
Abstract
Objectives
The aims of this study were to compare the sedative effect, feasibility of venous angiocatheter placement and influence on heart rate (HR), systemic blood pressure (SBP) and echocardiographic variables of two multimodal anaesthetic protocols in uncooperative cats; and to compare their influence on HR, SBP and echocardiographic variables 20 mins after sedation and after elective ovariectomy.
Methods
Eighteen stray female cats randomly received intramuscular (IM) ketamine (2 mg/kg) and methadone (0.3 mg/kg) plus dexmedetomidine (7 µg/kg; group D, n = 9) or alfaxalone (2 mg/kg; group A, n = 9). A sedation score (0–15 [from none to good sedation]) was assigned at 5 mins, 10 mins, 15 mins and 20 mins after IM injection. Venous angiocatheter placement and echocardiographic examination feasibility scores (both from 0 to 3 [from very difficult to very easy]) were recorded at 20 mins. Echocardiography, HR and blood pressure measurements (Doppler and oscillometric methods) were performed at 20 mins and at the end of surgery.
Results
Sedation and angiocatheter feasibility scores did not differ significantly between groups (P >0.05); the feasibility score of echocardiographic examination was higher in cats in group D (P = 0.01). HR was higher in group A at 20 mins and after surgery (P <0.05). The systolic arterial pressure obtained with the Doppler method was statistically significantly higher in cats in group D than in group A at 20 mins (P = 0.01), while postoperatively there were no differences between groups. Cats in group D showed significantly higher atrial diameters (P <0.05) and slower atrial flows (P = 0.04) compared with group A; ventricular thickness and atrial function did not differ between groups (P >0.05). Most echocardiographic variables were not different at 20 mins vs postoperatively.
Conclusions and relevance
Both protocols allowed for effective sedation; however, cats in group D presented alterations in some echocardiographic measurements; the use of alfaxalone, combined with ketamine and methadone, is recommended to obtain a reliable echocardiographic evaluation in uncooperative cats.
Introduction
A complete echocardiographic examination, preferably performed on conscious animals, is essential to diagnose occult feline cardiomyopathies. 1 However, sedation is sometimes necessary in uncooperative cats to ensure patient compliance, to avoid stress and to allow for high-quality echocardiographic recordings.2–8 To be clinically useful, sedative agents should preserve hemodynamic conditions to minimally alter echocardiographic measurements. 9
The use of a single drug is often not enough to obtain an adequate sedation level, so a multimodal approach is required. Table 1 reports some multimodal anaesthetic protocols and their effects on the cardiovascular system and echocardiographic variables in cats.9–13 Most describe mono- and bi-dimensional left atrial (LA) and left ventricular (LV) variables, and LV systolic and diastolic function.9–11,13 However, only one study has evaluated the effects of sedative agents on the echocardiographic measurements of LA size and LV diastolic function in cats, 10 which are important components of the pathophysiology of feline cardiomyopathies.5,14–19
Multimodal anaesthetic protocols with effects on echocardiographic variables reported in the feline veterinary medicine literature

IM = intramuscular; ACP = acepromazine; BTF = butorphanol; IV = intravenous; KET = ketamine; LA = left atrium; LV = left ventricle; DEX = dexmedetomidine; BUPRE = buprenorphine; FS = fractional shortening; SV = stroke volume; PV = peak velocity; SBP = systemic blood pressure; AFX = alfaxalone; MTD = methadone; MDZ = midazolam; CV = cardiovascular; EF = ejection fraction; LA:Ao = left atrium to aortic root ratio; IVS = interventricular septum; CO = cardiac output; HR = heart rate; ID = internal diameter
The combination of alfaxalone, a low subanaesthetic dose of ketamine (1 mg/kg) and methadone does not affect the main echocardiographic variables, allowing for sufficient sedation in compliant domestic cats. 12 However, in uncooperative cats, higher doses of drugs are required, and it would be of interest to investigate whether higher doses significantly alter the echocardiographic parameters. The degree of sedation and feasibility of echocardiographic examination have not been evaluated when alfaxalone, a higher subanaesthetic dose of ketamine (2 mg/kg) and methadone are administered. This alfaxalone combination has not been compared with data obtained if dexmedetomidine plus ketamine and methadone at the same doses were given. Furthermore, knowing how echocardiographic parameters change if isoflurane is administered to achieve an adequate anaesthetic depth for elective surgery in premedicated cats may be helpful. To our knowledge, this combination has been investigated in dogs but not in cats. 20
The first aim of the study was to compare the sedative effect and feasibility of angiocatheter placement when one of two multimodal sedative protocols was used in uncooperative stray cats. The influence of the different protocols on heart rate (HR), systemic blood pressure (SBP) and echocardiographic variables, including LA measurements and diastolic function, was also investigated. The second aim was to compare HR, SBP and echocardiographic measurements recorded 20 mins after sedation and after isoflurane administration for elective surgery. We hypothesised that alfaxalone plus methadone and ketamine would provide similar sedation to a combination of dexmedetomidine, methadone and ketamine, thereby permitting the cat to be handled during echocardiographic investigation. It was also hypothesised that dexmedetomidine, methadone and ketamine could induce LA and LV function impairment.
