
Abstract
Practical relevance:
Abdominal ultrasound plays a vital role in the diagnostic work-up of many cats presenting to general and specialist practitioners. Ultrasound examination of the kidneys and perinephric space can provide important information on several conditions including chronic renal disease, hydronephrosis and perinephric pseudocyst formation.
Clinical challenges:
Despite ultrasonography being a commonly used modality, many practitioners are not comfortable performing an ultrasound examination or interpreting the resulting images. Even for the experienced ultrasonographer, differentiating between incidental findings, such as a medullary rim sign, and pathological changes can be challenging.
Aim:
This review, part of an occasional series on feline abdominal ultrasonography, discusses ultrasonographic examination of the normal and diseased kidney and perinephric space. Aimed at general practitioners who wish to improve their knowledge of and confidence in feline abdominal ultrasound, this review is accompanied by high-resolution images and videos available online as supplementary material. A subsequent article will address ultrasonography of the collecting system including the renal pelvis and urinary bladder.
Equipment:
Ultrasound facilities are readily available to most practitioners, although use of ultrasonography as a diagnostic tool is highly dependent on operator experience.
Evidence base:
Information provided in this article is drawn from the published literature and the author’s own clinical experience.
Keywords
Scanning the urinary tract
B-mode ultrasonography is the modality of choice to image the feline urinary tract and is considered to be complementary to radiography. 1 The main indications for ultrasonography of the feline urinary tract include haematuria, stranguria, the identification of small, enlarged or irregular kidneys on abdominal palpation, the presence of azotaemia on bloodwork or abnormal urinalysis results and to investigate damage to the urinary tract in trauma cases. 2 Ultrasound provides information regarding the size, shape, contour and internal architecture of the kidneys, and the appearance of the ureters and retroperitoneal space, while negating the need for time-consuming excretory urography studies.2,3 Furthermore, sampling of renal parenchymal lesions can be readily performed under ultrasound guidance. As mentioned in previous articles in this series, despite being widely available, the principal disadvantage of ultrasonography is that its use as a diagnostic tool is largely dependent upon clinician experience, which is very variable.
Preparation
Where possible, it is usually desirable to fast animals waiting for an elective examination. This is arguably less important if the intention is to scan solely the urinary tract, although colonic gas can occasionally interfere with visualisation of the left kidney. Sedation is preferable if the ultrasound examination is to include the ureters. These are particularly small structures in the cat and immobilisation of the patient is necessary to identify and follow each ureter as it emerges from its respective kidney and travels caudally to the urinary bladder. Consequently, it may be necessary to fast animals regardless, to allow sedation to be administered safely.
Any abdominal hair in the region to be scanned should be clipped and acoustic coupling gel applied to remove the air gap between the transducer surface and the skin. As for imaging other abdominal structures in the cat, the use of a high frequency (ideally 11–15 MHz) linear transducer is recommended to provide optimum image resolution of the urinary tract. Readers are referred to previous articles in this series (the liver and the normal gastrointestinal tract – see box on page 423) for a more detailed discussion pertaining to patient preparation and transducer choice.
Scanning technique for the kidneys
Since the feline abdomen is narrow relative to that of most dogs, it is possible to scan both kidneys from the same side with the cat in lateral recumbency. The author’s preference, however, is to scan the left kidney with the cat in right lateral recumbency and vice versa (Figure 1). It is also possible to scan the kidneys with the cat in dorsal recumbency.

For scanning the left (a) and right (b) kidneys, the transducer is typically positioned just caudal to the last rib
The feline kidneys are relatively easy to find. They are typically more caudally located in the abdomen compared with canine kidneys and usually ventral to the third to fifth lumbar vertebrae, 4 hence it is not normally necessary to use an intercostal approach. Note they are very mobile and easily displaced by even mild transducer pressure. Their superficial location within the abdomen lends itself to the use of a high frequency transducer. Each kidney should be scanned in both transverse (from cranial to caudal) and longitudinal (medial to lateral) planes.
Given that it is possible to scan both kidneys from the same side with the cat in lateral recumbency, it is important to avoid inadvertently mistaking one kidney for the other – particularly in cats with unilateral renal disease. The safest way to identify which kidney is being imaged is to assess renal location in relation to the caudal vena cava and aorta (see box). If there is still doubt, the cat can be placed into dorsal recumbency and each kidney allowed to fall to its respective side and reimaged.
Normal appearance of the kidneys
Feline kidneys are oval in shape. Renal length from the cranial to the caudal pole in healthy cats varies from around 3 cm to 4.5 cm2,4–6 and is influenced by several factors including age, gender, neutering status and body weight.7–9 The kidneys tend to be larger in males and intact cats compared with females and neutered cats and are known to decrease in size with age.4,7–11 A study in 2013 reported mean renal size in three cat breeds: Sphynx (4.09 ± 0.33 cm), British Shorthair (3.77 ± 0.43 cm) and Ragdoll (3.87 ± 0.41 cm). 12 The ratio of cortical to medullary thickness was reported to be similar in all three cat breeds: Sphynx 0.93 ± 0.43, British Shorthair 0.91 ± 0.26 and Ragdoll 0.88 ± 0.31. 12 In some large breeds such as the Maine Coon, kidney size may naturally be slightly larger and fall outside of the normal range. In some cats, the right kidney may be slightly longer than the left, but the two kidneys should still be similar in length.4,9,11,12

