
Abstract
Objectives
The aim of this study was to describe the outcomes and determine the reluxation rate of cats undergoing closed coxofemoral joint reduction, and to investigate potential risk factors for reluxation of the affected coxofemoral joint.
Methods
Case information was obtained from electronic medical records from Ocean State Veterinary Specialists and Bay State Veterinary Emergency and Specialty Services between January 2008 and May 2020. Data obtained from 51 cats with coxofemoral joint luxations included patient signalment, direction of coxofemoral joint luxation, concurrent injuries, ease of reduction, time of injury to closed reduction, bandage application and outcome. Data were analyzed for association with outcomes.
Results
Closed reduction of coxofemoral joint luxation in cats had a 51% success rate. The only risk factor demonstrating a statistically significant benefit to the success of closed coxofemoral joint reduction was the application of a bandage (P = 0.02).
Conclusions and relevance
It may be worth attempting closed coxofemoral joint reduction in cats prior to recommending surgery. Placing a bandage (Ehmer or hobbles) after closed reduction may decrease the risk of the coxofemoral joint reluxating, but more studies are needed to evaluate this further. The outcome after closed reduction management for coxofemoral joint luxation in cats is similar to the previously reported success rate in dogs.
Introduction
Coxofemoral joint luxations have been shown to account for up to 90% of all luxations in cats and dogs.1,2 Closed reduction is frequently the first choice of treatment as it allows the patient to maintain their original anatomy and is the least invasive treatment.
A 1984 study demonstrated that closed coxofemoral joint reductions were successful in the long term in approximately 47.3% of dogs. 1 A subsequent study in 1986 showed a reluxation rate of 64.8% in dogs and cats, but only four of the 71 cases were cats. 2 Two of those four cats were available for long-term follow-up. One cat’s coxofemoral joint remained in place (follow-up 3 months) and the other cat’s coxofemoral joint reluxated. 2 No study evaluating the outcomes of closed coxofemoral joint reductions in cats alone was found in a search of the literature.
Multiple surgical procedures have been reported to correct coxofemoral joint luxation in cats, including transarticular pinning and open coxofemoral joint reduction and stabilization. The coxofemoral joint can also be removed with a femoral head and neck excision or replaced with a total hip replacement. However, surgery does come with costs and potential risks of morbidity, including longer anesthesia times and surgical site or implant infections.
Open coxofemoral joint reduction can be performed in cats in which closed coxofemoral joint reduction fails. A 2012 study looked at toggle rod stabilization of coxofemoral joint luxation and reported an 86% success rate, with only 2/14 cats reluxating the affected coxofemoral joint. 3 In another study, open reduction with transarticular pinning was successful in 77% of cats. 4
Micro-total hip replacements can also be performed in cats. One study included eight cats, which all had excellent outcomes, with the majority of the animals in the study followed up to at least 1 year after surgery. 5 Femoral head and neck ostectomies have also been shown to have good-to-excellent long-term clinical outcomes, 6 with complete or near complete return to function by 1–2 months postoperatively.6,7
Conservative management has also been reported in cats where the coxofemoral joint is unable to be closed reduced and surgery is not pursued. A pseudoarthrosis can form between the femoral head and the ilium allowing for a limited range of motion without discomfort. 8 A retrospective study was able to examine and radiograph 13 cats that had untreated hip luxations (mean length of follow-up 28 months). All cats had functional use of the affected limb and a normal level of activity according to the owners. 9
The purpose of this study was to determine the reluxation rate of feline coxofemoral joints after undergoing closed reduction. Potential factors that may influence the success of closed coxofemoral joint reduction were also investigated. The results may help determine if closed coxofemoral joint reduction is a reasonable first choice in cats with coxofemoral joint luxations, prior to pursuing a surgical treatment.
It was hypothesized that closed coxofemoral joint reduction in cats would be successful in the majority of cases, similar to the reported success rate for dogs. Successful closed reduction was defined as the coxofemoral joint remaining in place without subsequent reluxation during the study period (January 2008 to May 2020).
