats with previous negative veterinary experiences, those not habituated to handling and those described as having a very anxious or fearful temperament should receive an anxiolytic before the visit.
Information on anxiolytics for use prior to the veterinary visit, including doses and best timing of administration, is given in Table 1. By recording in the cat’s medical record (in a pop-up or easily viewed location) caregiver education, anxiolytics or analgesics recommended pre-visit, the cat’s preferences and the cat’s emotional state, best practices for each cat can always be followed.
Examples of sedative/anxiolytic drugs that can be used prior to veterinary visits
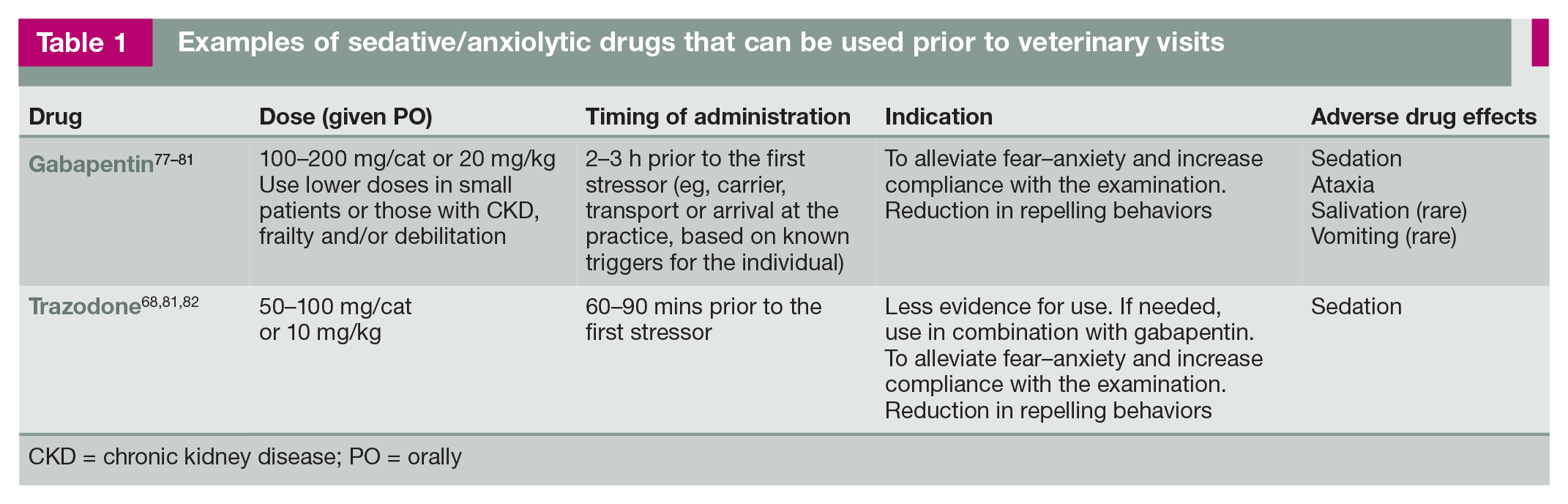
CKD = chronic kidney disease; PO = orally
Anxiolytics
Gabapentin is an excellent feline anxiolytic and more effective than other pharmaceuticals and nutraceuticals, as demonstrated by reduced distress during transport and examina-tion.77-79,83 Gabapentin administration also improves the quality of medical care, increasing the ability to perform a complete examination that may otherwise be impossible in cats that display intense fear-associated behav-iors; 77 such behaviors, which can lead to injury, are reduced with a single dose of oral gabapentin. 77 Researchers have identified the lowest stress scores to be 2-3 h after gabapentin administration,77-79 with the studied and recommended dose being 20 mg/kg78,79,83 or 100-200 mg/cat. 77 Gabapentin is 100% renally excreted, 78 and significantly higher levels of serum gabapentin are found in cats with IRIS stages 2 and 3 chronic kidney disease (CKD) as compared with cats without renal disease. 80 It is suggested to use 50% of the lower doses of gabapentin in cats with reduced renal func-tion.77,80 Gabapentin is safe to use in cats with systemic illness, including hyperthyroidism, due to its minimal cardiovascular effects, and can facilitate the performance of procedures such as blood pressure measurement and phle-botomy.80,83 Caregivers should be warned that cats may be ataxic after receiving gabapentin and this effect can last for several hours after the cat is discharged. Therefore, cats should be kept indoors for at least 8 h and, for some, preventing access to high perches/stairs may be sensible to avoid falls.
A small study has evaluated pregabalin in cats at 5 mg/kg and 10 mg/kg doses and determined that signs of anxiety and the fear associated with car transportation were reduced. 84 Additionally the pharmacokinetics of pre-gabalin have been investigated, showing no safety concerns with doses up to 7.5 mg/kg. 85
Trazodone is a sedative that has been recommended for use as a single agent or in combination with gabapentin. Studies provide conflicting information about efficacy and sample sizes were small, making it challenging to draw firm conclusions.68,82 Trazodone has minimal cardiovascular effects and so is safe for use in cats with systemic illness. 81
No research on the use of benzodiazepines as a pre-visit anxiolytic is available. Dis -inhibition and repulsion can occur with some benzodiazepines (eg, diazepam, alprazo-lam)86,87 and oral diazepam has been associated with hepatotoxicity. 88 Acepromazine is not an anxiolytic and can also cause disinhibition and repelling behaviors.
Anxiolytics are most effective when administered prior to patient arousal and best given in the home environment. Anxiolytics can even be administered prior to general anesthesia as fasting times have been shortened to 3 h and medication within a small-volume treat does not impact anesthesia. 65 Note that a similar approach can also be used for hospitalized cats undergoing planned procedures or examination, and to reduce anxiety in hospitalized and boarding patients; lower doses may be considered where repeat usage is required. Encourage veterinary teams and caregivers to use a hands-off approach to medicating the cat to further reduce anxiety and improve the efficacy of the anxiolytic medication (see Video 3 in the supplementary material).
Motion sickness medication
For cats who experience signs of motion sickness, such as lip-licking, drooling or vomiting, maropitant can be prescribed 4 h prior to trav-el. 89 There are no contraindications to its use in combination with anxiolytics. Fasting the cat for 2-3 h before travel is also advised.
Analgesia
Degenerative joint disease (DJD), which includes osteoarthritis (OA) and spondylosis, and periodontal disease are common chronic pain conditions in cats.90-92 In addition, the possibility of a range of other sources of acute or chronic pain should always be considered if a cat is presented as being challenging to handle during a veterinary visit. Additional analgesics may be prescribed to administer prior to visits to reduce pain and to prevent protective emotions escalating during travel and examination. Appropriate ongoing chronic pain management should also be provided. See the ‘2022 AAHA Pain Management Guidelines for Dogs and Cats’ and ‘2022 ISFM Consensus Guidelines on the Management of Acute Pain in Cats’ for further information.93,94
Cooperative care, the future of cat friendly
Cooperative patient care involves utilizing a combination of classical conditioning, to create positive emotional associations with certain contexts, and operant conditioning using positive reinforcement to teach desired behavioral responses that facilitate the delivery of veterinary care. This approach can help animals feel physically and mentally comfortable with veterinary care and, most importantly, able to make their own decisions about engaging with the humans who provide it. The overarching goal is to enable cats to make appropriate cognitive and emotional associations with the veterinary experience. This results in cats who can calmly accept human proximity and voluntarily cooperate with medical interventions.
Positive reinforcement training utilizes experiences individual cats find rewarding, such as accepting food treats and, for some, positive social interactions, to increase the probability of a particular behavioral response. These engaging triggers are also cues for the positive (engaging) emotional system of desire-seeking and will encourage a positive emotional bias that can enhance self-confidence in the individual. By offering these in response to the expression of desired behaviors and postures, the veterinary team can develop:
Cooperative care helps cats feel more comfortable, relaxed and in control in husbandry and medical situations where they may naturally feel anxious, fearful and/or frustrated. The desired behavioral and postural outputs of the more positive emotional bias are not initially automatically offered by the cat and so training involves the successive reinforcement of approximations of them. In addition, approximations of equipment required (eg, nail clippers) and/or sensory experiences associated with equipment and husbandry procedures may initially be used to gradually increase a cat’s confidence and exposure through classical and operant conditioning. For example, snipping of dried spaghetti can be used to teach a cat to remain relaxed when hearing a sound that approximates that of nails being clipped. Likewise, different containers of varying size and shape brought toward the cat’s body can be used to approximate the initial stages of medicating. Box 7 and Figure 10 provide examples of cooperative care training in action.


