
Abstract
Objectives
The aims of this study were to describe the type, presentation and prognostic factors of feline humeral fractures over a 10-year period and to compare three stabilisation systems for feline humeral diaphyseal fractures.
Methods
In total, 101 cats with humeral fractures presenting to seven UK referral centres between 2009 and 2020 were reviewed. Data collected included signalment, weight at the time of surgery, fracture aetiology, preoperative presentation, fixation method, surgical details, perioperative management and follow-up examinations. Of these cases, 57 cats with humeral diaphyseal fractures stabilised using three different fixation methods were compared, with outcome parameters including the time to radiographic healing, time to function and complication rate.
Results
The majority of the fractures were diaphyseal (71%), with only 10% condylar. Of the known causes of fracture, road traffic accidents (RTAs) were the most common. Neutered males were over-represented in having a fracture caused by an RTA (P = 0.001) and diaphyseal fractures were significantly more likely to result from an RTA (P = 0.01). Body weight had a positive correlation (r = 0.398) with time to radiographic healing and time to acceptable function (r = 0.315), and was significant (P = 0.014 and P = 0.037, respectively). Of the 57 humeral diaphyseal fractures; 16 (28%) were stabilised using a plate–rod construct, 31 (54%) using external skeletal fixation and 10 (18%) using bone plating and screws only. Open diaphyseal fractures were associated with more minor complications (P = 0.048). There was a significant difference between fixation groups in terms of overall complication rate between groups (P = 0.012). There was no significant difference between fixation groups in time to radiographic union (P = 0.145) or time to acceptable function (P = 0.306).
Conclusions and relevance
All three fixation systems were successful in healing a wide variety of humeral diaphyseal fractures. There was a significantly higher overall complication rate with external skeletal fixators compared with bone plating; however, the clinical impact of these is likely low.
Keywords
Introduction
Feline humeral fractures are relatively uncommonly encountered in veterinary practice, accounting for between 4.4% and 9.5% of feline fractures.1–4 Of these fractures, between 75% and 87% are diaphyseal;4–6 this is in contrast to dogs, which have a higher proportion of humeral condylar fractures.4,5 This difference is due to the relatively straight profile of the humeral shaft, the wider and straighter humeral condyles, and lack of supratrochlear foramen in the cat,5–7 and the well-documented prevalence of canine breed predisposition to structural weakness in the condylar area.8–11 Interestingly, a recent study identified 18 cats with suspected patellar fracture and dental anomaly syndrome 12 that presented with humeral condylar fractures, six of which were bilateral and two demonstrated a humeral intercondylar fissure on the contralateral limb. This report suggested that there is likely an at-risk population of cats with a similar structural weakness to that identified in dogs.
Several reports have documented outcomes for various treatment methods for small numbers of feline humeral fractures, but no studies to date have compared the outcomes of different treatment options solely or exclusively in cats. Longley et al 13 compared fixation methods in distal and supracondylar humeral fractures in a population of 12 cats and 25 dogs, which showed significantly higher rates of overall complications following use of external skeletal fixation (ESF) compared with plate and screw fixation but no with difference in final or long-term follow-up being reported in dogs and cats.
Intramedullary (IM) pinning with or without cerclage wire has been documented in feline humeral fracture repair in two small case series14,15 of 14 transverse or oblique fractures and one comminuted fracture. The average time to weight bearing was 25 14 and 3–5 15 days postoperatively, with no pin migration, bone shortening or fragment collapse radiographically evident in one study, 14 and normal, complete fracture healing documented between 4 and 12 weeks in the other. 15
The use of an interlocking nail (ILN) for feline humeral fracture repair was reported in one cat 16 with a closed, grade V mid-diaphyseal humeral fracture that achieved radiographic union at 12 weeks postoperatively and was weightbearing with no lameness at 4 and 11 months after ILN placement. Another case series reported on five feline humeral fractures (a total of 121 diaphyseal fractures in dogs and cats) in which an ILN was used. 17 Of these cases, 95% healed with good (favouring limb after exercise) or excellent (total absence of lameness) functional outcome and with 94% radiologically healed by 16 weeks. There was no mention of complications involving the feline humeral cases.
Bone plating (BP) has been documented as a fixation method for diaphyseal humeral fractures in dogs 18 and approaches are described for cats. 19 BP has also been reported in five cats with Y-T humeral fractures with supracondylar comminution. 20 Three of five cases had a satisfactory outcome, with one being severely lame and the other requiring amputation due to implant failure. Plate–rod constructs (PRCs) have also been reported in humeral fracture fixation of cats. One study reported on minimally invasive plate osteosynthesis for PRC fixation in two cats with non-articular humeral fractures, 21 with clinical union achieved at 36 ± 2 days with no complications and excellent functional outcome.