Materials and methods
An electronic medical record search was performed at Ocean State Veterinary Specialists and Bay State Veterinary Emergency and Specialty Services for all cats with a diagnosis of coxofemoral joint luxation between January 2008 and May 2020. Cases without radiographs available for review were excluded. Data recorded included age, breed, sex and reproductive status, cause of coxofemoral joint luxation (as reported by the owner, if known), direction of coxofemoral joint luxation, the presence of concurrent injuries, ease of reduction (if noted in the record at the time of closed coxofemoral joint reduction), time elapsed between the date of injury and date of closed coxofemoral joint reduction, whether or not a bandage was applied after reduction, the type of bandage and the length of time the bandage was left on.
Maintenance of reduction was evaluated by palpation on physical examination by a veterinarian or radiographs, when available. Additional follow-up information was acquired from both the primary care veterinarian’s records and owner questionnaires. Owners were contacted by telephone and responses to a standard set of questions were recorded (Figure 1). Information regarding veterinary clinics (emergency or primary) the cat had been seen at since the injury, level of activity restriction, residual lameness or gait abnormalities, extent of recovery, activity level (indoor only or indoor/outdoor status), medication administration and cause of death, if applicable, was requested. Medical records from all known veterinary clinics the cat had been seen at since the injury were requested. The patient was considered lost to follow-up if five attempts to contact the owner were made without a response.
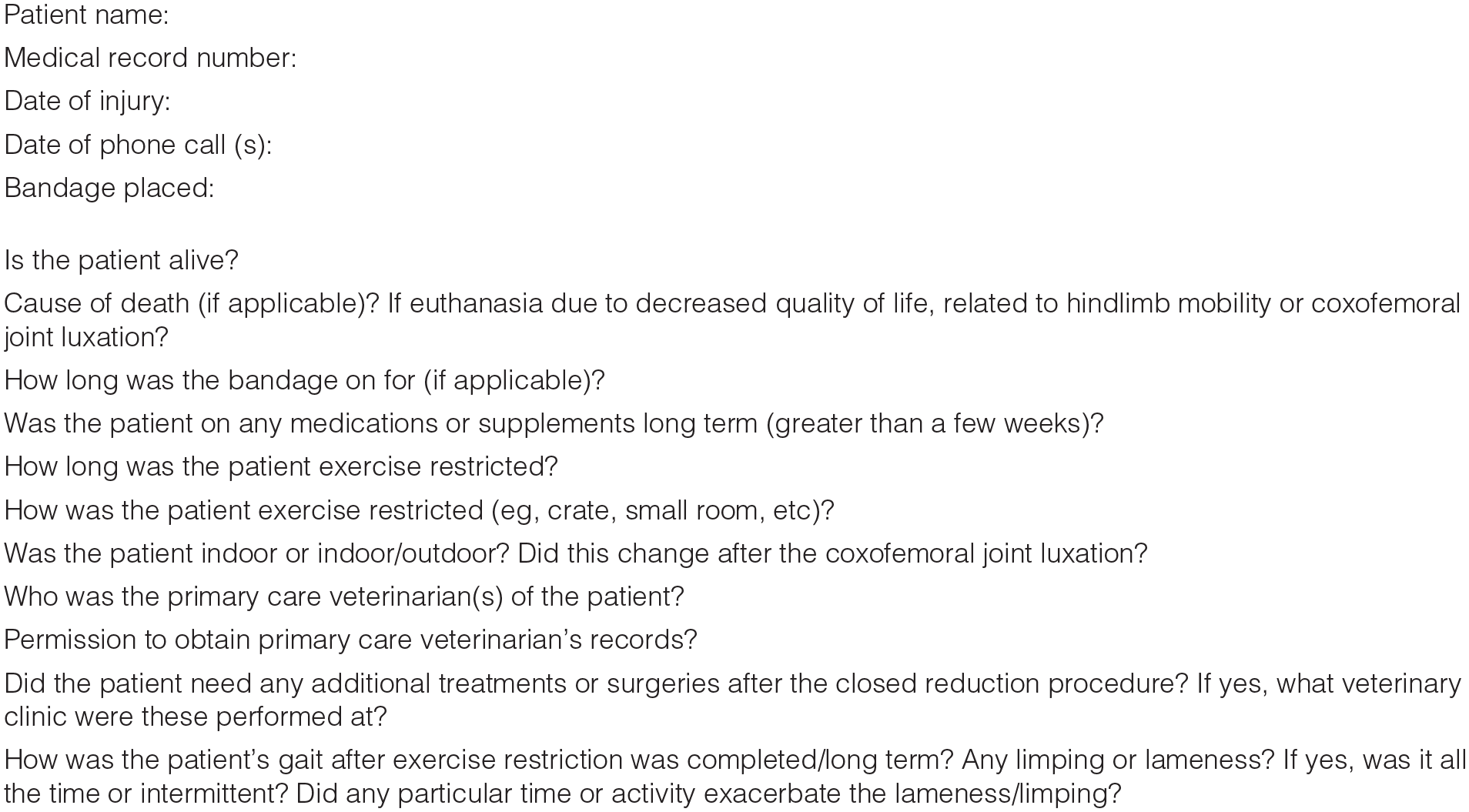
The set of standard questions asked to owners that were contacted by telephone
The number of days from closed coxofemoral joint reduction until either the coxofemoral joint reluxated or the end of follow-up was calculated. End of follow-up was determined by the date of the last physical examination by a veterinarian, date of death or date of the last communication with the owner. A positive outcome was determined if the patient continued to have no lameness at home and if a physical examination was performed by a veterinarian documenting the coxofemoral joint to be in place prior to the date of our communication with the owner.