Example of cooperative care. This cat was trained to be comfortable with weighing scales to prevent fear of the equipment and to allow weight to be monitored at home on a routine basis for early detection of obesity or weight loss. Image courtesy of Ilona Rodan
Cooperative care involves both the handler (person) and patient (cat) learning new skills that are underpinned with a sound knowledge of what a cat is in terms of their behavior and how they learn. Education programs should take into account individual cat-related factors (eg, temperament, previous veterinary experiences), as well as the caregiver’s knowledge and skill when it comes to implementing the necessary interactions to facilitate appropriate learning, plus their expectations of their cat and the learning process. To ensure cooperation from the cat is optimal, handler skills need to be developed and practiced by both the caregiver at home and by the veterinary professionals working with the cat in the practice. This way, the cat comes to the practice with a solid foundation of required behaviors (or approximations of such behaviors) and in a calm, relaxed emotional state that the veterinary team can build on to reduce stress during the clinical experience.
Being cat-focused and adapting to a cat’s comfort levels, and where they are on their journey of cooperative care learning, is pivotal to being cat friendly. In addition, with the care-giver and veterinary team working in similar ways with the cat, a team approach is created, with the cat’s physical health and mental wellbeing at the core. This leads not only to stronger caregiver-veterinarian relationships but also stronger veterinarian-caregiver-patient relationships.
It is important to recognize that cats vary greatly in their individual temperaments and previous experiences within veterinary practices. Beginning cooperative care education from kit-tenhood gives us the best chances of true long-term cooperation, thus minimizing negative experiences. However, not all cats are obtained during kittenhood or stay with the same care-giver and/or practice, and so it is important to be able to assess each individual cat’s comfort with veterinary handling and procedures (and what factors may be leading to such experiences). Caregivers should not be tasked with trying to educate cats who are showing signs of distress or have existing health or behavior problems. In cats with problem behaviors, cooperative care education programs should only be performed with the input of a suitably qualified feline behaviorist.
Principles for interacting with cats
Pleasant, effective interactions with feline patients result from developing a plan based on species-specific needs, understanding each individual, utilizing a calming environment (see accompanying ‘Cat Friendly Veterinary Environment Guidelines’ 60 ), and adapting according to the condition and life stage of the cat. How well the veterinary team is prepared for each patient’s visit will greatly influence how the examination proceeds.
Preparing the cat and caregiver for veterinary visits
Practices often have technicians or nurses educate clients about preparing the cat at home. Alternatively, client care coordinators or veterinary care assistants can be trained to supply the information either electronically or in person. Providing information on websites and social media, including videos or links to videos supporting this education, can be helpful (Boxes 6 and 7). Anxiolytics may be needed based on an individual’s prior experiences and temperament, and potentially analgesia if the cat has a known painful condition (see ‘Pre-visit anxiolytics and other useful pharmacotherapy’). The success of the caregiver’s preparations for the trip to the practice influences the cat’s emotional state during transportation and examination.
Veterinarian preparation
Review medical records prior to the appointment, both for medical health and to identify the best means to work with the individual patient.
Develop a plan for working with cats
Ensure all team members understand cats as both a species and as individuals, their emotional and behavioral responses, and how best to interact with and handle them. Minimize wait times and stressors in the waiting area. Only experienced team members with feline-specific knowledge should work with conscious cats. Training is critical to support other veterinary professionals to ensure respect for cats, and appropriate interactions and handling. Share these Guidelines and other resources at bit.ly/JFMSCatFriendly to further team education.
Examination room preparation
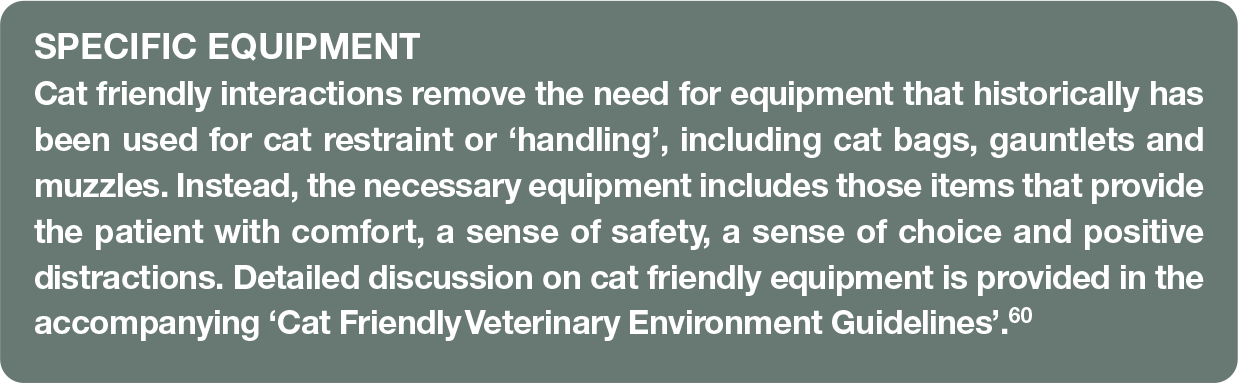
Prepare the cat-only examination room (if available) with all equipment that may be needed before the appointment to avoid sensory arousal of the cat caused by exiting and re-entering the room. See the accompanying ‘Cat Friendly Veterinary Environment Guidelines’ 60 for a list of equipment for the cat friendly examination room, and additionally for information on working in multispecies practices. Importantly, the only non-medical equipment needed to interact with and handle cats is a variety of treats, soft blankets or towels, and a high-sided bed or the bottom half of their own cat carrier. Once the room is prepared, the cat and caregiver can enter. Many practices recognize the benefit of bringing the cat in a covered carrier directly from the vehicle to the examination room. Provide towels sprayed with synthetic feline pheromones to cover carriers if the caregiver has not done so. Perform the examination and other outpatient procedures (eg, blood pressure measurement, phlebotomy, cystocentesis) in the examination room.
Considerations for home visits
Home visits are common for hospice and palliative care patients and end-of-life appointments. Additionally, some veterinarians offer only house calls or home visits for feline patients.
Performing the appointment in a cat’s home environment does not remove the potential for distress, which is associated with unfamiliar people entering and performing unfamiliar procedures in their territory.22,95 In one study, cat stress scores were shown to be higher in the home environment than the clinical environment, with increased struggling, vocalizing and agitation. 95 The same study reported that systolic blood pressure (SBP) measurements were the same in both the home and clinical environments, 95 though another study has shown lower SBP in the home environment. 22 The principles discussed in these Guidelines regarding handling techniques, hiding options, and so forth, are just as relevant in the home environment as they are in the practice.
Feline preferred locations and positions
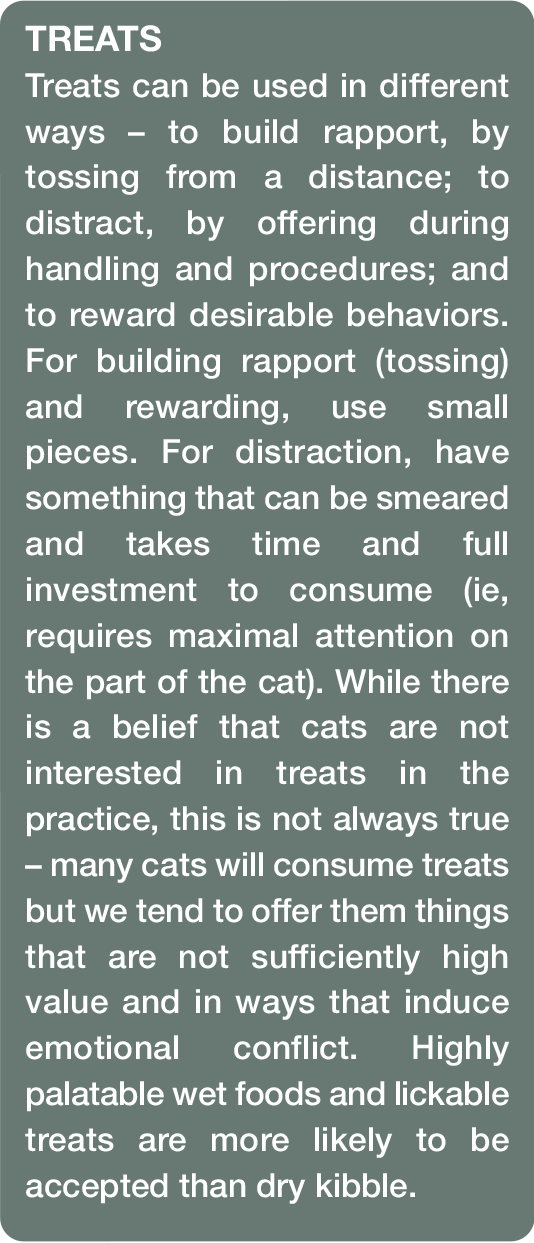
Start the examination and do as much as possible in the cat’s chosen location and position. In terms of location, this might include on the floor, on the weighing scales, inside the bottom of the carrier with the lid removed, in a cat bed, or in the caregiver’s or veterinary professional’s lap (Figure 11). Cats may prefer being covered with a warm blanket or towel (Figure 12) pre-sprayed with synthetic feline pheromones, or may respond favorably to soft conversation from the caregiver or interaction with toys. Lower-level lighting in the examination room may soothe some cats and dimmer switches in these rooms can allow varying light levels to accommodate each situation. Use of treats for distraction and reinforcement of desired behavior is often helpful; have lots of options available, such as liquid/tube treats, pill pouches, canned food and dry cat treats. The ideal position for the cat during examination is very individual, and includes sitting, standing or lying down.