ESF was used to stabilise a variety of feline diaphyseal humeral fractures in a study of 13 cats. 22 Eleven of 13 cats achieved union, with mean time to ESF removal in mildly comminuted fractures being 5 weeks and 4 days, and 10 weeks and 3 days in severely comminuted fractures. Linear–circular ESF has also been used for feline humeral fracture repair in two case series of four cats.23,24 Seven of eight cats in these studies had supracondylar or intracondylar humeral fractures. Seven of eight cats had excellent functional outcome; complication requiring revision surgery was only reported in one case. 24
Therefore, the aims of this study were to detail the types of humeral fractures seen in cats at referral centres across the UK, and to compare the results of humeral diaphyseal fracture fixation based on radiographic and clinical findings, as well as report on the complications encountered with the different fixation methods. We hypothesised that fracture stabilisation with PRCs would result in a similar time to radiographic and clinical resolution as ESF stabilisation but have lower complication rates.
Materials and methods
Criteria of inclusion
Clinical records and radiographs of all cats presenting with humeral fractures to seven different referral centres around the UK between 2009 and 2020 were reviewed. Information collated included sex and neuter status, age and weight at the time of surgery, fracture aetiology, details of preoperative presentation, surgical fixation methods used, details of surgery, perioperative management and details of follow-up examinations.
Fractures were classified according to the level of comminution using a modified version of the Winquist Hansen system.16,25 Complications were classified as minor (that required no medical or surgical treatment to correct), major (surgical or medical treatment required for resolution) or catastrophic (permanent and unacceptable function of the limb, resulting in amputation). 26 With regard to surgical fixation methods, for inclusion in the study, we required a full medical history with details of a humeral diaphyseal fracture repair using either ESF, PRCs or BP, information regarding the fixation method used and at least one follow-up examination with radiographs. When comparing the time taken to achieve radiographic union between the different fixation methods, cases that did not have radiographic union documented on follow-up radiographs were excluded.
Surgical procedure
All surgeries were performed by board-certified surgeons or by residents in training under direct supervision of a board-certified surgeon. A craniolateral, lateral, craniomedial or minimally invasive approach was made for diaphyseal fractures dependent on surgeon preference, fixation system used and location of the fracture. For ESFs, either a type Ia, Ib, type II modified or I/II hybrid ESF was applied. An IM pin (1.6–2.4 mm) was used in all but one case and tied into the construct in two-thirds of cases. For ESF pins, primarily positive profile-end threaded half pins were used in the proximal areas of the humerus with a centrally threaded transcondylar pin being used when appropriate. All pins were placed according to established safe corridors of insertion 27 and connected to the fixation bar with clamps.
Open reduction or minimally invasive approaches were used for plate fixation on the lateral, craniolateral, craniomedial or medial aspect of the humerus. Veterinary cuttable plate (2.0–2.7 mm; Depuy Synthes), locking compression plate (2 or 2.4 mm; B Braun Vetcare), dynamic compression plates (2.4 or 2.7 mm; Depuy Synthes) or string of pearls (Orthomed) plates (2 mm) were used, with bicortical screws being used where possible.
Postoperative management
All owners were instructed to either crate or room rest their cats for a period of 4–8 weeks. Fractures were recorded as healed based on the surgeon’s case report referring to the radiographs. A delayed union was defined as fracture healing being evident but slower than the expected rate, but progressing to full union. 28
Information was collected based on the reported findings from clinical examination by the veterinarian relating to complications, assessment of lameness and grade of function (unacceptable function, acceptable function or full function) 26 of the operated limb from the case files. Postoperative re-checks were performed 4–8 weeks following the first recheck if necessary; recheck times were not standardised and at the surgeon’s discretion. Time to function was defined as the first entry of acceptable or full function of the operated limb in the records.
Statistical analysis
Statistical analysis was performed using IBM SPSS Version 26.0. Surgical fixation methods were compared to ordinal variables using the Kruskal–Wallis test; when independent variables included only two groups, a Mann–Whitney U-test was used to assess against ordinal variables. Independent-scale variables were compared to ordinal variables or non-normally distributed scale variable using a Spearman rank correlation test. When two scale variables of normal distribution were compared, a simple linear regression test was used and when an ordinal independent variable was compared to a normally distributed dependent variable a one-way ANOVA was used. A P value of <0.05 was considered to be statistically significant.