Materials and methods
Subjects and study design
This prospective, randomised, blinded clinical study was approved by the Institutional Ethical Committee for Animal Care at the University of Milan (OPBA_29_2022) and included domestic shorthair female cats from different feline colonies referred to the Veterinary Teaching Hospital of the University of Milan (Lodi, Italy) for elective ovariectomy. Written informed consent was acquired from the legal representative of each cat. Food was withheld for 12 h and water for 6 h before the beginning of the study. Owing to their nervous/aggressive nature and poor complicity, the cats were not subjected to pre-anaesthetic clinical examinations or blood tests. Cats were considered healthy (American Society of Anaesthesiology status score I) based on complete blood count, blood chemistry profile and if they were free from feline immunodeficiency virus (FIV) and feline leukaemia virus (FeLV). Blood was obtained from the jugular veins of the sedated cats.
Cats were randomly (www.randomizer.org) allocated to one of two groups. Cats in group D received intramuscular (IM) dexmedetomidine 7 µg/kg (Dexdomitor; Vetoquinol), ketamine 2 mg/kg (Nimatek; Dechra) and methadone 0.3 mg/kg (Semfortan; Eurovet Animal Health BV). Cats in group A received IM alfaxalone 2 mg/kg (Alfaxan; Dechra), ketamine 2 mg/kg and methadone 0.3 mg/kg. The drug combinations were prepared and administered by an anaesthesiologist. Administration was via the quadriceps muscles, with the cat restrained with the help of a blanket while still in the trap cage.
After treatment administration (T0), the cats were placed in a cage inside a quiet room and observed for signs of sedation every 5 mins (T5) up to 20 mins (T20) by a second anaesthetist, who was blinded to group allocation. The degree of sedation was assessed by a modified numerical scale adapted from Gurney et al (Table 2), 21 for which the sum of the scores ranged from 0 (no sedation) to 15 (profound sedation). The operator assessed responses to tactile (touching the body) and auditory (hand-clapping) stimulation as well as motor skills to evaluate ataxia. At T20, an intravenous (IV) catheter was placed in the cephalic vein, blood work analysis was performed, and each cat underwent HR and arterial blood pressure (BP) measurement. Arterial BP was measured five times