
Abstract
Objectives
The aim of this study was to compare post-mortem CT findings with necropsy findings in domestic cats.
Methods
Post-mortem CT and necropsies were performed in 20 cadavers of domestic cats. The sensitivity, specificity and agreement between the post-mortem CT and necropsy findings were determined.
Results
There were a total of 315 post-mortem findings; 183 were identified by post-mortem CT and 132 were identified by necropsy. Post-mortem CT demonstrated a higher sensitivity to identify the findings mainly in bones. The higher indices of agreement between post-mortem CT and necropsy were related to abnormalities of pleural space, bones and joints.
Conclusions and relevance
This study demonstrated that post-mortem CT and necropsy provided different information. Thus, their use in conjunction with each other might improve the understanding of the cause of death and the identification of post-mortem lesions.
Introduction
Post-mortem radiology and cross-sectional imaging have grown considerably since the introduction of virtual autopsy (Virtopsy) in 2003. 1 Virtopsy consists of postmortem use of modern radiology imaging modalities, such as MRI, CT and photogrammetry prior to necropsy. 2 Post-mortem CT (PMCT) has being increasingly used in human medicine because it is a fast and minimally invasive examination, presents little risk of contamination, and has a high sensitivity and specificity for the detection of small fractures, joints dislocations and the presence of foreign objects, such as projectiles of firearms and small quantities of gas, not always identified by necropsy.3,4 In addition, it allows three-dimensional reconstructions that also help to identify external body injuries. 5
Radiographic images should be taken prior to necropsies, to help pathologists detect intraluminal gas collections,6,7 but the use of PMCT is still in its infancy in veterinary medicine, with only a few isolated published case reports.8–14 Experimental research comparing PMCT and needle biopsy with conventional necropsy in dogs with histiocytic sarcoma has been reported. 15
Pet owners who want to know the cause of death of their animals might feel more comfortable allowing a PMCT rather than a necropsy because PMCT is non-invasive and causes no damage to the corpse. Also considering a clinical application, most veterinarians would like to know the cause of death of their patients, and PMCT may provide such answers, when necropsy is not permitted by the owner either because of personal or religious reasons.
Additionally, there is a forensic aspect related to PMCT. Approximately 50% of domestic violence victims report that their pets have also suffered some form of abuse. 16 Cats are the companion animals that suffer the most human abuse. 17 The increasing number of outdoor cats with access to the streets and surrounding neighborhoods make them easy targets for abuse. They are at increased risk of accidental trauma, with 24% of these animals being victims of mechanical injuries. 18 Burns, throwing from a height, drowning, intoxication, firearm injury, beating, mutilation and suffocation are the main forms of abuse against cats. 17 These types of injury can cause damage to internal organs/cavities. 19 Although some lesions may be easily detected by necropsy, other lesions, such as small fractures and pathological gas collections, are much more easily detected with PMCT. 20
We believed that PMCT might provide additional and valuable information prior to necropsies in cats, regardless of the cause of death. To our knowledge, there are no original research experiments of PMCT involving feline species. The hypothesis of this study was that PMCT could be a complementary imaging method to necropsy in domestic cats.
The aim of this study was to compare the findings of PMCT and necropsy in domestic cats.
Materials and methods
This was a prospective study (from June 2015 to April 2017). Twenty cadavers of domestic cats were subjected to PMCT, which was followed by necropsy. Cadavers of domestic cats of any age, sex or breed were included in the study. Informed consent was obtained from the donors of the cadavers.
The project was approved by the Ethics Committee of Animal Use, School of Veterinary Medicine and Animal Science of the São Paulo State University ‘Júlio de Mesquita Filho’ (UNESP) – Botucatu campus (number 81/2015) and School of Veterinary Medicine and Animal Science of the University of São Paulo (number 4720160216).
