
Abstract
Practical relevance:
Traumatic joint luxations are usually associated with significant trauma and there may be concomitant systemic injury. Joints are unstable as a result of injury to one or more supporting structures and the clinician should aim to determine which structures are damaged with physical examination, diagnostic imaging and careful assessment under sedation/anaesthesia. The aim is to reduce the joint back to its anatomical position, and then to maintain this through repair of damaged structures. However, where this is not possible, replacement or removal (arthrodesis/excision arthroplasty) of the joint remain viable options.
Clinical challenges:
Owing to the small size of feline joints and the severity of damage often seen, surgical management of these cases can be challenging. The first priority is to ensure the patient is systemically well before embarking on any specific surgical treatment of a luxated joint. Cats also present challenges in the postoperative period and a lack of patient and owner compliance can be detrimental to postoperative outcomes.
Aims:
This article aims to help the reader diagnose joint luxations and to assist decision-making with an overview of the management and treatment options available.
Evidence base:
There are a number of original articles and textbook chapters in the literature covering aspects of different joint luxations, particularly for the more common luxations. This article draws on information from key feline research and, where necessary, extrapolates from relevant canine research. The authors also offer practical guidance based on their own clinical experience.
Introduction
Traumatic joint luxations are severely debilitating and usually the result of motor vehicle accidents or other significant injury such as the animal getting a limb trapped and then falling or struggling to get free. This review focuses on the diagnosis and management of traumatic appendicular joint luxations in cats, which are far more common than ‘congenital’ or developmental joint luxations. Conventional luxation terminology refers to the direction of displacement of the distal limb in relation to the proximal limb.
Presentation and initial management
Cats are usually lame, often severely to non-weightbearing, and the affected limb may also be abnormally positioned. With any trauma patient, the initial focus should be directed towards the systemic health and immediate stabilisation. A major body system assessment should be performed that prioritises the cardiovascular, respiratory and neurological systems. Prior to administering opioid analgesia, a basic neurological examination is also needed, including assessment of mentation, gait and finally withdrawal reflex and deep pain perception in all four limbs. Joint luxations are not infrequently associated with other soft tissue or orthopaedic injuries such as fractures. Once the patient is cardiovascularly stable and comfortable, a more thorough physical examination, including assessment of the luxation, can be performed, followed by diagnostic imaging/manipulation under sedation or anaesthesia. Where wounds are present, the principles of wound management should be adhered to prior to any orthopaedic surgery, and the approaches required are comprehensively covered elsewhere. 1
Forelimb joint luxations
Scapula
The scapula is attached to the thoracic wall via large muscle groups, with the primary muscle attachment being the serratus ventralis. Other important girdle muscles include the deeper rhomboideus and more superficial trapezius. As a mobile muscular connection between bones, this is technically a synsarcosis joint and scapular avulsion is therefore different from the other diarthrodial articular joint luxations described in this review, but is included for completeness.
Scapular avulsions are rare and typically occur after severe trauma. Clinically, the scapula is dorsally displaced during weight-bearing, resulting in a marked mechanical lameness. Although straightforward to diagnose on examination, radiographs or preferably CT (Figure 1) should be used to check for associated scapular fractures. 2 Neurological trauma to the brachial plexus can occur concurrently and a full neurological examination should be performed prior to intervention. Conservative management will lead to persistent lameness and therefore surgery is recommended.

(a) Lateral radiograph showing displacement of one scapula dorsal to the contralateral scapula and the dorsal spinous processes. (b) Three-dimensional reconstruction of a CT scan of the same region. CT is more sensitive for identifying associated fractures in the region. The long arrow shows the relative position of the avulsed dorsally displaced scapula compared with the normally positioned one (short arrow)
The goal of surgery is to temporarily affix the scapula to the body wall in an anatomically correct position to allow fibrous healing to occur. 3 Surgical intervention usually comprises primary reconstruction of the serratus ventralis muscle, followed by placement of fine orthopaedic wire, or heavy gauge suture material (such as 3.5 M nylon monofilament), through a single hole drilled in the caudal scapular angle, and then encircling the adjacent fourth or fifth rib. 3 Strict cage rest is recommended for 6 weeks post-surgery, and good outcomes are reported, although some dorsal drift of the scapula may be seen in the longer term.
Shoulder
Shoulder luxations are rare in cats.4,5 The shoulder joint is spanned by passive stabilisers (glenohumeral ligaments and joint capsule), and the major and minor active muscular stabilisers (infraspinatus, supraspinatus, subscapularis muscles, biceps brachii, teres minor and deltoids). The collateral ligaments are confluent with the joint capsule making them challenging to visualise in cats. While shoulder luxations could potentially occur in any direction, only lateral luxations are reported in cats;4,5 the authors have, in addition, seen medial luxations. Luxations can be difficult to diagnose clinically in a cat, and careful palpation under sedation or anaesthesia with radiography is recommended.
Closed reduction, under heavy sedation or general anaesthesia, should be attempted first once fractures have been ruled out with radiography/CT. Closed reduction is achieved by applying lateral or medial pressure to the greater tubercle while the leg is held in extension. Having an assistant apply gentle traction to the limb may assist with reduction. External coaptation should be attempted for 1 week following successful reduction (a Velpeau sling should be applied for a medial luxation and a Spica splint for lateral luxations), with cage rest for 4–6 in weeks total. After closed reduction and the application of external coaptation, orthogonal radiographs should be taken to ensure the shoulder joint remains reduced.
Surgical reduction and stabilisation is indicated if closed reduction fails or if there are concurrent injuries. Although quite well described and not infrequently performed in dogs, there is little experience with these procedures in cats. Assuming similar principles, the joint should be inspected and then repaired (capsulorrhaphy) using fine interrupted monofilament sutures; 1.5 M polydioxanone is preferred by the authors, and pre-placing them increases the accuracy and number placed. Further stabilisation is recommended – either through placing prosthetic collateral ligament or by transposing the biceps tendon medially (medial luxations) or laterally (lateral luxations). The authors would advise prosthetic ligaments placed through bone tunnels in the first instance (Figure 2), and this technique has been recently described in feline cadavers resulting in palpable and objective stability in all treated joints. 6 Although not yet evaluated in clinical cases, this type of technique is well recognised in dogs.7,8

Model showing bone tunnel locations and sutures for repair of traumatic shoulder luxation. Dashed and solid lines indicate medial and lateral sutures, respectively
For severely damaged shoulder joints or a failed primary repair, there are several salvage options. Excision arthroplasty (both the glenoid and humeral head) or partial distal scapulectomy would relieve pain and promote formation of a pseudoarthrosis. The suprascapular nerve courses under the acromion and should be preserved. Excision arthroplasty for a comminuted scapula fracture has been shown to provide a good long-term functional outcome with an acceptable degree of mechanical lameness. 9 Shoulder arthrodesis is significantly more complicated; however, the outcomes can be excellent in the authors’ experience. A craniolateral bone plate (preferably with locking screws) and screw fixation is applied to maintain the shoulder at 105–110° while arthrodesis progresses (Figure 3).

