
Abstract
Practical relevance:
Diabetes mellitus (DM) is one of the most common feline endocrine disorders. It has been shown by several studies that DM in cats frequently coexists with pancreatitis.
Clinical challenges:
It has not been definitively established what the exact pathogenetic association between DM and pancreatitis is in the cat. However, the association between these two conditions is most likely bidirectional, with DM predisposing cats to pancreatitis and vice versa. Diagnosis of pancreatitis in cats with DM is crucial because concurrent pancreatitis commonly leads to difficulties in the management of DM. When pancreatitis is associated with diabetic ketoacidosis (DKA), therapeutic management is even more challenging.
Aims:
This review focuses on the concurrent presence of DM or DKA and pancreatitis in cats, mainly focusing on their clinical management.
Evidence base:
Information provided in this review is based on feline-specific clinical research when available. In addition, comparative and human research, as well as clinical experience, has been used to enrich knowledge in areas where feline-specific research is not yet available.
Introduction
Diabetes mellitus (DM) is one of the most common feline endocrine disorders, with 1/200 cats attending primary care practices estimated to be affected.
1
In humans, DM is classified as type 1, type 2, ‘other specific types of diabetes’ and gestational DM. 3 Type 2 diabetes, associated with insulin resistance and obesity in adults, is approximately nine times more frequent than type 1 diabetes. 4 The category ‘other specific types of diabetes’ includes disturbances in glucose metabolism due to other disorders (eg, other endocrinopathies or pancreatic disorders) or uncommon conditions (eg, genetic disorders). 3 Historically, diabetes due to exocrine pancreatic disease was described as pancreatogenic or pancreatogenous DM, but more recent literature refers to it as type 3c diabetes. 5 The most commonly identified cause of type 3c diabetes in humans is chronic pancreatitis. 6
It is currently assumed that most diabetic cats have type 2-like DM, similar to what is observed in humans. 7 The category ‘other types of diabetes’ is also thought to apply in cats, although it is less clearly defined than in human diabetology. When diseases such as hypersoma-totropism or pancreatitis are present in a diabetic cat, DM should probably be classified as ‘secondary/associated with another disease’. 8
Pancreatitis is the most common disorder of the exocrine pancreas in cats and, in the majority of cases, is believed to be idiopathic.9,10 Classification of feline pancreatitis has not been universally standardised and, therefore, there is often confusion with regard to the terminology used. Feline pancreatitis is most commonly classified based exclusively on histopathological criteria, and several studies have described and categorised the histopathological features of the pancreas in cats with pancreatitis.11–13
There are two main forms of pancreatitis in cats: acute and chronic.11,12 Some authors have further differentiated interstitial and necrotising pancreatitis, but this differentiation is often only possible post mortem. Predominant histopathological features of acute pancreatitis are neutrophilic inflammation, peripancreatic fat necrosis and, in cases of severe disease, pancreatic necrosis. In contrast to acute pancreatitis, chronic pancreatitis is characterised by lymphocytic plasmacytic infiltration and permanent histopathological lesions;11,12 the latter is the histopathological feature that typically differentiates acute and chronic pancreatitis. Fibrosis and acinar atrophy represent the main permanent histopathological changes that define chronic pancreatitis. It should be noted that some cats show histopathological evidence of both acute and chronic pancreatitis (eg, necrosis and concurrent fibrosis or a mixed inflammatory infiltrate).
Relationship between pancreatitis and DM
Humans
The relationship between pancreatitis and dM in humans is believed to be bidirectional. Some studies have shown that patients with DM are more likely to develop pancreatitis, 5 with one meta-analysis, for example, showing that diabetic individuals were 92% more likely to develop acute pancreatitis compared with controls. 14 However, more commonly, pancreatitis precedes DM and is believed to be implicated in the pathogenesis of DM. 5 Although an episode of acute pancreatitis may rarely lead to DM, DM typically develops as a result of chronic pancreatitis. In fact, increased disease duration is an important risk factor for the development of DM in chronic pancreatitis. 5 Therefore, it seems that continuous inflammation of the pancreas is necessary in most cases for the development of DM.
