
Abstract
Practical relevance:
Cats frequently present with diaphyseal fractures, which require treatment in order to achieve a good return to function. These fractures often occur due to significant trauma; for example, as a result of road traffic accidents, high-rise syndrome and dog bite wounds. The first priority is to ensure the patient is systemically well before embarking on any specific surgical treatment of a fracture.
Clinical challenges:
Surgical management of diaphyseal fractures can be challenging due to the surgical approach for some bones being technically demanding, for example because of the presence of important neurovascular structures, and the small size of feline bones, which limits the choice of implant size and strength. Further, it may be difficult to visualise fracture alignment when using minimally invasive techniques, although the use of intraoperative fluoroscopy can aid with this, and malalignment can be common for some fracture repairs, particularly in cases where anatomical reconstruction is not possible.
Aims:
This review focuses on diaphyseal long bone fractures and aims to assist decision-making, with an overview of the management and treatment options available.
Evidence base:
Many textbooks and original articles have been published on aspects of managing fractures in small animals. The authors also provide recommendations based upon their own clinical experience.
Introduction
In the UK, there is an estimated population of 10.7 million cats. 1 With a growing feline population, veterinary practitioners and specialists are increasingly required to treat a variety of fractures involving the humerus, radius and/or ulna, femur and tibia and/or fibula. Diaphyseal fractures are often a consequence of a significant trauma, such as road traffic accidents, 2 dog bite wounds and human abuse, all of which can lead to damage of multiple body systems, including injured limbs and fractured bones. 3 Cats might also sustain a long bone fracture as a result of being stepped on, having something fall on them and falling from a height.
Initial patient assessment and management
As diaphyseal fractures are usually secondary to high-energy trauma, the initial assessment should be focused on rapid evaluation of life-threatening respiratory, circulatory or neurological conditions. A thorough description of the evaluation process and management of polytrauma in cats is beyond the scope of this article (for further information see Voss K 4 and Fletcher DJ, et al 5 ); however, as a brief summary, mental status, respiratory rate and pattern, heart rate, mucous membrane colour, capillary refill time and body temperature should be assessed for evidence of haemodynamic compromise.
Routine blood analysis may be required to safely anaesthetise the patient and to determine the cat’s overall health status. Minimal screening of haematocrit, plasma total solids and blood urea nitrogen will help to rule out subclinical problems such as anaemia or renal disease. In traumatised patients, a more intensive work-up is indicated, however. Further diagnostic procedures should be centred around abnormal findings.
Abdominal pain, bruising, vomiting and urinary tract signs should alert the clinician to the possibility of abdominal injury. once the patient can be handled safely, the abdomen should be thoroughly and gently palpated, with special attention paid to the integrity of the abdominal wall and urinary bladder filling.
Screening thoracic and abdominal imaging (eg, using ultrasonography, as well as radiography if the cat is stable) should be performed in all traumatised cats to detect concurrent pathologies. Thoracic trauma has been reported in 17% of cats that sustain limb fractures in road traffic accidents (Figure 1). 2 Pulmonary contusions are the most prevalent thoracic lesion, and can also occur in combination with other thoracic injuries including pneumothorax, pleural effusion, rib fractures and diaphragmatic rupture.2,3 With pelvic fractures or other significant injuries affecting the caudal half of the body, damage to the urinary tract is common, but this can be easily missed without the use of imaging as clinical signs can be vague and non-specific and may take some time to become apparent. A focused assessment with sonography for trauma (FAST) can be a useful first-line diagnostic screening tool to evaluate the abdomen and thorax. Any free fluid identified should be sampled and analysed. If the creatinine and potassium concentrations of the abdominal fluid are higher than peripheral samples, this indicates the presence of urine in the abdominal cavity. Likewise, if the packed cell volume level in the abdominal fluid exceeds blood levels, this indicates haemorrhage. If the patient is stable, abdominal radiographs should be obtained to help diagnose any urinary tract injuries (specifically urinary bladder rupture), abdominal wall hernias and intra-abdominal bleeding. It should be noted that in patients with a small bladder leak, there is still likely to be some bladder distension, and so it is important to look for the presence of abdominal free fluid.

Left lateral radiograph of a cat with mild pneumothorax following a road traffic accident. The heart base is elevated from the sternum and free gas is present between the caudal lung lobes
Appropriate analgesia should be provided as soon as possible after presentation, with frequency and dosages based on pain scoring. In the event of a long bone fracture, a full mu-opioid agonist such as methadone (0.1-0.4 mg/kg IM or slow IV) is recommended; this can also provide a mild sedative effect, which can assist with emergency imaging. Non-steroidal anti-inflammatory drugs (NSAIDs) can be considered in conjunction with opioids for multimodal analgesia if the patient is stable and the biochemistry is unremarkable.
Diagnosing a diaphyseal fracture
An orthopaedic examination should be performed once the animal is considered stable and can be handled safely. Minimal restraint and pressure should be used when examining the cat. A complete orthopaedic examination consists of careful, systematic palpation of all four limbs and spine, generally examining any known affected limb last. Frequently, palpation alone can isolate the injured area by identifying pain, swelling, effusion or instability. If this is not the case, manipulation can help identify instability in ligaments or fractures.