Lateral postoperative radiograph of a shoulder arthrodesis stabilised with a 2.4 mm locking compression plate, plus a K-wire and screw (placed as a lag screw to compress the surfaces together) crossing the joint
Elbow
Elbow luxation is rare in cats due to the inherent stability of the joint courtesy of the anconeus locking into the olecranon fossa unless the elbow is flexed more than 45° (Figure 4). Around 65% of elbow luxations are lateral, 10 thought to be due to a combination of a larger medial humeral trochlea and its more acute distal articular slope minimising medial movement. Based on cadaveric cat studies, both medial and lateral collateral ligaments need to be damaged for elbow luxation to occur. 11 Elbow luxations, therefore, usually require significant trauma and concurrent injuries can be seen in up to 10% of cats, including fractures of the head and forelimb as well as pulmonary injuries. 10 Note that if the radial head is luxated in association with an ulnar diaphyseal fracture, this is a particular injury called a Monteggia fracture (not covered in this article).

Three-dimensional CT reconstructions of the feline elbow; (a) craniolateral view and (b) caudomedial view. The arrow in image (b) highlights the anconeal process engaging in the caudal humeral fossa and providing stability to the elbow joint (cats do not have a complete supratrochlear foramen, as seen in dogs). Also note the medial supracondylar foramen (arrow [a]; not present in the dog), which contains the median nerve and brachial artery

Cats will normally present non-weightbearing with the elbow slightly flexed and the antebrachium in slight adduction. The elbow will be markedly swollen, painful and crepitant. Depending on the direction of the luxation, the lateral humeral epicondyle will be more palpable with a medial luxation and less evident with a lateral luxation. Radiography should be performed to assess for fractures before attempting closed reduction (Figure 5a,b). Closed reduction (see box below) is recommended but is only successful in 50% of cats. 10 After reduction, the elbow is assessed by performing the Campbell’s test (see box below); if it re-luxates or is highly unstable, surgery is recommended. If stable, then a Spica splint or Robert-Jones bandage that maintains the elbow in extension is recommended for 3–4 weeks in conjunction with cage rest. If not tolerated, then cage rest is a reasonable alternative.
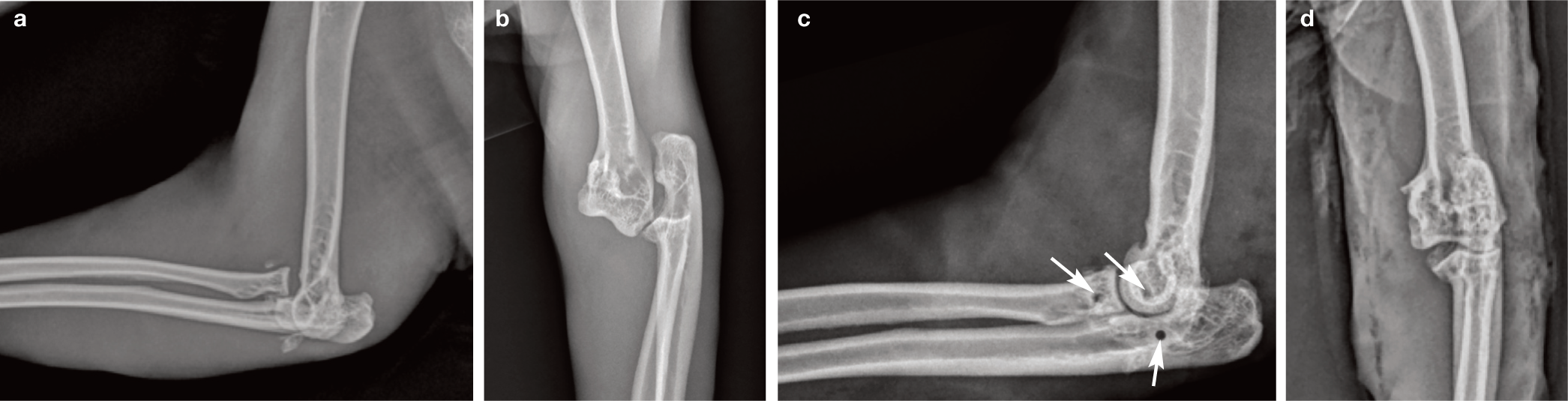
(a) Mediolateral and (b) caudocranial radiographs showing a lateral elbow luxation with small comminuted fragments, consistent with avulsion injuries of the collateral ligaments. Note that the small ovoid bone just cranial to the radial head (in image [a]) is a sesamoid in the supinator; this is not uncommonly seen in cats, and does not represent an avulsion fragment. (c) Mediolateral and (d) caudocranial radiographs post-surgery with the elbow reduced. Arrows indicate the position of the three bone tunnels drilled for placement of the prosthetic ligaments.
Surgical repair involves an open lateral approach (irrespective of the direction of luxation) and prosthetic ligaments are placed either via bone tunnels or using screws with washers or suture anchors. The authors prefer bone tunnels owing to the small size of the feline elbow, and both biomechanical and small clinical series support their application.11,12 Separate 2.0 mm transcondylar, transradial and transulnar bone tunnels are drilled from lateral to medial, and suture prostheses are placed to stabilise the joint (Figure 5c,d). A small medial approach and threading the suture onto a straight-eyed needle help with placement. Polydioxanone or nylon monofilament suture is appropriate and the authors recommend using 3.5 M sized suture, although doubled 1.5 M has been reported. 12 Any remaining ruptured ligaments and joint capsule should be sutured with fine slowly absorbable monofilament sutures, such as 1.5 M polydioxanone. Cage rest without coaptation is recommended for 4–6 weeks postoperatively.
Carpus
The carpus has a complex anatomy, with seven carpal and five metacarpal bones arranged in three joint levels: antebrachiocarpal, middle carpal and carpometacarpal. The feline and canine manus differ a little as cats do not possess a straight medial collateral ligament of the carpus (dogs have a straight and oblique component). Further detail on the anatomy and comprehensive management of carpal injuries is available elsewhere. 13
Carpal luxations and hyperextension injuries are common and most readily apparent on physical examination, with affected cats having a palmigrade stance. Radiography under sedation or anaesthesia is nevertheless critical for two reasons: (1) to determine if there are fractures present; and (2) to facilitate stress radiography, which enables the exact location of the instability to be determined. Carpal hyper-extension injuries associated with injury to the antebrachiocarpal, middle carpal or carpometacarpal joints are most common, and are associated with damage to the palmar ligaments and palmar fibrocartilage. Unfortunately, these structures cannot heal sufficiently to provide stability and, therefore, the treatment of choice is usually arthrodesis. In most instances, pancarpal arthrodesis is preferred, as although partial carpal arthrodesis has the advantage of maintaining the antebrachial carpal joint, and thus greater range of motion postoperatively, it can be difficult to confidently rule out injury at that joint level; if missed, this could lead to persistent lameness.
Pancarpal arthrodesis is best achieved with a dorsally applied plate and the usual principles of arthrodesis apply. Owing to the small size of the metacarpals, a hybrid pancarpal arthrodesis plate (Figure 6), with 1.5 mm screws in the third metacarpal and 2.0 mm screws in the radius, is recommended; however, other 1.5 or 2.0 mm plates, such as dynamic or locking compression plates, or veterinary cuttable plates can also be used. Dorsal plates can also be combined with Kirschner (K)-wires that cross the carpus to increase the stability of the repair. Whatever plating system is used, it is highly recommended that the plate covers more than 50% of the metacarpal bone to reduce the risk of metacarpal fracture. 14 The authors do not use postoperative casting and prefer strict cage rest to avoid potential issues and complications associated with casts. 15