using a high-definition oscillometry (HDO) method (Vet HDO High Definition Oscillometry; medVET) and five times using the Doppler method (Minidop ES-100VX). Systolic (SAP), mean (MAP) and diastolic arterial (DAP) pressure were obtained with the oscillometric method, and only SAP was obtained with the Doppler method. The highest and lowest values were excluded, and the mean of each method was recorded. 22 The cuffs were selected according to the manufacturer’s instructions, with a cuff size of 1 and 2 cm for HDO and Doppler methods, respectively. The cuff was positioned distally to the left elbow, with the cat in right lateral recumbency. The first echocardiographic examination (fEchoCG) was performed 10 mins after IV catheter positioning.
Sedation modified numeric scale (adapted from Gurney et al) 21
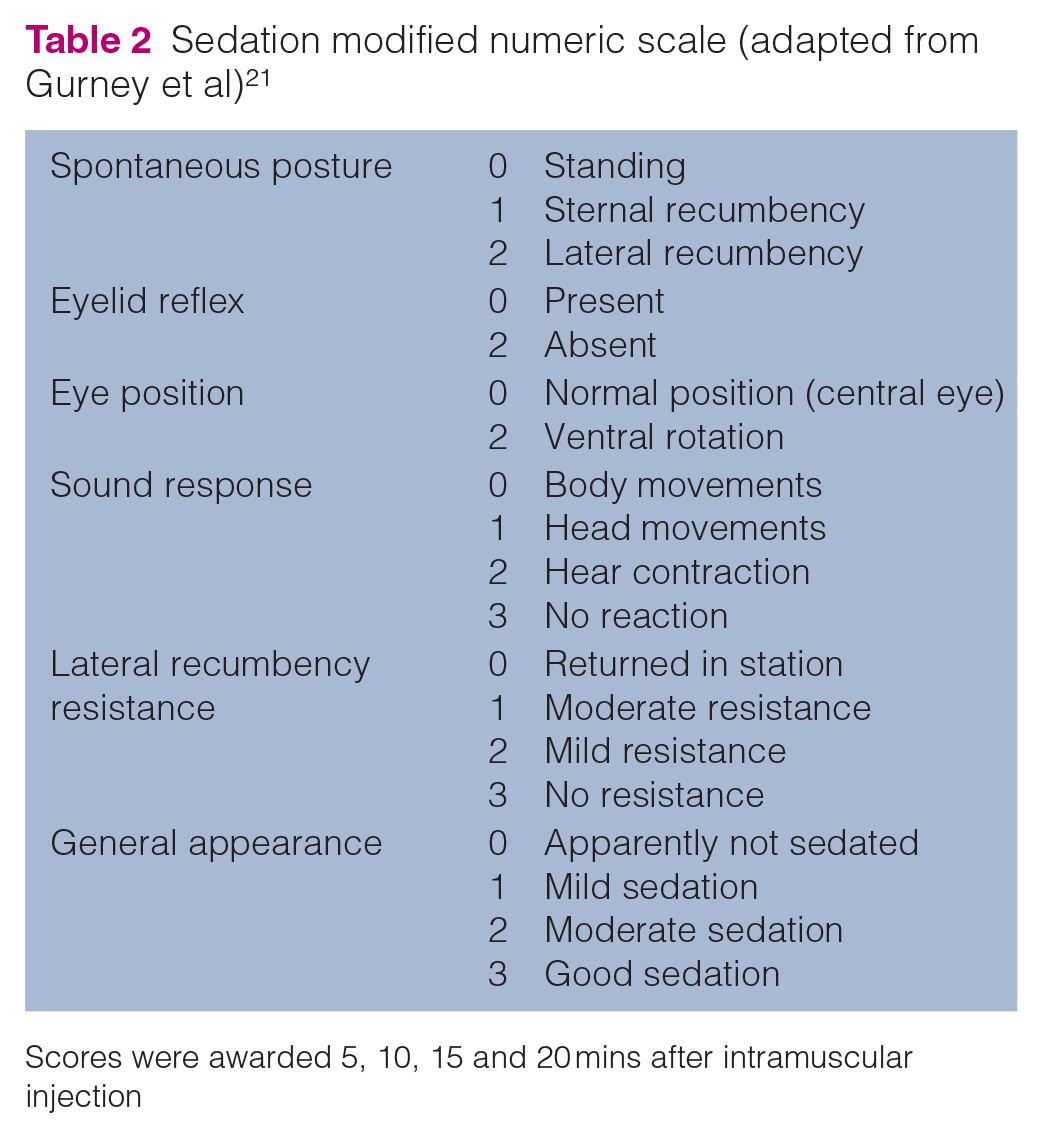
Scores were awarded 5, 10, 15 and 20 mins after intramuscular injection
The ease of restraint during both IV catheter insertion and echocardiographic procedures were assessed using two simple descriptive scales modified from Bortolami et al, 23 ranging from 0 (very difficult) to 3 (very easy), by the same blinded anaesthetist (Tables 3 and 4). An IM dexmedetomidine (group D) or alfaxalone (group A) supplementary dose (2 μg/kg and 1 mg/kg, respectively) was administered if sedation was insufficient for the angiocatheter placement. In the case of evident movements, IV propofol (Proposure; Boehringer Ingelheim) was administered to effect during the echocardiographic procedure; the dose required was recorded. Throughout the observational period, any adverse reaction such as twitches, tremors, excitement or vomiting were recorded. After the fEchoCG, all cats underwent ovariectomy; general anaesthesia was induced with IV propofol and maintained with isoflurane in oxygen after orotracheal intubation. Five minutes postoperatively, defined as skin closure and isoflurane interruption, a second echocardiographic examination (sEchoCG) and BP measurements (HDO and Doppler) were performed.
Simple descriptive scale of intravenous catheter placement feasibility (adapted from Bortolami et al) 23

Echocardiographic evaluation feasibility simple descriptive scale (adapted from Bortolami et al) 23
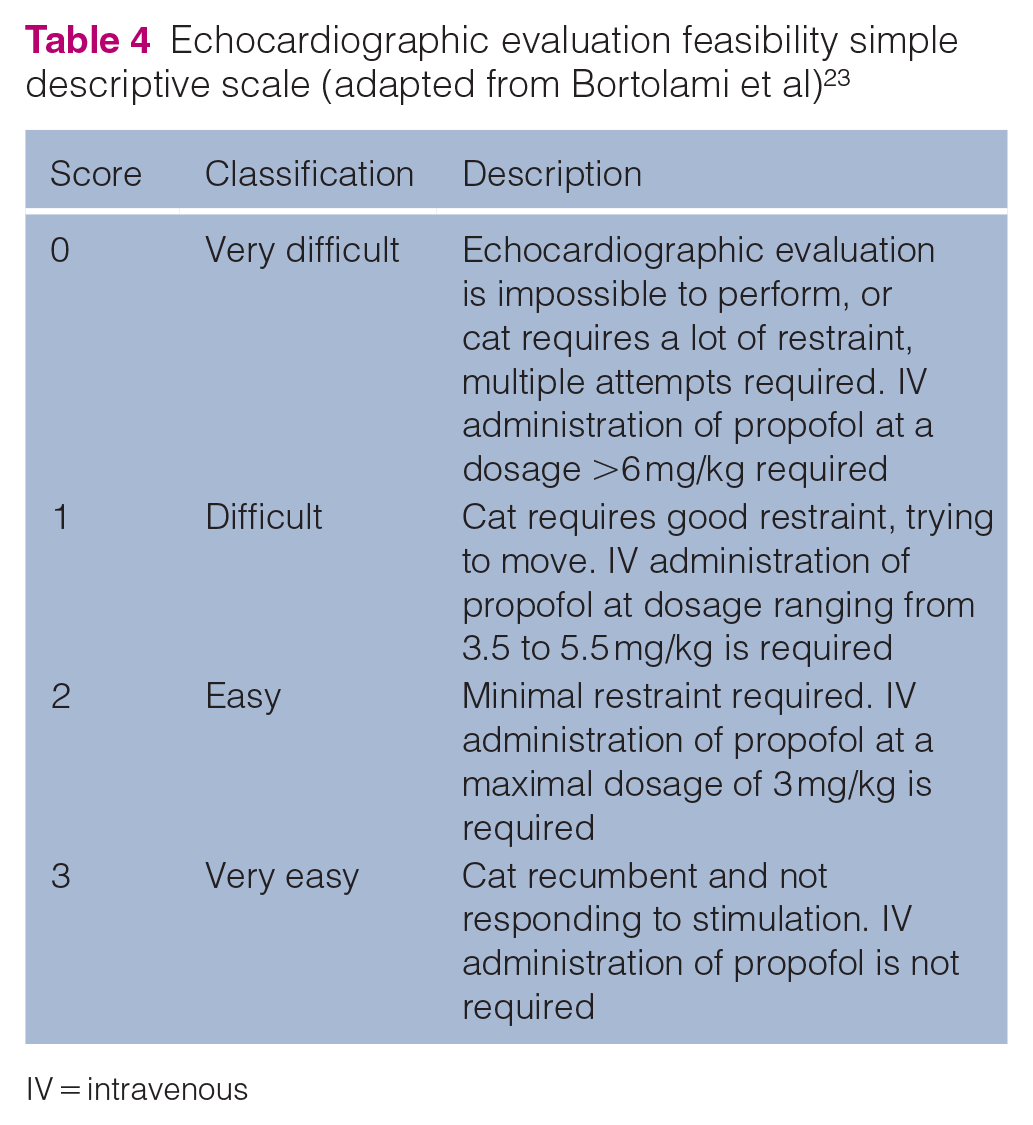
IV = intravenous