Although the exact mechanisms involved in the pathogenesis of DM in chronic pancreatitis are not fully understood, both deficient insulin production and insulin resistance are believed to occur. The increased concentration of inflammatory cytokines within the pancreatic parenchyma leads to beta (p)-cell dysfunction and subsequent loss. In more advanced stages, chronic pancreatitis leads to pancreatic fibrosis that eventually impairs endocrine pancreatic function. 5
Cats
An association between DM and pancreatitis has also been identified in cats and dogs, and their pathogenic relationship has been the subject of extended discussions and research.15,16 In cats, it is fairly well established, both in clinical and histopathological investigations, that
In many cases where DM and pancreatitis coexist, it is impossible to determine which disease came first. As in humans, it is likely that a bidirectional association exists, with pancreatitis both occurring as a result of DM and having a causal effect on DM. 15 In relation to the former, experimental hyperglycaemia has been shown to induce pancreatic inflammation in cats. 22 Regarding the latter, extension of inflammation from the exocrine to the endocrine pancreas can lead to progressive destruction of the islets of Langerhans, impaired p-cell function and, subsequently, DM. Peripheral insulin resistance is also likely to occur. As in humans, chronic pancreatitis is believed to be more commonly related to the development of DM in cats. 23 However, acute exacerbations of chronic pancreatitis commonly occur, and therefore many cats present with DM and acute pancreatitis.
Diagnosis of DM and pancreatitis
Diagnosis of DM in cats is typically straightforward and is based on the presence of persistent hyperglycaemia and glucosuria in conjunction with compatible clinical signs, such as polyuria/polydipsia, polyphagia and weight loss.7,24
In contrast, the clinical diagnosis of pancreatitis is often challenging in cats and requires a combination of findings from the history and clinical presentation, pancreatic markers and imaging studies.9,11 With regards to clinical presentation, cats with pancreatitis often show mild and non-specific clinical signs such as anorexia and depression.
In terms of pancreatic markers, fPLI is a species-specific immunoassay that is currently considered the most sensitive and specific serum test for the diagnosis of pancreatitis in cats.9,11 However, especially in cases of chronic pancreatitis, fPLI can be normal and, therefore, a normal fPLI result does not 100% exclude the presence of pancreatitis.11,25 More recently developed colorimetric lipase activity assays (such as the 1,2-o-dilauryl-rac-glycero-3-glu-taric acid-[6’-methylresorufin] ester [DGGR] assay) have shown better performance than traditional catalytic assays, but results from different studies are conflicting, and their clinical value has not yet been established.26–29
For imaging, abdominal ultrasound is currently considered the modality of choice for the diagnosis of pancreatitis in cats (Figure 1). 11 (See Griffin 30 for a review of ultrasonographic examination of the normal and diseased pancreas.) It is important to note that a normal pancreas on ultrasound examination cannot rule out pancreatitis. This can be true of acute pancreatitis cases but is particularly the case with chronic or mild pancreatitis, where pancreatic changes are often not detected. Although abdominal ultrasound is considered to have high specificity, its sensitivity ranges between 11 and 67%. 11 In cases where ultrasonographic examination of the pancreas is unremarkable but clinical suspicion of pancreatitis is high, it has been recommended that ultrasound examination is repeated 2-4 days later.30,31

Ultrasound image of the left limb of the pancreas (between the measuring calipers) in a 10-year-old domestic shorthair cat with chronic pancreatitis. The pancreas is enlarged, mildly irregular in shape and diffusely heterogeneous in echogenicity. The pancreas appears mostly hyperechoic, likely representing pancreatic fibrosis due to chronic ongoing inflammation
Recommended diagnostic work-up for cats with DM and suspected pancreatitis
It is the authors’ opinion that cats with DM should be examined at least once for pancreatitis using Spec fPL and/or abdominal ultrasound. In cats with good glycaemic control and no other clinical signs, repeated testing for pancreatitis may be performed every 6–12 months. In diabetic cats that have even mild signs of inappetence, depression, gastrointestinal (GI) signs (eg, occasional vomiting) or that have poor glycaemic control, testing for pancreatitis should be performed more often as needed. The Spec fPL assay can be used to assess pancreatic inflammation in cats with further concurrent diseases (such as chronic kidney disease [CKD]) as these do not appear to affect serum Spec fPL concentrations. 32 The effect of concurrent diseases, such as CKD, have not been reliably evaluated for other markers of pancreatitis (such as DGGR lipase), however, and their use in these cases is not recommended. 33
Basic principles of the management of DM
Insulin is the key element in the therapeutic management of feline DM. Long-acting or intermediate-acting insulin products are usually recommended, and the treatment should be started as soon as possible after diagnosis. The initial approach for management of a diabetic cat is to initiate insulin therapy with glargine (100 U/ml [Lantus; Sanofi-Aventis] or 300 U/ml [Toujeo; Sanofi]), protamine zinc insulin (PZI; Prozinc, Boehringer Ingelheim) or insulin detemir (Levemir; Novo Nordisk) at a starting dose of 1-2 units (U) per cat q12h.7,24 After the initiation of insulin treatment, periodic monitoring is necessary to find the appropriate insulin dose and ensure safe and effective treatment. Diabetic cats with concurrent chronic pancreatitis are managed with the same insulin products that are usually recommended for uncomplicated feline diabetes.