Postoperative radiographic view of a 1.5/2.0 hybrid pancarpal arthrodesis plate with adjunctive K-wire. The plate has been applied to the dorsal aspect of the third metacarpal bone and the radius. Some surgeons will bend the plate to give 15° of carpal extension
Hindlimb joint luxations
Hip
Hip luxations are the most common joint luxation seen in both dogs and cats, and are usually the result of a motor vehicle accident.16,17 Luxation implies damage to the joint capsule, which should be repaired where possible as it provides stability to the joint. The teres ligament is usually also ruptured and radiographs should be carefully checked for any damage, or fracture of the dorsal acetabular rim, as this too has a role in hip stability.
The femoral head typically luxates in a craniodorsal direction (72%), 17 which commonly results in a severe to non-weightbearing lameness with the affected limb externally rotated and abducted. A clinical diagnosis can usually be made by determining the relationship of the greater trochanter to the dorsal iliac spine and ischial tuberosity (Figure 7). If the femur is within the acetabulum the landmarks form a triangle, with the trochanter the most ventral point. However, if the greater trochanter is no longer ventral relative to the ischial tuberosity and ilial wing a dorsal/craniodorsal luxation is likely present. Diagnosis is confirmed with lateral and dorsoventral radiographs (Figure 8a,b), which need to be evaluated carefully for acetabular fractures and fractures of the femoral head, particularly in immature animals. Caudoventral luxations are also possible but are much less common (Figure 8c,d).
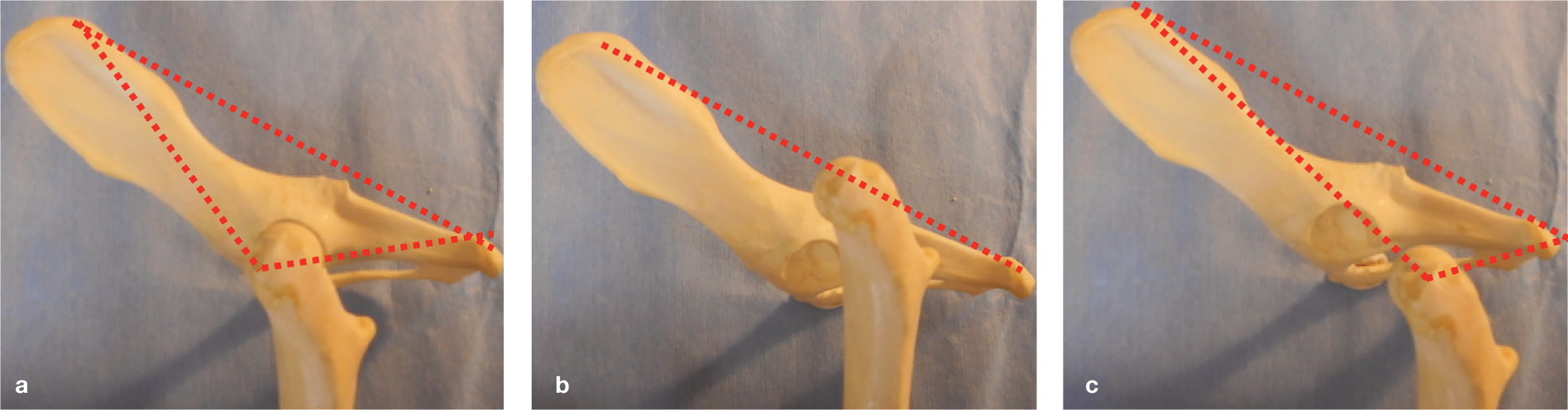
Model showing landmarks for diagnosis of a hip luxation: (a) shows the normal relationship of the landmarks, with the greater trochanter being ventral to the dorsal iliac wing and the ischial tuberosity; (b) in a dorsal or craniodorsal luxation, the greater trochanter is no longer palpable ventral to the other landmarks; (c) in a ventral luxation, the greater trochanter is usually more ventral and caudal than expected (compared with the contralateral)

(a) Lateral and (b) dorsoventral view radiographs showing a typical craniodorsal hip luxation. (c) Lateral and (d) ventrodorsal radiographs showing a typical caudoventral luxation, where the femoral head may overlie or engage the obturator foramen