Ethical approval
Ethical approval for this study was granted by the Animal Welfare and Ethical Review Body (AWERB) on 22 September 2021 with a veterinary investigation number for reference of VIN/20/029.
Results
A total of 101 feline humeral fractures were identified. The male to female ratio was 2:1 and a total of 11 breeds were represented, with 78% of the cases being domestic shorthair cats. Median age at presentation was 12 months (range 2–178) and mean body weight was 3.9 kg (range 800 g to 7 kg). Aetiology of the fracture was reported as being unknown in 47% (n = 47/101) of cases. Road traffic accidents (RTAs) were documented as the aetiology in 26% (n = 26/101) of cats. A summary of the fracture morphological characteristics and aetiologies are presented in Tables 1, 2 and 3.
Proportion of cases in each sex and neuter status group that were confirmed to be caused by an road traffic accident (RTA)

Data are n (%)
MN = male neutered; ME = male entire; FN = female neutered; FE = feline entire; NR = not reported
Fracture characteristics and variation between cats in our study

Data are n (%)
Distribution of fracture positions between cases confirmed to be caused by a road traffic accident (RTA) or not and a summary of the aetiologies for each fracture position

Of the 57 humeral diaphyseal fractures reviewed, 16 (28%) were stabilised using a PRC, 31 (54%) using ESF and 10 (18%) using BP. There was no significant difference between treatment groups in terms of age, weight, fracture grade or whether a fracture was open or closed.
All cats underwent general anaesthesia for surgery supervised by a veterinary anaesthetist; local analgesic nerve blocks were performed at their discretion. A summary of perioperative and postoperative management can be found in Tables 4 and 5.
Details of intraoperative antibiotics and postoperative antibiotic administration in each diaphyseal fracture stabilisation group (where available, the doses and frequency of administration are included)

IV = intravenous; PRC = plate–rod construct; SC = subcutaneously; BP = bone plating; ESF = external skeletal fixation
Number of patients discharged with oral analgesia
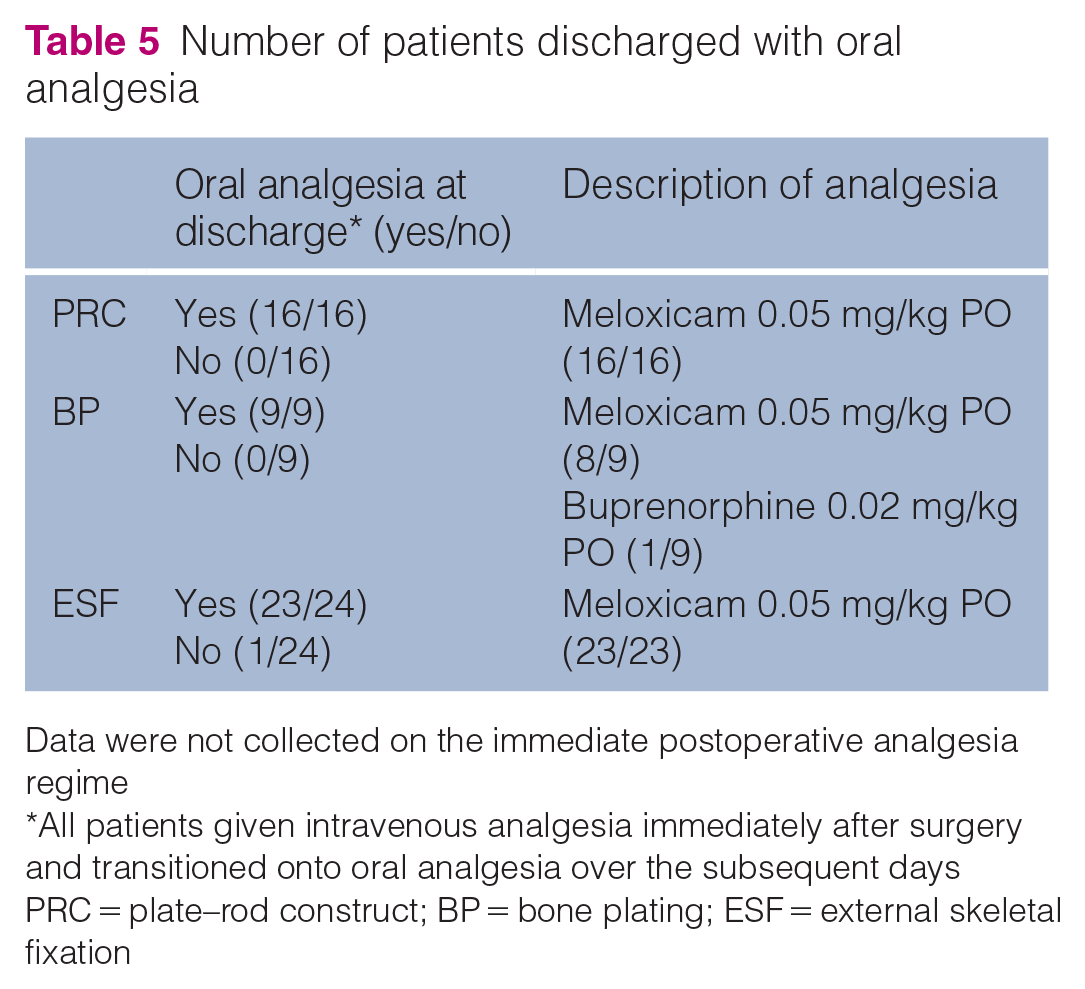
Data were not collected on the immediate postoperative analgesia regime
All patients given intravenous analgesia immediately after surgery and transitioned onto oral analgesia over the subsequent days