Monitoring and insulin dose adjustment
In unstable diabetic patients, usually characterised by persistent hyperglycaemia, a tendency to develop hypoglycaemia and/or high glycaemic variability and diabetic ketoacidosis (DKA), close glucose monitoring can prevent clinical hypoglycaemia – a common and serious (potentially life-threatening) complication of insulin. Close glucose monitoring can also allow for more appropriate adjustments of the insulin dose; initially, re-evaluations are recommended at 1, 2–3, 3–4 and 8–10 weeks after diagnosis. Cats with concurrent DM and chronic pancreatitis are often unstable diabetic patients, and so for these cats frequent glucose monitoring is more important than in a well-controlled diabetic animal without pancreatitis.
Long-term care of diabetic cats and adjustments to their medications should be based primarily on owner observations in association with periodic in-clinic assessments; the latter should include a complete physical examination, body weight evaluation, and measurement of serum glucose and fruc-tosamine concentrations. Glucose concentrations and glucose curves are usually initially carried out in the clinic. Subsequently, if appropriately trained, most owners can perform home monitoring by measuring capillary blood glucose with a portable blood glucose meter validated for cats. With motivated owners who have a calm diabetic cat, the use of a continuous (or flash) glucose monitoring system (eg, FreeStyle Libre; Abbott Laboratories), which measures interstitial glucose, can be proposed, and the sensor applied, within the first weeks of treatment (Figure 2). 34 Aiming for normal or near-normal blood glucose concentrations is not recommended, as this increases the risk of hypoglycaemia. Most diabetic cats are considered well controlled if their blood glucose is maintained at between 80 and 200 mg/dl (4.4–11.1 mmol/l). Insulin dose adjustments, if required, are made in steps of 0.5–1 U/injection. In the case of symptomatic hypoglycaemia, an insulin dose reduction of 25–50% is recommended.

Procedure for applying a continuous glucose monitoring system (FreeStyle Libre; Abott Laboratories) in a diabetic cat. (a) Shave the dorsal aspect of the neck. (b) Clean the skin with chlorhexidine and alcohol wipes (allow the site to dry before proceeding; if necessary, use dry gauze). (c) Peel the lid completely off the sensor pack and unscrew the cap from the sensor applicator. (d) Line up the dark mark on the sensor applicator with the dark mark on the sensor pack and, on a hard surface, press down firmly on the sensor applicator until it comes to a stop; lift the sensor applicator out of the sensor pack. (e) The sensor applicator is ready to apply the sensor; add some drops of glue to the surface of the sensor that will contact the skin. (f) To apply the sensor, place the sensor applicator over the site and push down firmly. (g) Make sure the sensor is secure. (h) Open the FreeStyle LibreLink app on a smartphone, select ‘start new sensor’ and hold the phone within 4 cm of the sensor to scan it. (i) The sensor will be ready to provide a glucose reading after 60 mins. (j) Secure the sensor by covering it with a plaster patch. The sensor is further secured with (k) a cotton bandage and (l) an elastic bandage. The cat is then ready to go home
Glucose variability
As continuous glucose monitoring systems (eg, FreeStyle Libre) are increasingly being used, the concept of glycaemic variability (see box) is becoming more widely recognised and increasingly important. In diabetic cats with high glucose variability during treatment, insulin analogues such as insulin glargine (100 U/ml or 300 U/ml) or insulin detemir are generally preferred. In humans, the use of insulin analogues has been shown to reduce glycaemic variability more effectively compared with other insulin preparations (eg, neutral protamine Hagedorn [NPH] insulin). 36 Additionally, in some cats, the addition of the extended-release glucagon-like-peptide-1 (GLP-1) analogue exenatide may be helpful in reducing glycaemic variability and improving glycaemic control.37,38 If high glycaemic variability cannot be improved in any way, insulin dose reduction should be considered to avoid the risk of hypoglycaemia.