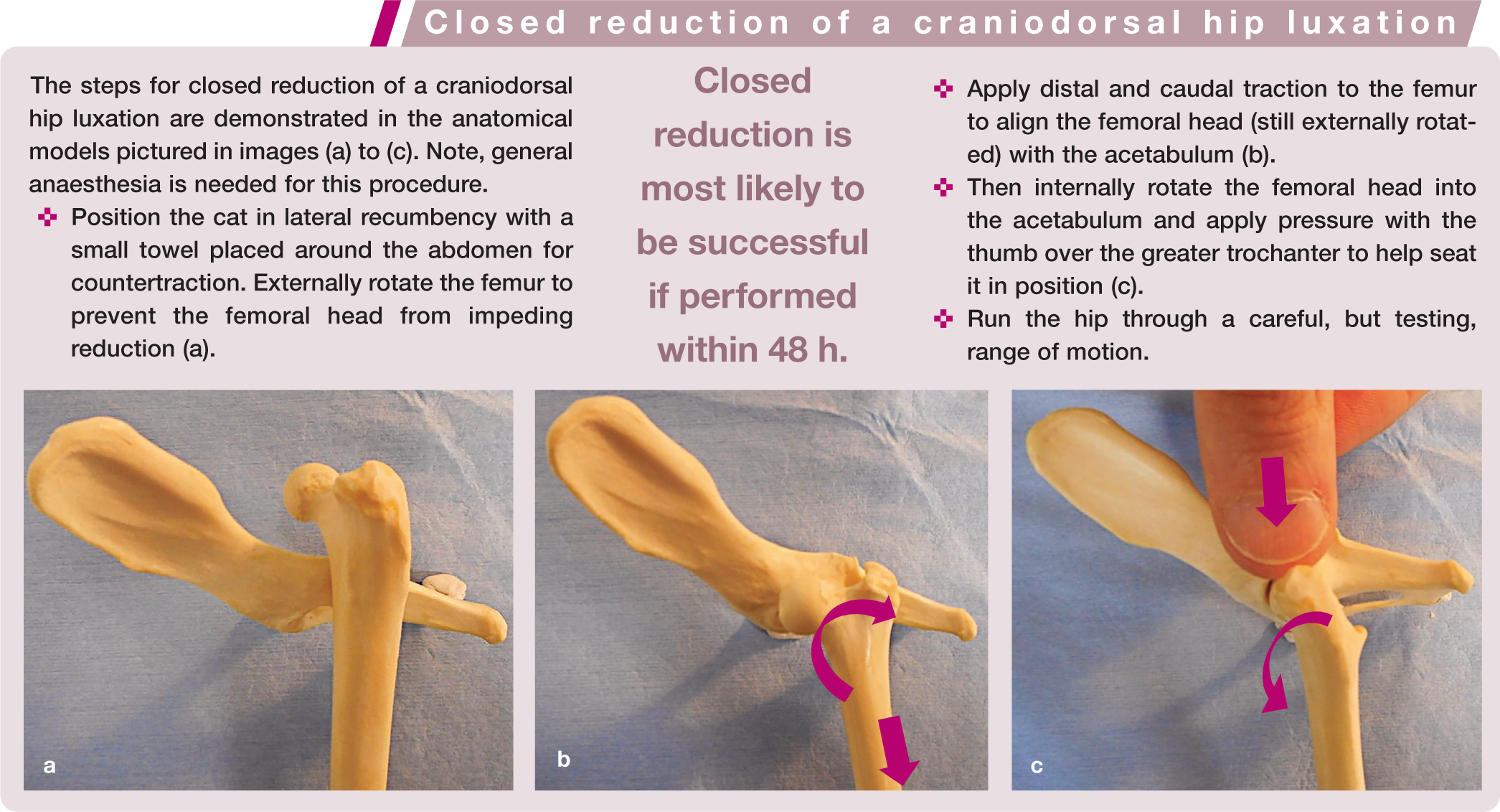
Closed reduction can be attempted and is most likely to be successful if performed within 48 h (see box on page 23). Note that radiographs should be taken first, as closed reduction is contraindicated if there are fractures of the femoral head, neck or acetabulum. The rate of re-luxation following successful closed reduction is around 50%. Historically, Ehmer slings have been recommended but they are hard to maintain in cats and do not seem to influence re-luxation rates; 16 also soft tissue complications are not uncommon. The authors prefer the alternative of strict cage rest for 2–3 weeks. If the hip is very easy to reduce, it is anecdotally more likely to re-luxate in the early postoperative period.
Surgical stabilisation is indicated if closed reduction is not possible, reluxation occurs or there are associated fractures requiring repair. Additionally, surgical stabilisation is recommended if there are other concurrent orthopaedic injuries. Open reduction has the added benefit of allowing the haematoma and soft tissues to be removed from the acetabulum, as these can impinge on the reduction. There are several techniques reported for internal stabilisation and the three best established are described below. Currently there is no good evidence to suggest one is better than another; however, whichever technique is chosen, capsulorrhaphy with monofilament absorbable or non-absorbable suture is recommended wherever possible (sometimes the capsule is completely avulsed). Pre-placed fine monofilament absorbable sutures (2 M or 1.5 M polydioxanone) in a simple interrupted pattern are the authors’ preference, as tying each one off sequentially can make it difficult to place subsequent sutures as the capsule tightens down.
Stabilisation techniques
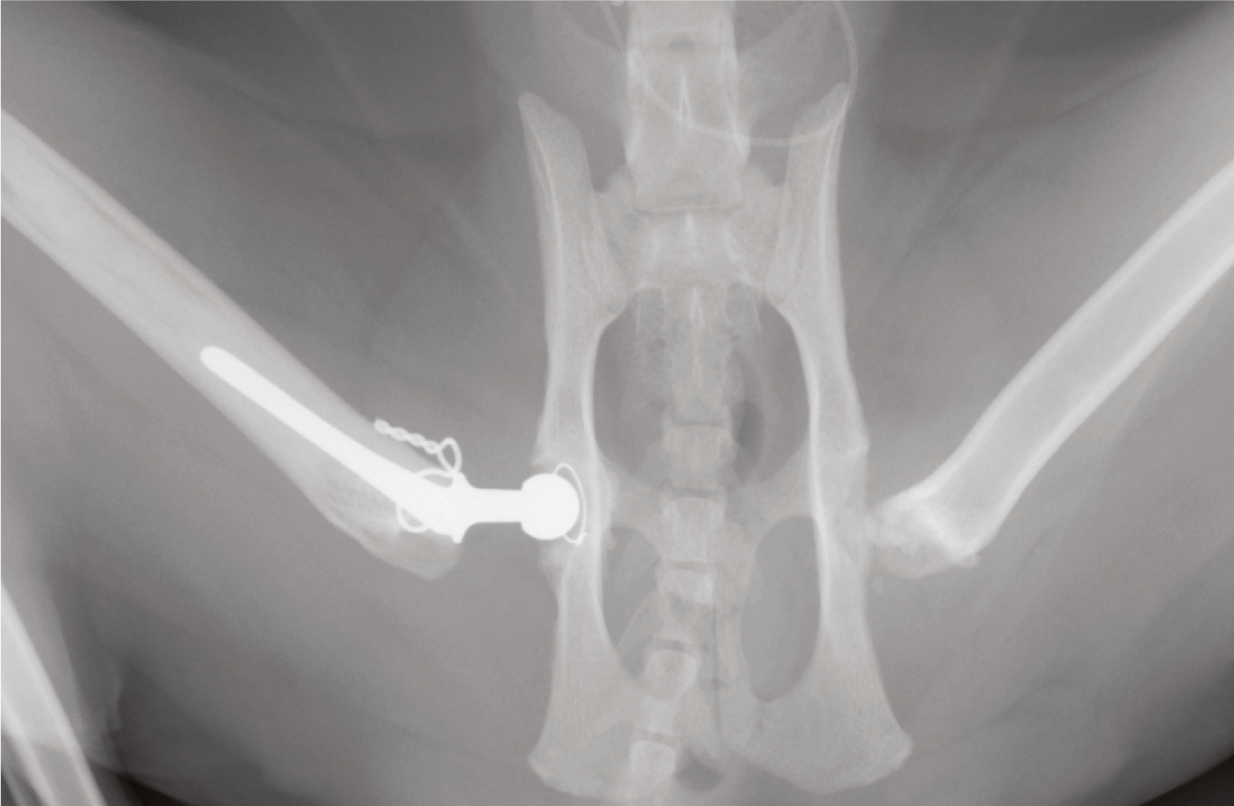
Modified Knowles toggle The modified Knowles toggle (Figure 9) has become popular in recent years, partly owing to the availability of commercial toggles. A tunnel is drilled through the acetabular fossa (usually 2.7–3.5 mm in size, depending on implants). A toggle, which is essentially a metal rod with a central eye-hole to thread suture through, is passed through the acetabular tunnel and then jiggled, so that the toggle flips to lie adjacent to the medial acetabular wall. The suture used could be 50 lb nylon leader line, or two strands of 4 M nylon or polydioxanone. A second hole through the femoral head and neck (2 mm in size most commonly) is then required to reattach the femoral head to the acetabulum. Correct placement of the femoral tunnel can be challenging and some advocate use of ‘C-guides’; the authors prefer to drill from the femoral head outwards, which requires extreme outward rotation of the femur to achieve access. Typically, the hole exits at or just below the third trochanter on the lateral aspect of the femur. The free ends of the suture are passed through the femur and tied with a button or via a second caudal-to-cranial hole drilled in the femoral diaphysis. A study of 14 cats with coxofemoral luxation treated with toggle stabilisation reported a success rate of 86% and good to excellent owner-assessed outcome. 18 ‘Homemade Piermattei’ toggles have been reported by modifying a small K-wire, although they have variable strength depending on configuration and are not recommended. 19