For each animal, two structured reporting systems were created with individual animal data (identification number, sex, age, body weight and clinical history). One was completed with necropsy findings and the other with PMCT findings (modified from Schweitzer et al 21 ). The radiologists were blinded to the necropsy findings and the pathologist was blinded to the PMCT findings. They were asked to determine the cause of death from the information gathered from PMCT or necropsy.
The cadavers were kept in a freezer at –18°C. Prior to the PMCT and necropsy, the cadavers were thawed at room temperature (15–35°C) for 24–48 h.
An entire body PMCT was performed for each cadaver using a 16-MDCT scanner (either Siemens SOMATOM Syngo CT 2012E Emotion or Philips MX8000-IDT). All cadavers were positioned in dorsal recumbency. The acquisitions were performed with a technique range from 120 to 130 kVp, and from 50 to 250 mAs. The slice thickness was set between 0.75 mm and 3 mm. The images were reconstructed using a bone/lung and soft tissue reconstruction algorithm. PMCT studies were viewed using a 27-inch iMac station and Horos viewer. Images were examined by two experienced clinicians on the basis of consensus (ACBCFP [Certified by the Brazilian College of Veterinary Radiology] and HGH [Diplomate ACVR and ECVDI]).
After PMCT, the cadavers were submitted to necropsy, performed by a veterinary pathologist (MRRM). The necropsy was performed through a mentopubic incision, followed by an in situ evaluation and removal of the organs in block extraction by groups to a posterior ex situ evaluation. During the necropsy, organ samples were collected for histological examination determined by the gross necropsy findings. If necropsy was not performed immediately after PMCT, the cadavers were kept in the same freezer until the necropsy could be carried out, following the same thawing process. After the necropsy, all cadavers were disposed of according to the current institution regulation.
Comparisons between PMCT and necropsy findings were performed according to the detected lesions/abnormalities in organs/systems. The comparison of all of the findings was made individually and grouped by organs/systems. For statistical analysis, necropsies were used as the gold standard. The analyzed parameters were sensitivity, specificity, positive predictive value and negative predictive value of PMCT, for each abnormality and organ/system. The kappa agreement index was set as poor (<0.00), slight (0.00–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80) and almost perfect (0.81–1.00). 22
Results
Of the 20 cadavers, seven (35%) were castrated males and 13 (65%) were spayed females. The mean ± SD weight of the animals was 3.43 ± 0.72 kg. The age of the cadavers was estimated as immature (<1 year; n = 2), adult (1–7 years; n = 15) and old (>7 years; n = 3). Two cadavers were Maine Coons and 18 were of mixed breed.
The mean ± SD time between death and PMCT scan was 24 ± 16.05 days. Only one case had no information on the time of death, as the cat was found dead on the road. Both PMCT and necropsy were performed on the same day in 15 cadavers. In the remaining five, the mean ± SD time between the PMCT and necropsy was 23 ± 12.63 days.
A total of 315 abnormal findings were identified; 183 using PMCT and 132 using necropsy (Table 1). Necropsy detected more skin and muscle lesions than PMCT, as well as subarachnoid hemorrhage, fluid in the mouth and trachea, pulmonary hemorrhage, hemopericardium and liver congestion. There was one cadaver with splenic rupture verified by necropsy that PMCT could not identify (Figure 1).