The fEchoCG and sEchoCG procedures were performed by an experienced cardiologist and measured offline by the same operator (MB), blinded to group allocation. Echocardiographic examinations were performed with an Esaote MyLab30 Vet Gold ultrasound machine (Esaote Medical Systems), equipped with a 4–11 MHz multifrequency phased array transducer, with the cats positioned both in right and left lateral recumbency, and shaved at the heart projection area on each side. All echocardiographic measurements were taken in accordance with the guidelines of the Echocardiography Committee of the Specialty of Cardiology, American College of Veterinary Internal Medicine, and the most recent literature.5,10,12–16,24,25 The evaluated echocardiographic measurements are provided in Table 5. For each variable, a mean of five measurements was recorded. A standard electrocardiogram was obtained to evaluate HR and diagnose any cardiac arrhythmias. Intra-observer variabilities were calculated by reanalysing one of the scans from each cat after a period of at least 8 weeks and comparing the results with the original data.
Description of the echocardiographic measurements included in the study
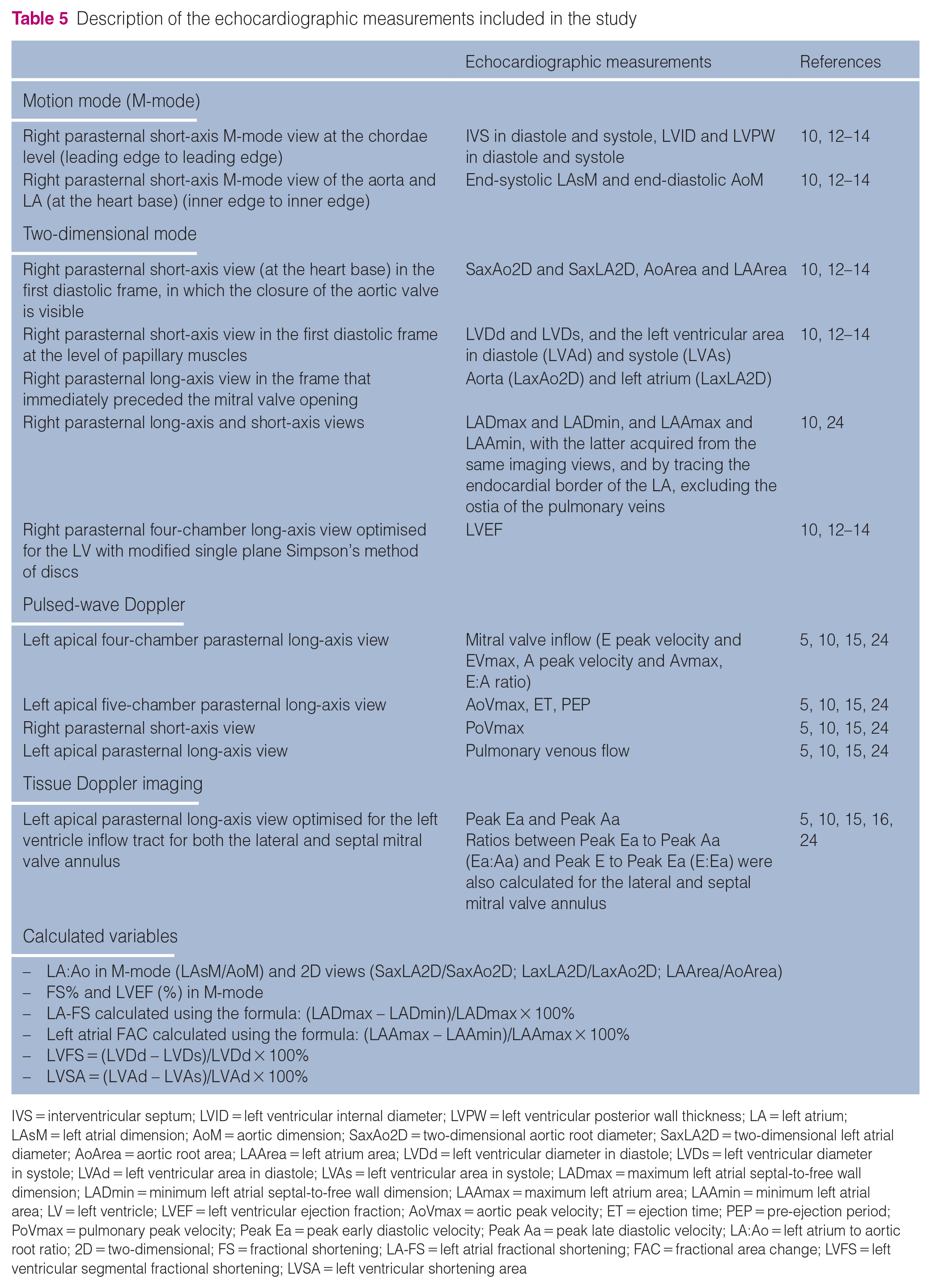
IVS = interventricular septum; LVID = left ventricular internal diameter; LVPW = left ventricular posterior wall thickness; LA = left atrium; LAsM = left atrial dimension; AoM = aortic dimension; SaxAo2D = two-dimensional aortic root diameter; SaxLA2D = two-dimensional left atrial diameter; AoArea = aortic root area; LAArea = left atrium area; LVDd = left ventricular diameter in diastole; LVDs = left ventricular diameter in systole; LVAd = left ventricular area in diastole; LVAs = left ventricular area in systole; LADmax = maximum left atrial septal-to-free wall dimension; LADmin = minimum left atrial septal-to-free wall dimension; LAAmax = maximum left atrium area; LAAmin = minimum left atrial area; LV = left ventricle; LVEF = left ventricular ejection fraction; AoVmax = aortic peak velocity; ET = ejection time; PEP = pre-ejection period; PoVmax = pulmonary peak velocity; Peak Ea = peak early diastolic velocity; Peak Aa = peak late diastolic velocity; LA:Ao = left atrium to aortic root ratio; 2D = two-dimensional; FS = fractional shortening; LA-FS = left atrial fractional shortening; FAC = fractional area change; LVFS = left ventricular segmental fractional shortening; LVSA = left ventricular shortening area