Radiographic imaging with orthogonal views is essential for precise determination of fracture configuration. Also taking preoperative radiographs of the contralateral limb for comparison is recommended; contralateral limb radiographs can additionally help with presurgical planning, including implant selection, precontouring of the plates and limb alignment. CT may be useful in areas where superimposition of the bones, for example the tarsi, carpi and pelvis, makes it difficult to determine fracture configuration on two-dimensional imaging. 6
Principles of diaphyseal long bone fracture management
Stabilisation is the best form of analgesia; reduction (achieving satisfactory limb alignment and length if the fracture is not anatomically reconstructable) and fixation of the fracture should therefore be undertaken as soon as the cat is considered stable for anaesthesia and surgery. The cat must be haemodynamically and metabolically stable, pulmonary function should not be compromised, packed cell volume and albumin should exceed 20% and 20 g/l, respectively, and haemoglobin should be at least 6 g/dl, otherwise the oxygen delivered to the tissues could be compromised. 7 The ultimate goal of a fracture repair is obtaining early ambulation and complete restoration of limb function.
Many implant types are suitable for fracture repair, and each has its own indications and contraindications. Decision-making should be tailored to the patient based on the following: mechanical factors – biomechanical evaluation of the fracture; biological factors – severity of concurrent soft tissue trauma and the patient’s age and general health; and clinical factors – such as temperament and owner compliance. The surgeon must determine whether the mechanical advantage gained by reconstruction outweighs the biological cost of fragment manipulation. With simple fractures, or those comminuted with reducible fragments, anatomical reconstruction can usually be achieved with a relatively low biological cost. However, in severely comminuted fractures, a more functional biological approach should be considered. 8 Under the latter protocol, care is taken to protect the soft tissues and the blood supply of the fracture fragments. Healing in this case is by the indirect route, with early callus formation responsible for much of the stabilisation.
In general, there are three systems applicable for the stabilisation of diaphyseal fractures – a bone plate and screws, external skeletal fixators (ESFs) and interlocking nails. Supplementary devices, such as intra-medullary (IM) pins, lag screws, pre-loaded neutral screws or cerclage wires, can be used, but only in combination with one or more of the three basic systems.
Plate osteosynthesis can be used in many long bone fractures. A large variety of plates are available, and they differ regarding strength and shape, design of the plate holes and indications (see box).
IM pins are a common method of internal fixation used in combination with other devices. IM pins are placed within the medullary cavity to align and support fractures. They can reduce bending forces, but they cannot prevent compression or rotational forces and, consequently, they should not be used as a sole method of fixation.
Plate-rod stabilisation is a fixation technique in which an IM pin is used in combination with a plate. The IM pin is used as a reduction device to align the main fracture fragments before the plate is applied. The pin protects the repaired fracture against bending forces and reduces the strain on the plate, while the plate resists axial collapse, rotation, shear and bending. Plate-rod constructs may be used to stabilise a variety of fractures, ranging in severity from simple transverse to highly comminuted. Advantages of the plate-rod construct over a bone plate alone include simplifying the fracture reduction, maintaining spatial alignment, reducing plate strain across the fracture gap and increasing the stiffness, load to failure and fatigue life of the construct. 9 In terms of plate strain, this has been reported to reduce by 20% for each 10% increase in pin diameter when using a nonlocking plate-rod construct. 10 Another study suggested that when a locking plate-rod construct is used, an IM pin of at least 30% of the IM diameter is required to provide a significant increase in bending stiffness compared with the LCP alone. 11

In reconstructable fractures, such as two-piece and some three-piece (two main bone segments and one large butterfly fragment) fractures, traditional treatment strategies of anatomical reduction and rigid stability are are often preferable and sometimes necessary. Both the bone and the plate share the load and the aim is to achieve direct bone healing. Bone plates in combination with lag screws and preloaded neutral screws 12 (for intrafragmentary compression) and cerclage wires are often used for these fracture. The authors’ preference is to use screws rather than orthopaedic wire, however, as improper use of the latter is more likely to result in postoperative complications. For example, a loose wire at a fracture site can have a negative impact on healing; as the wire moves, it disturbs the vascular buds attempting to revascularise and heal the fracture, resulting in no blood supply, no healing and non-union.
In non-reconstructable fractures (comminuted fractures), implants are applied in a bridging fashion and should withstand the load (as this will not be initially shared with the bone) until the bone has healed.
Fractures may be open and therefore contaminated or infected at presentation. In these instances, there are further management factors to consider (see the box below).

Diaphyseal fractures of the humerus
Fractures of the humerus account for 5-13% of fractures in cats. 14 Diaphyseal fractures of the humerus are typically caused by road traffic accidents, gunshot wounds and falling from a height.15,16 Injuries to the thorax, such as lung contusions and pneumothorax, can be encountered alongside fractures of the humerus due to the proximity of these locations; careful attention to the thorax is therefore important if humeral fractures are present. Patients with humeral fractures tend to present carrying the affected leg, with the elbow dropped and the paw resting on its dorsal surface because of pain and weakness in the extensor musculature. This presentation mimics that of a loss of proprioception resulting from nerve injury; hence, it is important to assess the sensory function of the radial nerve preoperatively by testing the sensitivity on the dorsum of the paw.