Statistical analysis
The response variable was time to reluxation. The factors that could affect reluxation were breed (domestic shorthair or other), age, sex (male or female), entire (yes or no), direction (dorsal or ventral), concurrent injury (yes or no), ease of reduction (difficult, moderate or easy), time from injury to reduction and bandage (yes and no). Analysis was undertaken by means of Cox proportional hazards regression. The proportional hazards assumption was tested by means of hazard rate and scaled Schoenfield residual plots. Univariate Cox regression (continuous or ordinal factors) or Kaplan–Meier analyses (categorical factors) were initially performed. If the univariate P value was <0.10, then the factors were entered into a multivariate Cox regression and retained if P <0.10. All previously unused or deleted factors were then individually added to the equation and retained if P <0.10. P values <0.05 were considered significant. Statistics were performed using a commercial statistics software (NCSS 2019, version 19.0.6).
Results
Eighty-seven cats presented to Ocean State Veterinary Specialists and Bay State Veterinary Emergency and Specialty Services between 1 January 2008 and 1 May 2020 with a coxofemoral joint luxation diagnosed on radiographs. Nine cats were euthanized on presentation owing to the severity of concurrent injuries. Of the remaining 78, a closed reduction was not attempted in 27 cats owing to concurrent injuries (n = 12), financial constraints (n = 8), chronicity of coxofemoral joint luxation (n = 3) or surgeon bias (n = 4). Of the 27 cats that did not have closed reduction attempted, 16 had a femoral head and neck ostectomy performed. Crate rest and medical management with pain medication were performed in five cats. Two cats had amputations performed owing to the severity of concurrent injuries to the limb. One cat had an open reduction performed. Three cats had no surgical procedures performed and were lost to follow-up after being discharged from the hospital.