Statistical analysis
Sample size calculation was performed using G-Power software. A minimum of nine cats per group was considered sufficient to have a power of 80%, with an alpha level of 0.05 and an effect size of 0.5 with regard to feasibility scores for venous angiocatheter placement (anticipated mean ± SD of 2 ± 1 for groups D and A).
Statistical analysis was performed using SPSS Statistics version 27 (IBM). Data were evaluated for normality with the Kolmogorov–Smirnov test. Non-normally distributed data were presented as median (range) and compared using the Mann-Whitney U-test (or the Kruskal–Wallis rank test for median difference analysis). Values from fEchoCG and sEchoCG were compared, as were the data obtained from each group. Intra-observer variability was quantified using a standard paired Student’s t-test, and the coefficient of variation (CV) was defined as the mean difference between measurements/average of measurements per 100%. The authors considered good agreement when the CV did not exceed 20%. A P value <0.05 was considered significant.
Results
One cat was excluded because it was diagnosed with hypertrophic phenotype cardiomyopathy and three cats were excluded because they were FeLV positive. Eighteen healthy female cats with a mean estimated age of 12 months (interquartile range [IQR] 9–24) and a mean body weight of 2.89 kg (IQR 2.65–3) were included in the study. Age and body weight were not statistically significantly different between groups (P = 0.89 and P = 0.08, respectively).
Sedation score (from T5 to T20) and angiocatheter insertion feasibility score were not statistically significantly different between groups (P >0.05). In group D, maximum sedation was achieved at T15 and maintained up to T20, with a median score of 12/15, while in group A the higher score was obtained at T10 and the median was 11/15. Mild side effects, such as tremors and hyper-reactivity to tactile stimuli and sounds (hand-clapping), were detected in five cats in group A. The feasibility score of the fEchoCG was statistically significantly higher in group D (median score 2 vs median score 1) (P = 0.01). To perform the echocardiographic procedures, 7/9 cats in group D and 9/9 cats in group A required supplementary propofol (7 mg [IQR 3.5–7.5] and 10 mg [IQR 8–16], respectively).