(a,c,e,g) Mediolateral and (b,d,f,h) craniocaudal radiographs (a,b) preoperatively and (c,d) immediately, (e,f) 8 weeks and (g,h) 15 weeks postoperatively, demonstrating a plate-rod repair of a complete closed comminuted mid-diaphyseal humeral fracture. A 2.4 mm Steinmann intramedullary pin was placed in a normograde fashion. The pin was anchored distally, engaging the proximal cortex of the supratrochlear foramen; note that this is not routinely recommended. A 2.4 mm 10-hole reconstruction locking plate has been used with three screws (including a transcondylar screw) both proximally and distally. No attempt has been made to reconstruct the fracture. At the 8-week follow-up (e,f) there was minimal radiographic progression of bone healing. At the 15-week follow-up (g,h) there was radiographic progression of bone healing and the cat’s clinical function had improved with no overt right forelimb lameness
Since the humerus cannot be properly immobilised with casts or splints, surgical fixation, typically with open reduction and internal fixation (ORIF) or external skeletal fixation, should be performed.
Surgical approaches to the humerus are technically demanding because of important neurovascular structures on the lateral and medial aspects of the bone, and the large amount of surrounding musculature. The humeral diaphysis is exposed through either a craniolateral (proximally) to lateral (distally) approach or a medial approach. 16 Indications for the craniolateral approach include proximal and mid-diaphyseal fractures. Indications for the medial approach include mid-diaphyseal fractures and distal fractures with limited distal bone stock and cases where double plating is indicated. Care should be taken to avoid the radial nerve if using a lateral approach to the bone, and the median, ulnar and musculocutaneous nerves if using a medial approach. The radial nerve courses laterally across the middle third of the humerus in a slightly oblique caudal to cranial direction and is located superficial to the brachialis muscle. In the cat, the median nerve and brachial artery pass through the supracondylar foramen, located on the medial surface of the humerus just proximal to the medial epicondyle. Medially, a neurovascular bundle containing the median, musculocutaneous and ulnar nerves, and the brachial artery and vein, is located at the caudal edge of the biceps brachii muscle.
If using a plate, the DCP, LC-DCP, LCP, VCP and reconstruction locking plate are suitable. A plate and rod combination or bilateral plating are generally the authors’ choice of treatment for fractures of the humeral shaft. The plate and rod combination is especially useful for addressing comminuted fractures; however, placing an adequately sized pin in the distal humerus can be challenging. LCPs are therefore useful in this scenario because they allow the placement of monocortical screws if needed. Reconstruction locking plates are also valuable as they can be contoured in three planes, allowing the screw hole to be positioned over the humeral condyle so a transcondylar screw can be placed. They can also function as an LCP and they can also be used with monocortical screws.
Little information is available for minimally invasive plate osteosynthesis (MIPO) of humeral fractures in cats, although a plate-rod combination applied using a medial approach via MIPO for the treatment of extra-articular humeral fractures has been reported in one study. Clinical union of the fractures was observed in the cats 36 ± 2 days postoperatively with no complications and excellent functional outcome. 20 Humeral alignment may be difficult to visualise during MIPO, justifying intraoperative imaging such as fluoroscopy. 21
Use of an ESF in combination with supplementary devices has been reported as an option for comminuted humeral fractures. 22 At least two pins should be used in each main bone fragment if possible. When placing the pins, care must be taken to prevent penetrating or damaging the radial nerve, and the supracondylar foramen should be avoided, as the median nerve and brachial artery course through it. 22

Diaphyseal fractures of the radius and ulna
Radial and ulnar fractures account for 2-14% of long bone fractures in cats. 24 The fractures usually involve the mid-third of the diaphysis and most fractures of the radius are accompanied by fractures of the ulna. 25 The radius of the cat has a torsional shape, with the cranial surface of the radius directed craniolaterally in the proximal part and craniomedially in the distal part; this should be considered when placing a long cranial plate (application to the tension surface), as it needs to be appropriately contoured to the torsional shape.
Cats have a pliable and extensive inter-osseous membrane, which facilitates approximately double the range of pronation (90–128°) and supination (40–50°) 26 compared with dogs. Due to this movement of the paired bones, fixation of the radius or ulna alone has a higher risk of complications as it is less likely to result in stable fixation of the adjacent bone. 24 As well as having implications for fracture repair, axial rotation of the antebrachium is an important normal function in cats; in particular, supination is vital for climbing, capturing prey and self defence. 14 When planning treatment of radial and ulnar fractures, every effort should be made to maintain the movement that occurs between the two bones by adequate fracture reduction, correct implant positioning and choosing the correct length of screws to avoid impinging on the ulna.