Total number of abnormal findings with post-mortem CT (PMCT) and necropsy with statistical analysis of PMCT vs necropsy considering each individual finding and the main groups

PPV = positive predictive value; NPV = negative predictive value; CNS = central nervous system; U = undetermined
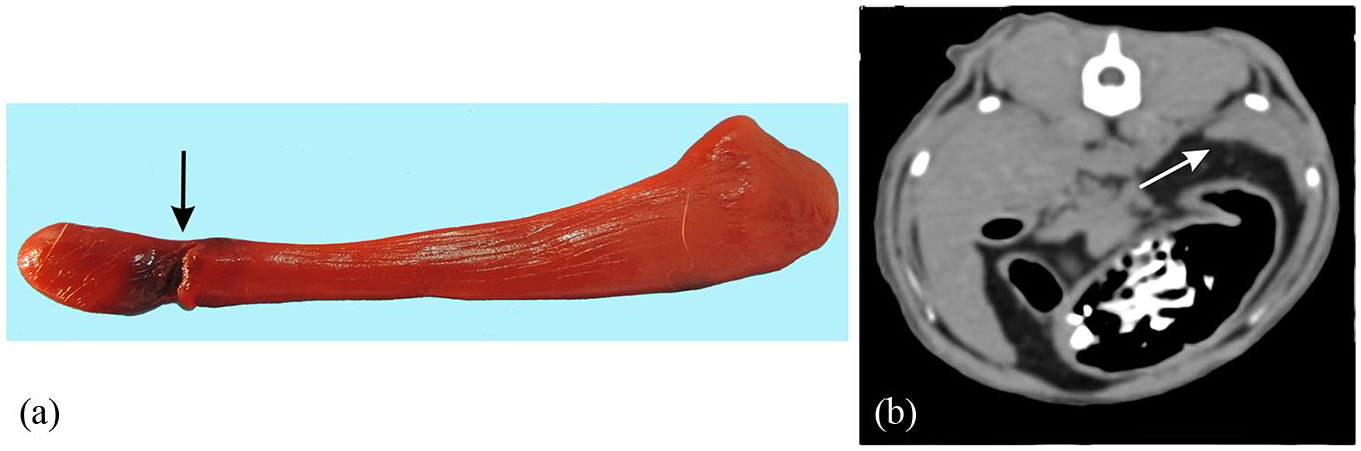
Mixed-breed male domestic cat. (a) Necropsy (background was manipulated to remove plate grooves) demonstrating a partial rupture in the dorsal extremity (head) of the spleen (black arrow), with an area of focal hematoma in the region of rupture. (b) Post-mortem CT transverse image in a soft tissue window (b) did not show the small rupture. White arrow points to the dorsal extremity of the spleen
PMCT was better at detecting gas in the subcutaneous tissue, brain and esophagus, and was better at identifying bowel distension and fluid content in the tympanic bulla and nasal cavity. Bone injury findings were also better identified by the PMCT, especially the skull and vertebra fractures (Figure 2). Nevertheless, one of the higher indices of agreement between the PMCT and necropsy were related to abnormalities of joints and bones (Figure 3). Pleural space agreement indexes were also one of the highest found in this study.

Mixed-breed male domestic cat that was found dead on the road. Post-mortem CT images in three-dimensional volume-rendered (a) caudal, (b) right and (c) left lateral aspects of the skull demonstrating a zygomatic process fracture of the temporal bone in the right side (black and white circles), and a temporal process fracture of the zygomatic bone also on the right side (white and black dashed circles). However, during (d) necropsy, these fractures were not identified. Focal hemorrhage (white arrowheads) in the right frontal musculature was seen and assumed to be secondary to contusion

Mixed-breed female domestic cat that was hit by a vehicle. (a) Necropsy showing separation of the interincisive and median palatine sutures (white arrow) and mandibular symphysis (white arrowhead). Post-mortem CT images with three-dimensional volume-rendered (b) ventral and (c) frontal aspects, which also identify both separation of the interincisive and median palatine sutures (red arrowhead) and mandibular symphysis (white arrowhead)
Of the 20 cadavers in this study, nine (45%) were presented owing to traumatic injury. Regardless of trauma, 11 (55%) cats were euthanized owing to the poor prognosis of the animal’s disease condition. The cause of the death of the nine cats that were not euthanized was established by combining information from the findings observed in PMCT and a comparison with the cause of death established by necropsy (Figure 4).