HR was statistically significantly higher in cats in group A compared with those in group D, both at T20 (173 beats/min [bpm; IQR 162–209] vs 89 bpm [IQR 80.0–104.8]; P = 0.01) and postoperatively (122 bpm [IQR 118–125] vs 104 bpm [IQR 92–117]; P = 0.01).
At T20, SAP obtained via the Doppler method was statistically significantly higher in cats in group D (125 mmHg [IQR 125–140]) compared with cats in group A (105 mmHg [IQR 80–105]; P = 0.01); no statistically significant differences were found between groups after surgery (P = 0.75), although tremors and interferences with the Doppler detector did not allow for the measurement of SAP in two cats in group A. The same was seen for SAP obtained with HDO at T20 (group D: 132 mmHg [IQR 122–159]; group A: 97 mmHg [IQR 93–103]; P = 0.01) and postoperatively (group D: 122 mmHg [IQR 118–122]; group A: 104 mmHg [IQR 92–117]; P = 0.09). There was no difference in SAP between the two methods at T20 or postoperatively (P >0.05). Statistically significant differences were seen in MAP and DAP (P = 0.01 and P = 0.03, respectively) measured with HDO between the groups at T20 (MAP in group D: 101 mmHg [IQR 92–101]; and MAP in group A: 72 mmHg [IQR 71–74]; DAP in group D: 81 mmHg [IQR 77–101]; and DAP in group A: 59 mmHg [IQR 56–63]) but not postoperatively (P >0.05).
All echocardiographic variables obtained from fEchoCG and sEchoCG were within the reference intervals (Table 6).2,16,24,26–29 The median time between fEchoCG and sEchoCG was 50 mins (IQR 35.5–55) in group D and 50 mins (IQR 42.5–59.5) in group A. Table 6 reports the echocardiographic values measured in groups A and D, respectively, at T20 (fEchoCG) and after surgery (sEchoCG). Differences between groups are also reported. Table 7 reports the differences between fEchoCG and sEchoCG in each group.
Comparison between group D and group A measurements taken during the first echocardiographic examination (fEchoCG; 20 mins after premedication) and during the second echocardiographic examination (sEchoCG; postoperatively)

Values in bold are statistically significant (P <0.05)
IQR = interquartile range; IVSd = interventricular septum thickness in diastole; LVIDd = left ventricular internal diameter in diastole; LVPWd = left ventricular posterior wall thickness in diastole; LAsM = end-systolic left atrial dimension from the right parasternal short-axis M-mode view; AoM = end-diastolic aortic dimension from the right parasternal short-axis M-mode view; SaxLA2D = left atrial diameter from short-axis two-dimensional view; SaxAo2D = aortic root diameter from short-axis two-dimensional view; LaxLA2D = left atrial diameter from right parasternal long-axis 2D view; LaxAo2D = aortic root diameter from right parasternal long-axis 2D view; AoA = aortic root area from right parasternal short-axis view; LAA = left atrium area; Evmax = E peak velocity; Avmax = A peak velocity; E:A ratio = E peak velocity/A peak velocity; AoVmax = aortic peak velocity; ET = ejection time; PEP = pre-ejection period; PoVmax = pulmonary peak velocity; FS = fractional shortening; EF = ejection fraction; LADmax = maximum left atrial septal-to-free wall dimension from right parasternal long-axis view; LADmin = minimum left atrial septal-to-free wall dimension from right parasternal long-axis view; LAAmax = maximum left atrial area from right parasternal long-axis view; LAAmin = minimum left atrial area from right parasternal long-axis view; LA-FS = left atrial fractional shortening; LA-FAC = left atrial fractional area change; LAD = short-axis left atrial diameter in diastole; Ao = short-axis aortic diameter in diastole; LVDs = systolic left ventricular dimension; LVDd = diastolic left ventricular dimension; LVPWs = systolic left ventricular posterior wall thickness; IVSs = systolic interventricular septal thickness; LVAs = systolic left ventricular area measured at the level of the chordae tendineae; LVAd = diastolic left ventricular area measured at the level of the chordae tendineae; LVEF = left ventricular ejection fraction; LVSF = left ventricular shortening fraction; LVSA = left ventricular shortening area; IVRT = isovolumic relaxation time; DTE = deceleration time of early diastolic transmitral flow; Adur = duration of A wave; Peak D = peak velocity of pulmonary vein diastolic flow; Peak S = peak velocity of pulmonary vein systolic flow; Peak AR = peak velocity of pulmonary vein reversal flow at atrial contraction; ARdur = duration of AR wave; S:D = ratio between Peak S to Peak D
Comparison between group D measurements during the first echocardiographic examination (fEchoCG; 20 mins after premedication) and during the second echocardiographic examination (sEchoCG; postoperatively) and group A measurements during fEchoCG (20 mins after premedication) and during sEchoCG (postoperatively)

Values in bold are statistically significant (P <0.05)