Diabetic remission
Cats previously diagnosed with DM that cease to receive exogenous insulin therapy and show no evidence of DM after 4 weeks are considered to be in diabetic remission. 2 The reported remission rate is highly variable and ranges from 17% to over 54%,39–41 with these data coming from very different studies, which makes it hard to draw meaningful comparisons. Interestingly, one study showed that 2 months after 30 cats were admitted with newly diagnosed DM and no clinical signs of pancreatitis, the serum Spec fPL concentrations were significantly higher in those that did not achieve remission than those that achieved remission. 18 These findings may suggest that cats with pancreatitis have a reduced chance of achieving diabetic remission; however, further studies are needed to support this hypothesis.

Basic principles of the management of pancreatitis in cats with DM or DKA
Acute pancreatitis and DM
The basic principles of the management of acute pancreatitis, which are described in the box below, are the same whether a cat is, or is not, diabetic. Most cats with concurrent DM and acute pancreatitis have already been diagnosed with the DM and are receiving insulin treatment. These cats are generally anorectic, which can make insulin management challenging and hospitalisation is typically required. The use of long-acting insulins (such as glargine) may be ineffective or may induce hypoglycaemia. It is therefore advisable, especially during the first days of hospitalisation, to switch to regular insulin administered intravenously (as a CRI), using the same protocol as for diabetic ketoacidosis (DKA) (see later). In cats that are newly diagnosed with concurrent acute pancreatitis and DM (ie, at the time of onset of DM), insulin treatment should also start with regular insulin IV until they are stable; the cats can then be switched to long-acting insulin before they are discharged. It should be noted that these newly diagnosed cats can often achieve diabetic remission after resolution of pancreatitis. These cats should be monitored closely to ensure appropriate adjustments of the insulin dose to avoid hypoglycaemia.

Acute pancreatitis and DKA
Cats that present with acute pancreatitis and DKA are a challenge for the clinician and require intensive care management. Figures 3 and 4 illustrate the diagnostic and therapeutic approaches for the management of cats with acute pancreatitis and DKA. 47
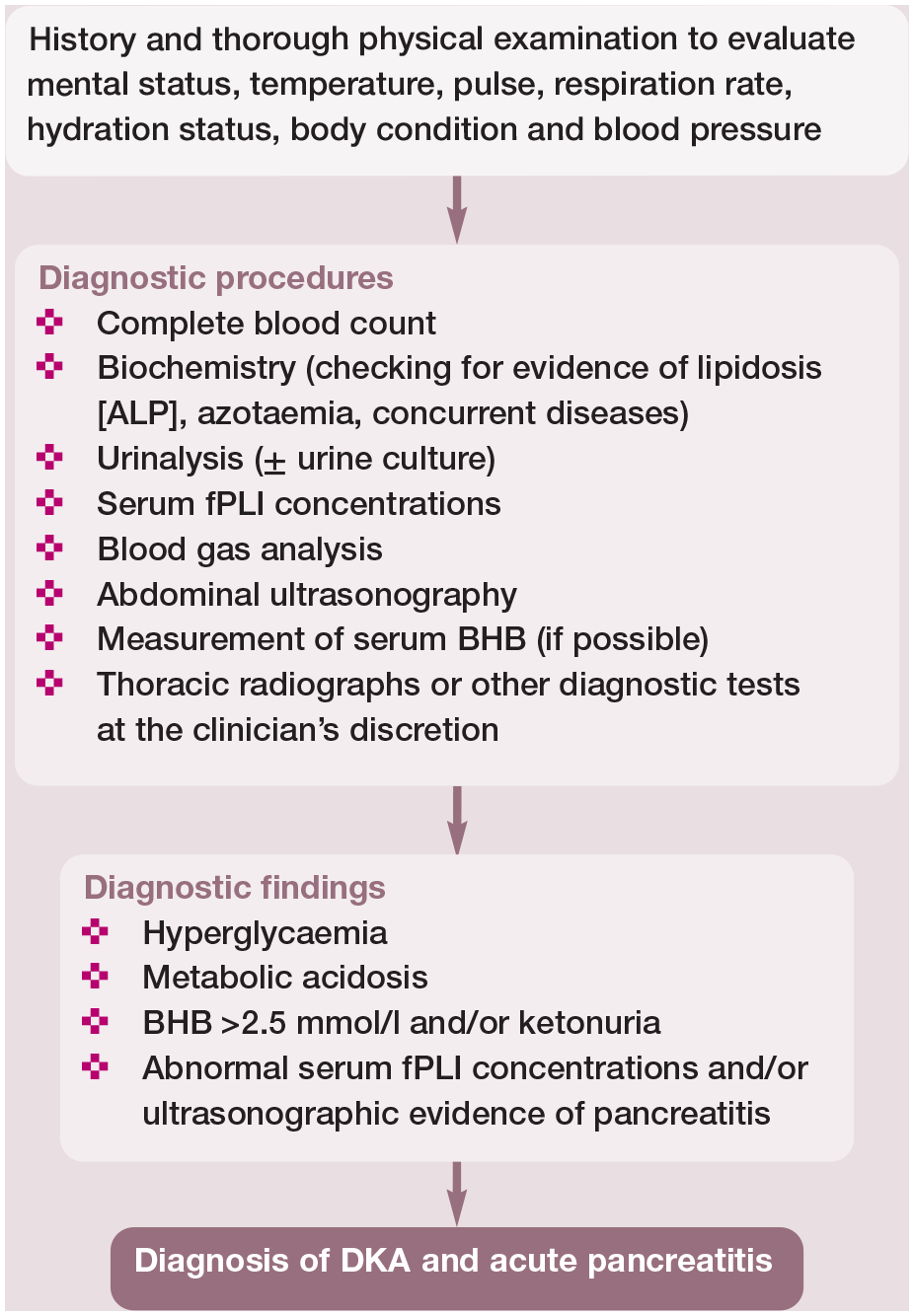
Diagnostic approach to the cat with diabetic ketoacidosis (DKA) and acute pancreatitis.46,47 This diagnostic work-up should be applied to any diabetic cat with acute pancreatitis to confirm, or rule out, DKA. ALP = alkaline phosphatase; BHB = beta-hydroxybutyrate; fPLI = feline pancreatic lipase immunoreactivity

