
Abstract
Objectives
The aim of this pilot study was to compare the quality of sedation and ease of intravenous (IV) catheter placement following sedation using two intramuscular (IM) sedation protocols in cats: hydromorphone, alfaxalone and midazolam vs hydromorphone and alfaxalone.
Methods
This was a prospective, randomized and blinded study. Cats were randomly assigned to receive an IM injection of hydromorphone (0.1 mg/kg), alfaxalone (1.5 mg/kg) and midazolam (0.2 mg/kg; HAM group), or hydromorphone (0.1 mg/kg) and alfaxalone (1.5 mg/kg; HA group). Sedation scoring (0–9, where 9 indicated maximum sedation) was performed at 0, 5, 10, 15 and 20 mins from the time of injection. At 20 mins, an IV catheter placement score (0–10, where 10 indicated least resistance) was performed.
Results
Twenty-one client-owned adult cats were included in this study. Sedation and IV catheter placement scores were compared between groups using Wilcoxon rank sum tests. Peak sedation was significantly higher (P = 0.002) in the HAM group (median 9; range 7–9) than in the HA group (median 7; range 3–9), and IV catheter placement scores were significantly higher (P = 0.001) in the HAM group (median 9.5; range 7–10) compared with the HA group (median 7; range 4–9). Spearman correlations were calculated between IV catheter placement score and sedation scores. There was a significant positive correlation of average sedation over time (correlation 0.83; P <0.001) and sedation at 20 mins (correlation 0.76; P <0.001) with a higher, more favorable IV catheter placement score.
Conclusions and relevance
These preliminary results suggest that the addition of midazolam to IM alfaxalone and hydromorphone produced more profound sedation and greater ease of IV catheter placement than IM alfaxalone and hydromorphone alone.
Introduction
Alfaxalone is a versatile central nervous system depressant with widespread use in veterinary medicine. It is a neuroactive steroid molecule used for sedation and induction of anesthesia that acts at the gamma-aminobutyric acid (GABA) receptor(s). It can be used with or without other hypnotic or analgesic agents, via various routes of administration and in multiple species, including cats.1,2
In addition to sedation, alfaxalone has been associated with dose-dependent cardiovascular changes when administered to cats. These include decreases and increases in heart rate and decreases in blood pressure, respiratory rate and arterial partial pressure of oxygen, as well as changes in several echocardiographic measurements.3–5 Additionally, some animals demonstrate undesirable behavioral effects such as ataxia, muscle tremors, paddling, opisthotonos, twitching and face rubbing when receiving alfaxalone, particularly during recovery.4,6–8
Alfaxalone has been combined in cats with other drugs to provide additional sedation.9–12 Some of these sedative drugs, such as alpha-2 agonists, have been associated with adverse effects on cardiovascular function. 13 The combination of alfaxalone with an opioid is clinically appealing, as it may provide greater sedation, as well as analgesia. However, the sedation from this combination may be insufficient, depending on the dose of alfaxalone and procedure being performed. 9
The benzodiazepine class of sedatives has minimal effect on the cardiovascular system. 13 Unfortunately, benzodiazepines are unpredictable as sedatives in cats.14,15 Studies investigating the use of benzodiazepines for sedation in cats have demonstrated that while some cats are sedated following their administration, many others become restless and more reactive to restraint than prior to drug administration. 14 Further, the use of benzodiazepines in cats can lead to undesirable behaviors such as vocalization, biting, clawing and more. 15 Consequently, benzodiazepines, when used alone, are not an ideal option to provide intramuscular (IM) sedation in cats.
Despite their negative qualities when used as sole agents, the combination of alfaxalone and a benzodiazepine may attenuate the effects of each other and produce superior sedation. Studies in other species, including pigs, dogs and goats, have provided evidence in support of this phenomenon, and a recent study in cats demonstrated that when administered intravenously (IV), midazolam reduces the required induction dose of alfaxalone.16–20 Multiple studies have evaluated the sedative effects of alfaxalone combined with an opioid in cats, but a review of the literature did not reveal any studies evaluating the effect on sedation of the addition of a benzodiazepine to alfaxalone and an opioid IM in cats.9–12,21
The aim of this pilot study was to determine whether an IM injection of alfaxalone combined with hydromorphone and midazolam provided superior sedation in cats than IM injection with alfaxalone and hydromorphone alone. We also evaluated whether the addition of midazolam to hydromorphone and alfaxalone would ease placement of an IV catheter. Our hypothesis was that cats which received hydromorphone, alfaxalone and midazolam would be more sedated and exhibit less resistance to IV catheter placement than those which received only hydromorphone and alfaxalone.