IQR = interquartile range; IVSd = interventricular septum thickness in diastole; LVIDd = left ventricular internal diameter in diastole; LVPWd = left ventricular posterior wall thickness in diastole; LAsM = end-systolic left atrial dimension from the right parasternal short-axis M-mode view; AoM = end-diastolic aortic dimension from the right parasternal short-axis M-mode view; SaxLA2D = left atrial diameter from short-axis two-dimensional view; SaxAo2D = aortic root diameter from short-axis two-dimensional view; LaxLA2D = left atrial diameter from right parasternal long-axis 2D view; LaxAo2D = aortic root diameter from right parasternal long-axis 2D view; AoA = aortic root area from right parasternal short-axis view; LAA = left atrium area; Evmax = E peak velocity; Avmax = A peak velocity; E:A ratio = E peak velocity/A peak velocity; AoVmax = aortic peak velocity; ET = ejection time; PEP = pre-ejection period; PoVmax = pulmonary peak velocity; FS = fractional shortening; EF = ejection fraction; LADmax = maximum left atrial septal-to-free wall dimension from right parasternal long-axis view; LADmin = minimum left atrial septal-to-free wall dimension from right parasternal long-axis view; LAAmax = maximum left atrial area from right parasternal long-axis view; LAAmin = minimum left atrial area from right parasternal long-axis view; LA-FS = left atrial fractional shortening; LA-FAC = left atrial fractional area change; LAD = short-axis left atrial diameter in diastole; Ao = short-axis aortic diameter in diastole; LVDs = systolic left ventricular dimension; LVDd = diastolic left ventricular dimension; LVPWs = systolic left ventricular posterior wall thickness; IVSs = systolic interventricular septal thickness; LVAs = systolic left ventricular area measured at the level of the chordae tendineae; LVAd = diastolic left ventricular area measured at the level of the chordae tendineae; LVEF = left ventricular ejection fraction; LVSF = left ventricular shortening fraction; LVSA = left ventricular shortening area; IVRT = isovolumic relaxation time; DTE = deceleration time of early diastolic transmitral flow; Adur = duration of A wave; Peak D = peak velocity of pulmonary vein diastolic flow; Peak S = peak velocity of pulmonary vein systolic flow; Peak AR = peak velocity of pulmonary vein reversal flow at atrial contraction; ARdur = duration of AR wave; S:D = ratio between Peak S to Peak D
Five (55.6%) cats in group D and four (44.4%) in group A presented false tendons without LV obstruction. One cat in group A (11.1%) had mild mitral insufficiency without mitral valve changes and without left outflow tract obstruction and systolic anterior movement of the septal leaflet. Two (22.2%) cats in group D had mild aortic insufficiency on continuous wave Doppler, and in one of these cats aortic regurgitation was seen only with colour Doppler after surgery. At the beginning of the echocardiographic examination, one cat (11.1%) in group A showed ventricular premature complexes, which resolved spontaneously after 2 mins.
Intra-observer variability in echocardiographic measurements ranged from 0.3% to 13.2%. M-mode measurements showed higher intra-observer variability than two-dimensional mode measurements.
Discussion
Echocardiographic examination is essential for the diagnosis and management of feline cardiomyopathies. In aggressive/uncooperative cats, echocardiography can be performed under sedation, to reduce the stress of restraint and improve image quality. 10 An ideal sedative drug or drug combination must guarantee a good quality of sedation (characterised by the absence of resistance to lateral recumbency and muscle relaxation), without affecting the cardiovascular system, to obtain echocardiographic measurements in line with those obtained in non-sedated cats. To reduce side effects and maximize the degree of sedation, it is necessary to use a multimodal approach. The most commonly used sedatives are alpha-2 agonists such as dexmedetomidine, opioids such as methadone or butorphanol, phenothiazines such as acepromazine, dissociative anaesthetic agents such as ketamine and neuroactive steroids such as alfaxalone. 10 Although these drugs are used to facilitate echocardiography in uncooperative cats, no studies have compared the sedative and cardiovascular effects, particularly on echocardiographic LA function, of an IM combination of methadone and ketamine at a high sub-anaesthetic dose (2 mg/kg) plus dexmedetomidine or alfaxalone.
In the present study, no significant differences were seen in sedation scores between groups at each time point. IV catheter placement is an invasive and painful procedure that can be stressful for the animal, and sedation is often required in uncooperative cats. 30 The results showed that there was no significant difference between the two protocols, indicating that both reached a sedation level sufficient to perform this procedure without administering additional IM drugs. To perform the echocardiographic examination, with cats completely immobile, patients in group D required a lower propofol dose than cats in group A. This result can be explained by considering the higher, but not statistically significant, sedation score obtained in cats in group D at T20. Mild side effects, such as tremors and hyper-reactivity to stimuli, were detected in cats in group A. Similar side effects (contraction of the ears and limbs, and increased reactivity to stimuli and sounds) are reported in other studies following IM administration of alfaxalone in cats.9,31–36 Although it has been reported that dexmedetomidine at a low IM dose (5 µg/kg) promotes emesis, 37 this side effect was not seen in cats in group D, perhaps due to the combination of dexmedetomidine with methadone, which may cross the blood–brain barrier more rapidly into the central nervous system, inhibiting the emetic centre.38,39
A decrease in HR was seen at T20 in cats premedicated with dexmedetomidine. Vasoconstriction caused by dexmedetomidine induced a higher SAP in cats in group D than in cats in group A, both at T20 and postoperatively. There were no differences in SAP seen between the HDO and Doppler methods, probably owing to the immobility of the patients and, consequently, the ease of measurement.