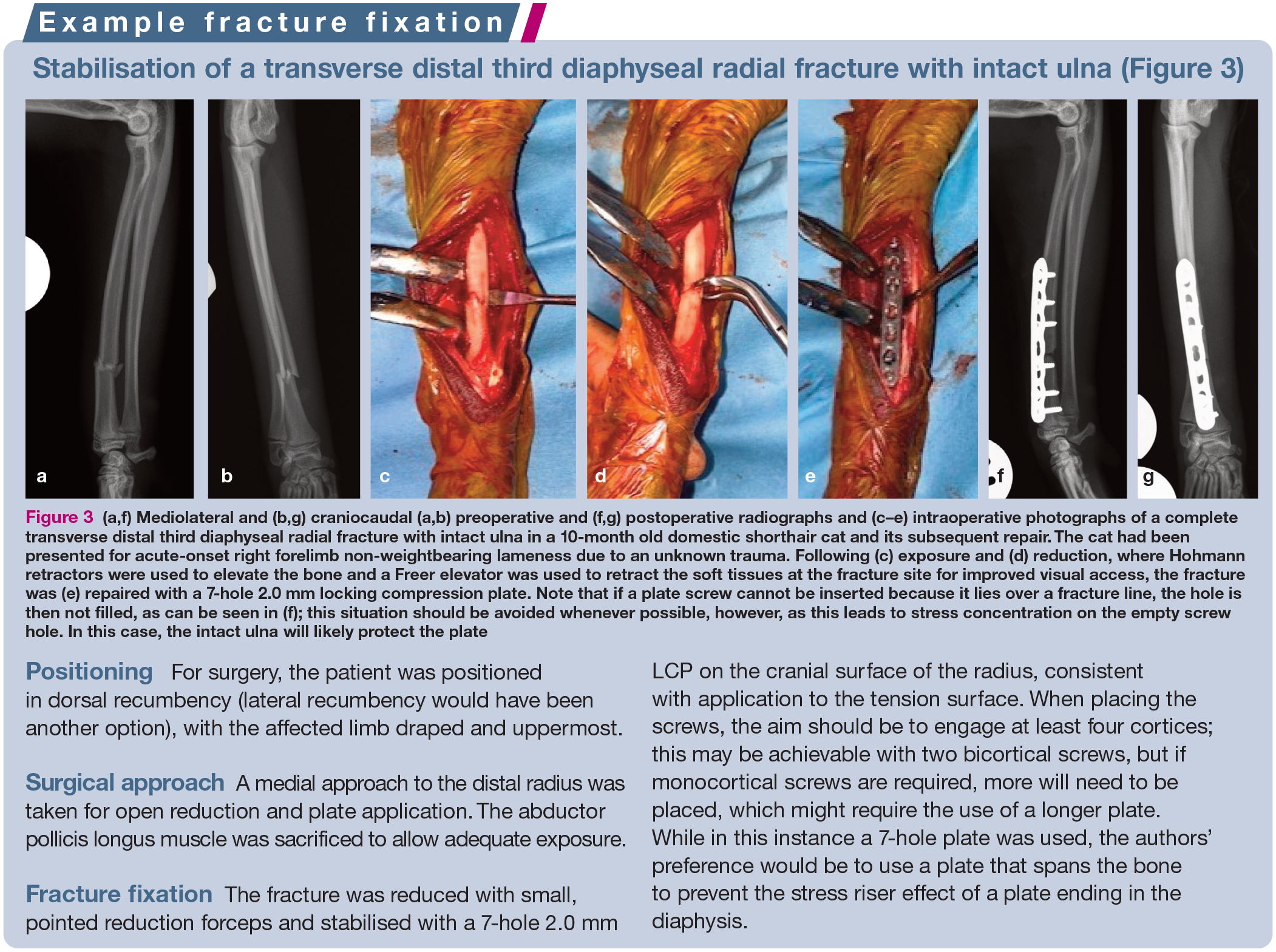

(a,f) Mediolateral and (b,g) craniocaudal (a,b) preoperative and (f,g) postoperative radiographs and (c–e) intraoperative photographs of a complete transverse distal third diaphyseal radial fracture with intact ulna in a 10-month old domestic shorthair cat and its subsequent repair. The cat had been presented for acute-onset right forelimb non-weightbearing lameness due to an unknown trauma. Following (c) exposure and (d) reduction, where Hohmann retractors were used to elevate the bone and a Freer elevator was used to retract the soft tissues at the fracture site for improved visual access, the fracture was (e) repaired with a 7-hole 2.0 mm locking compression plate. Note that if a plate screw cannot be inserted because it lies over a fracture line, the hole is then not filled, as can be seen in (f); this situation should be avoided whenever possible, however, as this leads to stress concentration on the empty screw hole. In this case, the intact ulna will likely protect the plate
Although the diaphysis of the radius is accessible through several approaches, the standard medial approach offers the most direct access to the bone with a minimal amount of muscle dissection. Medial plate application is also possible, and is generally the preference for distal fractures, with potential advantages including the ease of surgical approach and reduced interference with the tendons of the extensor muscles. Radial fractures can also be fixed by MIPO by making small skin incisions remote to the fracture through which the plate is inserted. Anatomical realignment of the radius is hindered by the tendency for the carpal and digital flexor muscles to create caudolateral displacement of the distal bone fragment. 27 DCPs, VCPs and LCPs are typically the plates of choice for radial and ulnar fractures.