Management of the cat with diabetic ketoacidosis (DKA) and acute pancreatitis. 46 This approach is also used in cats with diabetes mellitus and acute pancreatitis. BHB = beta-hydroxybutyrate; CRI = constant rate infusion; fPLI = feline pancreatic lipase immunoreactivity; IV = intravenous; PZI = protamine zinc insulin
Chronic pancreatitis is usually considered to be mild and can be managed on an outpatient basis in most cases. Many cats with chronic pancreatitis show hyporexia or even anorexia, which might interfere with optimal management of diabetes. These patients may benefit from an antiemetic medication, such as maropitant or ondansetron. Also, an appetite stimulant, such as mirtazapine, may be useful. Finally, an analgesic may be indicated in patients that appear to have abdominal pain.
In most cats with chronic pancreatitis, insulin treatment does not differ substantially from that for cats without pancreatitis, and therefore long-acting insulin preparations are typically used. However, due to the ongoing low-grade inflammation, the release of pro-inflammatory cytokines and periods of reduced appetite, good glycaemic control might be more challenging to achieve. Therefore, more intensive home monitoring and more frequent veterinary visits are typically required.
A proportion of cats with chronic pancreatitis are believed to have an autoimmune basis to their disease, although this has not been proven. In these cases, immunosuppressive treatment (eg, corticosteroids or ciclosporin) may be used if symptomatic treatment is not sufficient at controlling clinical signs. However, the benefits of such an approach remain unproven. Corticosteroids, ciclosporin or chlorambucil are also often used to manage concurrent intestinal and/or hepatic disease in cats with pancreatitis. Glucocorticoids with a high first-pass metabolism (eg, budesonide) could be a good first option, although their effectiveness for the management of pancreatitis (and especially concurrent intestinal or hepatic disease) is questionable. In addition, glucocorticoids should be used with caution because they interfere with insulin sensitivity, and a worsening of diabetic control is likely. If a diabetic cat receives corticosteroids for the management of pancreatitis or other disorders, high doses of insulin are likely to be required. If good diabetic control is difficult or impossible to achieve in these cats, an alternative immunosuppressive drug, such as chlo-rambucil or ciclosporin, should be attempted.