(a-e) Examples of towels and blankets being used to loosely wrap (rather than tightly restrain) anxious cats to facilitate the examination. Images courtesy of Ilona Rodan (a,b), the Feline Healthy Ageing Clinic, University of Liverpool, UK (c), Sam Taylor (d) and the AAFP (e)
Feline preferred areas of touch
Preferred areas of touch for cats are the same regions that socially bonded cats groom one another to strengthen the social bond.38,39 These regions are over the feline facial glands, which produce pheromones used to communicate between members of the species.38,39 The facial glands are illustrated and labeled in Figure 3. Massage or pet over these areas in the direction of the fur (Figure 13) and from a non-threatening position (ie, at the cat’s level, approaching from the side, where possible, to avoid direct eye contact). Ask caregivers about their cat’s individual preferences with regard to touch, bearing in mind that cats may allow only caregivers to pet certain areas. Most cats dislike touch over the caudal area, the abdomen and feet, and this should be avoided as much as possible. 38 If these areas need to be examined, perform this toward the end of the assessment.

(a,b) Massaging over the facial glands. These produce pheromones used in facial rubbing and are the preferred areas of touch in the head region (see Figure 3). In both these images, massage is over at least two of the facial glands. Images courtesy of Ilona Rodan (a) and the AAFP (b)
Communication and recording in the practice
Add as much supporting information as possible into the most visible area of the medical record. In addition to the medical diagnosis include: early history; stressors within the home physical or social environment; the cat’s emotional state during previous veterinary visits (including, for example, whether they choose to explore or hide within the examination room); medications to be given when preparing the cat for the visit; and the cat’s preferences regarding position and location for the clinical examination, areas of touch and phlebotomy sites. Always ask supporting questions prior to the examination (Box 8).


After the examination, recording what worked and what did not work (see Box 9 for examples) will help avoid protective behavioral responses and escalation at future visits. Appropriate record-keeping can also alert the wider team of the need to discuss with the caregiver scheduling of appointments at a quieter time and/or of longer duration, and that preparation prior to the appointment may be required. These aspects should be discussed in advance with the attending veterinarian. This is preferable to an appointment where the cat cannot be safely handled, procedures not completed, and the cat’s negative experience in the practice reinforced.
How to approach the cat
Prior to approaching, the cat should first be observed to assess their emotional state; while knowledge of the cat’s previous behavioral history is useful in planning your approach, the cat’s emotional state at each interaction needs to be assessed before initiating any contact. In an examination room situation, the cat should be allowed time to choose to come out of the carrier on their own accord and acclimatize to the room (Figure 14). This is preferable to reaching into the carrier (which risks the cat feeling threatened or trapped) and pulling the cat out, or tilting the carrier to force the cat out. The same holds true for hospitalized cats -begin by opening the cage door slightly and allowing the cat to choose to come to the front of the cage. For tips and techniques on enticing a cat out of their carrier, see ‘Recommendations for first interactions’, and Video 4 in the supplementary material.

Open the carrier door and allow the cat to come out on their own accord. Treats can be offered passively in front of the carrier to encourage the cat to exit. Image courtesy of Ilona Rodan
Explain the strategy to the caregiver or other team members and ask that they not interact with the cat unless the cat approaches them, which will give the cat more options. While the cat either chooses to remain in the carrier or is exploring, a history or update on the cat’s progress can be obtained; calm conversation will put everyone, including the cat, at ease.
By observing the cat’s movements and body language, including facial expressions, and response to room smells, your presence, noise and/or activity, a better understanding of the cat’s current emotional state, as well as their physical state, can be obtained. Leaving the door to the carrier open, where possible, so the cat can enter and exit at will, will impart a better sense of safety (access to carrier) and choice, and ease the cat’s anxiety about possible threats and frustration caused by the inability to escape. Throughout the examination it is essential that the cat has the choice to hide, as this is an important coping strategy, especially in an unfamiliar environment or when protective emotions are aroused.
General considerations when approaching a cat are highlighted in Video 5 in the supplementary material.
Recommendations for first interactions
- Cats feel more secure with all four feet in contact with a solid surface;
- Request that the caregiver facilitates moving the cat if you feel confident in their ability to do this safely in a cat friendly manner;
- Transfer the cat in their carrier or the bottom half of the carrier, if possible;
- If not using the carrier, use a loose towel to provide a sense of security; try to mimic the sensation that the limbs are in contact with a solid surface by bringing the cat, loosely protected in the towel, closer in toward your body.
What is the cat’s body language revealing?
At all times, use the information the cat is giving to determine appropriate ‘handling’. If the cat has approached with relaxed or positive body language and facial expressions (eg, ears up and forward, head and body upright, straight legs, tail up, positive vocalizations, relaxed position when lying down, exploring), then proceed with the examination. Cats who are exhibiting protective behaviors need a hiding option during the examination, or consideration should be given to rescheduling the appointment and dispensing anxiolytics for administration prior to the return visit (see Table 1). If it is necessary to proceed with the examination at the time, consider administering chemical restraint (see Table 2, page 1125). Analgesia should be provided for cats who are painful, with assessment of painful areas delayed until this has taken effect (eg, at the end of the examination or following sample collection). Some cats become frustrated with confinement in a cat carrier or cage, and allowing them additional time and space to explore the examination room, or other area, prior to approaching (eg, using treats to encourage positive engagement with the environment) can be helpful. Hiding options and consistency in care can also help diffuse frustration for cats in cages.
Commonly used sedation protocols that can be administered as a single IM injection in protective cats

Consider reducing doses by 25-50% if gabapentin or trazodone have been administered pre-visit IM = intramuscular
Sedation protocols for emotionally challenged cats*