Dual bone fixation with, in addition to radial fixation, ulnar fixation, involving placement of either a plate (Figure 4) or an IM pin (Figure 5) to provide additional mechanical support, is, in the authors’ opinion, the surgical treatment of choice.26–28 The application of a plate or ESF to the radius in conjunction with adjunctive stabilisation of the ulna (typically an IM pin) has been shown to be an effective repair method. 25 The use of external skeletal fixation may provide benefits for higher grade open fractures (see ‘open fractures’ box on page 665) as this method of repair can facilitate wound management while stabilising the fracture and provides the advantage of being easily removable, helping to avoid the perpetuation of implant-associated infection. Synostoses and radiohumeral luxation have been reported as complications associated with fractures stabilised by an ESF. 25
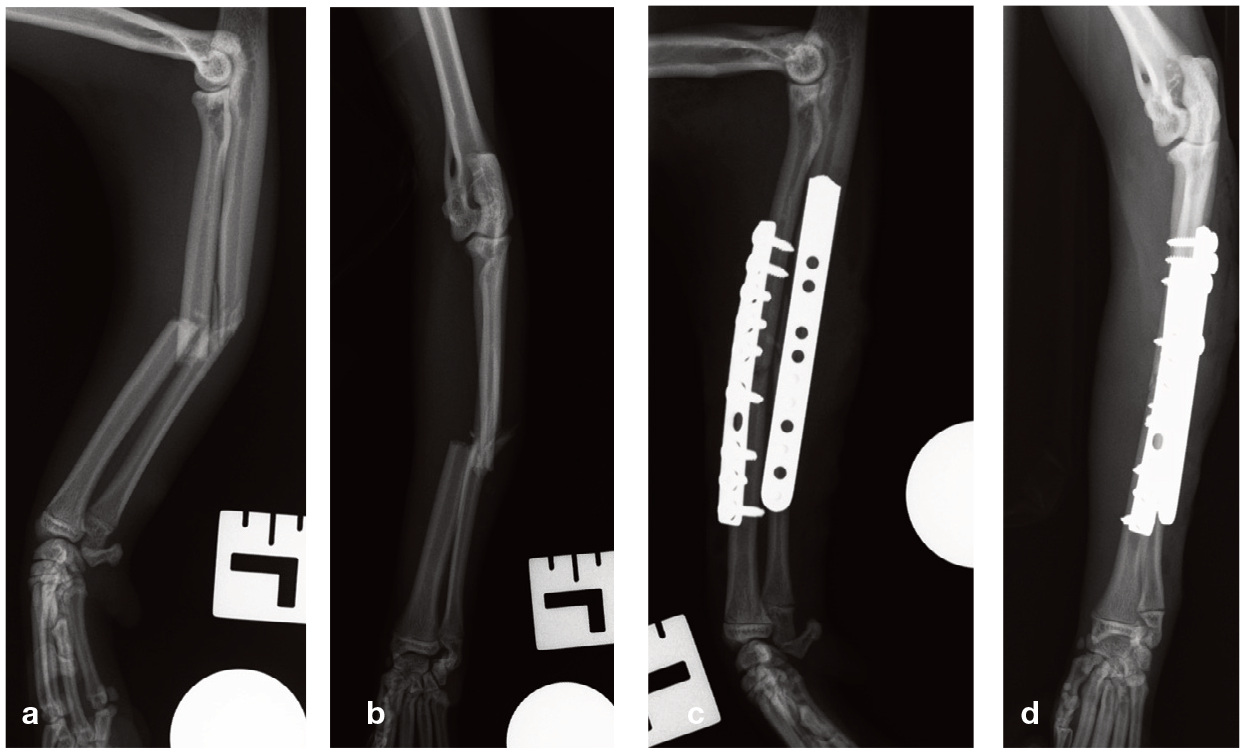
(a,c) Mediolateral and (b,d) craniocaudal (a,b) preoperative and (c,d) postoperative radiographs demonstrating the repair of a mid-diaphyseal fracture of the radius and ulna. (c,d) Both bones have been plated. A 10-hole 2.0 mm dynamic compression plate was used for the radius, with five screws placed proximally and four screws placed distally. The ulna has been stabilised with a 14-hole 1.5/2.0 mm broad veterinary cuttable plate with four 2.0 mm screws placed proximally and four 1.5 mm screws placed distally. The authors recommend using the longest possible plates, especially in non-reconstructable fractures

(a) Mediolateral and (b) craniocaudal postoperative radiographs demonstrating a plate-rod repair of a mid-diaphyseal fracture of the radius and ulna. The authors’ preference is to use a plate that spans the bone to prevent the stress riser effect of a plate ending in the diaphysis. Images courtesy of Philip Witte
The authors avoid external coaptation as it is unlikely to result in satisfactory healing of unstable fractures. In addition, external coaptation for fracture management requires a substantial commitment and careful management by the owner as well as weekly re-examinations by the veterinarian. Underlying skin irritation, bandage sores and ulcers are commonly associated with external coaptation.