Toggle stabilisation: (a) anatomical model showing the position of the acetabular hole (arrow) and orientation of the femoral tunnel (dashed lines) for placement of the toggle; (b) a ventrodorsal radiograph post-placement of a hip toggle. Inset image in (a) shows a toggle without suture

Iliofemoral suture stabilisation: (a) anatomical model showing the position of the femoral and ilial tunnels, and arrangement of the suture, using 50 Ib nylon leader line stabilised with a crimp; (b) ventrodorsal radiograph post-iliofemoral suture placement
Once the tunnels are prepared, a suture (heavy gauge nylon monofilament, or multiple strands of braided absorbable suture such as 3 M polyglactin, or 50 lb nylon leader line with a crimp) is passed through the ilial hole from lateral to medial and gently retrieved using small mosquite forceps. It is then passed up and over the femoral neck and through a second tunnel, forming a figure-of-eight. The suture material is tied, or the leader line is crimped, with the leg mildly abducted and internally rotated.
After repair, it is common to see persistent internal rotation of the femur for several weeks until the suture loosens or breaks, by which point fibrosis should provide permanent stability. Advantages of this technique are that it does not require extreme external rotation of the femoral head and also does not risk damaging the articular surfaces of the hip as implants are not intended to pass through the fovea capitis (unlike the toggle and transarticular pin).



Transarticular pinning: (a) lateral and (b) ventrodorsal radiographs showing stabilisation of a craniodorsal hip luxation with a temporary transarticular pin
Salvage procedures
Salvage procedures are recommended when a primary repair fails or is not feasible due to concurrent fractures or damage to the articular surfaces of the joint, or when finances are limited; they are also indicated in the rare case of pre-existing hip dysplasia/severe osteoarthritic change.