PRC = plate–rod construct; BP = bone plating; ESF = external skeletal fixation
Open fractures represented 18% (9/49) of fixation cases, with the remaining 82% (40/49) being closed. Median time to healing in the BP group was 53 days (range 28–98), and it was 56 days (range 28–154) in the PRC group and 70 days (range 21–448) in the ESF group (Figure 1). Median time to function in the BP group was 42 days (range 28–77), and it was 53 days (range 28–70) in the PRC group and 49 days (range 21–182) in the ESF group. A total of 3/57 (5%) fractures did not have documented union and had delayed healing reported on their radiographs. All three of these occurred in the PRC group, giving an 81% (13/16) documented healing rate vs 100% (31/31 and 10/10, respectively) achieving union in the ESF and BP groups. A summary of the cases that did not have documented radiographic union can be found in Table 6. The overall complication rates were 10% (1/10), 50% (8/16) and 65% (20/31) in the BP, PRC and ESF groups, respectively. Details of the complications can be found in Table 7.
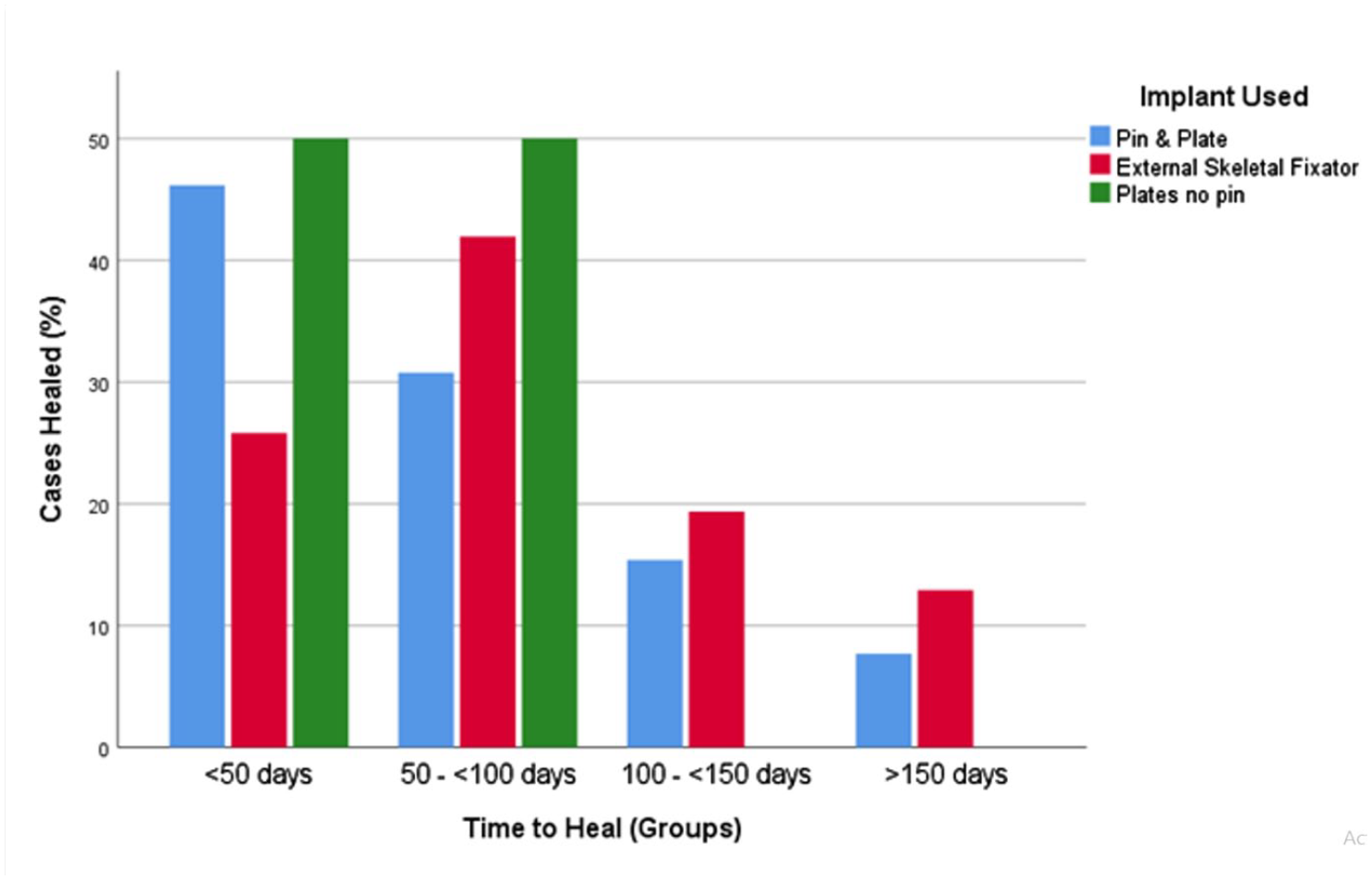
Time taken for the cases within each diaphyseal fracture treatment group to radiographically heal. The x-axis is divided into 50-day increments and the percentage of cases healed from each group within this time are displayed. Fractures that did not have documented union are not included in this figure
Descriptions of the three cases in the plate–rod construct group that did not have documented radiographic union after fracture repair and the reported radiographic findings from their first recheck after surgery

FN = female neutered; DSH = domestic shorthair; FE = female entire; MN = male neutered
Complications encountered in each diaphyseal fracture treatment group, divided into catastrophic, major or minor, with a description of the complications encountered

BP = bone plating; PRC = plate–rod construct; IM = intramedullary; ESF = external skeletal fixation; ROM = range of motion
There was a significant difference between the sexes and whether the fracture was caused by an RTA or not (P = 0.001), with neutered males being over-represented in the RTA group. There was also a significant difference between fracture position and aetiology of the fracture (P = 0.01), with significantly more diaphyseal fractures being caused by RTAs. The aetiology of the fracture had no significant effect on fracture grade (P = 0.160) but did have a significant effect on whether a fracture was open or closed (P < 0.001).