Diaphyseal fractures of the femur
Femoral fractures are common in cats, accounting for 20-26% of all fractures. 29 Surgical repair of diaphyseal femoral fractures should not be overly delayed as quadriceps contracture can develop in the presence of muscle contusion or laceration. Diaphyseal femoral fractures always require surgical stabilisation; for example, with ORIF or external skeletal fixation techniques. IM pins and cerclage wires, bone plates and screws, interlocking nails or a combination of these methods can be applied with great success when stabilising femoral diaphyseal fractures. The straight form of the femoral diaphysis in cats makes it especially suitable for plate osteosynthesis combined with IM pinning.

While the pin-plate combination has largely superseded the use of ESFs for femoral fracture stabilisation in cats, ESFs have been used, especially for comminuted femoral fractures. The presence of a large muscle mass around the femoral diaphysis, however, limits the use of external fixator pins to proximal and distal insertion sites, which impedes any ability to increase the stiffness of the construct. Only type I and type II ESFs can be used in the femur because of the proximity of the bone to the abdominal wall. An ESF in the femur can be combined with an IM pin, and a tied-in configuration enhances fixator strength and is therefore a suitable option for comminuted fractures in skeletally immature cats where the intraosseus pins may be at risk of pull-out. Additionally, insertion of an IM pin prior to application of the ESF facilitates spatial alignment of the main fragments without necessitating extensive soft tissue dissection. ESFs have been associated with higher complication rates compared with the plate-rod construct; some of the reported complications include patellar luxation, irritation of the pin-skin interface, especially at the level of the stifle, pin loosening and bone fracture after removal of the implants. 29
When performing the fixation, the femoral diaphysis is visualised through a lateral surgical approach. Care should be taken to preserve the caudal muscle attachments to the femur and bone fragments to preserve the blood supply, especially for intermediate fragments.
Bone plates are usually applied to the lateral surface (tension surface) of the femur. DCPs, VCPs and LCPs are commonly used. DCPs and VCPs can be applied in a bridging fashion for comminuted femoral fractures. In LCPs, the screw heads are the same size in both the 2.7 mm and 2.4 mm plates, and a 2.7 mm plate can therefore be used with a 2.4 mm screw; this can be useful in cats, where the small size of feline bones limits the choice of implant size. In distal diaphyseal fractures, the plate should be contoured accurately to account for the curve from the femoral shaft onto the femoral condyle. If a locking plate and locking screws are used in conjunction with an IM pin (see the next paragraph), placing some mono-cortical screws may help to avoid interference with the pin. A polyaxial (PAX) locking plate is another useful option as it allows polyaxial insertion of screws, meaning they can be angled to avoid joint spaces, anatomical structures and supplementary devices.
Plate-rod constructs can be useful to stabilise a variety of femoral fractures, from simple transverse to highly comminuted. Placement of an IM pin can be performed in a normograde or retrograde fashion for the femur. However, normograde insertion in a proximal-to-distal direction is strongly recommended because it allows for more accurate positioning of the rod within the trochanteric fossa and medullary canal. In addition, this technique reduces manipulation of the fracture site and better preserves the fracture haematoma. In contrast, retrograde insertion is associated with a greater risk of sciatic nerve injury, particularly in cats. To reduce this risk with either method, the femur should be adducted, and if retrograde insertion is used, the hip joint should be held in maximal extension.30,31
Ensuring careful assessment of limb alignment during surgery is critical as rotational malalignment is common, particularly in cases where anatomical reconstruction is not possible. Femoral fractures in cats have a tendency to be stabilised with retroversion of the femoral head and neck, which can lead to a functional gait abnormality and significantly increased risk of patellar luxation. There are different ways to assess alignment intraoperatively; for example, palpating the femoral head position, evaluating the hip range of motion and aligning the linea aspera on the caudolateral aspect of the femoral shaft either side of the fracture. The intertrochanteric crest and femoral trochlea are also used as landmarks of the proximal and distal fragments, respectively. If minimally invasive techniques are used for fracture repair, care must be taken as not all of the landmarks will be visible intraoperatively. The use of intraoperative fluoroscopy may prove beneficial, especially when closed reduction techniques are used.


(a,c) Mediolateral and (b,d) craniocaudal (a,b) preoperative and (c,d) postoperative radiographs showing a comminuted proximal diaphyseal femoral fracture in a 4-year-old domestic shorthair cat, sustained following a road traffic accident, and its subsequent repair. Due to the type of fracture and the limited space for the placement of screws, a plate–rod construct was chosen in order to increase the strength of the repair. A 2.8 Steinmann intramedullary pin was placed in a normograde fashion and a 2.7 mm polyaxial locking plate was applied

Diaphyseal fractures of the tibia and fibula
Tibial factures account for 10-20% of all fractures in cats.14,36 The majority of tibial fractures are of the mid- to distal diaphysis. 32 These fractures are often caused by falling from a height but can occur after any type of trauma. 37 Usually, both the tibia and fibula are fractured. The fibula is very thin in cats and does not contribute to weightbearing, but it is important for stifle and tarsal joint stability as it serves as an attachment site for the lateral collateral ligaments for both joints.