Closed reduction was attempted in 51 cats. Twenty-four of these cats were female (20 spayed and four entire) and 27 cats were male (25 castrated and two entire). Median age was 8 years (range 4 months to 17 years; mean 7.54 years). Domestic shorthair cats were over-represented (n = 39), with the remaining 12 consisting of other breeds (five domestic longhairs, three domestic mediumhairs, one Burmese, one Siamese, one Maine Coon and one Russian Blue). The most common cause of coxofemoral joint luxation was unknown trauma outdoors (n = 35). Other causes included accidental trauma caused by the owner (n = 5), being attacked by a dog (n = 5), falling from a height (n = 3) and vehicular trauma (n = 3).
In 22 cats the left coxofemoral joint was luxated and in the remaining 29 cats the right coxofemoral joint was luxated. Coxofemoral joint luxations were categorized as either craniodorsal (n = 41) or caudoventral (n = 10).
Thirty-one cats had concurrent injuries, while 20 did not. Fourteen of these cats suffered only skin injuries (13 cats with lacerations/abrasions and one cat with bite wounds). Six cats had skin lacerations in addition to orthopedic injuries. Five cats had small mineralized bodies within the acetabulum of the luxated coxofemoral joint. Five cats had sacroiliac luxations (three cats with bilateral, one with ipsilateral and one with contralateral). Five cats had pelvic fractures (four cats with pubic fractures, two with ipsilateral ischial fractures and two with contralateral ischial fractures). Other orthopedic injuries included femoral head fractures (two cats), a sacral fracture (one cat), transverse vertebral fracture of the sixth lumbar vertebra (one cat), luxation of the seventh and eighth sternebrae (one cat), luxation of the third and fourth sternebrae (one cat), fractures of ribs 12 and 13, in addition to a luxation of caudal vertebraes five and six (one cat), and one cat with ipsilateral stifle instability and luxation.
Median time of injury to date of attempted closed coxofemoral joint reduction was 0 days (closed reduction was performed on the same day as the injury); the mean was 1 day. Thirty-one cats were closed reduced at day 0, 11 cats on day 1, five cats on day 2, three cats on day 3 and one cat on day 21.
Ease of closed reduction was recorded in the medical records in 27 cats; four were difficult to reduce, two were reduced with moderate difficulty and 21 were reduced easily. A bandage was applied in 19 cats after closed coxofemoral joint reduction (six with hobbles and 13 with an Ehmer), while 32 did not have a bandage placed. Hobbles were placed after reduction of ventral coxofemoral joint luxations, while an Ehmer sling was placed after reduction of dorsal coxofemoral joint luxations. The median duration of bandage application was 12 days (range 1–16, with four bandages on for an unknown duration).
The coxofemoral joint was not documented to reluxate in 27 cats. Four of these cats were lost to follow-up immediately after discharge and were therefore excluded. Removing these cats from the data, the overall success rate for management after successful closed coxofemoral joint reduction was 23/47. One cat that had successful management after a closed coxofemoral joint reduction reluxated its coxofemoral joint 1077 days later after a similar traumatic event that caused its first coxofemoral joint luxation (playing with the other household cat). Given that the coxofemoral joint reluxated nearly 3 years later, the second coxofemoral joint luxation was considered a separate and isolated event. Therefore, this coxofemoral joint was considered to have had successful management of the initial coxofemoral joint luxation after closed reduction. Therefore, the overall success rate of closed coxofemoral joint reduction was 24/47 (51%). These 24 cats were followed for a median of 699 days (interquartile range 19–1625).
The overall failure rate for cats after closed coxofemoral joint reduction was 23/47 (49%). Five of these cats’ coxofemoral joints were unable to be reduced at all. Of these five cats, two had a femoral head and neck ostectomy performed and one had a hindlimb amputation performed owing to concurrent stifle luxation. The remaining two cats were discharged on crate rest and pain medication and were subsequently lost to follow-up.
Eleven of the 23 cats that were considered to have a failed closed coxofemoral joint reduction reluxated their coxofemoral joints immediately under the same anesthetic/sedation event as the closed reduction was performed. Two cats’ coxofemoral joints reluxated the day after closed reduction. The remaining cats reluxated on day 2 (one cat), day 6 (one cat), day 7 (one cat), day 11 (one cat) and day 45 (one cat).