Ventrodorsal radiograph showing a transilial pin placed to address sacroiliac instability, and a femoral head and neck excision for a non-salvageable traumatic hip luxation. It is critical to leave a smooth cut with no spurs and to ensure the femoral neck is removed, as well as the head. Inset image shows the orientation of the osteotomy (dotted line) to ensure complete removal of the femoral neck
Cats should be encouraged to exercise from 10–14 days after surgery, by playing games with them at home and, where tolerated, undertaking a passive range of motion exercises. Some cats are also amenable to hydrotherapy, which can be highly beneficial in recovery from FHNE. Complications reported include ongoing lameness, patellar luxation and sciatic neurapraxia. One study looking at owner assessment and follow-up veterinary examinations in 15 cats found 7/15 to have muscle atrophy and 4/15 to have pain on passive movement; however, 100% of owners felt the outcome of the procedure to be satisfactory. 21 A more recent study with owner questionnaire follow-up reported good to excellent medium- to long-term outcome, with 14/18 cats able to run, climb, jump, walk, play and groom normally. 22
Ventrodorsal radiograph showing cemented total hip replacement, and femoral head and neck excision on the contralateral side. A small cerclage wire has been placed around the proximal femur due to a small intraoperative fissure
Currently there is a lack of good data comparing THR with FHNE. One study compares THR in three cats with FHNE in two cats; outcomes such as pain on palpation, thigh circumference and range of motion were comparable or even favourable in cats with THR, 25 but larger studies are needed.
Stifle
Stifle disruption is a severely debilitating injury, often leading to complete femorotibial luxation (see Figure 14a in box on page 26). These injuries consist of a variable combination of rupture of the cranial cruciate ligament, caudal cruciate ligament, medial and/or lateral collateral ligaments and the menisci. The most commonly reported combination of injuries involves rupture of the medial collateral and the cranial and caudal cruciate ligaments. 26 A thorough review on stifle disruption is available and recommended for further reading. 27
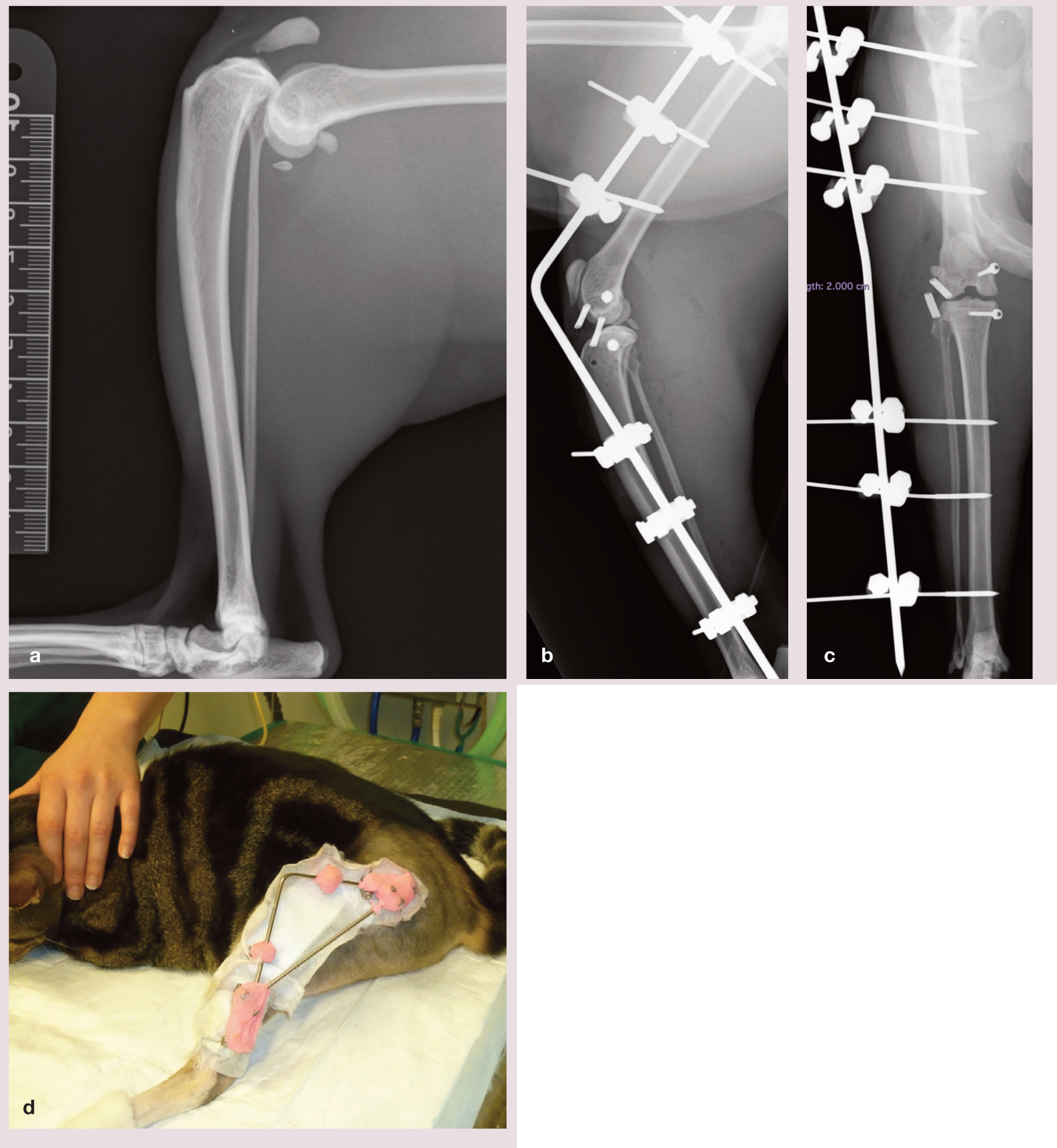
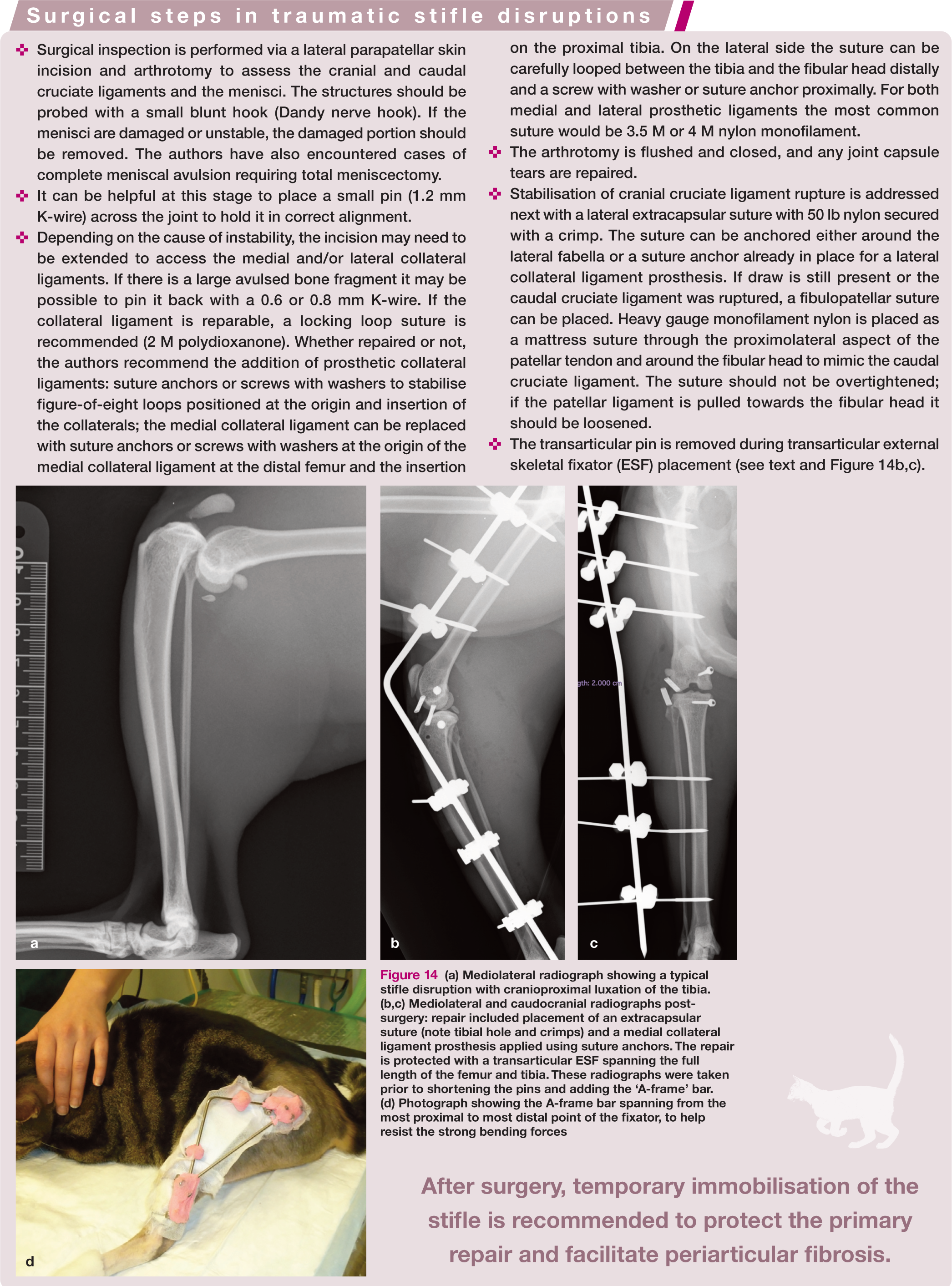
(a) Mediolateral radiograph showing a typical stifle disruption with cranioproximal luxation of the tibia. (b,c) Mediolateral and caudocranial radiographs post-surgery: repair included placement of an extracapsular suture (note tibial hole and crimps) and a medial collateral ligament prosthesis applied using suture anchors. The repair is protected with a transarticular ESF spanning the full length of the femur and tibia. These radiographs were taken prior to shortening the pins and adding the ‘A-frame’ bar. (d) Photograph showing the A-frame bar spanning from the most proximal to most distal point of the fixator, to help resist the strong bending forces
The diagnosis is best made under heavy sedation or general anaesthesia, where cranial draw, caudal draw, and varus and valgus stresses can be applied (ensuring the joint is reduced first). Radiographs, including stressed views, should be taken for planning and identification of other associated injuries, such as small avulsion fragments. Patellar luxation may also be present, but may not have been clinically relevant prior to the joint disruption – it is, therefore, important to carefully consider the cat’s orthopaedic history and check patellar tracking once the stifle has been surgically stabilised. The aim of treatment is to identify and repair damaged structures and to protect them while they heal. This typically involves primary repair of collateral ligaments where possible, followed by placement of prosthetic suture ligaments, and then temporary immobilisation.