The age of the cat had no significant correlation to time to radiographic union (P = 0.1) or complication rate (P = 0.371) when comparing the fracture stabilisation method used. However, increasing body weight had a positive correlation (r = 0.398) with time to radiographic healing and time to acceptable function (r = 0.315), which was significant (P = 0.014 and P = 0.037, respectively) but had no association with complication rate (P = 0.6).
Fracture grade had no statistically significant effect on the time to healing (P = 0.641), time to function (P = 0.427) or the overall complication rate (P = 0.592).
Whether a fracture was open or closed had no significant effect on the time taken to heal (P = 0.155), time to acceptable function (P = 0.195) or overall complication rate (P = 0.104). However, open fractures had significantly more minor complications than closed fractures (P = 0.048).
There was no significant difference in time to radiographic union between the fixation groups (P = 0.196); however, the difference in documented time to heal was significant (P = 0.019). The rate of complications was significantly different when comparing the method of repair (P = 0.012); however, implant selection had no significant effect on catastrophic (P = 0.322), major (P = 0.181) or minor (P = 0.113) complications.
Discussion
Diaphyseal humeral fractures were the most common fracture types in our population of cats, representing 71% of the fractures vs 27–39%4,5 previously reported for dogs. Condylar fractures were relatively uncommon, representing only 10% of fractures vs 40–73%4,5 reported in canine studies. This study demonstrated that ESF, PRC and BP were all successful methods of stabilisation for a wide variety of humeral diaphyseal fractures. Although ESF was the only device used for the most severely comminuted fractures (grade V), there was no significant difference in fracture grade, open/closed fractures or fracture orientation between implant groups. Our findings suggest that there is no advantage when selecting a particular fixation system for a type of humeral fracture so the surgeon should choose the system they think is most appropriate for the fracture according to their preference and experience.