Distal tibial fractures can be challenging to repair because of limited distal bone stock and minimal soft tissue coverage. Additionally, feline distal tibial fractures are often open (see the ‘open fractures’ box on page 665) and therefore contaminated or infected at presentation.37,38
When compared with fractures of other bones, tibial fractures have been reported to have a higher rate of complications such as delayed union, non-union and osteomyelitis. 38 Multiple factors have been proposed to result in delayed union and non-union, including inadequate blood supply from the limited extraosseous soft tissues, an insufficiently stable fixation, an excessive fracture gap and interposition of soft tissue in the fracture gap.39,40 From this perspective, biological osteosynthesis, despite providing less stable fixation, may therefore be appropriate in tibial diaphyseal fractures as it emphasises the preservation of the soft tissue surrounding the fracture site.
Many different stabilisation methods have been described for feline tibial fractures, including ORIF with a plate either used alone or combined with an IM device, orthogonal plate fixation via an MIPO approach, and type I and II standard ESFs (Figure 7) or circular-linear hybrid ESFs. While ESFs can have higher complication rates than using ORIF methods, they can be beneficial for comminuted open fractures as the fracture segments can be immobilised without invading or placing metallic fixation devices in the contaminated open area.
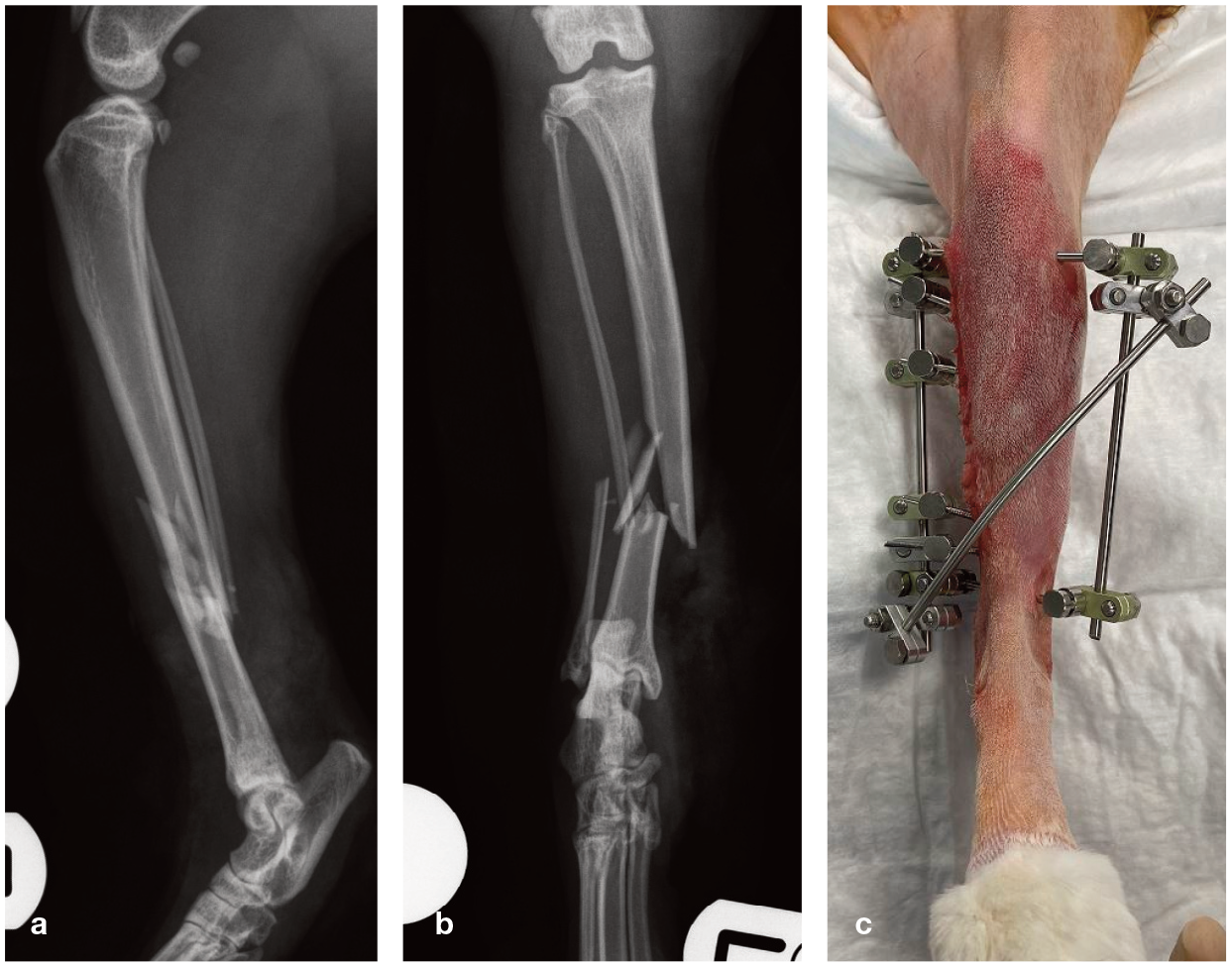
(a) Mediolateral and (b) craniocaudal preoperative radiographs showing type II open comminuted mid-diaphyseal fractures of the tibia and fibula, which were sustained after unknown trauma in a 3-year old male domestic shorthair cat. The injury occurred 48 h prior to referral. Given the degree of contamination, the soft tissue damage and the level of comminution, an external skeletal fixator (ESF) was considered the fixation method of choice. (c) Postoperative photograph showing the repair. A modified type II ESF was applied with three (2.4/2.0 mm) positive-threaded pins in both the proximal and distal bone fragments
Although the straight form of the tibia is ideal for inserting IM pins, these are not placed in the tibia as commonly as in the humerus and femur. IM pins should always be combined with a plate or an ESF and they should be inserted in a normograde fashion into the tibia as retrograde placement in cats can result in impingement of the pin on the patellar tendon. 41


(a,e) Mediolateral and (b,f) craniocaudal (a,b) preoperative and (e,f) postoperative radiographs and (c,d) intraoperative photographs of a type I open transverse left tibial distal diaphyseal fracture, as well as a transverse fracture of the fibula, in a 6-month-old domestic shorthair cat, and its subsequent repair. The injuries were sustained following an unknown trauma. The patient underwent surgery within 24 h of the injury. As the fracture was reconstructable, and the contamination and soft tissue damage were minimal, internal fixation as if the fracture was closed was pursued, but with profuse lavage before and during surgery. Orthogonal tibial plating was considered the fixation of choice and a cranial 2.0 mm veterinary cuttable plate (VCP) and a medial 2.0 mm locking compression plate were applied. When using two plates, it is preferable to end the plates at different positions in order to avoid the stress riser effect. Note that in this case, the cranial VCP was cut short for stiffness modulation