Materials and methods
Ethical approval and informed consent
This was an investigator-blinded, prospective and randomized pilot study. The study was reviewed and approved by the Clinical Studies Review Committee at the Cummings School of Veterinary Medicine at Tufts University (CSRC 009.18). Written or verbal informed owner consent was obtained for each study participant.
Animals
All cats presenting to the anesthesia service at the Cummings School of Veterinary Medicine at Tufts University from February 2019 to February 2020 were considered for enrollment. Cats were eligible for the study if they were undergoing a procedure that required sedation with a pure mu opioid agonist at the discretion of the attending anesthesiologist based on anticipated pain/discomfort, were classified under the American Society of Anesthesiologists (ASA) physical status of I–III, were 1–9 years old and required IV catheter placement. Cats were excluded if they were considered extremely fractious where IM premedication would be difficult, or if they had any contraindications to receiving hydromorphone, midazolam or alfaxalone, as deemed by the attending anesthesiologist. Once enrolled, the cats were randomly assigned to be administered hydromorphone and alfaxalone (HA group), or hydromorphone, alfaxalone and midazolam (HAM group) using a computer-generated randomized list (http://emerald.tufts.edu/~gdallal/assign.htm). Demographic information, including breed, sex, age, weight, body condition score (BCS: 0–9) and ASA status, was recorded. All cats were evaluated to determine their baseline behavior score (Table 1) after enrollment by approaching the cats in the cage and observing their response to this interaction.
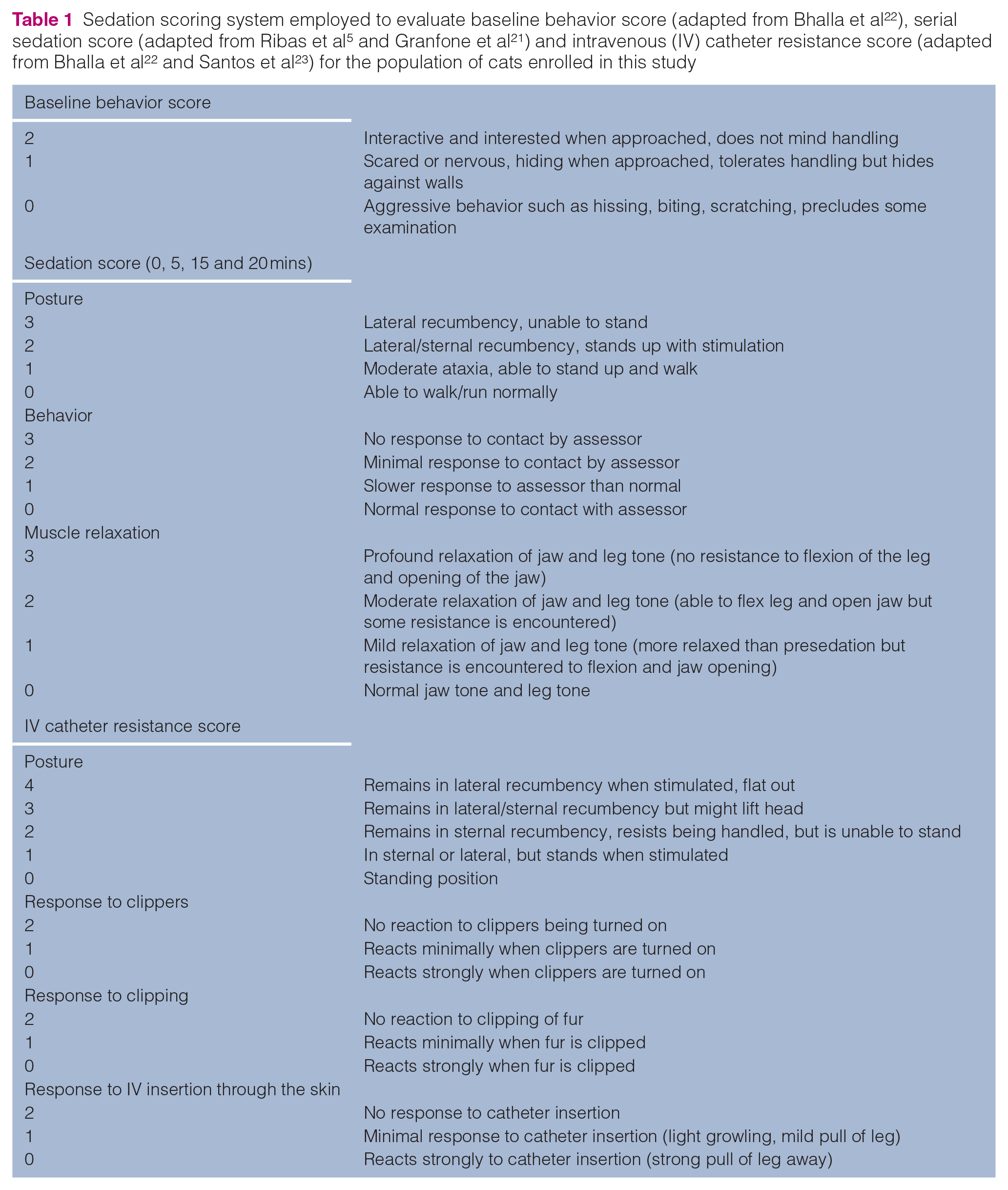
Sedation scoring system employed to evaluate baseline behavior score (adapted from Bhalla et al 22 ), serial sedation score (adapted from Ribas et al 5 and Granfone et al 21 ) and intravenous (IV) catheter resistance score (adapted from Bhalla et al 22 and Santos et al 23 ) for the population of cats enrolled in this study
Scoring system
A single observer, experienced in sedation and anesthesia of veterinary species, who was unaware of group assignment, performed all scores on all cats. The baseline behavior score was on a scale of 0–2; a score of 0 indicated a cat that was interactive and interested; a score of 1 indicated a cat that was nervous and hiding but tolerating handling; and a score of 2 indicated a cat that showed aggressive behaviors. This was a simple descriptive scale previously described in a sedation study in cats. 22 Sedation scoring consisted of three components (posture, behavior and muscle relaxation), each assessed on a four-point scale (0–3), which were summed to produce a total sedation score (range 0–9). Higher scores indicated a greater degree of sedation. The scoring system was previously used in studies evaluating sedation in cats.5,21 The IV catheter placement score similarly consisted of multiple components (posture, response to clippers, response to clipping and response to IV insertion through the skin) that were summed to produce a total score. A higher score indicated less resistance to IV catheter placement. This scoring system was modified from a scoring system previously described to assess resistance of sedated cats to IV catheter placement.22,23 In this study, the previously described subcategory of ‘response to restraint’ was removed as this was considered to overlap with an evaluation of posture, and the category of ‘response to IV insertion through the skin’ was added as this was identified as a point at which animals might uniquely show resistance. See Table 1 for the full scoring system. Additionally, at each time point, cats were evaluated for demonstration of adverse events, including hypersalivation or vomiting.
Study protocol
Baseline sedation was scored at 0 mins. Cats were administered either hydromorphone (0.1 mg/kg) and alfaxalone (1.5 mg/kg) for the HA group, or hydromorphone (0.1 mg/kg), alfaxalone (1.5 mg/kg) and midazolam (0.2 mg/kg) for the HAM group. Drugs were combined into a single syringe and administered into the epaxial muscles. Following injection, cats were placed in a cage, in a quiet room. Sedation scores were performed at 5, 10, 15 and 20 mins. After the final sedation score, cats had an IV catheter placed in the cephalic vein by a veterinary technician or veterinary student, while the single-blinded observer scored level of resistance to IV catheter placement. For IV catheter placement, cats were restrained in such a way as to maintain control of the head and extend the limb in which the IV catheter was to be placed. The IV catheter was inserted into the skin immediately after clipping the area and applying alcohol, and it was secured in place with surgical tape followed by a self-adhering bandage wrap. If rescue sedation was required to facilitate IV catheter placement, this was recorded. After IV catheter placement, cats completed participation in the study.
Statistics
Categorical variables were summarized using n (%) and groups compared using Fisher’s exact test. Continuous variables were summarized using median (interquartile range [IQR]) and groups compared cross-sectionally using Wilcoxon rank sum tests.