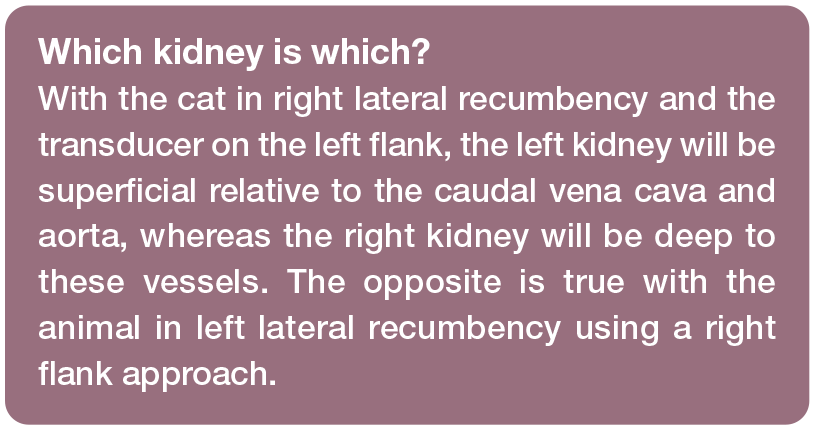
The renal capsule, outer cortex, inner medulla and collecting system can all be appreciated on ultrasound examination (Figure 2). The thin echogenic capsule surrounds the kidney except in the hilar region and is best visualised where the capsule is perpendicular to the beam. At non-perpendicular angles, echoes from the capsule are reflected away from the transducer and not detected. Triangular hypo-echoic zones may also be visible on either side of the kidney due to edge shadowing. 13
Ultrasound images of the normal feline kidney in longitudinal (a) and transverse (b) planes. 1 = renal capsule; 2 = cortex; 3 = corticomedullary junction; 4 = medulla; 5 = faint medullary rim; 6 = sinus; 7 = renal crest. In (a), note the normal acoustic shadowing (arrows) due to the presence of fat within the renal sinus. In (b), arrowheads indicate an edge-shadowing artefact and arrows highlight the normal proximal ureter as it emerges from the renal pelvis. Videos showing the normal kidney in longitudinal and transverse planes (with mild renal pelvic dilation, which can be a normal finding in some cats) are available as supplementary material
The renal cortex has a fine, granular echo-texture and is usually isoechoic to hypoechoic relative to the spleen, isoechoic to hyperechoic relative to the liver parenchyma and may be hypoechoic compared with the renal crest.10,14 An increase in echogenicity of the renal cortices of healthy cats is a common occurrence and is due to hormonally dependent intracellular fat deposition within the epithelium of the convoluted renal tubules of the cortex, leading to increased corticomedullary definition (Figure 3).15,16 This is more frequently observed in older, neutered male cats and can give the false impression of an abnormally hypoechoic liver if the liver and kidney are compared directly. 17 Thus, caution should be exercised when comparing renal echogenicity with that of other organs. 17 Interestingly, previous research has shown that there is no direct link between body condition score and the amount of lipid deposited within the kidney. 18

Increased cortical echogenicity, presumed to be due to fat deposition, in two cats aged 7 years (a) and 9 years (b) with no biochemical evidence of renal dysfunction. In (a), the renal cortex (1) is moderately hyperechoic relative to the spleen (2). In (b), note the enhanced corticomedullary definition as a result of increased cortical echogenicity. The measuring calipers indicate the craniocaudal length of the kidney
The medulla is the innermost part of the kidney and surrounds the renal pelvis. In normal cats, the medulla is hypoechoic compared with the cortex and can be almost anechoic, especially in younger individuals. It is, therefore, important not to confuse the normal medulla with dilation of the renal pelvis (pyelectasia). A clear demarcation should be present between the cortex and medulla. Short parallel echogenic lines at the corticomedullary junction represent the walls of the arcuate blood vessels. 10 Echogenic linear structures representing borders of the diverticula and interlobar vessels divide the medulla into lobular segments.
The peripelvic sinus often appears echogenic due to the presence of fat and can be particularly prominent in obese cats, 10 often exhibiting a faint distal acoustic shadow. 2 The renal pelvis is a potential space in many cats although, in some normal individuals, mild pelvic dilation up to 3.5 mm may be present (see the videos accompanying Figure 2, available as supplementary material).19,20 It may be possible to identify the normal feline ureter as it leaves the renal pelvis on transverse plane images if a high frequency transducer is used. However, unless ureteral dilation is present, the ureter can be very challenging to visualise ultrasonographically, since the normal ureteral diameter in the cat is only 0.4 mm. 21
Abnormalities of the kidneys
Diffuse disease of the renal parenchyma
While ultrasound is useful for detecting diffuse changes to the renal parenchyma, assessment is subjective, usually involving comparison with hepatic and splenic echogenicity. Assessing cortical echogenicity alone has been shown to be of limited use in the detection of mild degenerative or inflammatory renal disease in the cat. 31 Furthermore, ultrasound lacks specificity and there are often a number of differentials for any given diffuse change to the appearance of the kidney. For this reason, it is important to consider the ultrasound findings in the context of the signalment, clinical history, examination findings and any bloodwork available. It is also important to realise that the kidney can appear normal even when diseased.