At fEchoCG, cats in group D showed larger LA and LV diameters and areas than cats in group A, while atrial function and ventricular thicknesses were not significantly different between groups. The measurement of the left atrium to aortic root ratio (LA:Ao) was not significantly different between groups. The left auricle flow velocity was lower in group D, as well as the LV fractional shortening (LVFS) and the LV ejection fraction (LVEF) obtained in M-mode.
Comparison between the echocardiographic measurements taken at fEchoCG and sEchoCG showed fewer differences in group A than in group D, confirming that the alfaxalone protocol creates the least echocardiographic variability over time.
Dexmedetomidine increased the diameters and areas of the aorta and LA, but the left atrial area:aortic root area and left atrial dimension:aortic dimension ratios were not significantly different between groups. The measurement of the LA:Ao is reliable with both protocols, although the maximum atrial diameter and the maximum atrial area were overestimated with the use of dexmedetomidine. 40 From the results of this study, dexmedetomidine did not alter the functionality of the LA, allowing determination of the percentage of reduction of the atrial diameter in systole.
Dexmedetomidine caused an increase in LV diameters and areas due to the increased diastolic filling time, and the increase in telediastolic volume induced by bradycardia; 21 moreover, it determined a decrease in LVSF and LVEF, which evaluate the systolic performance and contractile response of the LV, respectively. Decreased contractility contributed, along with increased afterload, to increased BP. 41 Therefore, with this protocol, there was a risk of overestimating the size of the LV and underestimating ventricular function.
These findings show that dexmedetomidine – at the dose proposed in the present study – could induce the cardiologist to overestimate the atrial size and the measurement of ventricular diameters, and to underestimate the diagnosis of dynamic obstructive forms and the left auricle flow velocity. In this way, the cardiologist may erroneously suggest an increased risk of thromboembolism due to the marked bradycardia and the increased preload. 42 Furthermore, bradycardia can cause an increase in aortic and pulmonary regurgitations. 41
When administered at a dose <5 mg/kg, alfaxalone has no effect on cardiac output, LV telesystolic volume, LA size, short-axis aortic diameter in diastole, LA:Ao or LVEF. No changes in ventricular thicknesses and LVFS were also reported.43,44 In the present study, alfaxalone administration allowed the operator to obtain reliable measurements of ventricular thicknesses, LA:Ao, left chambers size diameter, left auricle flow velocity and LA function. In addition, it permitted assessment of the real risk of arterial thromboembolism, and, at a dose of 2 mg/kg, it did not result in bradycardia, facilitating the diagnosis of the dynamic obstructive cardiomyopathies.
In this study, abnormal ventricular tendons were detected in 47% of cats; these abnormal tendons are considered to be an anatomical variant of little relevance in non-purebred cats.45,46 These structures are present both in healthy cats and in patients with cardiomyopathy. Therefore, the presence of false tendons should be considered a normal finding in cats, and needs to be considered in echocardiographic measurements, in order to avoid the overestimation of ventricular thicknesses and the presence of cardiomyopathies.
This study had several limitations. First, the study was performed with uncooperative cats, so it was not possible to obtain basal echocardiographic measurements. Second, the study subjects were young cats (aged 1–2 years). 10 It is possible that sedation may have different effects on echocardiographic variables in older cats, with different myocardial/metabolic conditions. Another limitation is that this was a clinical study, and it was not possible to subject the same group of cats to both protocols. Furthermore, cats in both groups received different doses of propofol during fEchoCG, which could have differently influenced the echocardiographic variables. Finally, based on the results obtained, it is not known if the described sedative protocols have effects on cardiopathic cats and, therefore, should be used with caution if cardiopathies are suspected.
Conclusions
The results of this study showed that both sedative combinations permit the placement of venous angiocatheters, with a good level of sedation, even in aggressive/uncooperative cats. However, 7/9 cats in group D and 9/9 in group A required supplementary propofol to ensure immobility during the echocardiographic examination. The alfaxalone protocol seemed to be preferable for an echocardiographic examination in uncooperative cats, allowing echocardiographic measurements as similar as possible to those of non-sedated cats (comparing the physiological variables evaluated) to be obtained. However, the dexmedetomidine protocol did not affect LA function or LV thickness. It must be highlighted that the study subjects were healthy cats. It is possible that sedation protocols may differently influence LA and LV size and function in cats with cardiac diseases, haemodynamic alterations or metabolic disorders.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.