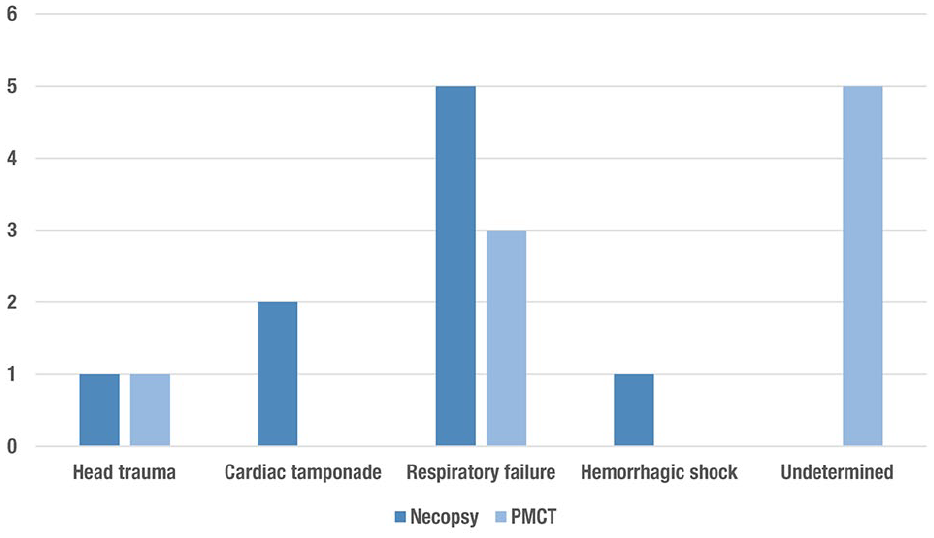
Causes of death detected by each method (necropsy and post-mortem CT [PMCT]) in the nine cats that died of natural causes
Discussion
PMCT is sensitive to the detection of gas in the body (cavity, organs and vascular system) and the amount of accumulated gas can represent a state of decomposition. 14 Pneumocephalus, identified in 14/20 animals with PMCT, is a common sign of autolysis. 23 Even though the presence of air inside the skull may also be associated with adjacent skull fractures, this was not true in this study as there was no pneumocephalus detected with concurrent skull fractures.
In this study, PMCT was superior to necropsy in detecting gas in the vascular system, subcutaneous tissue, pleural and peritoneal cavities, as reported in humans. 3 Necropsy is not sensitive in detecting very small amounts of gas, as gas easily escapes during necropsy. Thus, the calculated sensitivity of the technique, considering necropsy as the gold standard, often presented undetermined values such as pneumoperitoneum, pneumocephalus and gas in large vessels, eye globes, cardiac chambers and in the wall of the urinary bladder. However, pneumothorax was detected easily in necropsy, and thus PMCT obtained 100% sensitivity, 95% specificity and a kappa index of 0.83, which is considered an ‘almost perfect’ correlation. This is similar to results obtained in a French study of humans. 24
Almost half of the cats in this study had a history of trauma. Most of the bone injuries found were identified only by PMCT, which reflected in a moderate kappa value of 0.47. In addition, PMCT has identified chronic lesions and degenerative joint diseases, which may not contribute to the cause of death, but help to elucidate many of the clinical signs. PMCT is thus recommended prior to necropsy for any cadavers suspected of having a history of trauma, as it is more sensitive than necropsy to detect osseous fractures.
This study demonstrated that PMCT has a high sensitivity and specificity in identifying soft tissue/fluid content in body cavities in cases of traumatic death. The findings may represent autolysis or be related to a previous disease. The sensitivity in determining the presence of fluid content in the nasal cavity was 83%. However, PMCT was not able to determine the type of nasal fluid, such as blood. While the cadavers were thawed prior to the examinations, some of them were still internally frozen, which made it difficult to assess the actual Hounsfield unit values of the frozen organs and effusion. 25 Thus, classification of the effusion could not be performed with PMCT. The freezing process can also cause damage to the tissues and compromise pathological evaluation. If possible, cadavers should be completely thawed prior to both PMCT and necropsy.