Lateral thoracic radiograph of an 11-year-old female neutered domestic shorthair cat with a kidney (arrows) located in the caudodorsal thorax. Radiography was performed following an abdominal ultrasound examination during which only one kidney could be identified. Routine biochemistry and urinalysis revealed no evidence of renal dysfunction

Ultrasound image of the left kidney of a 3-year-old male neutered domestic shorthair cat with ethylene glycol toxicity. There is a marked increase in echogenicity of the cortex and outer medulla, resulting in the loss of normal corticomedullary definition. The cortex is hyperechoic relative to the spleen (asterisk). The right kidney had a similar ultrasonographic appearance. A video showing marked hyperechogenicity of the cortex and outer medulla of the kidney due to ethylene glycol toxicity in this cat is available as supplementary material
Increased cortical echogenicity
Increased cortical echogenicity may be seen as a result of glomerular or interstitial nephritis, acute tubular necrosis such as that seen with ethylene glycol or lily toxicity (see box), diffuse renal lymphosarcoma, feline infectious peritonitis (FIP) caused by feline coronavirus (Figure 6) and metastatic squamous cell carcinoma.1,32,33 Furthermore, increased renal echogenicity, renomegaly and pyelectasia were the most common ultrasonographic findings in a retrospective study involving 45 cats with acute kidney injury due to a variety of causes. 34
Ultrasound images of the left (a) and right (b) kidneys of a 6-month-old male Siberian cat with feline infectious peritonitis. Both kidneys are misshapen and have abnormally hyperechoic cortices. A large volume of echogenic retroperitoneal fluid is present bilaterally
Renal amyloidosis can also result in an increase in echogenicity of the renal cortex.10,35 Amyloidosis represents a collection of protein misfolding diseases in which abnormal quantities of pathologic amyloid protein are deposited between cells in various organs, ultimately resulting in organ failure. 36 Amyloid protein is insoluble and cannot be broken down by the body, eventually building up in certain tissues. The familial form of the disease is recognised in Abyssinian and Siamese cats as well as certain other oriental breeds.37–40 In the kidney, deposition occurs mostly within the medullary interstitium, although glomerular involvement is also common. 38 Despite widespread distribution of amyloid within different organs, the kidney is the main target organ in the Abyssinian; affected cats usually present with clinical signs related to chronic renal disease at a young age (<6 years).26,38 In contrast, the liver is primarily targeted in Siamese cats, resulting in chronic liver failure and/or spontaneous hepatic rupture.41,42
Additional ultrasonographic findings in cases of renal amyloidosis include bilaterally reduced corticomedullary definition and the presence of thick hyperechoic perirenal tissue. 14 Affected kidneys may be normal, increased or decreased in size depending on the duration of the condition.10,43 Decreased renal size is more common in the cat and may be accompanied by an increase in medullary echogenicity. 44
In cats with chronic end-stage renal disease such as that caused by chronic tubulointerstitial nephritis, chronic glomerulonephritis or chronic pyelonephritis, 45 there is often a concurrent increase in the echogenicity of the medulla resulting in a reduction or loss of normal corticomedullary distinction (Figure 7).35,46 The kidneys may also become small and irregular, and internal architecture may be difficult to appreciate. 46 Sometimes the cortex and/or medulla can have a striated appearance due to the presence of multiple radiating hyperechoic bands resulting from fatty change with tubular necrosis. There may be calcification of the renal parenchyma (nephrocalcinosis) and/or calculi within the renal pelvis. In some cases, it can be difficult to differentiate between parenchymal mineralisation close to the renal pelvis and calculi within the pelvis.