The most common aetiology for humeral fracture encountered in this population was an RTA. However, this figure is very likely an underestimate as the cause of trauma was not clearly identified in nearly half of the cats. In many of these, an RTA can be presumed. Male cats were significantly more likely to be involved in RTAs than female cats, which has also been found as a risk factor in previous studies29–31 and is suspected to be related to the differing roaming or behavioural habits of male cats, although evidence for this is conflicting.31–34 Other risk factors for RTAs,30,31 such as age and breed, were not found to have a significant association with RTAs in this study.
There was a significant association between diaphyseal fractures and RTAs. This may be due to cats most often being hit perpendicular to the long axis of the humerus and the shaft experiencing supraphysiological bending and shear forces upon it. Although RTAs are considered to be high-impact traumas, there was no association between the level of comminution and whether the fracture was caused by an RTA or not.
There were no significant differences in healing time between implant groups. Variability between recheck was an anticipated limitation of our retrospective data collection, and significance may have been found with more standardised recheck times. All cases that did not have documented union were in the PRC group. It is likely that the cases did in fact achieve union but the time that this occurred could not be documented as they did not return for further rechecks. The positive correlation of body weight with time to healing was also documented in feline femoral fractures, 35 and it was hypothesised that heavier cats have a prolonged healing time, which could be due to the higher forces imparted on the bones following fracture fixation. Larger implants are generally used in heavier cats, however, which should negate this increased force. Further research is required into this, and body condition score should also be recorded in future studies.
Open fractures were not common and were significantly more likely to be caused by gunshot wounds than other traumas; all of the fractures caused by gunshots were open. A previous study not only found RTAs and other high-velocity traumas to be risk factors for open fractures in cats, but also that the humerus is one of the lowest-risk bones for open fractures in the appendicular skeleton. 36 Minor complications were significantly higher in cats with open fractures compared with those with closed fractures. Most of the minor complications found in our study involved infection or delayed healing, which could be associated with the open nature of the original injury. 37 The retrospective nature of this study limited the detail to which open fractures were described. A more comprehensive classification system such as the Gustilo-Anderson Open Fracture Classification Scheme,37,38 or the new scheme proposed by the Orthopaedic Trauma Association, 39 could be used in future studies to allow more accurate analysis of open fractures and their effect on the complication rate and clinical outcome.
There was a significant difference between fixation methods in the overall complication rate. The majority of the complications associated with the ESF group were pin tract infections. It is important to note that minor pin tract infections are almost inevitable with ESF due to soft tissue impalement and motion of soft tissue around the pin.6,40 A previous study showed pin tract infections in feline humeral ESF to be exclusively superficial, rather than deep infections, and manageable. 41 An alternative method for future prospective studies could include the use of implant–skin interface scoring system for ESF. 42
The findings of this humeral fracture study are similar to those found in a previous study comparing feline femoral diaphyseal fracture stabilisation. 35 There were no significant differences in time to radiographic union between the BP, ESF and PRC groups when they were used to stabilise feline femoral diaphyseal fractures and ESF also had the highest number of minor complications in feline femoral fractures. PRCs had the least complications in feline femoral diaphyseal fracture fixation, whereas BP showed the lowest complication rate in this study. PRCs were used in more than half of the cases in the femoral fracture fixation study but only a quarter of the humeral fracture cases. The lack of medullary canal distal to the epicondylar ridge in many cat humeri has been shown to make IM pin placement more challenging in this bone, 27 which may have contributed to the comparatively higher complication rate seen in PRC humeral fracture repair.
This was a multicentre study and so had the inevitable limitations associated with that including different surgeons, protocols and variable follow-up times. Owing to the relatively low incidence of feline humeral fractures seen each year in referral practice, it would take a long time to perform a prospective single-centre study comparing outcomes from feline humeral fracture fixation. There were differing numbers of cases for each fixation group, and having similar numbers for each stabilisation system would have been optimal for data analysis.
Conclusions
Diaphyseal fractures were the most common humeral fracture type seen in cats. PRCs, BP and ESF were all applied successfully for the stabilisation of such fractures. ESF was associated with a higher number of complications; however, the majority of these complications were manageable and had no bearing on overall outcome.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animals described in this work for all procedures undertaken. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.