The surgical steps in traumatic stifle disruptions are described in the box on page 26. While temporary immobilisation of the stifle postoperatively is recommended to protect the primary repair and facilitate the development of periarticular fibrosis, there are disadvantages of prolonged joint immobilisation including decreased range of motion, compromised cartilage health and reduced production of synovial fluid. 28 The optimal length of time for immobilisation is not known, but typically 2–3 weeks is adequate, and no more than 6 weeks. 29 Historically, this was achieved with a transarticular pin placed through the joint just proximal to the trochlear groove, exiting at the cranial cortex of the tibia. However, damage to intra-articular structures is inevitable and infection, pin loosening, bending or migration, bone fracture and pain are also reported. 30 The authors prefer a transarticular ESF; a type I laterally placed ESF, with an A-frame bar, is sufficient to immobilise the joint (Figure 14b–d). Complications associated with joint immobilisation may be avoided in part with the use of a hinged transarticular ESF. 31
The fixator is typically removed at around 4 weeks post-surgery, and a period of cage rest for up to 6 weeks in total is advised. Range of motion will initially be very restricted but should improve with increasing activity. Physiotherapy and other rehabilitation exercises will give a better outcome, and a more detailed review on feline rehabilitation can be found in an earlier JFMS series.32,33
If repair is not possible, or fails to produce a good result, then arthrodesis of the stifle is feasible. This is recognised to result in an altered gait, with many cats circumducting the affected limb. However, in a two-cat case series, both cats were climbing and jumping, albeit with circumduction of the affected limb, at 6 months and 20 months after surgery. 34
Tarsus
The tarsus, like the carpus, has a complex anatomy with multiple bones and several different joint levels. The tarsocrural (hock) joint and the tarsometatarsal joint levels are the ones most commonly involved in traumatic luxations.
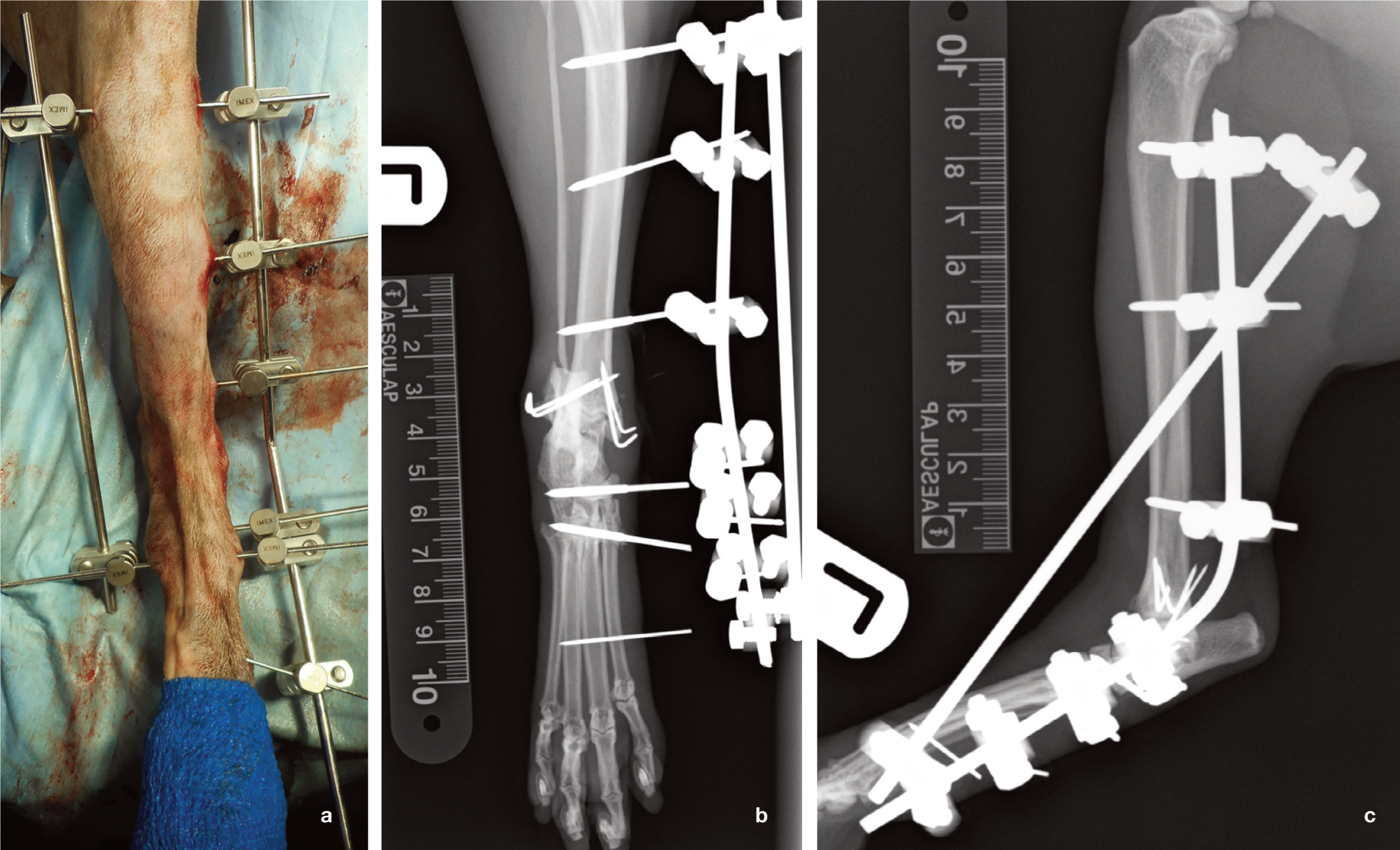
The tarsocrural joint is the articulation between the distal tibia, distal fibula and the talus (Figure 15). Tarsocrural instability is common in cats and may be a result of avulsion fractures of the medial and/or lateral malleoli or disruption of the collateral ligaments, and can be associated with a high degree of soft tissue injury (Figure 15a). 35 Careful manipulation of the tarsus under sedation or general anaesthesia can give an indication of the degree and location of instability; if the contralateral limb is normal this should be used for comparison, as cats have increased joint laxity compared with dogs. Mediolateral stresses should be applied with the tarsocrural joint in flexion and extension. Stress radiographs (valgus and varus stress [Figure 15c,d], and dorsal and plantar stress) are vital for accurate demonstration of the instability and may reveal previously missed non-displaced fractures (Figure 15b).
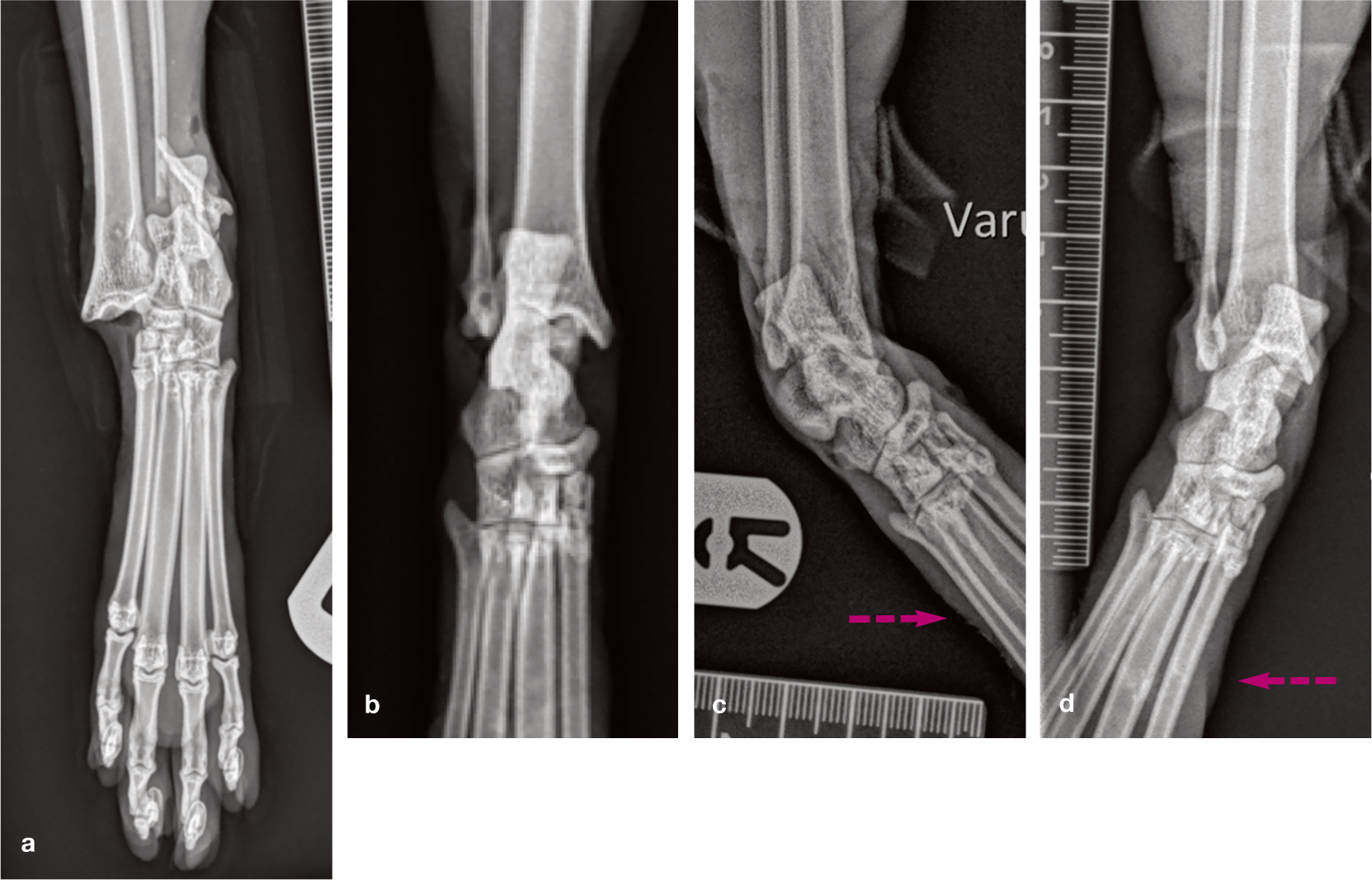
(a) Dorsoplantar radiograph showing a markedly displaced (laterally and proximally) tarsocrural luxation with distal fibular fracture. (b–d) Dorsoplantar radiographic views: (b) instability is not clear on a neutrally positioned tarsal radiograph; (c) varus and (d) valgus stress views reveal bilateral instability, worse on the lateral aspect. Arrows denote the direction of stress applied during radiography using tapes and ties
The malleoli are the point of origin of the medial and lateral collateral ligaments. Cats have short collateral ligaments only, made up of straight and oblique branches (Figure 16). The oblique branch of the medial collateral ligament is the tibiotalar portion and is partially hidden deep to the medial malleolus. The straight branch of the medial collateral ligament is the tibiocentral ligament and inserts on the dorsomedial process of the central tarsal bone. 37 The lack of soft tissue in this area predisposes the joint to open fractures and luxations, and the tarsus is particularly prone to shearing injury. For these cats wound management is the immediate priority once the cat is stable. There are several options for management of these luxations, as described below.