(a-c) Loss of corticomedullary distinction in three cats with chronic end-stage renal disease. In (c), the kidney is abnormally small and slightly irregular in outline. Slight mineralisation of the medulla was also identified (not shown). Videos showing a loss of corticomedullary distinction due to chronic end-stage renal disease are available as supplementary material
Unfortunately, most of the above ultrasonographic changes have a low sensitivity and low specificity for azotaemia. 11 Furthermore, renal abnormalities on ultrasound may be apparent in healthy, non-azotaemic cats, particularly when older.11,25 This may be due to a combination of increasing prevalence of subclinical renal disease as cats age 47 and the relative insensitivity of creatinine for the detection of renal disease. 48 Therefore, while ultrasonography can provide further information in cats with chronic renal disease, it is not recommended as a screening test. 11
Decreased cortical echogenicity
Decreased renal cortical echogenicity is a rare ultrasonographic change but may be seen in cats with acute renal failure and lymphoma. 2
Medullary rim sign
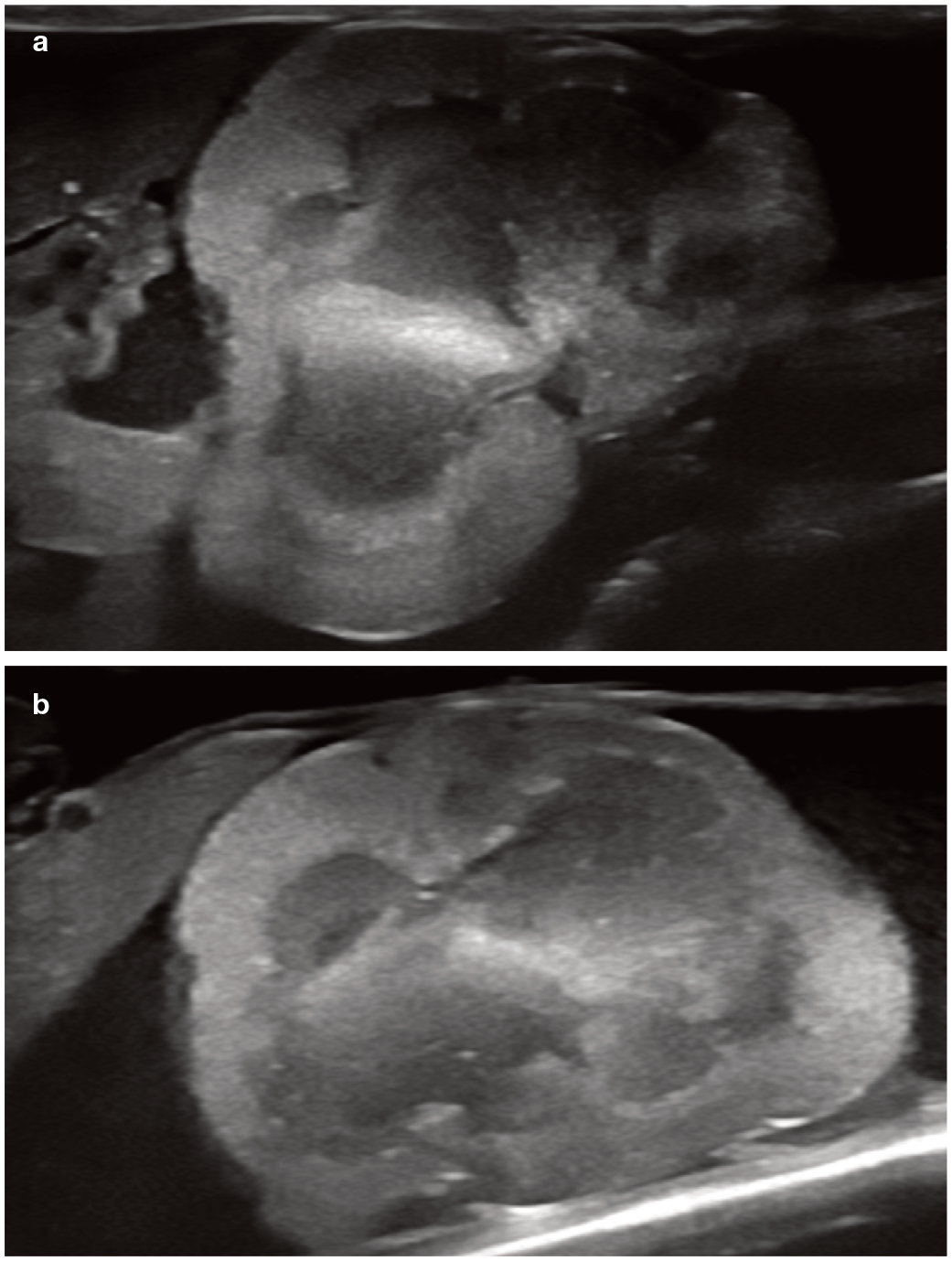
In some cats, a hyperechoic band paralleling the corticomedullary junction may be visible within the outer zone of the medulla. This is known as a medullary rim sign and has been recognised in both normal cats (especially older individuals) and in association with several pathological conditions such as acute tubular necrosis, pyogranulomatous vasculitis due to FIP, lymphoma, portosystemic shunts and chronic interstitial nephritis (Figure 8).15,32,43,49 In one study, the incidence of a medullary rim sign was similar in both azotaemic and non-azotaemic cats. 11 In many cases, the ultrasonographic appearance arises as a result of mineral deposition within the lumina of the renal tubules.15,49 The outer zone of the medulla is a highly metabolically active region of the kidney and hence vulnerable to ischaemia. 50 It is hypothesised that following an insult, damaged renal tissue may undergo dystrophic mineralisation resulting in a medullary rim sign. 49 In FIP, the medullary rim sign is believed to be the result of peri-vascular infiltrates producing an increased number and size of acoustic interfaces. 49
(a) Medullary rim sign (arrows) in the kidneys of a 4-month-old female domestic shorthair cat with a congenital extrahepatic portosystemic shunt. Note that both kidneys are visible from the same side. Uroliths, presumed to be ammonium urate, were also identified within the bladder during the ultrasound examination. A video showing the pronounced medullary rim sign in this cat is available in the supplementary material. (b) Medullary rim sign (arrows) in an 11-year-old domestic shorthair cat with lymphoma. A video showing a medullary rim sign in a cat with chronic renal disease is available as supplementary material
In summary, a medullary rim sign is a relatively common non-specific finding that can be seen in both normal and abnormal kidneys. Although, therefore, it is unreliable if used as the sole indicator of renal disease, it may signal subclinical renal disease or previous renal injury. 51 However, some authors have gone as far as to say that there is no evidence of an association between the medullary rim sign and clinical renal disease in cats, thus questioning its usefulness entirely. 11
Diffuse renal neoplasia
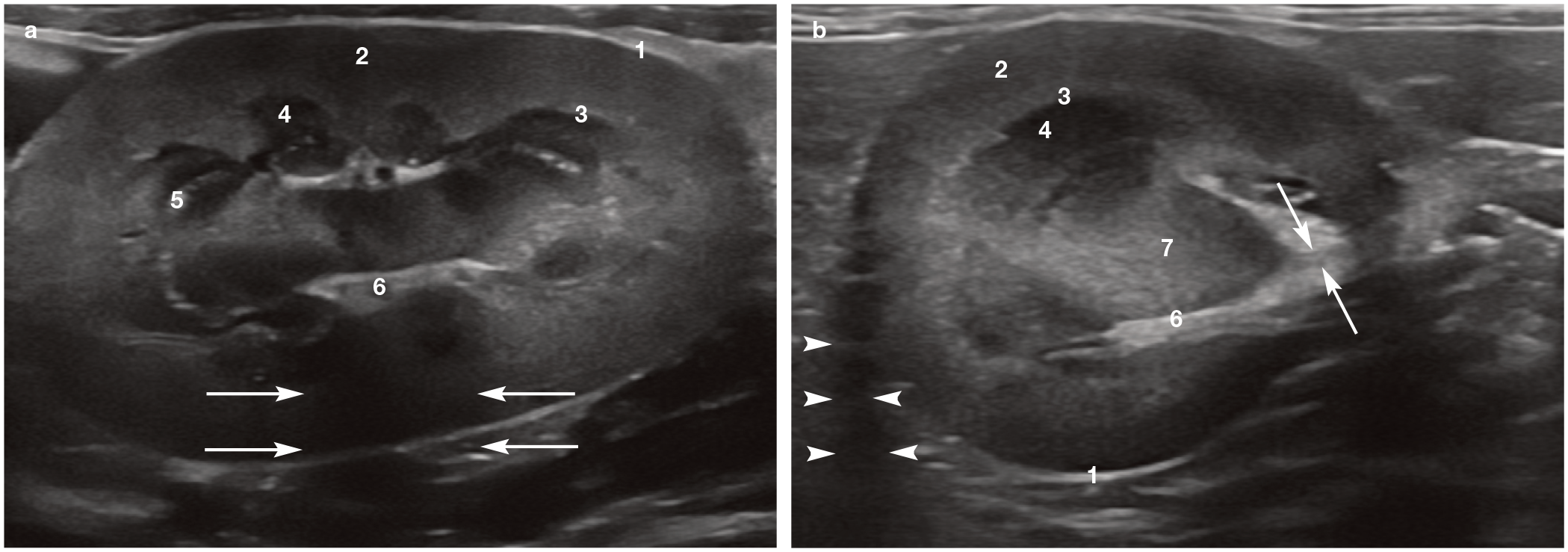
Most renal tumours produce focal lesions. An exception to this is lymphoma, which can also result in diffuse changes within the kidney. Lymphoma is the most common neoplasm of the feline kidney and occurs bilaterally in a high proportion of cases. Reported ultrasonographic findings include renomegaly, abnormal shape, increased cortical echogenicity, the presence of hypoechoic masses and nodules, pyelectasia and hypoechoic subcapsular thickening (Figure 9). 52