For each component of the sedation score (posture, behavior and muscle relaxation; each with a range of 0–3) and total sedation score (range 0–9), median (IQR) scores were graphed by time point and group. Peak sedation was determined by group for each component, as well as total sedation as the highest number across time points for each component and the sum of all of the components respectively. Generalized estimating equations (GEEs) accounting for repeated measures were fit for each sedation outcome as a continuous measure at post-baseline time points to estimate mean differences between groups across the four time points (no interactions between group and time were statistically significant). GEEs were also fit for posture, behavior and muscle relaxation using a multinomial distribution, to estimate the odds of lower sedation in group HA vs HAM. Spearman correlations were calculated between IV catheter score and sedation score at 20 mins, as well as average sedation levels from 5 to 20 mins. Statistical significance was set at a P value ⩽0.05.
Results
Demographics
Twenty-one cats were included in the study; 11 were randomized to the HA group and 10 to the HAM group. Baseline characteristics by group are shown in Table 2. In the HA group, two cats (18%) were considered overweight (BCS >5), while in the HAM group, seven (70%) were considered overweight. The remaining cats were considered normal weight (BCS 4–5). Across groups, ASA status ranged from I to III, and baseline behavior score ranged from 0 to 2.
Baseline characteristics and behavior identified for cats that received hydromorphone (0.1 mg/kg) and alfaxalone (1.5 mg/kg) with (HAM) or without (HA) midazolam (0.2 mg/kg) for sedation

Data are n (%) unless otherwise indicated
DSH = domestic shorthair; DLH = domestic longhair; DMH = domestic mediumhair; IQR = interquartile range; BCS = body condition score; ASA = American Society of Anesthesiologists
Sedation scores
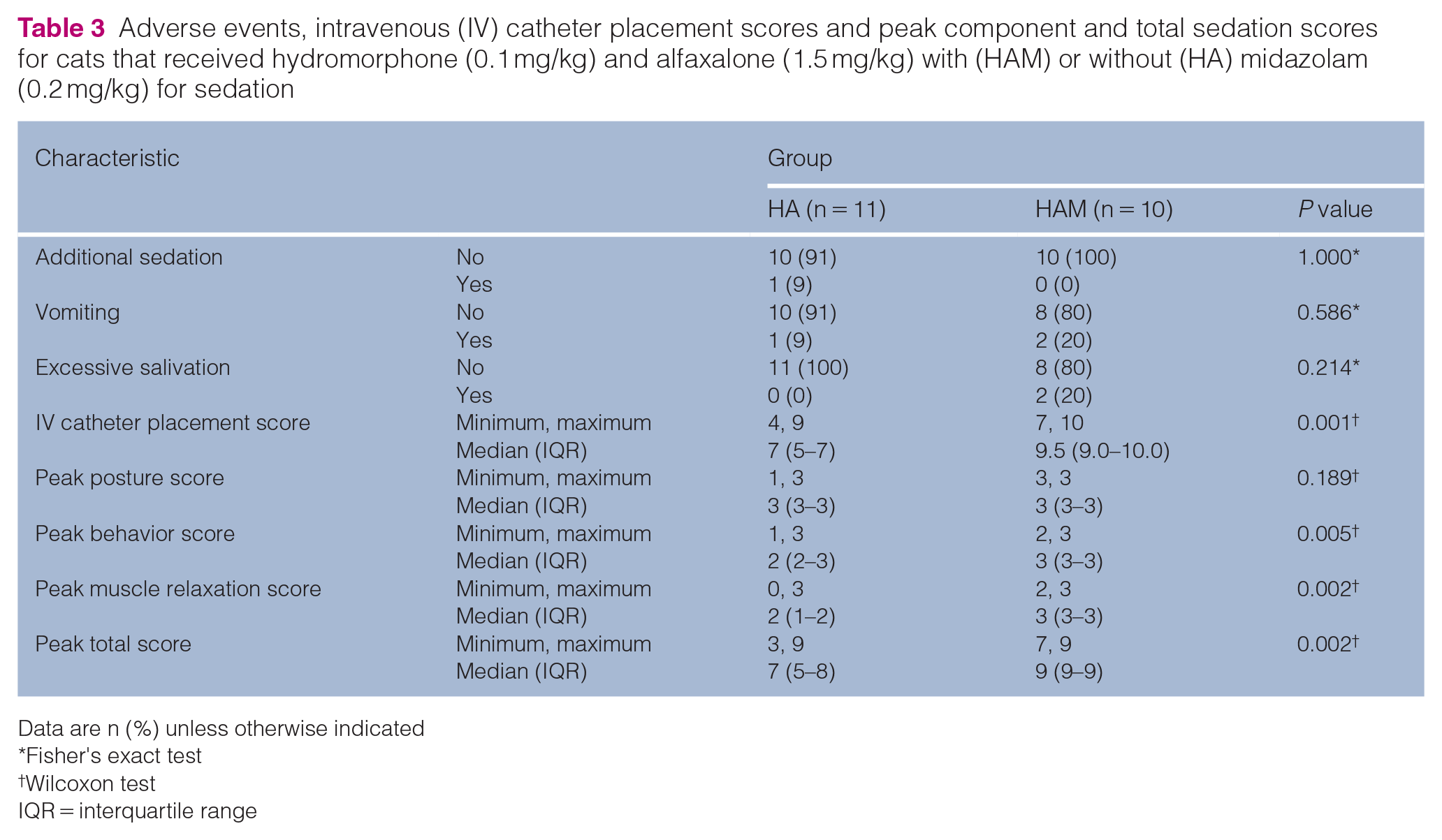
Peak total sedation (P = 0.002), behavior (P = 0.005) and muscle relaxation (P = 0.002) scores were significantly higher in the HAM group compared with the HA group (Table 3).
Adverse events, intravenous (IV) catheter placement scores and peak component and total sedation scores for cats that received hydromorphone (0.1 mg/kg) and alfaxalone (1.5 mg/kg) with (HAM) or without (HA) midazolam (0.2 mg/kg) for sedation