Provide oxygen by mask during sedation. The goal of these sedation protocols is to enable placement of an IV catheter for further sedation or to induce anesthesia
Gabapentin (20 mg/kg PO) or trazodone (10 mg/kg PO) are given 2 h prior to leaving the house. In exceptional circumstances, trazodone 5-10 mg/kg PO and gabapentin 20 mg/kg PO can be given in combination 2 h prior to leaving the house
IM = intramuscular; SC = subcutaneous; PO = oral; ASA category = American Society of Anesthesiologists’ physical status classification
Protocol from Sarah Heath (Behavioural Referrals Veterinary Practice, UK) and Matthew Gurney (Zero Pain Philosophy)
Always continue to assess and reassess a cat’s body language during any interaction, as their emotional states and behavior can change. An inhibited cat who is freezing can become more aroused if the cause of the fear is not addressed and sympathetic handling is not applied. If they perceive that their inhibition response is unsuccessful, they may change to one of the other available responses such as avoidance or repelling behaviors (Box 4). Confident cats can become frustrated if they are physically restricted during examination, and such cats may be happy to initiate a short amount of contact with you but may not be happy with prolonged intense contact.39,97 Some of these cats can be distracted using treats (see box) and will permit further examinations to be performed while they are eating. Clinical interactions are a dynamic process and the veterinary team must be prepared to adapt, slow down when required, and give the cat breaks in order to complete the necessary work.
How to perform a cat friendly physical examination
General approach
In most cases, only one person is needed to examine a cat. Although practices may ask that basic physiological data (temperature, heart rate, respiration rate) are gathered and weighing is performed prior to the veterinarian examining the patient, this should be avoided – not only to increase efficiency, but to prevent the need for additional handling and the risk of triggering protective emotions. The veterinarian should enter first, either with or without another team member who (if present) will remain throughout the appointment.
Most veterinarians approach a physical examination with a checklist that moves from head to tail. Although this may ensure that the veterinarian meets basic standards of care, flexibility in the order of the evaluation, based on the cat’s preferences, minimizes patient distress. Progressing carefully and slowly through the examination, while allowing the cat to make choices about positioning and handling, and taking short breaks when necessary, will facilitate the evaluation. If the cat resists aspects of the examination, attempt different distraction techniques, such as massaging over the facial glands or making food treats passively available to the cat (eg, on the examination table); proceed with examination in short manageable segments; or perform other parts of the evaluation and then return to the areas of hesitation. The least preferred aspect of the examination varies among cats; some may resist interaction with certain equipment (eg, stethoscope, weighing scales), while others may be wary of handling of individual body parts or deep palpation of the abdomen. It may be best to leave these particular aspects until last.
For most cats, auscultation of the heart and lungs is the best first step, as it is the least invasive; moreover, if subsequent chemical restraint is needed, the necessary assessment of the cardiovascular and respiratory systems will have been performed. However, the respiratory rate of the cat is ideally recorded prior to any physical interaction. Where possible, the heart should be auscultated on a number of occasions during the examination as the heart rate and detectability of a heart murmur will vary throughout the examination. 98
For evaluation of musculoskeletal disease (predominantly DJD), a combination of physical examination and caregiver assessment is essential, as caregivers may have recognized changes in their cat’s normal behaviors and mobility.99,100 Several questionnaires have been validated for this purpose, and can be provided to caregivers in advance of the appointment.101-106 Visual assessment of mobility is best conducted in the home, as many cats do not move normally in the practice. Do not coerce the cat to move during the physical examination; instead, the veterinary team should request caregiver videos of the cat walking, jumping, and climbing up and down stairs for the veterinarian to assess.
If a cat consistently resists portions of the evaluation or demonstrates protective behavior despite the provision of hiding options and other positive reinforcements, consider alternative approaches based on immediacy of need (see ‘Preparation prior to visiting the veterinary practice’, ‘Cooperative care, the future of cat friendly’ and ‘Protective cats’).
Tips for performing an effective physical examination while minimizing stress
The following are suggestions to facilitate completion of the examination with the least stress for the cat. If required, use blankets or towels to cover or gently wrap – but not to tightly restrain – the cat (Figure 12).

Approach the cat from an angle when examining the head, to avoid direct eye contact. Image courtesy of Ilona Rodan


Combine abdominal palpation with head and neck petting and massage to make the experience more positive.

Palpation of the spine for degenerative joint disease. Image courtesy of Ilona Rodan

(a,b) Oral examination. Note the examiners are avoiding pulling on the cat’s fur to raise or lower the lips. Images courtesy of the AAFP (a) and Feline Healthy Ageing Clinic, University of Liverpool, UK (b)

Cat sitting on a warm blanket on weighing scales. The scales are zeroed after placing the blanket and before the cat is enticed onto them. Image courtesy of Kelly St Denis
Considerations for specific procedures
When considering the best (ie, most cat friendly) way to perform a specific procedure, it is important always to remember that each cat is an individual and be prepared to adapt and try a different approach or technique based on information from the cat. If the procedure is one that is going to be required on an ongoing basis, then introducing it slowly to acclimatize the cat, and training them to offer an appropriate posture or behavior to assist in the performance of the procedure, should be considered. This may take more time and effort initially but the investment will be worth it in the longer term. Use treats or other positive reinforcement to reward the cat for appropriate postures and behaviors, both while undertaking the procedure and immediately afterwards (see Video 8 in the supplementary material for examples).
When obtaining blood, urine or any other samples, consider collecting extra and storing it for a day or two, so that further tests can be performed if indicated. In the majority of cases, only one or two veterinary team members are needed to collect laboratory samples. In cats demonstrating protective emotions and behaviors, collection of samples should be performed by experienced team members only; valuable experience with sample collection can be gained on anesthetized patients or on calm cats. However, even experienced persons may have challenges with an individual or on a certain day. If there is difficulty with collecting a sample or with intravenous (IV) catheterization due to lack of experience or ability, discontinue after two attempts and ask someone else to try; if they are not successful, reconsider the approach required.
Review the cat’s history and consider any factors that may influence how you approach the procedure. For example, cats who have a history of severe dental disease may be painful around the head and so the jugular vein may not be a good choice for a blood sample. Likewise, brachycephalic cats often do not tolerate their head being lifted for a jugular sample, obese cats may not have veins that are easy to find, and arthritic cats and Scottish Folds may not be comfortable with extension of some of their joints. Rather than extending or holding over a joint, move the humerus forward or the femur back to accomplish the desired positioning. Life stage also needs to be taken into consideration, as the approach to an adult or senior cat may be very different to that for a kitten, due to size and the presence of comorbidities (see ‘Life stage handling’). Always ensure the cat has adequate analgesia prior to starting any procedure and do not be afraid to provide chemical restraint if required.
Importantly, the lifestyle of the cat also needs to be taken into consideration, with feral or street/community cats needing a very different approach to companion cats (see ‘Working with feral or street/community cats: key principles’).
Blood pressure measurement
Cat friendly interactions performed in a cat friendly environment should reduce the risk of situational hypertension. Always work where the cat is comfortable, be it on their own bedding or warm towel or blanket, or in their caregiver’s lap. If the carrier has a removable top, and the cat prefers, allow the cat to stay in the bottom half of the carrier (partially or fully covered with a blanket, if required). Coccygeal measurements (Figure 20) are preferable for some oscillometric machines, 129 and for cats with OA in peripheral joints or with sarcopenia. 130 Radial measurements (Figure 21) are preferable in obese cats. 131 For further details on feline hypertension, see the ‘ISFM Consensus Guidelines on the Diagnosis and Management of Hypertension in Cats’ 132 and the AAFP’s Hypertension Educational Toolkit (catvets. com/hypertension).