Renal lymphoma affecting the left (a,b) and right (c,d) kidneys in an 11-year-old male neutered domestic shorthair cat. Both kidneys are markedly enlarged (left kidney 6.5 cm in length; right kidney 7.0 cm in length), have hyperechoic cortices, mild pyelectasia and hypoechoic subcapsular thickening. The subcapsular thickening is shown more clearly between the arrows on the close-up view of the right kidney (d). A video showing renomegaly due to lymphoma is available as supplementary material
On ultrasound, the subcapsular thickening is recognised as a hypoechoic band or halo surrounding the renal cortex (Figure 10) and is believed to represent regional subcapsular infiltrate with lymphosarcoma tissue, rather than subcapsular fluid accumulation as had been previously hypothesised. This finding should not be confused with fluid due to a perinephric pseudocyst, which is anechoic and typically much larger in volume. Valdes-Martinez et al found that the hypoechoic subcapsular thickening had a sensitivity and specificity of 60.7% and 84.6%, respectively, for the diagnosis of renal lymphoma and positive and negative predictive values of 80.9% and 66.7%, respectively. 52 Therefore, hypoechoic subcapsular thickening, while frequently associated with lymphoma, is not pathognomonic for the condition and can also be seen in other disease processes such as FIP (effusive form), undifferentiated malignant neoplasia and renal anaplastic carcinoma.52,53 In some cats with lymphoma, hyperechoic foci or striations may also be visible throughout the medulla. 10

(a-f) Ultrasound images of the kidneys of five cats with renal lymphoma. Images (a) and (b) are from an 11-year-old male neutered Maine Coon with confirmed high-grade renal lymphoma. Both kidneys are markedly enlarged and irregular, and surrounded by a hypoechoic halo. Foci of mineralisation and mild renal pelvic dilation are also present. Images (c) and (d) are from a 12-year-old female neutered Siamese and a 6-year-old female neutered domestic shorthair cat, respectively. In each case, the kidney (indicated by the calipers in [d]) is enlarged, has a hyperechoic cortex and a hypoechoic halo (arrows) surrounding the cortex. Image (e) shows the left kidney of a 9-year-old male neutered domestic shorthair cat undergoing treatment for renal lymphoma. The kidney is mildly enlarged and slightly irregular. The cortex is thick and hyperechoic, and partially surrounded by a hypoechoic halo (arrows). Image (f) is from an 11-year-old male neutered domestic shorthair cat. Although no scale is visible, the kidney (indicated by the calipers) measured 4.7 cm in length, was mildly irregular and had reduced corticomedullary distinction
Focal and multifocal disease of the renal parenchyma
Focal renal lesions are usually easier to identify with ultrasound than diffuse changes. Interpretation of focal and multifocal changes within the kidneys is also typically less subjective compared with diffuse disease.
Cavitary lesions
The condition is congenital and characterised by the presence of renal cysts. Most cysts occur within the cortex or at the corticomedullary junction. 64 As the cat matures, the cysts progressively grow in size and insidiously replace normal renal parenchyma, resulting in a steady decline in renal function. In some cats, cysts will also develop in the liver and pancreas (as discussed in the previous article in this series on the pancreas – see box on page 423).54,65 On ultrasound examination, the cysts are thin-walled, spherical or ovoid, variably sized structures with anechoic contents that are usually associated with strong distal acoustic enhancement (Figure 11). 54 Differentiation of a cyst from a solid hypoechoic mass is achieved by increasing the gain setting on the ultrasound machine. 14 Internal echoes will usually appear within a solid mass, whereas a cyst will normally remain anechoic. The presence of echogenic material within a cyst can be an indicator of infection, 22 haemorrhage, side and/or grating lobe artefact or range ambiguity artefact resulting from echoes produced by structures beyond the kidney.13,64 Loss of normal corticomedullary distinction and foci of mineralisation may also be detected. 64