The medial collateral ligaments supporting the tarsocrural joint in a cat include the tibiotalar ligament, partially deep to the medial malleolus, and the tibiocentral ligament, with its insertion on the dorsomedial process of the central tarsal bone. The lateral collateral ligaments supporting the tarsocrural joint in the cat include the oblique talofibular ligament and the calcaneofibular ligament, which has an oblique and a straight component. Adapted from Nicholson et al, 36 with permission



Positions of medial and lateral collateral ligament drill holes and tunnels for prosthetic ligaments used in the repair of traumatic tarsal luxations. Adapted from Nicholson et al, 36 with permission
Photograph and caudocranial and mediolateral radiographs showing examples of a modified type II ESF (a), and a type I ESF with A-frame bar in position (b,c). In both cases the main bar was a bent Steinmann pin, which is a recommended alternative to connecting two straight bars with a double clamp
The transarticular fixator is also particularly useful in shearing injuries where there is soft tissue trauma in addition to joint destabil-isation. The fixator maintains the joint in reduction but can provide access for regular wound maintenance, as covered in detail elsewhere. 1
External coaptation with a splinted dressing or cast is an alternative to external skeletal fixation, but only if primary stabilisation has been performed as coaptation alone does not provide sufficient stability for ligament healing. However, soft tissue injury as a result of external coaptation occurs in up to 60% of cases and this rate may be higher in smaller patients with less soft tissue coverage. 15 One case series did not show any additional benefit of placing prosthetic ligaments with an ESF over a transarticular ESF without prosthetics; 38 however, some surgeons still advocate prosthetic ligaments, and the authors would use them if the injury was chronic.
Should the primary repair fail, or if joint preservation is not realistic, then salvage with a pantarsal arthrodesis is the best option. It is possible to perform an arthrodesis with an external fixator; however, this is not recommended and a plate positioned medially, 39 dorsally or dorsal and medial is advised.40,41
Other tarsal luxations
There are many small ligaments that stabilise the bones of the tarsus. Damage to the main plantar ligament leads to calcaneoquartal instability, which gives a bowed appearance to the pes and a plantigrade stance. Rupture of the short distal plantar ligaments, often with concurrent metatarsal fractures, produces tarsometatarsal instability (Figure 19a,b). Unfortunately, only dorsal instability lends itself to conservative management with splints or casts, whereas the preferred option for medial, lateral or plantar instability is to perform a partial tarsal arthrodesis, with a plate applied to the lateral aspect of the pes. The problem of the different size of the metatarsal bones relative to the tarsal bones is resolved by anatomic plates with smaller screw holes for the metatarsal and larger screw holes for the tarsal bones (Figure 19c).

Lateral (a) and dorsoplantar (b) radiographs showing tarsometatarsal fractures with luxation. A mediolateral postoperative radiograph (c) shows a laterally applied hybrid arthrodesis plate to manage the injury
Digit luxations (Figure 20) are generally rare. Athough surgery for these injuries is described, they are generally not especially amenable to direct repair. Initial management should be conservative, including closed reduction where needed to realign the joints and then support with coaptation while the joint fibroses. If lameness persists then excision arthroplasty of the joint or digit amputation could be considered.

Lateral (a) and dorsoplantar (b) radiographs showing severe metatarsophalangeal joint luxations. Closed reduction and stabilisation in a supportive dressing or placement of small tunnels with circumferential sutures are options for management
Key Points
Joint luxation can be a result of damage to a range of different ligamentous and soft tissue structures. Identification of the structures involved is key to selecting the most appropriate treatment.
Stress radiography is very useful for evaluation of the carpus and tarsus, and can also be helpful for the stifle. However, careful palpation (with neutral radiography to rule out concurrent fractures) is essential for all joints being evaluated, as instability is not always so well demonstrated on stress radiography.
The evidence base for treatment in cats is lacking compared with dogs. Furthermore, care should be taken when extrapolating studies from dogs due to some key differences in anatomy, particularly with regard to joint ligament arrangement.
Where specific implant and suture sizes have been suggested by the authors, they are recommended based on surgery for an average sized domestic shorthair cat. The clinician needs to carefully consider their selection of implants for any individual cat.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.