Risk factors for coxofemoral joint reluxation were evaluated for 42 cats. Of the remaining nine cats, five were unable to be initially reduced and the other four cats were lost to follow-up immediately after discharge from the hospital. Cats that had a bandage placed had a lower risk of coxofemoral joint reluxation (P = 0.02) than cats that did not have a bandage placed. No association was found between age, breed, sex, reproductive status, direction of coxofemoral joint luxation, concurrent injuries, time of injury to time of reduction, ease of reduction or type of bandage placed (hobbles or Ehmer sling).
Discussion
In this study, management of feline coxofemoral joint luxations using closed reduction was successful in 51% of cats, similar to previous reports of dogs. This supports our hypothesis that approximately half of cats with a coxofemoral joint luxation can be successfully managed with closed coxofemoral joint reduction. Seventy-eight percent of the coxofemoral joint luxations in this study were dorsal, consistent with previous studies. 2
In this study, concurrent injuries in patients that had a closed coxofemoral joint reduction performed did not have a statistically significant effect on the success of the closed reduction of their coxofemoral joint luxations. Five cats had a small mineralized body within the acetabular space of the luxated coxofemoral joint with a radiographically intact acetabulum and femoral head. This fragment likely represented an avulsion fragment from either the acetabulum or the femoral head from the origin or insertion of the ligament of the femoral head. Three of these five cats had additional injuries: one with skin wounds, one with a sacral fracture, and the third had a contralateral sacroiliac luxation and ipsilateral ischial and pubic fractures. These three cats all had successful closed coxofemoral joint reductions performed with no coxofemoral joint reluxation during the study period. Of the other two cats, one was lost to follow-up and one reluxated after 11 days, after which the cat had a femoral head and neck ostectomy performed. Closed reduction in eight dogs and two cats with an avulsion fragment from the femoral head within the coxofemoral joint had satisfactory outcomes, according to a 1986 study by Basher et al. 2
Two cats with femoral head fractures of the luxated coxofemoral joint had closed reductions performed. In both cats, the femoral head fracture was not seen by the initial emergency clinician who performed the closed reduction procedure. The fracture was noted on the radiology report received the following day. It is possible that if there was a known femoral head fracture, closed reduction would not have been attempted in these two cats. One of these two cat’s coxofemoral joints reluxated immediately and was unstable, so a femoral head and neck ostectomy was performed. The other cat’s coxofemoral joint was initially in place, but on a recheck examination 3 days later it had reluxated. A femoral head and neck ostectomy was also performed in this cat. The fracture of the femoral head may have contributed to the instability of the coxofemoral joint and subsequent reluxation.
Ease of reduction, when recorded in the medical record, was also not statistically significant in this study. Anecdotally, the amount of periarticular soft tissue trauma around the joint may affect the ease of reduction of the luxation. For example, if the joint capsule is torn near the femoral neck or avulsed from the femoral neck the joint capsule is more likely to be trapped between the femoral head and the acetabulum when closed reduction is attempted. 10 Theoretically, this could make it easier for the joint to reluxate. Therefore, if closed reduction is more difficult, it may indicate that fewer periarticular soft tissues are disrupted and that it may be more difficult for the joint to reluxate. However, this is a very subjective parameter and only 27 cases had ease of reduction recorded in their medical records. A standardized scoring system to determine ease of reduction in a larger study population may provide more insight into whether this parameter is a useful indicator for determining the likelihood of coxofemoral joint reluxation.