(a) Ultrasonographic appearance of polycystic kidney disease (PKD) in a 2-year-old male neutered domestic shorthair cat with multiple cysts, some septated, throughout both kidneys. (b) Severe PKD in a 16-year-old male neutered Persian cat. Cysts were also identified within the liver and pancreas
Ultrasound is very sensitive for the detection of PKD and there is good agreement between ultrasound and genetic testing. 62 Cysts can be identified ultrasonographically by an experienced ultrasonographer using a high frequency transducer from around 7 weeks of age onwards. 62 Biller et al reported a sensitivity of 91% for the ultrasonographic detection of renal cysts in cats over 36 weeks of age, although this reduced to 75% in cats under 16 weeks of age. 58 A study conducted over a decade later reported a slightly higher sensitivity of 96.2% and a specificity of 91% when assessing cats between 10 and 12 weeks of age. 54 The improved sensitivity is most likely to be due to advances in ultrasound technology in the intervening period. A separate study demonstrated that ultrasound had 100% repeatability for the detection of renal cysts when used in cats 10 months of age and older. 63
Although genetic testing is available, and can be used in cats of any age, it is only able to detect PKD that is associated with the PKD1 mutation. 63 Furthermore, while ultrasound allows the severity and progression of the disease to be determined, this is not possible with the genetic test. 54 It is, therefore, recommended that both genetic testing and ultrasound are used to evaluate at-risk individuals to ensure optimal diagnostic sensitivity and to monitor progression of the disease. 54
It should be noted that not all renal cysts are associated with PKD. Cystic renal disease has been identified with low prevalence in Maine Coons but is unrelated to the PKD observed in Persian cats (Figure 12). 66 Also, occasional cysts may be present in the renal cortex of cats with chronic renal disease and are usually considered to be incidental findings. 10 A renal cystadenoma has been reported in an 11-year-old domestic shorthair cat and should be considered a differential for any complex cystic structure associated with the kidney. 67

Two small cysts (arrows) within the kidney of a 3-year-old male neutered Maine Coon cat. There is also a reduction in corticomedullary distinction
Bilateral perirenal abscesses have also been reported in a male neutered domestic shorthair cat. 69 In this case, abdominal ultra-sonography revealed the presence of a bilateral perirenal subcapsular accumulation of fluid containing echogenic debris. The kidneys were hyperechoic with reduced corticomedullary distinction and a medullary rim sign. Perirenal abscessation was confirmed following ultrasound-guided drainage of the subcapsular fluid, which revealed a large number of degenerate neutrophils and bacterial cocci. Concurrent necrotising suppurative pyelonephritis was diagnosed on histopathological examination post mortem.
Although not described in the case reports above, abscesses can also contain gas, resulting in a reverberation artefact within the abscess lumen.
Renal infarction
Renal infarcts are commonly identified during ultrasound of the feline kidney and are more frequently present in older cats. 71 An infarct is a region of necrotic tissue, usually a renal pyramid, that has been deprived of its blood supply. Infarcts may be classed as acute or chronic, although the vast majority seen in cats are chronic. Using ultrasound, chronic infarcts are recognised by the presence of a wedge-shaped or linear hyperechoic zone within the renal cortex (Figure 13). 10 The renal capsule may be slightly indented at the level of the infarct due to contraction of fibrous tissue and, in some cases, an acoustic shadow may be seen due to the hyperattenuating properties of the infarct. 10

(a,b) Multiple hyperechoic wedge-shaped lesions representing chronic infarcts are present throughout the cortex of the left kidney of a 12-year-old male neutered domestic shorthair cat with chronic kidney disease. A video showing incidental chronic renal infarcts at the caudal pole of the left kidney of an elderly cat is available as supplementary material
Chronic infarcts are usually considered to be incidental findings, 35 although a study of 600 cats found that those with renal infarction were 4.5 times more likely to have hyper-trophic cardiomyopathy than individuals without renal infarcts. 71 This led the authors of the study to recommend screening cats with renal infarcts for occult cardiomyopathy. 71 Interestingly, cats with hyperthyroidism were not more likely to have renal infarction compared with cats without the disease.
Solid parenchymal lesions
Differentials for solid focal or multifocal lesions within the renal parenchyma include granulomas and neoplasia. Neoplasms of the feline kidney include lymphoma, carcinoma, sarcoma and metastatic disease. As mentioned earlier, lymphoma can result in the presence of solitary or multiple hypoechoic nodules or masses within one or both kidneys (Figure 14). Carcinomas, sarcomas and metastases are more likely to present as heterogeneous nodules or masses with mixed echogenicity, although hypoechoic and hyperechoic masses are also possible (Figure 15).