Data are n (%) unless otherwise indicated
Fisher's exact test
Wilcoxon test
IQR = interquartile range
There was no statistically significant difference (P = 0.19) in peak posture score between the HA and HAM groups.
Median total sedation, posture, behavior and muscle relaxation scores by time point are shown in Figure 1.

Median (interquartile range) sedation scores over times 0 to 20 mins for behavior, muscle relaxation, posture and total scores for cats that received hydromorphone (0.1 mg/kg) and alfaxalone (1.5 mg/kg) with (HAM; n = 10) or without (HA; n = 11) midazolam (0.2 mg/kg) for sedation. Higher scores indicate a greater level of sedation
Across the four post-baseline time points, cats in the HAM group had significantly higher mean total sedation (P <0.001), posture (P = 0.014), behavior (P <0.001) and muscle relaxation (P <0.001) scores than cats in the HA group (Table 4). The HA group was significantly more likely to have a less sedate posture (P = 0.007), behavior (P <0.001) and muscle relaxation (P <0.001) score than the HAM group (Table 4).
Average difference in sedation scores and odds of a better sedation response for cats that received hydromorphone (0.1 mg/kg) and alfaxalone (1.5 mg/kg) with (HAM) or without (HA) midazolam (0.2 mg/kg) for sedation

CI = confidence interval
IV catheter resistance score
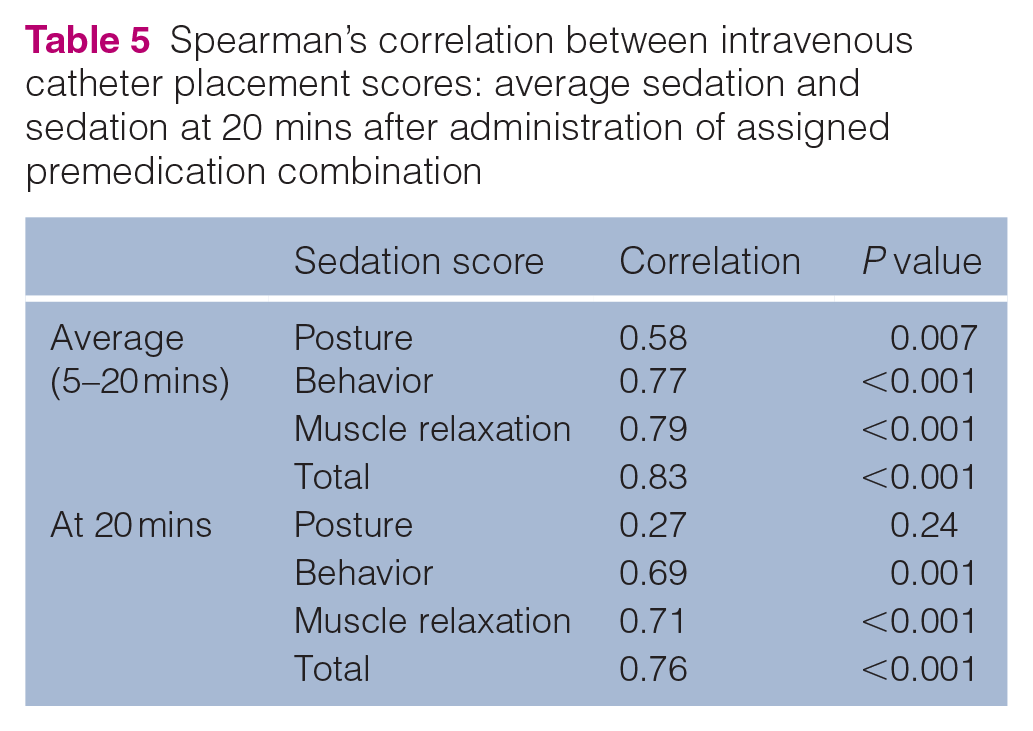
IV catheter placement scores were significantly higher (P = 0.001) in the HAM group than in the HA group (Table 3). There was a positive association between higher IV catheter scores with both higher average total sedation and all individual sedation components, as well as higher total sedation, behavior and muscle relaxation at 20 mins when IV catheter placement was attempted (Table 5). One cat in the HA group required rescue sedation with 1.8 µg/kg IV dexmedetomidine to place an IV catheter.
Spearman’s correlation between intravenous catheter placement scores: average sedation and sedation at 20 mins after administration of assigned premedication combination
Discussion
This pilot study demonstrated that an IM injection of alfaxalone combined with hydromorphone and midazolam provided superior sedation in cats than an IM injection of alfaxalone and hydromorphone alone. The deeper sedation was likely clinically relevant, as cats in the HAM group demonstrated significantly less resistance to IV catheter placement.