Coccygeal blood pressure measurement being taken while the cat remains relaxed in a cat bed. Image courtesy of the AAFP

Radial blood pressure measurement being taken while the cat is relaxed in the base of their carrier. Image courtesy of the Feline Healthy Ageing Clinic, University of Liverpool, UK
Additional considerations for Doppler machines
✜ Avoid clipping the fur; instead wet down the contact area, either by using a damp cotton ball (cotton wool) or by gently massaging ultrasound gel into the paw.
✜ Use quiet clippers if clipping the fur is required to detect blood flow (see accompanying ‘Cat Friendly Veterinary Environment Guidelines’ 60 ); allow time for the cat to resettle before measuring SBP.
✜ Do not hyperextend or place hands over joints while measuring blood pressure, as painful joints are often undiagnosed. As many cats do not like to have their feet touched, gently hold the paw (Figure 21) or let it rest in the palm of your hand, rather than holding the foot tightly.
✜ Use headphones. If not available, use the lowest volume needed to hear pulsatile blood flow, and turn down or off when moving the probe.
✜ Keep ultrasound gel in a small bottle with a pump-action top.
Venipuncture
The venipuncture site should be chosen based on the individual, and a small gauge needle, appropriate for the size of the animal, selected. Insulin syringes (28-31 G needles) can be used for neonatal and pediatric patients or where small volumes of blood are required. If clipping of fur is performed, use quiet clippers (see accompanying ‘Cat Friendly Veterinary Environment Guidelines’ 60 ). For cleaning the skin or wetting down the fur if not clipping, use dilute chlorhexidine or similar, avoiding alcohol-based products due to their strong scent. For cats undergoing planned phlebotomy that withdraw with needle touch (eg, hospitalized patients or cats coming in for regular screening tests), apply topical local anesthetic 30 mins before the procedure, when possible.133,134 Advance the needle slowly and gently – avoid ‘stabbing’.
Tips for jugular sampling
Use minimal handling, tilting the head up gently while avoiding the whiskers. Do not restrain the legs or hang the forelimbs over the edge of the examination table, as it causes the cat to lose their sense of control and can be painful. If the cat raises a forelimb, consider wrapping the cat loosely in a towel so they can freely move their legs, but team members are protected. Cats who are very active in the practice may be able to be distracted with a liquid treat and a hands-free blood sample collected (Figure 22; see also Video 8 in the supplementary material).

Cats having a jugular blood sample collected with (a) no physical handling and (b) only minimal handling, including no restraint of the forelimbs. Note the use of a liquid treat to distract the cat in image (a). Images courtesy of the Feline Healthy Ageing Clinic, University of Liverpool, UK (a) and Ilona Rodan (b)
Tips for medial saphenous vein sampling
The medial saphenous vein is appropriate for use in cats with head or forelimb shyness, as well as for cats with cervical and/or elbow OA; it is also suitable for routine use. The cat should be placed in a semilateral position, so that the dorsal half of the body retains a comfortable, sternal posture (Figure 23). Forcing the cat into full lateral recumbency takes away all sense of control for the cat. The cat can be snuggled by the handler, loosely wrapped in a towel, and massaged over the facial glands and/or distracted with treats. Let the tail remain in a natural position as determined by the cat. The limb used for sampling should be stabilized without tightly holding over the joints, pumping the foot or using the full weight of the hand; and refrain from hyper-extending the tarsal joint, which can cause unnecessary discomfort.

Medial saphenous venipuncture with the cat in a semilateral position. Image courtesy of Eliza Sundahl
Tips for cephalic sampling
Avoid hyperextending elbow joints. Place a hand behind the humerus to advance the fore-limb and prevent retraction. Allow the cat to snuggle back into the body of the handler if they choose. Some cats may wish to hide their head from view into an offered loose towel or blanket. The forelimb used for sampling should be stabilized without tightly holding or pumping the foot (Figure 24).

Cephalic venipuncture with a 25 G butterfly catheter. The patient remains comfortable within the bottom half of the carrier. Image courtesy of Ilona Rodan
Cystocentesis
Have the cat standing, held gently against the body of the assistant, who will have one arm around the cat’s head/neck area and the other slightly retracting the hindleg at the thigh (Figure 25). Use one hand to localize and hold the bladder and the other to perform the cystocentesis. Where possible, use distraction techniques. If performing cystocentesis in lateral recumbency, avoid hyperextending the hindleg; hand placement should likewise avoid feet and joints, and do not hold the tail (Figure 26). Dorsal recumbency collection may be necessary during ultrasound-guided cystocentesis, in which case the cat should be placed in a blanket-padded trough for full body support. If the patient demonstrates any distress, do not proceed with this approach, but make an effort to trial lateral recumbency or standing approaches or a plan to provide chemical restraint.

Standing cystocentesis. The cat is held gently against the body of the assistant, who is slightly retracting the hindlimb, holding at the thigh. Image courtesy of Kelly St Denis

Cystocentesis in lateral recumbency. Note the hindlimbs are not being held at the joints or feet. Image courtesy of Ilona Rodan
IV catheter placement
The key points of IV catheter placement are the same as for venipuncture, except that local anesthetic can often be incorporated more easily into the catheterization protocol as more time may be available to prepare. When cats are presented with significant dehydration or low blood pressure, the size of catheter should be chosen based on the size and status of the vein (regardless of body size). This will reduce unnecessary pain for the patient and the risk of damage to the vein. Determining the site of catheter placement needs to take into account the length of time it will be in place, how comfortable this position will be for the cat, and whether it interferes with their ability to eat, drink, rest comfortably, sleep and/or groom. The goal should be to secure the catheter adequately so that it stays in place, but to minimize the dressing required to keep it clean and covered. Full leg bandages are often not tolerated well by cats and can impede comfortable resting postures. Distally, toes should be left exposed in order to assess for reduced digit temperature or cyanosis (indicating an over-tight bandage), as well for the presence of any odors or discharge. In cases where tape has stuck to fur, utilize safe veterinary products that dissolve the adhesive rather than pulling the tape and fur away.
During removal of IV catheters, caution should be exercised when cutting tape, in order to avoid cutting the catheter itself, which can then become a venous foreign body.
Cat friendly administration of injections
Factors contributing to painful injections
✜ Quantity of the medication and the site that it is administered;
✜ pH and temperature of the medication;
✜ Needle length and gauge;
✜ Sharpness of the needle; dulling of the needle occurs with penetration of rubber stoppers and, therefore, the needle should be replaced just prior to injection; 135
✜ Route of administration (IV, intramuscular [IM] or subcutaneous [SC]);
✜ Underlying patient comorbidities, as well as fear-anxiety predisposing to hyperalgesia;
✜ Potentially irritant drugs; certain chemo-therapeutics, for example, may cause pain or tissue damage in the case of extravasation, and should only be administered through stable IV catheters.
Strategies for reducing injection site pain
✜ Use the medication according to the manufacturer’s instructions. For example, if it is labeled for IV use, do not administer intramuscularly or subcutaneously, as the pH may cause a pain response;
✜ Use the smallest needle length and size suitable to administer the drug correctly the first time. This will vary based on the viscosity of the liquid being administered;
✜ Replace the existing dull needle with a new needle after removing medication from a vial and before administration of the drug to the patient;
✜ If the injection has an acidic pH or is known to sting on administration, consider anxiolytics/ chemical restraint, where possible;
✜ Remove any air bubbles;
✜ IM and SC injections should be administered efficiently and at a consistent rate. Some IV drugs require slow administration. Follow manufacturer recommendations;
✜ Inject with the needle going in and coming out at the same angle. Avoid moving the needle around during injection;
✜ If the manufacturer’s directions state it to be acceptable, allow the drug to come to room temperature before administration. 136
The veterinary team should consider ways to reduce the number of injections given. For example, is it possible to mix some medications into one syringe or administer medication diluted within fluids being given subcutaneously? Alternative routes of administration that may sting less should be considered if the safety, absorption and efficacy of the drug is not impacted. Assigning regions of the body for specific injections and avoiding repeated use of the ‘scruff’ area is helpful for tracking any inflammatory responses to injection. Use the site that involves minimal handling of the individual cat for IM injections.
Microchipping
Perform microchipping under sedation/ anesthesia in conjunction with other procedures (eg, spay/neuter), whenever possible, and use a smaller-sized microchip if available. Placement of a microchip without consideration of the potential for pain, leading to an aversive experience, can potentially influence future appointments at the veterinary practice. When microchipping conscious cats or kittens, have a team member massage over the facial glands or use other distraction techniques. An occasional cat may require anxiolytics, analgesia or chemical restraint prior to microchipping.
Ultrasound examination
Many patients requiring ultrasound examination are unwell and/or older and likely to have DJD-associated musculoskeletal pain. Analgesia should be administered prior to ultrasound, and chemical restraint is also generally preferred, both to improve image acquisition and reduce patient fear-anxiety. The cat should be supported in a blanket-padded trough or other appropriate form of soft warm bed during the procedure. Food distraction may be helpful if the cat is conscious. Become comfortable with scanning patients in positions that are comfortable for them; for example, bladder checks can be performed standing, and emergency scans/fluid checks (eg, point-of-care ultrasound to check for effusion in dyspneic patients) can be performed in the cat’s carrier or hospital cage (Figure 27).