It has been reported that it is difficult to differentiate the etiology of pulmonary lesions seen in PMCT that present as the ground-glass attenuation pattern. 26 In this study, pulmonary edema was one of the main findings of necropsy but had a poor kappa index (–0.38) with PMCT. In human cadavers, PMCT pulmonary evaluations have the same limitations, as the positional hypostasis (accumulation of post-mortem fluid or blood in certain parts of the body due to gravity) presents characteristics that can be confused with injuries such as pulmonary edema, aspiration and pneumonia. 26 Interestingly, the hypostasis in humans does not appear to be the same as in small animals. Human corpses are hardly repositioned, except in criminal acts. In this study, the accumulation of blood on a particular side of the lungs has not been as evident as in humans, as cats are lighter than humans and have been repositioned as a result of packing, storing, thawing and positioning for PMCT, without a particular positioning protocol. However, the poor kappa index led us to conclude that PMCT was not able to differentiate pulmonary edema from hypostasis. Future studies could be performed to better elucidate the differentiation between common findings of cadaveric phenomena and ante-mortem pulmonary lesions.
The evaluation of abdominal cavity findings showed interesting results regarding the detection of liver diseases. In this study, the sensitivity of the test was 75%, specificity was 94% and kappa index was moderate (0.69). Values were considered high when compared with a human study. 23 It was reported that parenchymal findings of abdominal organs, even with laceration of abdominal organs, are poorly identified by PMCT, especially in non-contrast studies. 23 Similarly, liver laceration was observed on necropsy in one cadaver in this present study; however, PMCT was not able to detect the lesion. PMCT also failed to detect a splenic rupture in one of the cats.
Regarding the urogenital system, PMCT showed 63% sensitivity and 50% specificity. Renal atrophy, renomegaly, kidney stones and urinary bladder blood clot had higher sensitivity and specificity among the nephropathies in this study.
The most frequent cause of death was respiratory failure, proposed by both PMCT and necropsy techniques. In contrast to a recent human study that showed a kappa correlation index of 0.75 in determining the cause of death by non-contrast PMCT, 27 this study showed difficulty in determining the immediate cause of death, with five cases classified as undetermined through PMCT. Nevertheless, the results showed that in some cases where PMCT identified lesions not seen at necropsy, such as in skull fractures or in the identification of a small amount of gas, the association between the two techniques should provide a better understanding of the cause of death.
One of the shortcomings of this study is the low number of cadavers and the heterogeneity of the sample. It would have been good to have a larger number of cadavers that could have been separated into groups with a significant amount of different types of suspected cause of deaths. The presented nine cases of violent death and 11 clinical cases showed that the use of PMCT was equally important in both forensic and clinical circumstances.
Another limitation of this study was that necropsy was considered as the gold standard for statistical analysis, which resulted in some undetermined values due to the higher number of PMCT lesions identified in comparison with necropsy. Yet, a comparative study using the kappa agreement index allowed both techniques to be evaluated independently of the gold standard.
Conclusions
This study demonstrated that PMCT and necropsy provided different information regarding post-mortem findings in cats. Thus, the combination of PMCT and necropsy may improve the understanding of the cause of death and identification of post-mortem lesions mainly related to osseous fractures and accumulation of gas in the organs and body cavities.
Footnotes
Acknowledgements
The images used in this study were acquired by the PISA (Plataforma de Imagem na Sala de Autópsia), São Paulo University Medicine School, and by the Surgery Department of the School of Veterinary Medicine and Animal Science, University of São Paulo, Brazil.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and belongs to the project entitled ‘The Legal Veterinary Medicine Applied to Expertise in Cases of Crime Against Fauna’, approved in the Forensic Science Publication Notice 25/2014 (grant number 10.99999.000199/2016-08).
Ethical approval
This work involved the use of experimental animals; or involved the use of non-experimental animal(s) (owned or unowned) outside of established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care. The study therefore had ethical approval from an established committee as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.