The successful use of midazolam in conjunction with hydromorphone and alfaxalone IM is appealing because it allowed for improved sedation with the addition of a drug that is described in the literature to cause only minimal cardiovascular alterations as an alternative to increasing the dose of alfaxalone. 13 Previous studies investigating the use of alfaxalone in cats demonstrate that cardiovascular and behavioral effects are dose-dependent. For example, in one study, cats that received a dose of alfaxalone of 1 mg/kg IM did not demonstrate changes in body temperature, heart rate, respiratory rate, mean arterial blood pressure or adverse recovery behaviors, whereas cats receiving higher doses were subject to some change in these variables. In that same study, the authors concluded that an alfaxalone dose of 1 mg/kg IM was too low to allow for reliable sedation in healthy cats. 4 It could be argued that a dose reduction of alfaxalone is unnecessary, since even in studies where altered cardiovascular variables were reported, the changes were minimal.3–5 However, these studies were most often conducted in healthy cats, and ill cats may be more sensitive to changes in cardiovascular status.
The combination of alfaxalone, hydromorphone and midazolam may also be advantageous because midazolam has some additional desirable properties such as muscle relaxation, anxiolysis and anticonvulsant effects. 13 The property of muscle relaxation could potentially counteract some of the negative effects reported for alfaxalone, such as tremors, paddling, twitching and so on. Although the incidence of these adverse behaviors was not specifically recorded in this study, muscle relaxation scores were significantly higher in the HAM group than in the HA group, suggesting that this theoretical benefit holds true in cats, especially as this has been demonstrated in other species. 16
An unexpected observation from this study was that sedation appeared to persist for longer in the HAM group than in the HA group. Figure 1 shows that over time, median behavior scores decreased in the HA group while they remained stable in the HAM group. The addition of midazolam to alfaxalone and an opioid could be beneficial, if prolonged sedation is desired. Additionally, it may allow for more control over duration of sedation since midazolam can be antagonized by administering flumazenil; however, this was not specifically investigated in this study.