(a,b) Examples of a cat having an ultrasound examination in the bottom half of their carrier. Images courtesy of Sam Taylor
Radiology
Minimize human exposure to radiation (legal requirements in many regions prohibit the presence of humans in the x-ray room during exposure). Analgesia should be administered, as many patients requiring radiographs are painful. Chemical restraint or anesthesia will reduce patient distress and pain, and help in the acquisition of diagnostic quality radiographs. Use warm towels, blankets, soft beds or padded troughs on the table to limit hypothermia. Neither ties nor heavy sandbags should be used as positioning aids, even in a sedated/ anesthetized cat.
Nail clipping
Perform nail clipping under anesthesia in conjunction with other procedures, where possible. In conscious patients, use a loose towel wrap, positive reinforcement and minimal handling. Consider the potential for underlying painful disease, such as dental disease or DJD, which may be impacting the cat’s ability to maintain their own claws, and pretreat with analgesics if required. For indoor cats, point caregivers to appropriate resources (eg, the AAFP’s Claw Friendly Educational Toolkit, catvets.com/claw-friendly-toolkit) and teach them to trim nails.
Ear cleaning
In the absence of aural discomfort or disease, feline ears do not require cleaning. Cleaning should only be performed after an otoscopic examination (under chemical restraint or general anesthesia, where possible) and cytological assessment. Take care as some ear cleaners can be irritating to the ear canal and nasopharynx. Instead, use saline to moisten and facilitate the removal of debris, and avoid placing large quantities of fluids directly into the ear to reduce the risk of irritation to the nasopharynx.
Grooming
Any grooming that is more involved than a hygiene clip or single mat removal is best performed under chemical restraint or general anesthesia. Avoid brushing if the coat is matted, as the brush will pull on the skin and cause pain. Consider the potential for underlying disease (obesity, dental disease, muscu-loskeletal disease), which could be reducing the cat’s ability to groom.
Rectal examinations and anal gland expression
Rectal examination or enema administration in cats should not be performed without analgesia, chemical restraint or anesthesia. Impacted anal glands in cats should also not be expressed without consideration given to providing analgesia or chemical restraint.
Life stage handling
Regardless of age, cats must be handled in a respectful manner, minimizing distress as much as possible. Starting off with cat friendly interactions during kittenhood can help prevent negative responses in the future.12-14
Neonates and pediatrics (0-12 weeks)
While traditionally it might have been considered normal practice to scruff pediatric and neonatal feline patients, due to their size and demeanor, scruffing is no longer recommended for cats at any life stage. It is a mistaken premise that scruffing makes patients easier to work with. Scruffing causes negative responses 71 that impact on future visits, as the cat will remember the painful or stressful event.
Rather than such forceful restraint, the ideal is to incorporate the same cat friendly techniques as used in adult cats, with some simple modifications. A kitten can be loosely wrapped in the same manner as an adult cat, but on a smaller scale using a tea towel or washcloth. Alternatively, a gentle pediatric cradle hold can be used to help control movement (Figure 28). Neonates and young kittens can be quite receptive to having the facial glands massaged, and this can often prove a good distraction technique while procedures such as vaccinations are performed. Kittenhood is a critical time in terms of the animal’s emotional and cognitive health, and kittens will readily form emotional associations with novel experiences. Early veterinary experiences for these individuals are, therefore, particularly important.
In rabies-endemic countries, a bite from a kitten that is under the age for rabies vaccination can potentially mean quarantine or euthanasia for that animal. Practicing cat friendly interactions is extremely important in these young patients to decrease this risk.