Having a bandage placed was shown to be associated with a decreased risk of coxofemoral joint reluxation after closed reduction in this study (P = 0.02). This should be interpreted with caution, as only 19/46 (41%) cats had a bandage placed after closed coxofemoral joint reduction. The bandage type and duration the bandage was left on was also not standardized. In 4/19 cats, the bandages came off after only 1 day and was not replaced. Therefore, it is possible that the bandage did not play a role in the success of closed coxofemoral joint reduction in these four cats. If these four cats are excluded, having a bandage placed is no longer associated with a decreased risk of coxofemoral joint reluxation. A 2019 study that included 92 dogs showed that 50% of patients with an Ehmer sling placed after closed reduction experienced soft-tissue injury secondary to the sling. One of the risk factors for severe soft tissue injury in this study was poor owner compliance. 11 In our experience, cats are often more difficult to exercise restrict and less tolerant of bandages. Therefore, cats may require more frequent rechecks with a veterinarian to evaluate the bandage if owners are unable to do so at home. Difficulty evaluating the bandage at home could lead to poorer owner compliance and potentially a higher risk of soft-tissue complications with bandaging in cats. Additional studies are needed to further assess whether post-reduction bandaging may be of benefit in cats.
The main limitations of this study result from its retrospective design. The anesthetic/sedation protocols were not standardized, and closed reductions were performed by veterinarians of varying experience (surgeons, emergency veterinarians, interns and residents). Some patients were placed under general anesthesia and some patients only received heavy sedation. It is our experience that reducing coxofemoral joint luxations with general anesthesia is more successful. More research would be helpful to determine if coxofemoral joint luxations would be more easily reduced with the patient under general anesthesia (with or without an epidural) to allow the greatest muscle relaxation.
The retrospective nature of this study also led to a lack of standardization of post-reduction care (ie, exercise restriction and bandaging). Based on the owner questionnaire some cats were simply kept indoors, some were crate rested and some were confined to a single room. Duration of exercise restriction varied from a few days to 6 months. Only 19/46 cats had a bandage placed post-reduction, increasing the likelihood of a type II error.
An additional major limitation to this study was that not all patients received recheck radiographs after discharge from the hospital. Palpation of the coxofemoral joint can be hindered by a patient’s obesity and fractiousness. Subjectively, it is generally easier to palpate the anatomy of the cat coxofemoral joint than that of the dog. Despite this, radiographs would ideally be obtained at all recheck examinations, even if coxofemoral joint luxation is not suspected based on physical examination. Therefore, it is possible that the actual success rate of closed coxofemoral joint luxation is <51% owing to a reluxation being missed by not obtaining recheck radiographs.
Conclusions
Closed reduction is a reasonable first choice for many cats with a coxofemoral joint luxation as the reluxation rate is approximately 50%. If closed reduction is attempted, case selection is very important. Patients should have no intra-articular fractures (proximal femur or acetabulum) as these fractures may lead to incongruency of the coxofemoral joint. Intra-articular fractures also cause damage to intra-articular cartilage, cause chronic pain and accelerate the development of arthritis. If coxofemoral joint reduction is attempted in a patient with intra-articular fractures, open reduction and rigid stabilization is preferred to restore the joint surface and minimize the aforementioned long-term consequences. 7 A total hip replacement or femoral head and neck ostectomy would also be a suitable option for patients with intra-articular fractures. Patients with a small mineralized body within the coxofemoral joint but with an intact femoral head and acetabulum may still be considered for closed reduction.
Even with successful closed coxofemoral joint reduction, owners should be educated about the possibility of reluxation and be prepared for the possibility of the patient needing an additional procedure. If coxofemoral joint reluxation occurs after closed reduction, transarticular pinning or open coxofemoral joint reduction and stabilization can be performed to preserve the patient’s original anatomy. Total hip replacement or femoral head and neck ostectomy can be considered as a salvage procedure. However, approximately half of cats with closed coxofemoral joint reduction can have successful outcomes, maintain their original anatomy and do not require additional surgery.
Footnotes
Acknowledgements
The authors thank Joe Hauptman DVM, MS, DACVS for his assistance in performing the statistical analysis for this project.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or nonexperimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.