Large multilobulated hypoechoic mass (arrows) at the caudal pole of the kidney of an 8-year-old male neutered domestic shorthair cat. A diagnosis of renal lymphoma was confirmed following ultrasound-guided fine needle aspiration of the mass
Granulomatous diseases affecting the kidney are rare. 72 However, granulomatous and pyogranulomatous lesions can be seen in cats with the dry form of FIP, in which renal involvement is common. 73 Renal granulomas due to FIP may present as hyperechoic nodules, sometimes with a hypoechoic centre, 10 and are often seen in conjunction with renomegaly and abdominal lymphadenopathy (Figure 16). 53

(a,b) Small focal hyperechoic lesions (being measured between the calipers) within the kidneys of a 6-year-old Ragdoll cat with suspected metastatic carcinoma. A video showing a renal nodule within the cortex of the left kidney of this cat, suspected to represent metastatic carcinoma, is available as supplementary material. (c) Large, hyperechoic (compared with normal renal cortex) mass located at the caudal pole of the kidney of a 9-year-old female neutered domestic shorthair cat. Nephrectomy and subsequent histopathology revealed the mass to be a well-differentiated renal carcinoma. (d) Large, irregular and partially cavitary, hypoechoic mass (arrows) occupying the caudal pole of the kidney of a 9-year-old male neutered British Shorthair cat. Note the slight increase in echogenicity of perirenal fat at the site of the mass. A high-grade sarcoma was confirmed by histopathology. (e) Renal cell carcinoma (papillary variant) of the right kidney of a 12-year-old male neutered domestic shorthair cat. The caudal pole of the kidney is effaced by a large heterogeneous mass (arrows). A small anechoic area of presumed necrosis was identified within the mass

Subtle focal heterogeneous lesions (arrows) within the renal cortices of a 10-month-old male neutered domestic shorthair cat with feline infectious peritonitis. Videos of these lesions in the same cat are available as supplementary material
Perinephric disease
Perinephric disease occurs only infrequently in cats and encompasses perinephric/retroperitoneal fluid, and perinephric pseudocysts, haematomas, urinomas and abscesses (see page 419 for ultrasonographic description of perirenal abscessation). 74
Retroperitoneal fluid due to acute renal failure
With the onset of acute renal failure, hypoechoic to anechoic fluid may start to accumulate within the retroperitoneal space. In a study of 238 cats, the presence of perinephric fluid was more strongly associated with azotaemia than any other ultrasound finding. 11 In a further study of 45 cats with acute kidney injury, retroperitoneal fluid was associated with oliguria and anuria, although all cats had received intravenous fluid therapy prior to imaging. 34 Retroperitoneal fluid is believed to represent an ultrafiltrate caused by fluid leaking in a retrograde fashion from the tubules into the interstitial space and overwhelming lymphatic drainage within the perirenal and retroperitoneal connective tissues. 75 Obstruction to urine flow may also play a role. 75
Perinephric fluid should be differentiated from subcapsular fluid or fluid due to a perinephric pseudocyst (below). Perinephric fluid creates confluent anechoic fluid pockets dissecting between areas of retroperitoneal fat and forms a pointed shape along its non-renal border. 11 It may be a more accurate indicator of renal disease than the ultrasonographic appearance of the kidney and is more likely to be present following intravenous fluid administration rather than at presentation in hypovolaemic cats. 11
Perinephric pseudocysts
Occasionally, fluid collects between the renal cortex and the capsule, resulting in a peri-nephric pseudocyst. The term pseudocyst reflects the fact that there is no epithelial lining and hence these are not true cysts per se. 76 The fluid is usually a transudate or modified transudate that accumulates as a result of underlying parenchymal disease, and can be unilateral or bilateral.77,78 Older male cats appear to be predisposed to the condition and many present for investigation of abdominal distension and clinical signs referable to renal dysfunction.76–82
Ultrasonography is the method of choice to diagnose perinephric pseudocysts. 74 Ultra-sonographically, the kidney is surrounded by a large volume of subcapsular fluid that tends to increase in size over time (Figure 17).74,83 Fluid within the capsule is typically anechoic, reflecting a low protein and cell content. Since concurrent renal disease such as chronic interstitial nephritis is common, the kidneys may be small and irregular, and diffusely hyperechoic with a loss of normal corticomedullary distinction.76,77 Perinephric pseu-docysts have also been reported in association with PKD, hydronephrosis, hydrothorax (due to a direct communication between the pleural cavity and pseudocyst) and renal neoplasia.77,82,84 While the majority of pseudocysts are subcapsular, extracapsular fluid accumulation (between the renal capsule and retroperitoneal lining) has also been reported in two cats.84,85
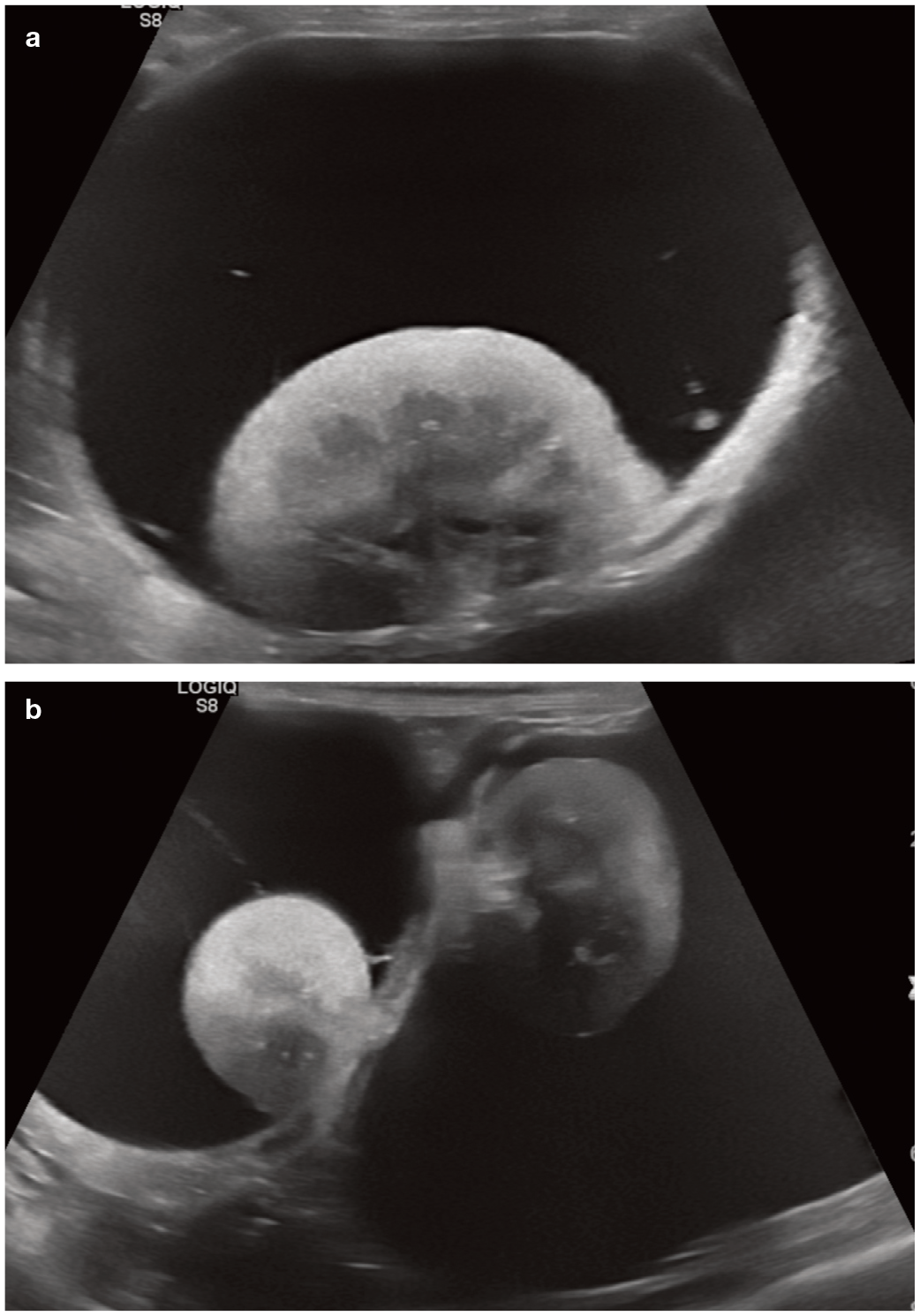
(a,b) Bilateral perinephric pseudocysts in a 15-year-old male neutered domestic shorthair cat that was initially presented with marked abdominal distension noted by the owner. The kidneys are small and irregular, with reduced corticomedullary distinction. Urine specific gravity was 1.012, consistent with a reduced concentrating ability and compatible with chronic kidney dysfunction
Perinephric pseudocysts can contribute to abdominal discomfort, and while percutaneous drainage under ultrasound guidance can help to temporarily alleviate this, recurrence is common.77,78,83 Surgery to resect the renal capsule may prove more effective in preventing reaccumulation of fluid and relieving clinical signs; however, neither this procedure nor percutaneous drainage will alter the progression of the underlying renal disease.77,80 The long-term prognosis for cats with pseudocyst formation is determined by the severity of the renal dysfunction present at initial diagnosis. 77