Although it is beyond the scope of this study to determine the mechanism of action of the observed increased alfaxalone induced sedation with the addition of midazolam, it may be of note that both of these drugs act at the GABA receptor. Alfaxalone, acts at a unique binding site on the GABA receptor to increase chloride conduction into the cell, leading to hyperpolarization of the postsynaptic membrane and, ultimately, inhibition of pathways that are responsible for arousal and awareness. At higher concentrations, alfaxalone will additionally act at the GABA binding site as a GABA agonist. 2 Benzodiazepines work at the receptor by increasing the affinity of the receptor for GABA. 13 Synergistic effects that lead to intensified central nervous system depression can occur between benzodiazepines and other drugs (ie, barbiturates, ethanol, etomidate and propofol) when they both have activity at the GABA receptor. 13 Therefore, this might be the case with alfaxalone as well.
There were some limitations to this study. The number of cats was too small to perform adjusted analyses, and some baseline characteristics were not balanced across groups. More cats were overweight in the HAM group, and their level of sedation may have been affected by overall higher drug doses for lean body weight. However, in animals with more adipose tissue, it is possible that less drug was successfully administered IM, which would be expected to have the opposite effect on sedation. More cats in the HA group had a higher ASA status, which might actually strengthen the conclusions in this study, as more systemically compromised cats would be expected to be more easily sedated, though the HA cats had lower sedation scores. Finally, more cats in the HAM group demonstrated ‘aggressive behavior’ at baseline, while a greater number of cats in the HA group acted ‘scared or nervous’ or ‘interactive and interested’. It is possible that there could have been an interaction between these baseline behavior and sedation scores that was not detected as a result of limited sample size. A larger sample size that would allow for adjusted analysis may be indicated in future studies to determine how any difference in baseline characteristics between groups may have affected the findings in this pilot study. It would be prudent in future studies to utilize these pilot data to perform a sample size calculation to ensure a sufficient number of cats for such analyses. Another limitation of this study was that, although inclusion criteria were broad, animals presenting to a teaching hospital often represent a more compromised population of animals with underlying cardiovascular or other systemic disease, so our findings may not be generalizable to a larger population. Also, the drug combination was only evaluated in cats that were 1–9 years old, so caution should be taken in extrapolating these findings to pediatric or geriatric animals. Although the sedation and IV catheter resistance scorings were all performed by a single observer, IV catheter placement was not always performed by the same individual or by an individual of the same level of training. Additionally, the method of assessment of the cats in this study was not a validated scale, though, to our knowledge, a validated scale for sedation and IV catheter placement in cats does not exist at this time. As previously mentioned, peak sedation levels did not necessarily occur at 20 mins in all cats, but for this study design, that was when resistance to IV catheter placement was evaluated. Therefore, cats that had higher sedation scores earlier but that did not persist until 20 mins, might have had improved IV catheter resistance scores if evaluated at a different time period. However, despite that observation, there was still a significant positive correlation between average sedation and sedation at 20 mins and IV catheter resistance score. Finally, as this was a pilot study, there was not a power analysis or sample size calculation performed prior. Although statistical analysis did yield significant results with the number of study subjects, subsequent studies would benefit from application of this data to calculate the number of study subjects needed while not unnecessarily enrolling excess animals. Also, prior to this study, what magnitude of difference on this sedation scale was clinically relevant was not defined. The data from this study could be utilized to define what is considered to be clinically desired sedation for power calculation prior to subsequent studies.
The findings of this pilot study lead to several questions that warrant further investigation. Since only one dose of alfaxalone was used, it would be of interest to evaluate whether adequate sedation can be achieved when combining midazolam and hydromorphone with an even lower dose of alfaxalone. Additionally, it would be beneficial to evaluate whether lowering the dose of alfaxalone leads to minimized cardiovascular effects. This knowledge may be particularly beneficial in terms of sedation for higher risk sedation candidates.
Conclusions
The findings of this pilot study support our hypothesis that the addition of midazolam to IM alfaxalone and hydromorphone in cats leads to an increased level of sedation, and that the increased sedation allows for easier IV catheter placement. Further research is warranted to further elucidate the potential benefit of this sedative combination.
Footnotes
Acknowledgements
The authors would like to thank clinicians at the Cummings School of Veterinary Medicine at Tufts University for their help in patient recruitment. The authors would also like to thank the veterinary students and veterinary technicians who facilitated patient participation in this study.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (owned or unowned) and procedures that differed from established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient. The study therefore had ethical approval from an established committee as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.