Pediatric cradle hold. Neonates may be held by placing one hand over the dorsum, holding the base of the jaws with thumb and forefinger. The other hand holds the lower half of the kitten and helps control the animal’s movement. Image courtesy of Ellen Carozza
Mature adult and senior cats
There are additional considerations as cats advance into mature adult and senior life stages. 123 As mentioned, the prevalence of DJD increases as cat age,90,91 as does the prevalence of concurrent diseases such as CKD137,138 and hyperthyroidism. 139 Assessment for frailty using modified frailty scales 123 will further guide the veterinary team on appropriate cat friendly interactions with the patient.
It is important to assess any aging cat for musculoskeletal pain (Box 10) before deciding how the required procedure is going to be performed. Attempts should be made to keep joints in a neutral position and minimize flexion/extension. Cats with chronic diseases such as CKD or hyperthyroidism will likely require procedures such as blood sampling on a more frequent basis, so taking time to reduce distress and make the experience more positive for these patients will be beneficial in the longer term and, in turn, will increase client compliance. Cats with hyperthyroidism and CKD are both more at risk of hyperten-sion;140-142 in the experience of the Task Force members, the risk of damage and bruising during venipuncture is greater in these patients, further underlining the importance of a cat friendly approach. Patients with DJD should receive analgesia, too, which can be given by the caregiver at home.
Aging has implications for a cat’s emotional state, and an increase in anxiety can be seen in older patients. It is also important to remember the potential for cognitive decline and to consider how this may impact the patient’s perception of the veterinary experience. 143
Working with feral or street/ community cats: key principles
✜ Do not physically handle these cats when they are not sedated or anesthetized.
✜ The pre- and post-sedation area should be warm, quiet and dimly lit to reduce stimulation.
✜ Work with local charity groups to ensure cats are presented to the practice in suitable carriers, including a wire trap, restraint cage or side-loading wire carrier.
✜ Keep carriers covered at all times to reduce visual stimulation.
✜ If it is necessary to move cats between carriers, bear in mind that they will be more willing to move to a hidden location; hence, cover the cage they need to move into and uncover the one they need to move out of.
✜ Where possible, the cat should remain within the same carrier throughout the procedure, reducing the risk of disease spread and the mingling of scents between cats.
✜ Place incontinence pads under the wire trap/ carrier both pre- and post-sedation to allow urine/feces or vomit to be cleaned away with minimal disturbance to the cat. Incontinence pads can be placed on top of towels and blankets to provide extra warmth and comfort, but it is best to avoid putting any bedding directly in the carrier as this can interfere with administration of IM injections, and it can be difficult to dispose of the bedding if it becomes soiled.
✜ Have all anesthetic drugs and medication drawn up and prepared in advance, to reduce the time the cat carrier is uncovered.
✜ Administer sedation intramuscularly using either a restraint cage, or ‘forks’ to restrain a cat that is in a wire basket or trap. Ensure that forks or the squeeze action of the restraint cage are introduced slowly and gently (never quickly or forcefully) to restrain the cat against the side of the cage to allow IM injection.
✜ Reverse sedatives where possible post-sedation to reduce the risk of hypothermia.
✜ Recover the cat from sedation/anesthesia in the carrier in which they are going to be returned. The carrier should be side-opening to allow quick and safe release.
Management of the hospitalized cat to reduce stress
Hospitalization can be a challenging time for a patient as they are in an unfamiliar environment and handling for procedures (eg, IV catheter placement, measurement of vital parameters, medicating) is likely to be required. If IV therapy and/or frequent patient monitoring are not indicated, it is ideal to manage the cat’s medical condition at home.
If the cat needs to be hospitalized, efforts should be made to reduce triggers for protective emotions and to maintain manageable levels of emotional arousal. Ensuring that the cat can cope with their environment will reduce the potential for distress and this, in itself, will likely expedite recovery, reduce pain and encourage voluntary food intake. 6 Prior to admission, information should be obtained from the caregiver (verbally or preferably using a history questionnaire) on the cat’s temperament, dietary preferences, litter preferences and preferred interaction with humans. Relevant information regarding temperament (eg, confident or timid), prior history and preferred interactions should be passed on to all team members, noted in the medical record and hospitalization chart, and/or added to the cage (in the form of a label or card attached to the door, or by writing directly on the cage door, if plastic/acrylic). The accompanying ‘Cat Friendly Veterinary Environment Guidelines’ 60 contain example new client and dietary history questionnaires, and a cat friendly hospital chart as supplementary material. They also discuss cage layout and, in particular, the importance of hiding places. Box 11 summarizes further ways to reduce the potential for distress during hospitalization.
Always individualize what is most important for each patient, and take into consideration when finalizing the treatment plan.
Scheduling interactions
Interactions and procedures that require handling should preferably be scheduled so as to minimize interventions. Where possible, synchronize medication with vital parameter monitoring, or combine procedures (eg, check heart rate and flush an IV catheter at the time a medication is due), to reduce the number of times a cat is handled, ideally within the cage. Assuming there are no contraindications, it may be possible to combine timing of medications by, for example, putting oral medications together in a gelatin capsule. If the cat is distressed by being orally medicated, then choose another route (eg, IV), if appropriate. Where analgesic medications with a sedative or anxiolytic effect are being used, schedule interventions for when these are at peak effect (eg, place an IV catheter 30 mins after methadone is administered); similarly, consider using local anesthetic creams or gels prior to IV catheter placement and blood sampling, 144 and allow adequate time for effect (minimum 30 mins).133,134
Allow periods of uninterrupted sleep or rest during standard resting periods (ie, at night), as proper rest and maintenance of circadian rhythms is recognized to be vital for recovery in human patients, 145 and likely similar is true in cats. Ensure minimal disturbance from lights and noise in the ward during these times.
Handling hospitalized cats
Much of the discussion in the earlier sections on ‘Principles for interacting with cats’ and ‘How to approach the cat’, as well as the below section on ‘Protective cats’, is relevant to approaching and handling hospitalized cats. In general, if there is a quiet, cat-only area in which to perform procedures, give medications, check IV catheters, and so on, then use that area. Examinations, treatments or euthanasia should not be performed in front of other cats. Such procedures can be performed in the cage if no such area is available but use minimal and cat friendly handling techniques. The veterinary team should evaluate whether all monitoring and assessments are truly needed and whether the information acquired would change case management. For example, checking the temperature of hospitalized patients twice a day may not be necessary, especially if other parameters are normal and the cat is bright, alert, responsive and eating, or has undergone a routine procedure. Interactions should incorporate the use of positive emotional triggers, such as food treats, grooming or playing with toys, and, if accepted by the cat, be recorded and communicated to the team.
Some cats may show frustration associated with hospitalization and methods to minimize this emotion are described in Box 12.57,146
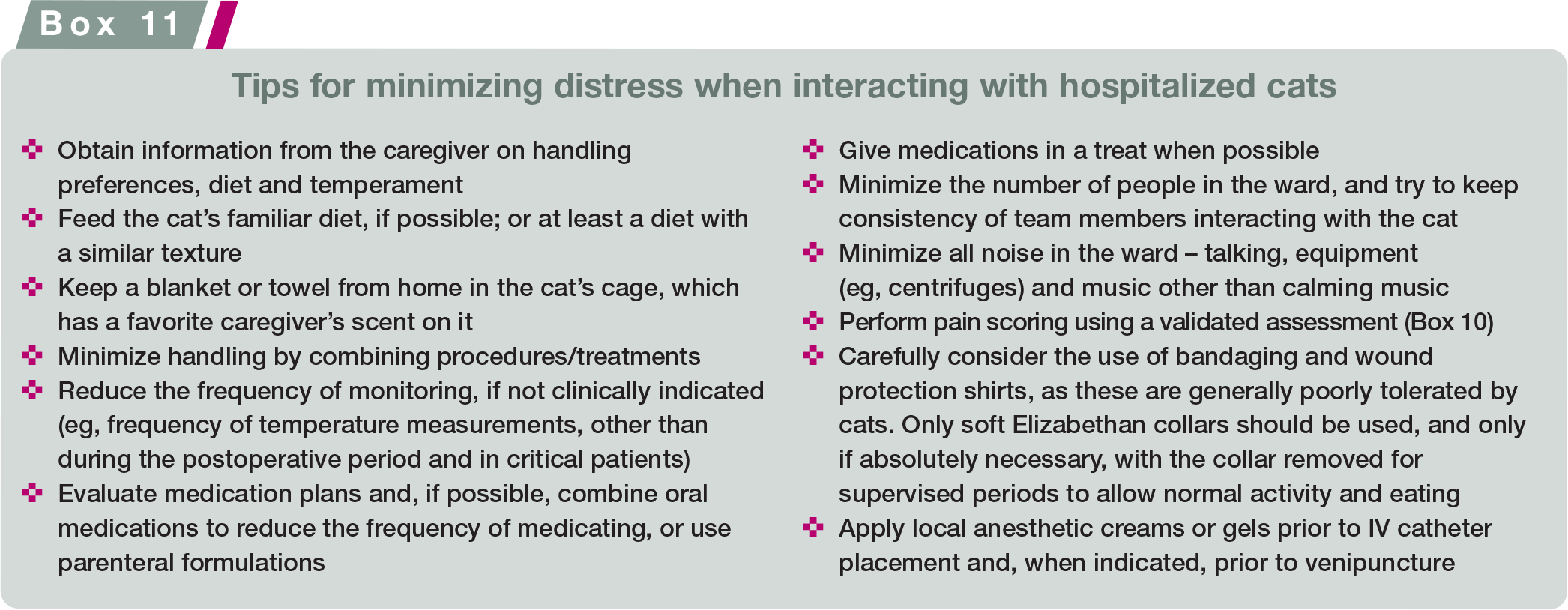

Attention to nutrition
A positive association between adequate nutrition and hospital discharge has been demonstrated in dogs and cats. 147 Conversely, metabolic derangements associated with malnutrition are likely to impact negatively on the prognosis of hospitalized cats, 148 and the stress of hospitalization itself is likely to reduce food intake. 149 Information on the cat’s normal diet, including preferred treats, should be obtained when taking the history. Furthermore, a nutritional assessment of the patient should be performed routinely, along with recording of voluntary intake as a proportion of the resting energy requirement (RER). Pain management, and control of nausea and ileus, will encourage intake but assisted feeding interventions (a feeding tube and/or appetite stimulants)
should be considered promptly in patients consuming less than RER for 3 days or more, which includes any period of inappetence prior to admission. 148 For more information, readers are referred to a review by Witzel Rollins and Murphy on nutritional assessment in the cat, 150 and the ‘2022 ISFM Consensus Guidelines on Management of the Inappetent Hospitalised Cat’. 151 Note that syringe feeding is not recommended due to the risk of aspiration, food aversion and procedure-related stress.
Protective cats
Cats who appear challenging or difficult in the veterinary practice have intensified emotional states – commonly fear-anxiety, pain or frustration, but also, on occasion, emotional arousal connected with intense desire-seeking (Box 3). Protective behaviors can be caused by previous life or veterinary experiences, particularly if the recommendations in these Guidelines, as well as the accompanying ‘Cat Friendly Veterinary Environment Guidelines’, 60 are not followed. Such cats may exhibit repelling behaviors (eg, hissing, swiping, scratching or biting) if forcibly handled or unable to retreat/hide. The earlier section on ‘The emotional state’ describes protective emotions that can lead to these behaviors. By providing a cat friendly environment and following all the principles outlined in these Guidelines, with pre-visit preparation, and careful and positive interactions, it may be possible for these cats to improve rather than become increasingly more difficult with each visit.
Protective behaviors may also be due to pain, making a pain assessment essential (Box 10). Use validated acute or chronic pain assessment tools,105,109,114 where indicated, provide analgesia and assess the cat’s response and change in demeanor. Historical knowledge of the cat’s temperament and demeanor in the practice is also useful, as these patient factors can influence the results of pain assessment tools.
Algorithm 2 presents a decision-making tree to assist the veterinary team on how to proceed with cats who exhibit protective behaviors.