The ideal diet for cats with DM and chronic pancreatitis is unknown. Like for acute pancreatitis, diets formulated for diabetics (eg, high protein, moderate fat, low carbohydrate) should be suitable for most cats with chronic pancreatitis. However, anecdotally, some cats with chronic pancreatitis do not tolerate diets with a relatively high fat content and such a diet might even exacerbate pancreatitis. These cats might benefit from a GI diet with a lower fat content. However, the effect of these diets on diabetic control is not known.
Key Points
✜ DM is one of the most common feline endocrine disorders and frequently coexists with pancreatitis in cats.
✜ Currently, it is assumed that most diabetic cats have type 2-like DM, similar to what is observed in humans. The category ‘other types of diabetes’ is also thought to apply in cats, although it is less clearly defined than in human diabetology.
✜ Pancreatitis is the most common disorder of the exocrine pancreas in cats and, in the majority of cases, is believed to be idiopathic. Chronic and acute pancreatitis in cats are most commonly differentiated by the presence or absence of permanent histopathological lesions, respectively.
✜ The exact pathogenetic association between DM and pancreatitis in cats has not been established. Most likely, the association between diabetes and pancreatitis is bidirectional; therefore, DM likely predisposes cats to pancreatitis and vice versa.
✜ Diagnosis of DM in cats is typically straightforward, whereas clinical diagnosis of pancreatitis is often challenging and requires a combination of findings from the history and clinical presentation, pancreatic markers and imaging studies.
✜ Insulin is the key element in the therapeutic management of feline DM, and cats with concurrent chronic pancreatitis are managed with the same insulin products. For cases of acute pancreatitis, insulin management can be challenging, and long-acting insulins may need to be switched to regular insulin.
✜ The basic principles of management of acute pancreatitis in a diabetic cat are the same as for a non-diabetic cat and treatment is generally supportive. When a cat presents with acute pancreatitis and DKA, more intensive care management is required. Cases of chronic pancreatitis in most cases are mild and managed on an outpatient basis.

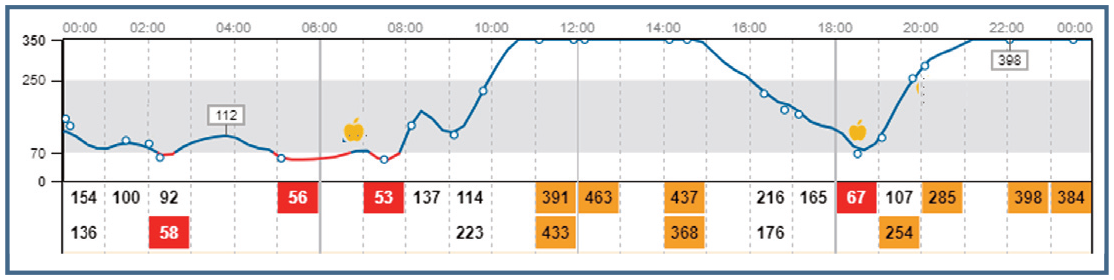
Interstitial glucose (IG) fluctuations over 24 h, measured with a continuous glucose monitoring system (Freestyle Libre), in Mikky. IG concentrations detected by the scans are reported as numbers and are identified by the empty circles; red boxes highlight IG values <70 g/dl (3.9 mmol/l); orange boxes highlight IG values >250 mg/dl (13.9 mmol/l); apples represent meal times. High glycaemic variability is evident from this trace

Abdominal ultrasonography of Mikky’s pancreas, which is diffusely hyperechoic with the presence of a pseudocyst. Courtesy of Alessia Diana

Supplemental Material
sj-pdf-1-jfm-10.1177_1098612X221106355 – Supplemental material for Feline Comorbidities: Clinical perspective on diabetes mellitus and pancreatitis
Supplemental material, sj-pdf-1-jfm-10.1177_1098612X221106355 for Feline Comorbidities: Clinical perspective on diabetes mellitus and pancreatitis by Panagiotis G Xenoulis and Federico Fracassi in Journal of Feline Medicine and Surgery
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.