Urinoma
Leakage of urine from the urinary tract as a result of trauma can lead to the formation of a uriniferous pseudocyst (urinoma),86,87 which can mimic the appearance of a peri-nephric pseudocyst resulting from chronic renal disease. The two may be differentiated by aspirating fluid from the cyst. Urea and creatinine levels will be higher in a urinoma than in the bloodstream. 86

Perinephric abscessation and haemorrhage
Perinephric abscessation and haemorrhage are further differentials to consider when peri-nephric fluid is present. 88 However, abscesses and haematomas generally contain echogenic, rather than anechoic, fluid and haematomas are usually associated with a history of trauma (Figure 18).74,89 Additionally, aspiration and analysis of cystic fluid should allow the distinction to be made.

Fluid (F) within the retroperitoneal space in a 5-year-old male neutered domestic shorthair cat presenting with a recent history of lethargy and inappetence; 8 weeks prior to referral the cat had an abscess resulting from a bite wound along the dorsum. A moderate volume of highly echogenic fluid was present throughout the retroperitoneal space, consistent with pus. Fine-needle aspiration of the fluid confirmed the diagnosis of retroperitoneal empyema. Asterisks indicate retroperitoneal fat

Ultrasound image of the left kidney of a 3-year-old male neutered domestic shorthair cat with chronic membranous glomerulonephritis, confirmed following a Tru-cut biopsy. The biopsy site is mildly hyperechoic (arrow) relative to the rest of the cortex. Mild haemorrhage (arrowhead) has occurred caudal to the kidney, the volume of which was clinically insignificant
Key Points
The normal length of the feline kidney is 3.0–4.5 cm.
Echogenic renal cortices are common in healthy cats due to lipid deposition within the epithelium of the convoluted renal tubules.
Ethylene glycol toxicity results in a profound increase in renal cortical echogenicity within hours of ingestion. Over time, medullary echogenicity increases, leading to a loss of corticomedullary distinction.
In cats with chronic end-stage kidney disease, the kidneys are small and irregular, often with increased echogenicity and a loss of corticomedullary distinction. The cortex may appear striated and parenchymal mineralisation is not uncommon. Renal pelvic dilation is also present in some cats.
A subcapsular hypoechoic halo around the kidney can be suggestive of lymphoma but is also seen in other conditions such as FIP. Definitive diagnosis requires tissue sampling.
PKD may be accompanied by cysts within the liver and pancreas.
Ultrasound can be used to diagnose perinephric pseudocyst formation, which has a characteristic appearance. Renal changes are usually also visible due to underlying CKD.
Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not necessarily required.
Informed consent
This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.