Procedural sedation
Sedating protective cats for procedures (physical examination, blood tests, etc) reduces the potential for future distress and enhances human safety. Ideally, as discussed earlier, pre-visit anxiolytics will have been prescribed, or the procedure postponed, but sometimes this is not possible. In these situations, the safest combination of sedative and analgesic drugs should be used to minimize adverse effects and injection volume. In some circumstances, pre-sedation assessment will not be possible due to the cat’s demeanor and protective behavior. Choosing drugs with minimal cardiovascular adverse effects and sedating the cat before protective behaviors escalate avoids the stress and negative consequences (physiologically and emotionally) of heavy restraint and forced procedures. Note that induction chambers are not recommended due to increased cardiovascular risks to the cat from high-dose inhaled anesthetics and to team members from unscavenged gases,65,81 as well as the considerable distress caused to the cat.
IM injections can be given into the lumbar, hindlimb or neck region, with the cat remaining in the bottom half of a cat carrier if anxiolytics have not been given pre-visit. Additionally, if not given pre-visit, oral gabapentin can be administered in a treat during the consultation or in the carrier. Chemical restraint will be less effective in the presence of high arousal; hence, as discussed, cats should be placed in a quiet area, with the carrier covered with a blanket. Sedated patients must be monitored at all times. 81 Removing IV catheters and dressings prior to recovery, if safe to do so, avoids the need for additional sedation later.
Tables 2 and 3 outline commonly used sedation protocols that can be administered intramuscularly as a single injection in protective cats, and sedation protocols for emotionally challenged cats, respectively. For detailed discussion on feline sedation, readers are referred to the ‘AAFP Feline Anesthesia Guidelines’ 65 and a review by Simon and Steagall on feline procedural sedation and analgesia. 81
Creating cat friendly interactions from a human behavior change perspective
Changing human behaviors that are in conflict with cat friendly interactions, whether our own behaviors or the behaviors of others, can be challenging.
Human behavior change theories can be helpful, assisting us to:
1) Understand the external and internal influences on human behavior that facilitate and prevent desired behavior.
2) Design, implement and assess interventions to facilitate desired behavior.
The COM-B model 152 identifies three factors – capability, opportunity and motivation -that influence human behavior.
✜
Example questions include:
- Do veterinary teams and caregivers have relevant knowledge about cat behavior and communication to understand cats’ interaction preferences?
- Do they know how to put that knowledge into action when interacting with cats?
✜
- Do caregivers have the time to train their cats to voluntarily go in the carrier and remain calm during carrier travel?
- Do caregivers and veterinary team members have treats on hand to reward calm behavior or to use to increase positive (engaging) emotions during interactions?
- Is the practice supportive of these approaches being taken by individual team members?
✜
When trying to facilitate the change toward cat friendly behaviors within the veterinary team it is important to identify possible barriers to the desired behavior in terms of these factors. This will be individual to every practice: team training can help overcome barriers in capability; modeling of cat friendly interactions may afford social opportunity for other team members to also start to work in this way; but a cultural change in the practice may also be required to give physical opportunity (eg, longer appointments). The automatic motivation to interact in a cat friendly manner may be something many of us recognize in ourselves, but tapping into the reflective motivation of other team members may be required to facilitate their behavioral change.
An example question for reflective motivation is:
- Do veterinary team members believe cat friendly interactions are the right way to interact with cats?
Example questions for automatic motivation include:
- Does interacting in a cat friendly way (or other way) make you feel good?
- Is interacting in a cat friendly way (or other way) reflexive in nature?
Human behavior change is increasingly being recognized as a key component in improving animal welfare. It is our behavior that needs to change – in order to facilitate a positive change in the emotions and resulting behaviors of our feline patients during their veterinary experience.
Conclusions
The ‘Cat Friendly Veterinary Interaction Guidelines’ replace the previous ‘AAFP and ISFM Feline-Friendly Handling Guidelines’, 1 incorporating supporting evidence for the continued adoption of cat friendly interactions. These Guidelines should be used in conjunction with the ‘ISFM’s Cat Friendly Principles for Veterinary Professionals’ 153 and the accompanying ‘Cat Friendly Veterinary Environment Guidelines’. 60 It may take time for all team members in the practice to implement these suggestions, but a gradual introduction, education and involvement of the team in the incorporation of these steps will result in wider adoption as the benefits are recognized. The Guidelines also prepare practices and individuals for the AAFP Cat Friendly Practice/ISFM Cat Friendly Clinic Programs, an AAFP Cat Friendly Certificate (catvets.com/certificate) and the ISFM Cat Friendly Veterinary Professional course (courses.icatcare.org).
The benefits of incorporating cat friendly interactions into veterinary practice include efficiency and effectiveness, resulting in time saving, and more positive emotions for the veterinary team, cats and caregivers. Feline and human safety, both physically and in terms of mental wellbeing, is enhanced, with the veterinary experience respecting the cat as an individual while achieving the required clinical outcome.

Summary Points
✜ The ‘2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques’ provide up-to-date information about best practices for veterinary professionals during feline interactions, taking into consideration both human and feline safety.
✜ Improved interactions with cats significantly enhance their welfare by correctly addressing both their current physical and emotional health.
✜ A cat friendly approach from the veterinary team allows successful examination and required interventions during the veterinary visit, improving team satisfaction and cat caregiver confidence in the veterinary team.
✜ The importance of understanding and responding to the current emotional state of the cat is key for successful interactions and enables every visit to be tailored to the individual.
✜ A cat friendly environment is also fundamental for achieving an optimal veterinary visit, and is the focus of the accompanying ‘2022 ISFM/AAFP Cat Friendly Veterinary Environment Guidelines’. 60
Supplemental Material
sj-docx-5-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-docx-5-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-docx-6-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-docx-6-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-docx-7-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-docx-7-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-pdf-1-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-pdf-1-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-pdf-2-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-pdf-2-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-pdf-3-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-pdf-3-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-pdf-4-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-pdf-4-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-pdf-8-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-pdf-8-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Supplemental Material
sj-pdf-9-jfm-10.1177_1098612X221128760 – Supplemental material for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques
Supplemental material, sj-pdf-9-jfm-10.1177_1098612X221128760 for 2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques by Ilona Rodan, Nathalie Dowgray, Hazel C Carney, Ellen Carozza, Sarah LH Ellis, Sarah Heath, Lee Niel, Kelly St Denis and Samantha Taylor in Journal of Feline Medicine and Surgery
Footnotes
Acknowledgements
The AAFP Cat Friendly Practice Program is sponsored by Zoetis, Boehringer Ingelheim, Ceva Animal Health, Elanco, Hill’s, IDEXX, Merck Animal Health, Purina Pro Plan Veterinary Diets and Royal Canin, and is supported by Wedgewood Pharmacy. ISFM Cat Friendly Clinic is sponsored by IDEXX, Ceva, Royal Canin, Boehringer Ingelheim and Zoetis. The AAFP and ISFM gratefully acknowledge the support of these companies in enabling them to deliver and build on their Cat Friendly Practice/Clinic Programs.
Supplementary material
The following files are available online at jfms.com and can also be accessed at catvets.com/interactions and ![]() .
.
✜ Video 1: How to interact with your cat – the Battersea way.
✜ Video 2: Inhibition and left gaze bias.
✜ Video 3: Teaching your cat to get used to medication.
✜ Video 4: Removing a cat from the carrier.
✜ Video 5: Approaching a cat.
✜ Video 6: Myofascial examination.
✜ Video 7: Cat friendly tips for thorough dental examinations.
✜ Video 8: Cat friendly interactions in practice.
✜ AAFP client brochure – ‘Visiting your veterinarian: getting your cat to the veterinary practice’.
✜ AAFP client brochure – ‘You and your cat deserve a Cat Friendly Practice®’.
✜ ISFM guide for cat carers – ‘Taking your cat to the veterinary clinic’.
✜ ISFM guide for cat carers – ‘Cat Friendly Clinic: cat friendly veterinary care’.
Conflict of interest
Nathalie Dowgray is employed part-time as a postdoctoral researcher at the Feline Healthy Ageing Clinic funded by Royal Canin. Ilona Rodan serves on an advisory board for Royal Canin. Sam Taylor is employed by Linnaeus. All members of the Task Force have also received financial remuneration for providing educational material, speaking at conferences and/or consultancy work; however, none of these activities cause any direct conflict of interest in relation to these Guidelines.
Funding
The members of the Task Force received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.