Plates – typically 2.0 mm or 2.4 mm LCPs, 2.0 mm LC-DCPs or 2.0/2.7 mm VCPs – can be used for most fractures of the tibial shaft and have the advantage of easier postoperative management compared with ESFs. Plates are usually placed on the medial or craniomedial surfaces of the bone. The plate will need to be used in a bridging fashion for comminuted tibial fractures. A previous study reported a series of feline tibial fracture repairs in which the plates applied (either as a single medial plate or a plate-rod construct) to stabilise tibial fractures bent, causing tibial valgus deformation. 42 In the study, the implant failure occurred in oblique or spiral fractures with mild comminution located in the middle or distal third of the tibia. 42 Attention to plate selection and application should be made to avoid stress overload of the plate. In addition, malalignment or instability of the repair will cause dysfunction or degenerative joint disease of the tibiotarsal joint. Orthogonal plating of the tibia provides greater construct stiffness during mediolateral bending and a higher failure load in axial compression when compared with single plating and plate-rod constructs.32,42

Postoperative care
Initially, the patient should be confined, ideally to a single room with non-slip flooring or, alternatively, in a crate to restrict activity. If using a crate, short periods of walking outside of it may be permitted under supervision; however, jumping and play should be avoided.
Following a fracture repair, early controlled weightbearing is encouraged. Physiotherapy is important for the treatment of human fracture patients but it is used and documented far less in feline patients, presumably due to the misconception that they will not cooperate with therapeutic exercises. Although veterinary studies are lacking, it is likely that physiotherapy may be useful in some cases. Techniques such as massage can reduce swelling, and passive range-of-motion exercises may help to minimise joint stiffness. The judicious use of analgesics throughout the recovery period can help to allow more comfortable limb use. NSAIDs and additional analgesics such as gabapentin (5–10 mg/kg PO q8–12h) and oral transmucosal buprenor-phine (0.02mg/kg q8h) are recommended to decrease pain and inflammation and encourage limb use (for further information, please consult the 2022 ISFM Consensus Guidelines on the Management of Acute Pain in Cats 43 ).
Control radiographs are normally taken 6–8 weeks postoperatively in adult cats and 4 weeks postoperatively in skeletally immature cats. Most closed, uncomplicated fractures of the diaphysis of immature animals reach clinical union within 3–5 weeks, whereas mature animals reach clinical union in 6–10 weeks. 33 Follow-up radiographs should be taken during these time frames to ensure healing before the animal is gradually returned to normal activity.33,34
Key Points
✜ Diaphyseal fractures are usually secondary to high-energy traun and therefore the initial assessment should be focused on rapid evaluation of life-threatening respiratory, circulatory or neurological conditions before embarking on any specific treatment of a fracture.
✜ Orthogonal views are essential for precise determination of fracture configuration. Preoperative radiographs of the contralateral limb can help with pre-surgical planning.
✜ The surgeon’s strategy when treating diaphyseal fractures should be not to compromise the fracture biologically unless the intervention will contribute biomechanically.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and / or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/ or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed con- sent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.